1. Introduction
Many orthodontists in their practice have encountered under-age patients with disabilities whose oral health tends to be poorer than in the healthy population. Access to dental services for people with disabilities is difficult and expensive. Dental treatment in people with disabilities is challenging, as patient cooperation during procedures is difficult to achieve or outright impossible. Only about 40% of patients with disabilities cooperate with their dentist to the extent of making treatment possible [
1]. The other portion can only be treated under general anesthesia. This requires specialized equipment and additional staff qualified to work under such conditions, i.e., an anesthesiologist and a nurse anesthetist. Dental care provided under general anesthesia includes comprehensive conservative treatment, preventive treatment, and a range of surgical procedures [
1]. In Poland, insured disabled patients are guaranteed free dental care with refunds from the National Health Fund. The funding of orthodontic treatment for people with disabilities by the National Health Fund is subject to the same rules as those for healthy people. Before any orthodontic treatment can be undertaken, it is necessary to obtain dental impressions.
Classical impressions are particularly problematic in patients with disabilities due to difficulties associated with patient cooperation resulting from intellectual disabilities or in patients with various developmental disorders.
Fixed braces are not practicable in adolescent patients with disabilities due to the hygienic and nutritional challenges involved, the handling of the braces themselves, and the fact that such a treatment is not covered by health insurance. Orthodontic treatment for young patients with disabilities is therefore limited to the use of removable orthodontic appliances. It is very difficult or outright impossible to take good dental impressions in patients with disabilities without general anesthesia. The primary goal of dental impressions is to replicate the intraoral condition of the patient, forming an accurate and representative model. The acquisition of a high-quality model that closely resembles the original is crucial for the success of orthodontic treatment. Throughout the years, various impression materials and techniques have been employed to attain the desired level of precision [
2]. In the age of swift digital advancement, new imaging technologies have emerged in the field of dentistry as well. Digital Dentistry Technology (DDT) systems have surfaced, enabling the capture of three-dimensional images within the patient’s oral cavity. The term “CAD/CAM” (Computer-Aided Design/Computer-Assisted Manufacturing) pertains to the utilization of computers to assist in the design and fabrication of orthodontic and prosthetic appliances [
3,
4]. In dental prosthetics and implant prosthetics, the achievements of digital dentistry are applied especially at the stage of making intraoral records of the prosthetic field (intraoral scanners) and in the fabrication of prosthetic dental restorations (dental laboratory scanners and milling machines). Dentists are particularly interested in the applicability of the intraoral scanner: its usefulness and reliability in clinical procedures and potential interoperability with the relevant laboratory instrumentation [
5]. The digital transformation has also been embraced in orthodontics [
6,
7].
In 1999, Orthocad from Częstochowa introduced pioneering software that revolutionized orthodontics by enabling the scanning of impressions directly at the company’s headquarters. These scans were then used to generate digital 3D models, enabling the digital analysis and archiving of orthodontic data [
8,
9]. To date, many intraoral scanning devices have been developed around the world. In the future, digital optical impressions may eliminate the need for traditional impressions. The scanner enables the utilization of treatment techniques through computer software, whether for creating a clear aligner or for producing prosthetic restorations in a laboratory. This has streamlined access to digital technologies and enhanced the planning and monitoring of treatment progress, thereby augmenting its overall effectiveness [
8,
9,
10]. The scanning technique employed in this system has been designated the “Parallel Confocal/Telecentric” method, rooted in the principles of confocal microscopy. This method leverages parallelism and telecentricity to achieve precise and detailed imaging, enhancing the accuracy and reliability of the scanned data. Scanners provide several notable advantages, including minimized patient discomfort, enhanced time efficiency, streamlined clinical procedures, and simplified data storage. Their capacity for swift and uncomplicated electronic data transfer facilitates seamless communication, ensuring quick and easy access to information. This not only improves overall workflow but also contributes to the convenience and efficiency of orthodontic practices [
11]. In orthodontics, as in all branches of dentistry, the brief duration of clinical procedures is pivotal for ensuring a successful and comfortable experience for both the dentist and the patient. Efficient and time-effective procedures not only contribute to patient satisfaction but also optimize the overall workflow in orthodontic practices. This emphasis on a swift yet thorough approach underscores the commitment to delivering effective and patient-friendly orthodontic care [
12]. It is to be expected that computer-assisted treatment methods will determine the way dental surgeries and orthodontic and prosthetic laboratories operate in the future.
The objective of the study was to assess the time required for intraoral scanning using a scanner in the orthodontic treatment of patients with disabilities undergoing clear aligner therapy in comparison to the time needed for healthy subjects and to determine whether it is possible to perform such a procedure in disabled patients without the need for general anesthesia.
2. Material and Methods
The study participants were patients treated at a private orthodontic office in Szczecin, which had a contract with the National Health Fund for the treatment of disabled patients. All patients were qualified for orthodontic treatment using clear aligners. The participants were divided into two groups, each consisting of 42 individuals aged 8 to 12 years. Group I comprised patients with a disability certificate, with the level of disability classified as moderate. According to the criteria outlined in the Act on Vocational and Social Rehabilitation and Employment of Disabled Persons, moderate disability is characterized by impaired functionality of the body, resulting in the inability to work or perform professional duties, particularly in environments with limited work opportunities. In Group I, there were 11 boys and 31 girls. Patients with mild and severe levels of disability were excluded from this group. Group II (control) consisted of patients without a disability certificate. In this group, there were 21 boys and 21 girls.
In order to develop a treatment plan and fabricate braces, it is necessary to take impressions with silicone material in a two-step process or scan the patient’s teeth with an intraoral scanner. Maxillary and mandibular scans and bite registrations were performed with iTero Align Technologies (Cadent), software version 1.9 in Groups I and II. The scanner software enables time measurement throughout the scanning process. This functionality was used to evaluate the scan capture time in each group. An integrated portable scanner was used, consisting of a scanning camera (handpiece) and a computer with a monitor. The device allows for breaks to be taken during scanning. The multiple captured images are automatically stitched together into a whole. The digital impression is exported through a web portal to an external dental laboratory. Before scanning, teeth must be dried to accurately represent the oral situation.
Patient cooperation in the course of scanning was also noted. The research team consisted of 2 people. All scans were performed by one person who had been working with the scanner for one year. A second person from the team kept an eye on the sequence of scanning procedures and recorded the scanning time.
The statistical analysis of the results was conducted using Student’s t-test, and significance was set at p < 0.01. Boxplots depicting the distribution of scanning times were generated using the R statistical program, version 4.1.2 (The R Foundation for Statistical Computing, Wirtschaftsuniversität Vienna, Austria).
3. Results
The findings of the study are consolidated in two tables and two figures. Scan capture times for Groups I and II are presented in
Table 1 and
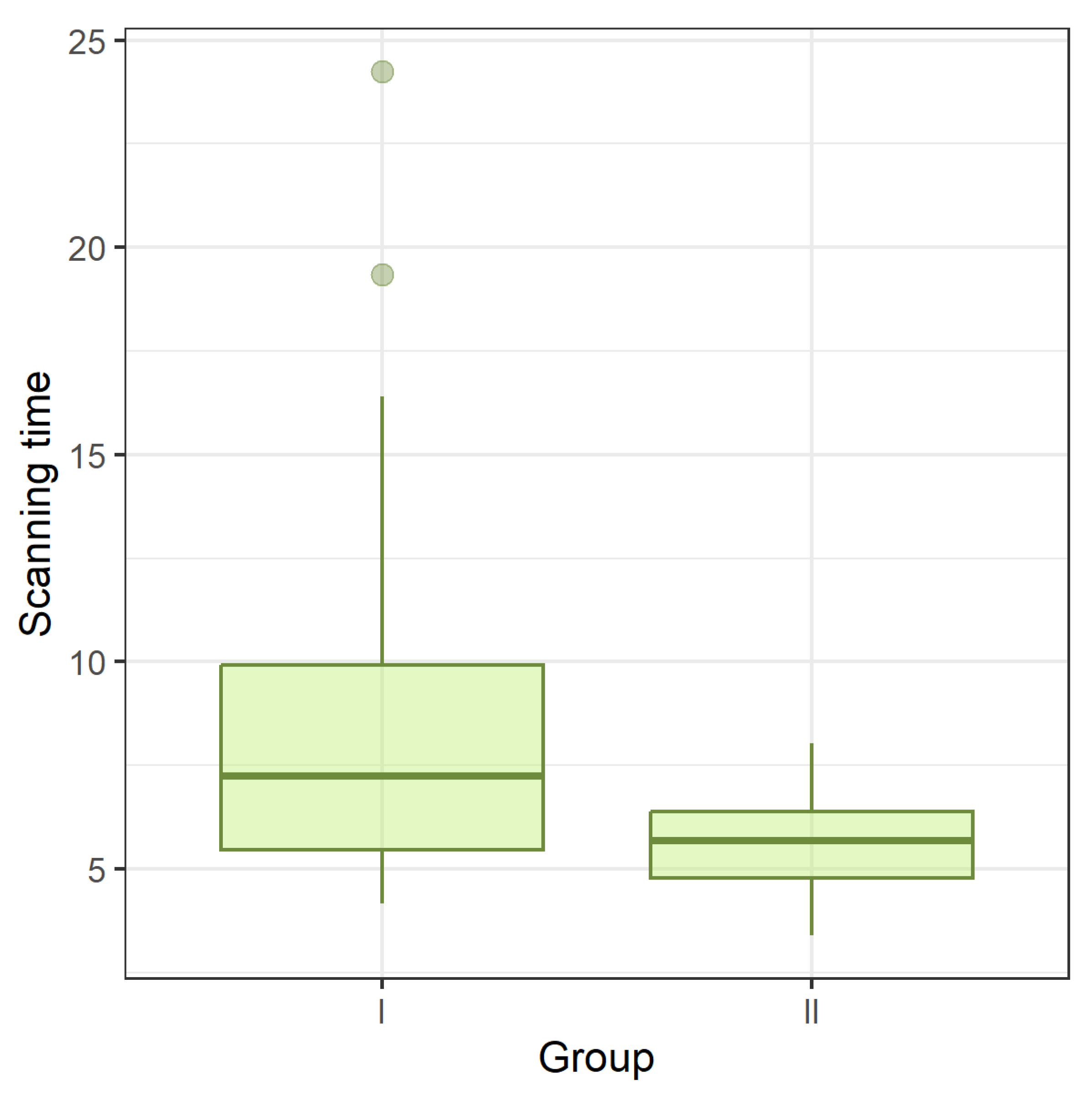
Figure 1.
No significant statistical differences were found between boys and girls in the two groups. In all patients in study Group I, full-mouth digital records were successfully taken without resorting to general anesthesia. The maximum scanning time in this group, recorded in a female patient, was 24.25 min. Despite such a long scanning time, a valid scan was captured. The long time was due to breaks taken during scanning for the patient to calm down so that the scanning could be resumed. Another patient in Group I, who did not cooperate on the first visit, had the scans taken without much difficulty on a subsequent visit. The scanning process itself and the images on the monitor kept the patients occupied and had a positive effect during the scanning procedure.
The mean scanning time in Group I was 8.59 min, and in control Group II—5.71 min.
The results demonstrated statistical significance, reaching a significance level of p < 0.001. Nevertheless, it is important to note that scans were successfully acquired from all patients in study Group I without the need for general anesthesia.
4. Discussion
In orthodontics, alginate impression masses are most commonly used for preparing removable acrylic appliances and for creating diagnostic models before treatment with fixed appliances. The time required to take an impression using alginate material, according to the manufacturer’s guidelines, is approximately 2.5 min, meaning that it takes 5 min to complete a set of impressions [
13]. Bite registration in the conventional approach is typically carried out using wax, which requires additional time. In the case of clear aligner treatment, if a scanner is not available, impressions need to be taken using silicone material in a two-step process. The time required for the two-step impression technique, as per the manufacturer’s guidelines, is around 4.5 min for the first step and 5 min for the second step. Therefore, a total of 14.5 min is needed for impressions of both arches [
14]. Occlusion registration is determined by technicians based on intraoral photographs and occlusion registration traces using an occlusal stencil.
In the literature, we did not find studies describing the scanning of patients with a disability assessment in orthodontic treatment. The time required for obtaining a digital impression using an intraoral scanner, as opposed to the time associated with obtaining a traditional impression, has been analyzed in several studies [
15,
16,
17]. Numerous studies consistently confirm that the chairside time needed to take alginate impressions is generally shorter compared to the time required for digital impressions [
16]. Furthermore, in a comparative analysis of intraoral scanning, alginate impressions, and polyvinyl siloxane (PVS), it was observed that alginate impressions still require the least amount of time [
17]. The process of scanning the upper and lower dental arches along with bite registration using a scanner in our control studies took 5.71 min, aligning with these described results. Sfondrini et al. [
18] discovered that the latest-generation scanners not only reduce the chairside time but also shorten the data-processing time.
Lee and Gallucci [
19] conducted a study using the iTero intraoral scanner. They compared digital impressions with traditional impressions made by a group of students. The results of their study indicate that the digital impression technique is easier to perform and requires less time and effort compared to traditional methods. It is also possible to repeat part of the study without the need to retake the entire impression. This feature was particularly useful in our study with patients from Group I with a disability assessment. These patients were more impatient, often requiring breaks during scanning, which extended the scanning time. Traditional impression taking using impression material cannot be interrupted until the material is completely set [
20,
21,
22]. In patients with disabilities, such impressions are often obtainable only under general anesthesia. This study found that intraoral scanning requires significantly less time than taking silicone impressions. However, it is important to note that potential intraoral anatomical differences and limited mouth opening may introduce complexity and potentially prolong the procedure. It is worth noting that the substantial vertical dimension of the scanner head used in the study may pose a challenge in capturing data from hard-to-reach areas.
For patients, scanning was less unpleasant than the standard procedure of taking impressions. Overall, it has been observed that digital impression methods provide greater comfort compared to conventional methods [
4,
12,
15,
18,
19,
23]. When patients were surveyed about comfort after undergoing conventional impressions (PVS or alginate) and intraoral scanning, impressions taken with digital methods and alginate were statistically more comfortable than those taken using PVS [
24].
The intraoral scanner scored higher in terms of reduced vomiting reflex and ease of breathing [
4].
A strong gag reflex can hinder the process of taking a traditional impression, especially in healthy patients, let alone in patients with disabilities. In all of these studies, it was found that the gag reflex is significantly reduced or even absent when digital methods are used [
3,
15,
23]. In our own studies, within Groups I and II, there was no observed occurrence of the gag reflex during scanning. Certainly, intraoral scanning may be the preferred method for patients with an overactive gag reflex.
The perception of time in relation to the impression method (conventional or digital) has been thoroughly examined, with intraoral scanning consistently appearing more comfortable for patients in terms of time [
4,
15,
16,
23,
24]. Burzynski et al. [
16] reported that patients perceived the digital method as being faster than expected, and Sfondrini et al. [
7] observed that although some patients still considered the intraoral scanning time to be long, they preferred the digital method in terms of time perception. This was particularly evident in our own study among patients with disabilities.
Intraoral digital impressions provide significant comfort for the patient, but at the same time, this is just the beginning of the benefits of a scanner [
12]. In addition to replacing traditional impressions, a scanner also serves a crucial diagnostic function. The quick and patient-friendly digital registration of an intraoral situation provides immediate access to a three-dimensional image. It allows for a preliminary analysis of dental arches in various projections and magnifications. Intraoral scanning enables the precise measurement of various dental parameters, including tooth size, transverse dimensions, Bolton discrepancies, overbite, and overjet. This technology allows for an accurate and detailed assessment of these dimensions, contributing to a comprehensive understanding of tooth anatomy and facilitating precise treatment planning in orthodontics [
3]. In contrast to the conventional procedure, this analysis is only possible several hours later. With intraoral scanning, it becomes possible to observe premature contacts on a monitor and immediately simulate a preliminary treatment plan. It is worth noting that the latest iTero Element 5D scanner with NIRI technology also includes caries detection features, expanding its diagnostic capabilities beyond traditional methods [
25]. Above all, digital impressions, compared to their conventional counterparts, guarantee absolute quality, and precise access to all anatomical details holds tremendous value in recording the prosthetic field.
Another advantage of using a scanner is that the dentist can participate in the design of dental prosthetics or orthodontic treatment. Integrating intraoral scanning allows for the creation of a digital diagnostic set, facilitating the simulation of a treatment plan. This capability not only aids in planning and visualizing the proposed treatment but also contributes to establishing a more meaningful and substantive relationship with the patient. The ability to visually communicate and involve patients in the treatment planning process can enhance their understanding and satisfaction with the proposed orthodontic interventions [
4]. With Invisalign orthodontic treatment, we have the ability to monitor the treatment process at each stage. Therefore, the use of intraoral scanning is highly beneficial and undisputed in dental practice. The ability to analyze registered images provides an opportunity to streamline clinical work and enables a quick flow of information both within the office and externally to the patient and dental laboratories [
26,
27]. The ease of digital data transfer significantly shortens transport time reduces costs and facilitates the visualization process, resulting in fewer inaccuracies and a shorter processing time in the laboratory [
4,
28].
The proper utilization of a scanner is a matter of training, and the benefits of using these devices undoubtedly encourage the adoption of the latest technology in dental practices [
29,
30]. Mangano et al. [
4] emphasized in their article that there is a learning curve associated with the introduction of intraoral scanning into dental clinics, and this aspect should be taken into account. Clinicians who are more familiar with digital technologies are likely to integrate scanners into their practice more easily. Conversely, older, less-experienced practitioners may perceive the use of these devices and associated software as more complex. The level of technological proficiency and adaptive abilities of practitioners can influence how easily they incorporate digital tools, such as intraoral scanners, into their workflows. Continuous training and support can be beneficial for clinicians transitioning to digital technologies [
31].
In the context of Invisalign treatment, intraoral scanning has been found to be a more appealing option for patients [
32]. It effectively distracts them from the typically controlling environment of a dental office. Additionally, the presence of parents, the age of patients, and thus, their level of maturity, are still considered potential disruptive factors. These factors must be taken into account, especially for underage patients with disabilities. Teenage patients in our study from both groups were intrigued by the scanner and the emerging image of their bite on the monitor, effectively reducing the disruptive factor. From our experience, digital impressions prove to be more time-efficient, requiring less time than traditional impressions. The ability to scan the entire arch in less than 3 min, combined with subsequent time savings (eliminating the need for gypsum models), positions intraoral scanning as a time-effective tool in the orthodontist’s toolkit.
In light of the latest advancements in Digital Dentistry Technology (DDT) and CAD/CAM, it is expected that computer-assisted treatment methods will define the operations of dental offices and prosthodontic laboratories in the future. Intraoral scanning appears to be an ideal method and may represent the future of orthodontics. It not only facilitates clinical procedures in terms of time and comfort for both the patient and the dentist but also serves as a starting point for the production of various customized orthodontic appliances, with aligners emerging as the most prevalent. With the continued development of aligner technology, intraoral scanners are becoming increasingly indispensable in modern orthodontic practices. It is anticipated that in the coming years, digital techniques will become an integral part of producing almost all orthodontic appliances. The ongoing evolution of 3D technology, particularly intraoral scanners, is ready to revolutionize the “way of thinking” in orthodontics, modernizing the role of the “traditional” orthodontist in diagnosis and treatment processes. Currently, the optimal approach involves integrating both conventional and digital impression methods in daily orthodontic clinical practice, leveraging the strengths and eliminating the limitations of each method.






{kind=link}