Abstract
Hamstring muscle injuries account for 12% of all injuries in soccer players. Several studies claim that the hamstring/quadriceps (H/Q) strength ratio has the potential to predict hamstring injuries, although the current evidence is not robust enough to definitively support this claim. Therefore, the main objective of the present study is to analyze whether there are changes in the H/Q ratio at different knee flexion angles and establish a measurement protocol capable of reducing the high prevalence of hamstring injury. We performed an observational study with 24 third-division soccer players. The conventional isokinetic H/Q strength ratio and H/Q strength ratio were measured at different knee flexion angles (15°, 30°, 45°, 60°, and 75°) at 60°/s and 180°/s. The conventional H/Q ratio differs from the H/Q ratios at 15° and 30° knee flexion at 60°/s and from the H/Q ratios at 15°, 45°, 60°, and 75° at 180°/s (p < 0.05). Based on the results obtained in this study, we recommend calculating the H/Q ratios at 15° and 30° knee flexion in the protocol for measuring the flexor and extensor strength of the knee. This additional data will establish more specific cut-off points that could predict and prevent future hamstring muscle injuries.
1. Introduction
Professional soccer has seen an increase in physical demand [1], leading to a rise in muscle injuries [2], particularly in the hamstring muscles [2,3]. This type of injury accounts for 12% of all injuries in professional soccer, and this figure rises to 33% for muscle injuries alone [4,5]. Hamstring injuries occur with greater incidence during matches [6], and 56% of hamstring injuries occur during the second hour of sports practice [7]. The incidence is 30% higher in men than in women [8]. Additionally, 20% of soccer players will experience a hamstring injury during their career, with a 20% recurrence rate [9]. Recurrence is often due to inadequate recovery or shortened rehabilitation periods [10], leading to more severe re-injuries and prolonged loss of functionality [11,12]. Injuries occurring in the dominant leg have a greater effect on muscle volume [13]. However, no strength asymmetries have been found in soccer players between the dominant leg and the non-dominant leg in knee flexion–extension movements [14].
Most cases of hamstring injuries are non-contact injuries [7], occurring in the last swing phase during high-speed running, with the knee close to full extension [5,9] when the hamstring must contract very rapidly (<250 ms) to decelerate the inertia [15]. We know that 80% of hamstring injuries occur in the biceps femoris, specifically in their long portion [9], possibly due to structural factors, and kinematic factors of running [16].
There are several non-modifiable risk factors that may increase the risk of hamstring injury: previous anterior cruciate ligament or hamstring injuries, age, weight, gender or race [17] and a previous hamstring injury [18,19]. Other modifiable risk factors include a deficit in hamstring or quadriceps muscle strength [4,19], decreased hamstring flexibility [20,21], gluteal muscle inhibition [22,23], increased biceps femoris/semitendinosus muscle activation ratio [24], muscle fatigue [25], and decreased hamstring/quadriceps (H/Q) strength ratio below 0.47 [26]. However, some authors state that these data only predict 2.7% of injuries [27]. Brockett et al. [28] found that the angle at which the maximum peak strength of the hamstring musculature was produced can be a predictive factor of hamstring injuries. Notably, the maximum peak strength of the hamstring musculature is optimal the closer it is to 0° of knee flexion [29]. Considering that the hamstring musculature reaches its maximum peak strength at approximately 30° of knee flexion (in healthy subjects) [28], hamstring injuries almost always occur with the knee in extension [9], the current measurement of the H/Q strength ratio may not be entirely accurate in predicting hamstring injuries, and these tests should be performed under more game-like circumstances [3].
In the measurement of knee strength, the angle where maximum torque occurs is not the same for quadriceps (≈70° concentric) as for hamstrings (≈60° concentric and ≈30° eccentric) as shown in the study by Small et al. [30]. The maximum torque depends, in part, on the lever arm, depending on the muscle length that varies depending on the joint range. In the anterior and posterior thigh muscles, the H/Q ratio may be reduced in clinical relevance for this reason [31] because when quantified at different joint angles, they cannot determine the co-contraction capacity of these muscles [32]. To solve this problem, measurements of the H/Q ratio can be made at specific knee flexion angles to improve athlete evaluation data specificity and sensitivity. Studying these new H/Q ratios with an emphasis on angles close to knee extension, where most hamstring injuries occur, can help reduce the total number injuries since specific strength protocols can be performed at knee angles where deficits have been found [31] since it has been seen that strength training at specific angles improves strength at that angle [30].
Therefore, the present study evaluated different H/Q ratios in male soccer players at various knee flexion angles and analyzed differences with the conventional ratio that could be used to improve the prediction of hamstring injuries.
2. Materials and Methods
2.1. Experimental Design
A quantitative cross-sectional study was conducted where biomechanical strength tests were performed. Subsequently, the differences between the conventional isokinetic concentric H/Q strength ratio (at 60°/s and 180°/s) and isokinetic concentric H/Q strength ratio at five different knee flexion–extension angles (15°, 30°, 45°, 60°, and 75° of knee flexion) were analyzed.
Informed consent was obtained prior to the measurements for the analysis of the data for research purposes. The study was based on the ethical principles for medical research on human beings, which were declared in the Declaration of Helsinki in 1964 and the last update in Brazil in 2013. Also, in relation to the use of databases, the principles of the Taipei Declaration were considered. At all stages of the research, the respect and protection of personal data were guaranteed in accordance with the provisions of the Organic Law 3/2018.
The study was approved by the Clinical Research Ethics Committee of the Hospital Clínico San Carlos of Madrid, Spain, with approval number C.P.-C.I. 15/416-E.
The isokinetic strength measurement tests were performed in the biomechanics laboratory of the San Juan de Dios School of Nursing and Physiotherapy, of the Comillas Pontifical University. Upon arrival at the laboratory, data were collected on weight and height [with which the body mass index (BMI) was subsequently calculated], age, dominance and playing position.
2.2. Subjects
Twenty-four healthy Spanish third-division male soccer players who were 21 ± 2 years old with a BMI of 22.06 ± 1.26 were evaluated. Subjects who had suffered knee and/or muscle (quadriceps and/or ischiocrural) injuries in the last 6 months were excluded.
A sample size calculation was performed by observing means with respect to a reference. An alpha risk of 0.05 and a beta risk of 0.2 were chosen. For the standard deviation and the minimum difference to be detected (10% of the mean), the variable measured in the study by Risberg et al. [33], maximum knee flexion strength in the dominant leg of soccer players [87.4 (13.6) Nm], was used. Ten percent was added for possible losses, and the final sample calculation resulted in n = 22.
2.3. Measurements
A PRIMUS RS dynamometer from BTE Technologies (Hanover, MD, USA) was used to perform the measurements. Participants were placed in a seated position with their hip flexed at 90°. Thigh straps were placed on the thigh to avoid hip offsets. It did not stabilize the trunk with more straps. The dynamometer shaft was correctly aligned with the femoral condyle. The pad was placed with a 30 cm lever arm in all subjects. Measurements were performed at two different angular velocities: at 60°/s, three flexion–extension repetitions were performed, and at 180°/s, five repetitions were performed. Before taking the measurements, a warm-up of 10 submaximal repetitions at 180°/s was performed to become familiar with the device. A 2-min rest was allowed between each measurement. In each test, the knee joint range varied from 100° knee flexion to 0° (full extension).
2.4. Statistical Analysis
The value of the conventional H/Q ratio was calculated by dividing the maximum peak concentric strength, in Newton, of the ischiocrural musculature by the maximum peak strength of the quadriceps musculature at each measurement. The ratios at the different knee flexion angles were calculated by dividing the strength exerted by the ischiocrural musculature by the strength exerted by the quadriceps musculature at each angle (15°, 30°, 45°, 60°, and 75° of knee flexion) at isokinetic speed (Appendix A (Table A1)).
Statistical analysis was performed using SPSS® Version 23 (IBM Corp., Armonk, NY, USA). As the sample was smaller than 30 subjects, the results were shown according to the median and interquartile range (Q1–Q3) using the highest value of each measurement. The Friedmann nonparametric test was used to analyze whether there were significant differences between the H/Q ratios measured (conventional and at established knee flexion angles). Post hoc test used was Bonferroni. The statistical test was performed for both velocities (60°/s and 180°/s). All statistical analyses used a significance level p > 0.05. To assess the degree of agreement among the different conditions, Kendall’s W (coefficient of concordance) was used. Kendall’s W ranges from 0 to 1, where W = 0 indicates no agreement among raters, while W = 1 represents perfect agreement. Values between 0.1 and 0.3 indicate weak agreement, between 0.3 and 0.5 indicate moderate agreement, and values greater than or equal to 0.5 suggest strong agreement. Kendall’s W was used to determine the consistency of the rankings across the different experimental conditions. Subsequently, for the different data pairs where significant differences were found, the Wilcoxon effect size (Wilcoxon’s r) was based on Cohen’s classification: values between 0.1 and 0.3 indicate a small effect, between 0.3 and 0.5 indicate a moderate effect, and values greater than or equal to 0.5 represent a large effect.
3. Results
In a seated position (with 90° of hip flexion), the H/Q ratio at 60°/s decreases as knee flexion increases (p < 0.001 and W = 0.594 (strong)). At 15° and 30° of knee flexion, higher H/Q ratios are observed [1.03 (0.88–1.21) and 0.83 (0.7–0.87)] but without significant differences between both angles (p = 0.105) compared to ratios obtained at 45° knee flexion [0.63 (0.55–0.77)], 60° knee flexion [0.53 (0.48–0.61)], and 75° knee flexion [0.47 (0.43–0.62)] (p < 0.05 and Wilcoxon’s r > 0.5 in all cases (large effect)) in all cases. As for the conventional H/Q ratio of 0.6 (0.54–0.65), significant differences were found between this and the H/Q ratio at 15° and 30° knee flexion (p < 0.001 and Wilcoxon’s r > 0.5 (large effect)) in both cases; Table 1 and Figure 1).

Table 1.
H/Q ratios at 60°/s at different degrees of knee flexion (15°, 30°, 45°, 60°, and 75°) and conventional isokinetic H/Q strength ratio.
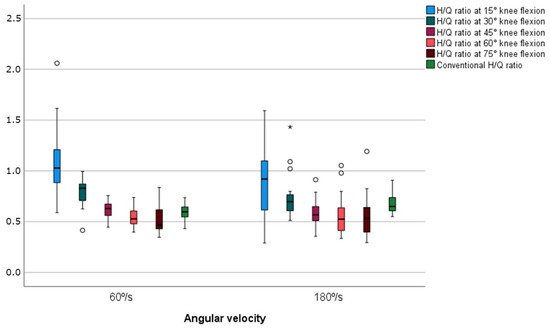
Figure 1.
H/Q ratios measured at 60°/s and 180°/s in a sitting position. The asterisk (*) represent extreme outliers, while circles (o) indicate mild outliers.
Similarly, at 180°/s, the H/Q ratios decreased as the knee flexed. At 15° and 30° of knee flexion, higher H/Q ratios were observed [0.91 (0.6–1.11) and 0.7 (0.6–0.77)] without significant differences (p = 0.226) comparatively to the ratios obtained at 45° knee flexion [0.57 (0.51–0.65)], at 60° knee flexion [0.52 (0.41–0.64)], and at 75° knee flexion [0.53 (0.39–0.64)] (p < 0.05 and Wilcoxon’s r > 0,5 (large effect) in all cases) As for the conventional H/Q ratio [0.65 (0.6–0.74)], significant differences were found between this and the H/Q ratio at 15°, 45°, 60°, and 75° knee flexion (p < 0.05 and Wilcoxon’s r > 0.5 (large effect in all cases; Table 2 and Figure 1).
Table 2.
H/Q ratios at 180°/s at different degrees of knee flexion (15°, 30°, 45°, 60°, and 75°) and conventional isokinetic H/Q strength ratio.
4. Discussion
The relationship between isokinetic concentric strength at 60°/s and 180°/s of the hamstring and quadriceps musculature (ratio) at different knee flexion angles was studied. The results obtained in our study indicate that at low angular velocities in isokinetic tests (60°/s), in addition to the conventional H/Q ratio, the H/Q ratios at 15° and 30° knee flexion should be considered since they are unique and provide more information on the athlete’s muscular state.
Our results align well with those obtained by Figoni et al. [34]. Although the hip flexion was slightly higher (120°) and the measured velocities were different (15°/s and 90°/s) than in Figoni et al.’s [34] study, the relationships found in terms of the calculated ratios were similar to ours. The H/Q ratios at 15°/s decreased as the knee flexed. At 15° and 30° of knee flexion, higher H/Q ratios were observed (2.00 (0.37) and 1.43 (0.33)) than the ratios obtained with higher knee flexion angles (0.89 (0.19) and 0.50 (0.11)) and comparatively with the conventional ratio obtained (0.70 (0.13)). The same occurred at 90°/s, with 15° and 30° of knee flexion; higher H/Q ratios were observed (1.24 (0.32) and 0.90 (0.20)) than the ratios obtained with greater knee flexion angles (0.75 (0.18) and 0.65 (0.13)) and the conventional ratio (0.66 (0.11)). The results may improve for the hamstring injuries risk assessment because evaluating H/Q ratios at 15° and 30° of knee flexion, where hamstring injuries are more likely to occur, provides a more accurate assessment of muscle imbalances than the conventional ratio.
Some authors claim that strength ratios measured with a dynamometer can predict the risk of hamstring injury, and others claim the opposite [26]. In the systematic review by Baroni et al. [35], the mean values of the conventional H/Q ratios of soccer players at different angular velocities measured with the participant seated (hip with 90° of flexion) were established. In the conventional H/Q ratio at 60°/s, the values were 0.65 ± 0.12 and at 180°/s 0.67 (0.17), results similar to those obtained in our study (0.59 (0.08) and 0.67 (0.09), respectively).
The cut-off point of the conventional H/Q ratio (below these values, we can consider the risk of muscle rupture) is 0.47 [26]. In contrast to the above, Dauty et al. [27] mentioned that these data should not be taken as the only reference for predicting hamstring injury since, in their study, only 2.7% of the injured players were below these values. In relation to the above, Grygorowicz et al. [36] determined that, regarding the conventional ratio, taking a value of 0.658 as a cut-off point has greater sensitivity (and therefore fewer false negatives) than a value of 0.47. However, taking 0.47 as the cut-off point has a higher specificity than taking a value of 0.658 (therefore, there will be fewer false positives), so it is difficult to determine what cut-off point to set.
When interpreting the strength values of the hamstring musculature and the H/Q ratio, it is necessary to take into account the level at which the athlete we are evaluating competes, since it has been indicated that second-division soccer players have a lower concentric hamstring strength peak (measured at 60°/s) than first-division soccer players and, therefore, a lower conventional H/Q ratio at 60°/s (0.59 (0.1) versus 0.62 (0.1)) [33]. In the present study, third-division players were measured whose mean conventional H/Q ratio at 60°/s resembles second-division players.
Dauty et al. [26] stated that with the strength values obtained using the dynamometer, more than one-third of hamstring injuries could be reduced. The results of their study concluded that hamstring injuries can be predicted 36.9% of the time if the concentric H/Q ratio at 180°/s is less than 0.47. They also state that if the concentric hamstring strength at 60°/s is 15% lower than the contralateral side, injury can be prevented 34% of the time. Additionally, Bourne et al. [9] reported that one-third of hamstring injuries could be reduced by finding muscle imbalances between the hamstring and quadriceps musculature.
Isokinetic knee dynamometric assessment in soccer players is usually performed in a seated position [37], but in the studies of Guex et al. [16] and Kellis et al. [37], the conventional H/Q ratio was found to be different according to the hip position. It seems interesting, beyond the conventional H/Q ratio, to analyze in detail the strength graph of the hamstring and quadriceps muscles to obtain ratios at different angles for predicting more injuries, as shown with hand grip strength [38].
It will be necessary to continue this line of research by relating the H/Q ratios at 15° and 30° knee flexion with future muscle injuries, establishing new cut-off points for predicting injuries with greater accuracy and reducing the incidence of hamstring injuries.
5. Conclusions
Ischiocrural muscle injuries are increasing annually, and while the conventional H/Q ratio is used for prevention, its utility remains controversial due to the lack of consensus on cut-off points. Our study suggests that H/Q ratios at 15° and 30° of knee flexion differ from the conventional ratio. Since these injuries frequently occur near full extension, incorporating these specific measurements into prediction protocols could be considered for future research.
6. Limitations and Future Lines of Research
This study included only male third-division soccer players, which limits its applicability to female athletes or higher-level professionals.
As this is an observational study, future research will need to be conducted to correlate these data with the injuries that occur.
Author Contributions
Conceptualization, R.C.M. and N.P.M.; methodology, R.C.M.; software, R.C.M.; validation, R.C.M., N.P.M. and M.J.M.B.; formal analysis, M.J.M.B.; investigation, R.C.M., N.P.M., M.J.M.B., L.C.M. and I.R.A.; resources, L.C.M. and M.J.M.B.; data curation, R.C.M. and M.J.M.B.; writing—original draft preparation, R.C.M., N.P.M. and I.R.A.; writing—review and editing, L.C.M. visualization, R.C.M., N.P.M., M.J.M.B., L.C.M. and I.R.A.; supervision, N.P.M.; project administration, R.C.M.; funding acquisition, L.C.M. and M.J.M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of the Hospital Clínico San Carlos of Madrid (C.P.-C.I. 15/416-E approved on 15 September 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Table A1.
Flexion strength, extension strength, and H/Q ratios at 60°/s and 180°/s at different degrees of knee flexion (15°, 30°, 45°, 60°, and 75°) and the maximum strength and conventional isokinetic H/Q strength ratio.
Table A1.
Flexion strength, extension strength, and H/Q ratios at 60°/s and 180°/s at different degrees of knee flexion (15°, 30°, 45°, 60°, and 75°) and the maximum strength and conventional isokinetic H/Q strength ratio.
| 60°/s Flexion Median (Q1–Q3) 2 | 60°/s Extension Median (Q1–Q3) | 60°/s H/Q Ratio 1 Median (Q1–Q3) | 180°/s Flexion Median (Q1–Q3) | 180°/s Extension Median (Q1–Q3) | 180°/s H/Q Ratio Median (Q1–Q3) | |
|---|---|---|---|---|---|---|
| 15° | 69.98 (48.58–88.72) | 63.98 (55.29–76.66) | 1.03 (0.88–1.21) | 55.81 (36.91–86.94) | 67.06 (53.89–85.95) | 0.91 (0.6–1.11) |
| 30° | 81.82 (72.82–91.31) | 95.17 (86.99–116.95) | 0.83 (0.7–0.87) | 63.28 (48.64–81.38) | 96.95 (71.16–115.27) | 0.7 (0.6–0.77) |
| 45° | 79.32 (74.36–94.19) | 127.26 (116.34–157.71) | 0.63 (0.55–0.77) | 64.04 (43.19–79.54) | 111.81 (79.24–134.78) | 0.57 (0.51–0.65) |
| 60° | 76.86 (68.98–90.11) | 149.13 (131.74–168.78) | 0.53 (0.48–0.61) | 56.94 (46.05–69.41) | 115.73 (88.21–132.7) | 0.52 (0.41–0.64) |
| 75° | 64.51 (58.03–74.44) | 141.16 (107.11–162.51) | 0.47 (0.43–0.62) | 44.44 (36.97–55.86) | 97.68 (72.56–116.37) | 0.53 (0.39–0.64) |
| Maximum | 96.10 (80.05–108.73) | 165.38 (149.19–177.24) | 0.6 (0.54–0.65) | 79.34 (65.98–99.12) | 124.43 (92.87–148.26) | 0.65 (0.6–0.74) |
1 The H/Q ratio at 60°/s and 180°/s was calculated by dividing the maximum hamstring strength value of the repetitions performed (measured in Newtons) by the maximum quadricep strength value of the repetitions performed. 2 Q1 is the first quartile data, and Q3 is the third quartile data.
References
- Jones, A.; Jones, G.; Greig, N.; Bower, P.; Brown, J.; Hind, K.; Francis, P. Epidemiology of injury in English Professional Football players: A cohort study. Phys. Ther. Sport 2019, 35, 18–22. [Google Scholar] [CrossRef]
- Eirale, C. Hamstring injuries are increasing in men’s professional football: Every cloud has a silver lining? Br. J. Sports Med. 2018, 52, 1489. [Google Scholar] [CrossRef]
- Grazioli, R.; Lopez, P.; Andersen, L.L.; Machado, C.L.F.; Pinto, M.D.; Cadore, E.L.; Pinto, R.S. Hamstring rate of torque development is more affected than maximal voluntary contraction after a professional soccer match. Eur. J. Sport Sci. 2019, 19, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; López-Valenciano, A.; Gámez Martín, J.A.; De Ste Croix, M.; Vera-Garcia, F.J.; García-Vaquero, M.D.P.; Ruiz-Pérez, I.; Myer, G.D. A preventive model for hamstring injuries in professional soccer: Learning algorithms. Int. J. Sports Med. 2019, 40, 344–353. [Google Scholar] [CrossRef]
- Lee, J.W.Y.; Mok, K.; Chan, H.C.K.; Yung, P.S.H.; Chan, K. Eccentric hamstring strength deficit and poor hamstring-to-quadriceps ratio are risk factors for hamstring strain injury in football: A prospective study of 146 professional players. J. Sci. Med. Sport 2018, 21, 789–793. [Google Scholar] [CrossRef]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef]
- Cross, K.M.; Gurka, K.K.; Saliba, S.; Conaway, M.; Hertel, J. Comparison of thigh muscle strain occurrence and injury patterns between male and female high school soccer athletes. J. Sport Rehabil. 2018, 27, 451–459. [Google Scholar] [CrossRef]
- Larruskain, J.; Lekue, J.A.; Diaz, N.; Odriozola, A.; Gil, S.M. A comparison of injuries in elite male and female football players: A five-season prospective study. Scand. J. Med. Sci. Sports 2018, 28, 237–245. [Google Scholar] [CrossRef]
- Bourne, M.N.; Timmins, R.G.; Opar, D.A.; Pizzari, T.; Ruddy, J.D.; Sims, C.; Williams, M.D.; Shield, A.J. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2018, 48, 251–267. [Google Scholar] [CrossRef]
- Maniar, N.; Shield, A.J.; Williams, M.D.; Timmins, R.G.; Opar, D.A. Hamstring strength and flexibility after hamstring strain injury: A systematic review and meta-analysis. Br. J. Sports Med. 2016, 50, 909–920. [Google Scholar] [CrossRef]
- Green, B.; Bourne, M.N.; Pizzari, T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: A systematic review and meta-analysis. Br. J. Sports Med. 2008, 52, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Hickey, J.T.; Timmins, R.G.; Maniar, N.; Rio, E.; Hickey, P.F.; Pitcher, C.A.; Williams, M.D.; Opar, D.A. Pain-free versus pain-threshold rehabilitation following acute hamstring strain injury: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2020, 50, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Svensson, K.; Eckerman, M.; Alricsson, M.; Magounakis, T.; Werner, S. Muscle injuries of the dominant or non-dominant leg in male football players at elite level. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 933–937. [Google Scholar] [CrossRef] [PubMed]
- DeLang, M.D.; Rouissi, M.; Bragazzi, N.L.; Chamari, K.; Salamh, P.A. Soccer footedness and between-limbs muscle strength: Systematic review and meta-analysis. Int. J. Sport Physiol. Perform. 2019, 14, 551–562. [Google Scholar] [CrossRef]
- Correia, P.; Santos, P.; Mil-Homens, P.; Gomes, M.; Dias, A.; Valamatos, M.J. Rapid hamstrings to quadriceps ratio at long muscle lengths in professional football players with previous hamstring strain injury. Eur. J. Sport Sci. 2020, 20, 1405–1413. [Google Scholar] [CrossRef]
- Guex, K.; Gojanovic, B.; Millet, G.P. Influence of hip-flexion angle on hamstrings isokinetic activity in sprinters. J. Athl. Train. 2012, 47, 390–395. [Google Scholar] [CrossRef]
- Orchard, J.W.; Chaker Jomaa, M.; Orchard, J.J.; Rae, K.; Hoffman, D.T.; Reddin, T.; Driscoll, T. Fifteen-week window for recurrent muscle strains in football: A prospective cohort of 3600 muscle strains over 23 years in professional Australian rules football. Br. J. Sports Med. 2020, 54, 1103–1107. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury recurrence is lower at the highest professional football level than at national and amateur levels: Does sports medicine and sports physiotherapy deliver? Br. J. Sports Med. 2016, 50, 751–758. [Google Scholar] [CrossRef]
- Roe, M.; Delahunt, E.; McHugh, M.; Gissane, C.; Malone, S.; Collins, K.; Blake, C. Association between eccentric knee flexor strength and hamstring injury risk in 185 elite Gaelic football players. Scand. J. Med. Sci. Sports 2020, 30, 515–522. [Google Scholar] [CrossRef]
- Chen, C.H.; Xin, Y.; Lee, K.W.; Lin, M.J.; Lin, J.J. Acute effects of different dynamic exercises on hamstring strain risk factors. PLoS ONE 2018, 13, e0191801. [Google Scholar] [CrossRef]
- Dallinga, J.M.; Benjaminse, A.; Lemmink, K.A.P.M. Which screening tools can predict injury to the lower extremities in team sports? A systematic review. Sports Med. 2012, 42, 791–815. [Google Scholar] [CrossRef] [PubMed]
- Schuermans, J.; Danneels, L.; Van Tiggelen, D.; Palmans, T.; Witvrouw, E. Proximal neuromuscular control protects against hamstring injuries in male soccer players: A prospective study with electromyography time-series analysis during maximal sprinting. Am. J. Sports Med. 2017, 45, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Schuermans, J.; Van Tiggelen, D.; Palmans, T.; Danneels, L.; Witvrouw, E. Deviating running kinematics and hamstring injury susceptibility in male soccer players: Cause or consequence? Gait Posture 2017, 57, 270–277. [Google Scholar] [CrossRef]
- Schuermans, J.; Van Tiggelen, D.; Danneels, L.; Witvrouw, E. Susceptibility to hamstring injuries in soccer: A prospective study using muscle functional magnetic resonance imaging. Am. J. Sports Med. 2016, 44, 1276–1285. [Google Scholar] [CrossRef]
- de Hoyo, M.; Naranjo Orellana, J.; Carrasco Páez, L.; Sanudo, B.; Jiménez-Barroca, J.J.; Domínguez-Cobo, S. Revisión sobre la lesión de la musculatura isquiotibial en el deporte: Factores de riesgo y estrategias para su prevención. Rev. Andal. Med. Deporte 2013, 6, 30–37. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Fouasson-Chailloux, A.; Ferréol, S.; Dubois, C. Prediction of hamstring injury in professional soccer players by isokinetic measurements. Muscles Ligaments Tendons J. 2016, 6, 116–123. [Google Scholar] [CrossRef]
- Dauty, M.; Menu, P.; Fouasson-Chailloux, A. Cutoffs of isokinetic strength ratio and hamstring strain prediction in professional soccer players. Scand. J. Med. Sci. Sport 2018, 28, 276–281. [Google Scholar] [CrossRef]
- Brockett, C.L.; Morgan, D.L.; Proske, U. Predicting hamstring strain injury in elite athletes. Med. Sci. Sports Exerc. 2004, 36, 379–387. [Google Scholar] [CrossRef]
- Guex, K.J.; Lugrin, V.; Borloz, S.; Millet, G.P. Influence on strength and flexibility of a swing phase-specific hamstring eccentric program in sprinters’ general preparation. J. Strength Cond. Res. 2016, 30, 525–532. [Google Scholar] [CrossRef]
- Small, K.; McNaughton, L.; Greig, M.; Lovell, R. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J. Sci. Med. Sport 2010, 13, 120–125. [Google Scholar] [CrossRef]
- Eustace, S.J.; Morris, R.; Tallis, J.; Page, R.M.; Greig, M. The influence of angle-specific torque of the knee flexors and extensors on the angle-specific dynamic control ratio in professional female soccer players. J. Sports Sci. 2022, 40, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Eustace, S.J.; Page, R.M.; Greig, M. Isokinetic strength differences between elite senior and youth female soccer players identifies training requirements. Phys. Ther. Sport 2019, 39, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Risberg, M.A.; Steffen, K.; Nilstad, A.; Myklebust, G.; Kristianslund, E.; Moltubakk, M.M.; Krosshaug, T. Normative quadriceps and hamstring muscle strength values for female, healthy, elite handball and football players. J. Strength Cond. Res. 2018, 32, 2314–2323. [Google Scholar] [CrossRef]
- Figoni, S.F.; Christ, C.B.; Massey, B.H. Effects of speed, hip and knee angle, and gravity-on hamstring to quadriceps torque ratios. J. Orthop. Sports Phys. Ther. 1998, 9, 287–291. [Google Scholar] [CrossRef][Green Version]
- Baroni, B.M.; Ruas, C.V.; Ribeiro-Alvares, J.B.; Pinto, R.S. Hamstring-to-quadriceps torque ratios of professional male soccer players: A systematic review. J. Strength Cond. Res. 2020, 34, 281–293. [Google Scholar] [CrossRef]
- Grygorowicz, M.; Michałowska, M.; Walczak, T.; Owen, A.; Grabski, J.K.; Pyda, A.; Piontek, T.; Kotwicki, T. Discussion about different cut-off values of conventional hamstring-to-quadriceps ratio used in hamstring injury prediction among professional male football players. PLoS ONE 2017, 12, e0188974. [Google Scholar] [CrossRef]
- Kellis, E.; Ellinoudis, A.; Kofotolis, N. Effect of hip flexion angle on the hamstring to quadriceps strength ratio. Sports 2019, 7, 43. [Google Scholar] [CrossRef]
- Oteo, J.A.; Benavente, P.; Garzón, M. Securities regulatory force fist in Spanish working age population. Anthropometric influence of variables of the hand and forearm. Rev. Iberoam. Cirugía Mano 2015, 43, 104–110. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).