Abstract
Splinting of the mobile teeth is a critical part of periodontal management to improve the prognosis and longevity of stable results of periodontally compromised teeth with increased mobility. Different types of splints are used in the dental field based on their mechanical and physical properties.The objective of the current in vitro study was to evaluate the flexure strength and flexural modulus of different types of splinting materials, such as: composite block, ligature wire, Ribbond®, InFibra®, and F-splint-Aid® bonded utilizing Flowable composites resin material. Seventy-five bar specimens were prepared with the dimensions of 25 × 4 × 2 mm, utilizing split metallic mold. Specimens were divided equally (n = 15) into five groups (one control group, four test groups). Different layers of splinting material were placed in between the layers of composite before curing. All the specimens were subjected to a three-point bending test by using a universal testing machine to calculate the flexural strength and flexural modulus. The entire data was subjected to statistical tests to evaluate the significance. Specimens from composite block groups showed the least mean value for flexural strength (89.15 ± 9.70 MPa) and flexural modulus (4.310 ± 0.912 GPa). Whereas, the highest mean value for flexural strength (168.04 ± 45.95 MPa) and flexural modulus (5.861 ± 0.501 GPa) were recorded by Ribbond® specimens. Inter group comparison of flexural strength showed statistically significant differences (P-value < 0.05), whereas comparison of flexural modulus showed non-significant difference among the groups (P-value > 0.05). Within the limitation of the present study, it was concluded that the Ribbond® exhibits maximum flexural strength and flexural modulus, whereas the composite blocks recorded the least values. Still, the decision making depends on the clinical scenario and the unique characteristic of each splint material.
1. Introduction
Patient satisfaction and improvement of oral health is considered as a major part of patient well-being during rehabilitation [1]. Tooth mobility is one of the most frequently encountered problems in the population which experience periodontal and periapical disease. Splinting has been advocated after repositioning of tooth/teeth to stabilize the tooth/teeth and to optimize healing outcomes, by allowing transmission of functional forces to support PDL regeneration [2,3]. The splint, as described by the glossary of prosthodontic terms, is a device that retains hard and/or soft tissue in a predetermined position [4]. Dental splint is also defined by Glickman’s as an appliance designed to immobilize the loose or diseased teeth [5]. In the literature, many indications have been listed for tooth splinting, such as; to secure teeth that were orthodontically moved, to stabilized avulsed and luxated tooth, and to fix teeth that are periodontally compromised [6,7]. Even regular physiologic functions, such as chewing and swallowing, are recognized to be affected by tooth mobility. Periodontal splinting is utilized to offer long-term retention of teeth, and when used correctly can greatly improve the comfort, prognosis, and outcome of therapy for a patient with severe periodontal diseases [8,9]. On the other hand, the decision related to dental splinting requires a thorough examination and multidisciplinary approach; not all teeth can be splinted, therefore an accurate diagnosis is essential [6].
Literature from the past revealed that the foremost signs for periodontal disease are occlusal problems, progressive mobility, and migration of teeth because of periodontal or periapical derangement [10]. Splinting of affected teeth is an option to improve the patients’ comfort and to provide better control of occlusion. Furthermore, splinting often preserves patients from tooth extraction and complex and costly prosthesis or implants [11]. However, especially in cases of severe horizontal bone loss and increased mobility, the decision of whether to preserve or extract the affected teeth is a challenging one. This decision should always be made on an individual level, taking into consideration the general factors of the patient and their expectations of the treatment [11]. Splinting is classified by Weisgold as a temporary method which is used over a short time for less than six months, provisional or semi-permanent which is used for a few months to several years for diagnostic purposes, and a permanent splint which is worn indefinitely [12].
Different types of splint materials are used in dentistry based on their flexibility to allow movement of dental structures. Splinting materials such as orthodontic wire, button slint, and fiber reinforced composite are attached to the teeth with the help of dental composites. Composite resin splints have been used for a long time due to advantages like ease in the construction, esthetically pleasant reduced cost, and ease of cleaning [13,14]. Elastic splint materials are oftentimes preferred, as they allow flexible instead of rigid splinting. In contrast to elastic, hard splinting materials reduce the physiologic mobility of teeth, and thus might eliminate bone remodeling stimulation in a previously jeopardized periodontium [15].
The modulus of elasticity is an indicator of the material hardness and illustrates a positive association between the modulus of elasticity and substance rigidity. Rigid splints are more probably made from materials possessing higher modulus of elasticity, for example, composite resin material. Additional quality is the flexure strength specifically is also termed as modulus of rupture, or transverse rupture strength is a physical feature [16]. The flexural strength represents the highest stress experienced within the material at its moment of yield. It is measured in terms of stress. Incidence of ankylosis may increase following improper selection of material or duration of splinting. Thus, the international association of dental traumatology (IADT) guiding principle recommends that splinting material should be flexible, somewhat rigid, and used for a short duration of time [6].
In the literature, some research exist, considerable to physical and mechanical qualities particularly flexural strength and modulus of elasticity of numerous splinting substances. To the best of our knowledge, no published data has been reported in the literature which compared the mechanical properties of splint materials as; F-splint-Aid®,Ribbond®, InFibra®, Ligature wire with composite. Thus, the goal of the current in vitro study is to assess the two physical properties, modulus of elasticity, and flexure strength of unlike splint materials bonded utilizing composites resin material.
2. Materials and Methods
The study protocol was prepared and presented to the institutional ethical review committee before obtaining ethical clearance. Detailed descriptions of the materials used in the experiment are given in Table 1.

Table 1.
Materials and their manufacturers.
Seventy-five bar specimens were prepared with the dimensions of 25 × 4 × 2 mm according to ISO specification 4049/2009. Test methods were followed according to the (American Society for Testing and Materials) ASTM D790 standards. Split metallic mold was used to prepare the uniform dimension of the specimen (Figure 1). Flowable composite resin was placed into the mold with an incremental pattern. According to the experimental groups, a different layer of splinting material was placed between the layers of composite. The specimens were polymerized by Bluephase™ unit (Ivoclar Vivadent, Schaan, Liechtenstein) equipment with 10 mm light probe, using light intensity of 1200 mW/cm2 with halogen like broadband spectrum ranging from 385–515 nm for 20 s.
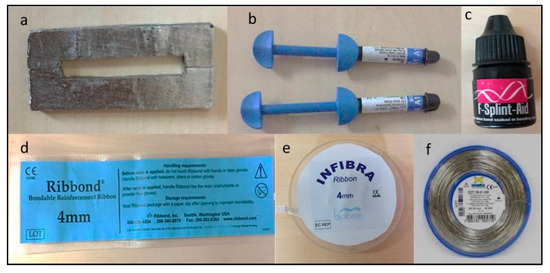
Figure 1.
Experimental materials: (a) Metallic mold, (b) Flowable composite resin syringes, (c) F-splint-Aid®, (d) Ribbond®, (e) InFibra®, (f) Morelli® Ligature wire.
Specimens were divided equally (n = 15) into five groups (one control group, four test groups) depending on the type of splint material used:
- Group 1 (control): composite block without splinting material
- Group 2 (test): composite with F-splint-Aid®
- Group 3 (test): composite with ligature wire
- Group 4 (test): composite with InFibra®
- Group 5 (test): composite with Ribbond®
The specimens were stored at 37 °C in distilled water for 24 h before being subjecting to the experimental testing. All the specimens were subjected to three-point bending test by using a Universal testing machine which was attached to a software programmed computer (ACME Engineers, India. Model No. UNITEST-10, Accuracy of the machine: ±1%) (Figure 2).
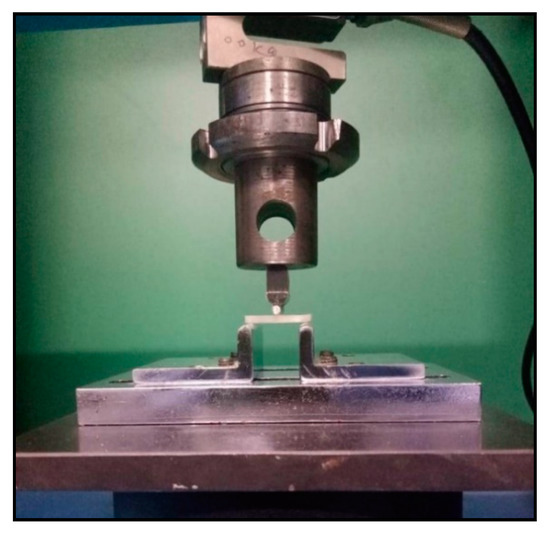
Figure 2.
Specimen attached to universal testing machine for three point bending test.
During the experimental period, the crosshead speed was adjusted to 1 mm/minute and the distance between support was 20 mm. The maximum load applied during the testing was reported in Newtons (N), whereas flexural strength and flexural modulus was recorded in megapascal (MPa) and gigapascal (GPa), respectively, for each group (Figure 3). Mean and standard deviations were calculated for each variable of all the groups. Flexural modulus was calculated by the software using the following formula [17];
where, (F/D) is the slope in Newton per mm measured in the straight line portion of the load deflection curve. F = Max loaf in Newton. D = Deflection. L = Distance between supports. B = Width of specimens. H = Height of specimens.
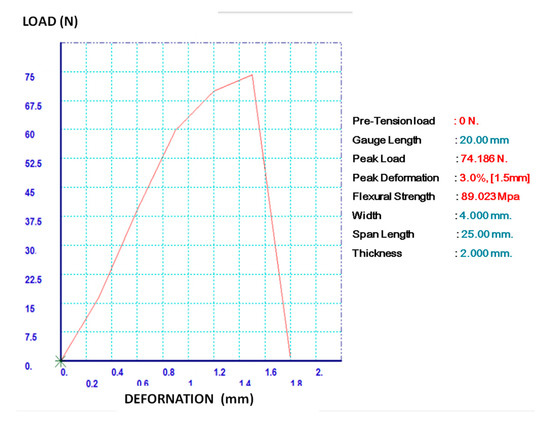
Figure 3.
Load deformation graph while conducting the experiment.
The statistical significance of inter-group difference in the distribution of mean flexural strength and modulus was tested using one-way analysis of variance (ANOVA) with post-Hoc Bonferroni’s test for multiple group comparisons. The underlying normality assumption was tested before subjecting the study variables to ANOVA. The entire data was entered in MS Excel software before statistical analysis. In the entire study, the p-values less than 0.05 were considered to be statistically significant. The entire data was statistically analyzed using statistical package for social sciences (SPSS version 21.0, IBM Corporation, NY; USA).
3. Results
The specimens were subjected to load application until fracture failure. Table 2 showed mean (±SD) value of maximum load (N) application, flexural strength (MPa), and flexural modulus (GPa). Figure 4 and Figure 5 represent inter-group distribution of flexural strength and flexural modulus respectively by using a Box–Whisker Plot. Specimens from Group 1 showed the least mean values for flexural strength (89.15 ± 9.70 MPa) and flexural modulus (4.310 ± 0.912 GPa). Whereas, highest mean values for flexural strength (168.04 ± 45.95 MPa) and flexural modulus (5.861 ± 0.501 GPa) were recorded by group 5 specimens.
Table 2.
Distributions of mean ± standard deviation (SD) maximum load, mean flexural strength, and mean flexural modulus across five study groups.
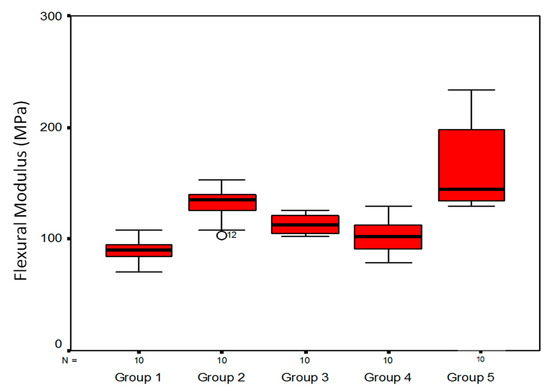
Figure 4.
Inter-group distribution of flexural strength (Box–Whisker Plot).
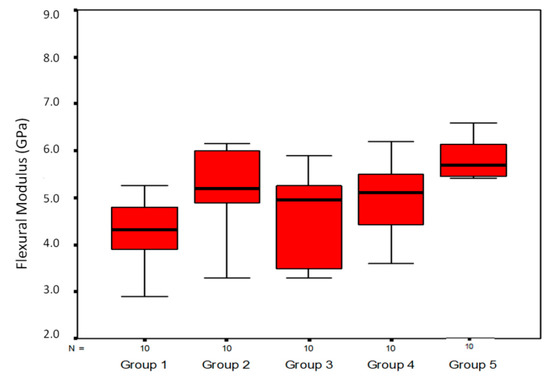
Figure 5.
Inter-group distribution of flexural modulus (Box–Whisker Plot).
Table 3 shows the inter-group statistical comparison of mean flexural strength. The distribution of mean flexural strength is significantly lower in Group 1 compared to Groups 2 and 5 (P-value < 0.01 for both). The distribution of mean flexural strength on Group 2 is significantly higher when compared to Group 4 (P-value < 0.01). The distribution of mean flexural strength is significantly lower in Group 2 as compared to Group 5 (P-value < 0.05). The distribution of mean flexural strength is significantly higher in Group 5 as compared to Groups 3 and 4 (P-value < 0.001 for both). Table 4 shows the inter-group statistical comparison of mean flexural modulus. The distribution of mean flexural modulus did not differ significantly across five study groups (P-value > 0.05 for all).
Table 3.
Inter-group statistical comparison of mean flexural strength.
Table 4.
Inter-group statistical comparison of mean flexural modulus.
4. Discussion
In the past, different approaches for evaluating splint rigidity have been used [18]. One of the advantages of in vivo investigations with patients is the presence of a natural PDL. However, the disadvantages of assessing splint rigidity in healthy individuals include the lack of increased tooth mobility, the risk of damaging sound enamel during splint removal, and the limited availability of test persons [2]. Therefore, in vitro studies using various types of models have also been conducted. The advantage of artificial models is that they are available anytime, the moderate inter-model variability compared to the patient, and the potential for intentional adjustment of tooth mobility. Besides, there is no risk of damaging sound enamel, as can happen in healthy individuals [13,19]. The core objective of the present in vitro study was to assess the flexural strength and flexural modulus of different splint systems used for periodontal splinting. Flexural strength and flexural modulus are vital mechanical properties which were employed in earlier experiments to evaluate and compare the physical properties of the restoration and restorative materials [20,21].
Reports from literature revealed that, in the past, mesh grids, wires and pins were frequently used with the adhesive systems for stabilization and splinting of teeth [22]. These splint materials stay in position just by mechanical locking around the restorative material that could lead to generation of shear planes and stress concentration and ultimately fracture of the composite with premature failure of the splint system. Newer and advanced splint systems, like bondable, polyethylene woven ribbons, have succeeded in overcoming the problems associated with older splint systems. Flexible splints such as the fiber-composite splint and polyethylene fiber used in the present study fulfill these requirements. For evaluating splint rigidity, objective tooth mobility assessment is required. The three-point bending test is a well-established tool used to evaluate flexural strength and flexural modulus in dental traumatology [18,23].
Ribbond® is a leno weave, ultra-high-molecular-weight polyethylene fiber with an ultra-high elastic modulus. The specially designed fiber network permits wetting of the fibers and the infusion of the resin into the fiber network [24]. An in vitro study conducted by Yapp and Powers showed that flexural strength and flexural modulus of Ribbond® was 153 MPa and 4.0 GPa, while in the current study it was 168.04 ± 45.95 and 5.861 ± 0.501 GPa, respectively [25]. In our study, the mean maximum load applied to Ribbond® splint group was 143.06 ± 30.73N. Whereas, contradictory results were reported by Kemaloglu et al. that showed mean fracture resistance of 919.86 ± 47.67 N [26]. While the present study showed that F-splint-Aid has 131.95 ± 16.48 MPa of flexural strength and 5.366 ± 1.042 GPa of flexural modulus, respectively, which is significant less when compared with the study performed by Yapp and Powers [25]. Composite and wire splints are one of the most commonly used splints in dental field and are flexible enough when the wire diameter is not more than 0.3–0.4 mm [27]. In the current research, it was observed that flexural strength and flexural modulus recorded by the wire composite splint are 122.95 ± 8.72 MPa and 4.629 ± 0.962 GPa, respectively. Sekhar et al., in a clinical study, compared the efficacy of Ribbond® ribbon with stainless steel wire [28]. We concluded that Ribbond® was an excellent material for splinting mobile teeth relating to patient comfort, durability, resistance to fracture, biocompatibility, and esthetic acceptability.
The result of the present study showed that the Ribbond® was found to have the highest flexural strength, followed by F-splint-Aid®, ligature wire, InFibra®, and composite block having the least flexural strength. The research carried out by Yapp and Powers in 2011, Gaspar Junior et al. in 2009, and Juloski et al. in 2012 showed that polyethylene fibers are more flexible than glass fibers and stainless steel wire, which is in agreement with the findings in the present study [25,29,30]. The higher flexibility of polyethylene as compared to the glass fiber and composite could be credited to its patented lock stitch pattern that avoids transfer of stress back into the reinforcement resin and distributes them into the weave [31]. Whereas, less flexibility of glass fiber reinforced composite may be because of resin pre-impregnation of the fibers [32]. While comparing flexural modulus, the highest was reported by Ribbond®, with composite with ligature wire having the least value.
The results of a study conducted by Dave Foek et al. in 2013 are in accordance with the results of the current study, which showed that the fiber reinforced ribbon was established to have the maximum flexural strength and flexural modulus, followed by fiber glass and polyethylene fiber [33]. Tina Puthen et al. in 2015 found that the wire-composite group demonstrated significantly lower bond strength compared to fiber glass group, which is similar to the results obtained in the present study [34].
There is some controversy that exists among the researchers on the employment of hand-impregnated versus pre-impregnated fibers in the restorative procedure. In the present study, hand-impregnated polyethylene fiber demonstrated higher flexural strength and flexural modulus as compared to hand-impregnated. The results are in agreement with the results reported by Ellakwa et al. and Gaspar Junior et al., as they found in their studies that hand-impregnated fibers exhibited higher flexural strength values [21,25]. Contrasting results were reported by Goldberg and Burstone in 1998, as they concluded that pre-impregnated fibers exhibit superior flexural strength because of their higher fiber units, attained during manufacturing procedure [35]. Intergroup comparison of mean flexural strength revealed that most of the groups having a statistically significant difference in flexural strength, except between a few groups such as composite block and composite with ligature wire, composite block and InFibra®, composite with ligature wire and InFibra®, composite with ligature wire, and F-splint-Aid®.
The empirical results reported herein should be considered in the light of some limitations. In the present experiment, the flexural strength and flexural modulus were examined under in vitro conditions, the applied load did not imitate the dynamic loading situation in the oral cavity. For long duration in the oral cavity, strain allocation may be exaggerated by viscoelastic and biological bone reactions. Consequently, the results of this study should be measured as an estimation of the early condition after a splint has been positioned [36]. Also, while performing a three-point bend test, stress was applied in one direction, therefore it fails to mimics the actual occlusal condition in many clinically possible loading conditions [30]. Further studies are required with protocol simulating experimental conditions more closely to the oral environment. Tayab et al. claim that in the dental field, both glass fiber and polyethylene-fiber have incredible potential for reinforcement, but decision making depends on the clinician’s understanding of the clinical condition and unique characteristics of each fiber type [37].
5. Conclusions
Current protocols and guidelines have stressed the importance of using flexible splints for the stabilization of traumatized teeth. The result of the present study suggests that the Ribbond® was found to have the highest flexural strength, followed by F-splint-Aid®, ligature wire with composite, InFibra®, and composite block showed the least flexural strength. While comparing flexural modulus, the highest was reported by Ribbond® and the composite blocks revealed the least value.
The results of this study provide clinicians with critical information regarding physical characteristics of the different splints on tooth mobility, thus allowing them to choose the most appropriate splint that will allow physiological movement during stabilization and regeneration of the traumatized periodontium. Within the limitations of this in vitro investigation, authors have recommended Ribbond® as the best material to be implemented in periodontal splinting.
Author Contributions
In the current article individual contributions of the author are as follows: Conceptualization: A.S., A.A., D.G. and S.M.; methodology: A.S., S.M. and N.T.; validation: A.S., N.T. and S.S.; formal analysis: A.S. and D.G.; investigation: A.S., N.T., S.M. and S.S.A.; resources: A.S., N.T., A.A. and N.T.; data curation: A.S., A.A., S.M. and S.S.; writing—original draft preparation: A.S. and D.G.; writing: A.S., A.A., N.T., S.M. and S.S.; supervision: A.S. and A.A.; project administration: A.S.; funding acquisition: A.S. and S.M.
Funding
This research was funded by the Deanship of Scientific Research (project no: 272/1440), King Khalid University, Abha, Saudi Arabia.
Acknowledgments
The authors have nothing to acknowledge.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Durrani, F.; Galohda, A.; Rai, S.K.; Singh, N.K.; Verma, R.; Yadav, D.S.; Karthickraj, S.M. Evaluation and comparison of stress distribution around periodontally compromised mobile teeth splinted with different materials: Three-dimensional finite element analysis. Indian J. Dent. Res. 2019, 30, 97–101. [Google Scholar] [PubMed]
- Hassan, M.W.; Andersson, L.; Lucas, P.W. Stiffness characteristics of splints for fixation of traumatized teeth. Dent. Traumatol. 2016, 32, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Von, A.T.; Filippi, A.; Lussi, A. Comparison of a new dental trauma splint device (TTS] with three commonly used splinting techniques. Dent. Traumatol. 2001, 17, 266–274. [Google Scholar]
- Hamilton, R.S.; Pons, P.T. The efficacy and comfort of full-body vacuum splints for cervical-spine immobilization. J. Emerg. Med. 1996, 14, 553–559. [Google Scholar] [CrossRef]
- Max, J.P. A systematic approach to the interpretation of tooth mobility and its clinical implications. Dent. Clin. N. Am. 1980, 24, 177–193. [Google Scholar]
- Andersson, L.; Andreasen, J.O.; Day, P.; Heithersay, G.; Trope, M.; DiAngelis, A.J.; Kenny, D.J.; Sigurdsson, A.; Bourguignon, C.; Flores, M.T.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2012, 28, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Ikarinen, K. Functional fixation for traumatically luxated teeth. Endod. Dent. Traumatol. 1987, 3, 224–228. [Google Scholar] [CrossRef]
- Mosedale, R.F. Current indications and methods of periodontal splinting. Dent. Update. 2007, 34, 168–180. [Google Scholar] [CrossRef]
- Kathariya, R.; Devanoorkar, A.; Golani, R.; Shetty, N.; Vallakatla, V.; Bhat, M.Y. To splint or not to splint: The current status of periodontal splinting. J. Int. Acad. Periodontol. 2016, 18, 45–56. [Google Scholar]
- Tarnow, D.P.; Fletcher, P. Splinting of periodontally involved teeth: Indications and contraindications. N. Y. State Dent. J. 1986, 52, 24–25. [Google Scholar]
- Sonnenschein, S.K.; Betzler, C.; Rütters, M.A.; Krisam, J.; Saure, D.; Kim, T.S. Long-term stability of splinted anterior mandibular teeth during supportive periodontal therapy. Acta Odontol. Scand. 2017, 75, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Berthold, C.; Auer, F.J.; Potapov, S.; Petschelt, A. Rigidity evaluation of quartz-fiber splints compared with wire-composite splints. Dent. Traumatol. 2012, 28, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Berthold, C.; Thaler, A.; Petschelt, A. Rigidity of commonly used dental trauma splints. Dent. Traumatol. 2009, 25, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Kumbuloglu, O.; Saracoglu, A.; Ozcan, M. Pilot study of unidirectional E-glass fibre-reinforced composite resin splints: Up to 4.5-year clinical follow-up. J. Dent. 2011, 39, 871–887. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Ostermann, F.; Woeste, S.; Sälzer, S.; Dörfer, C.E.; Schwendicke, F. Long-term survival and maintenance efforts of splinted teeth in periodontitis patients. J. Dent. 2019, 80, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ashby, M.F.; Cebon, D. Materials selection in mechanical design. J. Phys. IV 1993, 3, C7-1–C7-9. [Google Scholar] [CrossRef]
- Trevor, B.A. Why choose magnesium? Mater. Sci. Forum 2009, 618, 3–6. [Google Scholar]
- Mazzoleni, S.; Meschia, G.; Cortesi, R.; Bressan, E.; Tomasi, C.; Ferro, R. In vitro comparison of the flexibility of different splint systems used in dental traumatology. Dent. Traumatol. 2010, 26, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Berthold, C.; Holst, S.; Schmitt, J.; Goellner, M.; Petschelt, A. An evaluation of the periotest method as a tool for monitoring tooth mobility in dental traumatology. Dent. Traumatol. 2010, 26, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Narva, K.K.; Lassila, L.V.J.; Vallitu, P.K. Fatigue and stiffness of glass fiber-reinforced urethane dimethacrylate composite. J. Prosthet. Dent. 2004, 91, 158–163. [Google Scholar] [CrossRef]
- Ellakwa, A.E.; Shortall, A.C.; Shehata, M.K.; Marquis, P.M. Influence of bonding agent composition on flexural properties ofan ultra-high molecular weight polyethylene fiber-reinforced composite. Oper. Dent. 2002, 27, 184–191. [Google Scholar] [PubMed]
- Sujeetha, M.; Rajaram, V.; Mahendra, J. Stabilizing teeth with nonsurgical treatment—A report of two splinting cases. Int. J. Recent. Sci. Res. 2018, 9, 27616–27618. [Google Scholar]
- Hoeppner, M.G.; Fonseca, R.B.; Pfau, E.A.; Justo, F.R.; Fávero, A.; Bremm, L.L. Rehabilitation of periodontally compromised teeth with fiber-reinforced composite resin: A case report. Quintessence Int. 2011, 42, 113–120. [Google Scholar] [PubMed]
- Kemaloglu, H.; Pamir, T.; Tezel, H. A 3-year randomized clinical trial evaluating two different bonded posterior restorations: Amalgam versus resin composite. Eur. J. Dent. 2016, 10, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Yapp, R.; Powers, J.M. Flexural Strength and Modulus of Several Splinting Products. Dent. Advisor 2011, 38, 12. [Google Scholar]
- Kemaloglu, H.; Emin, K.M.; Turkun, M.; Micoogullari, K.S. Effect of novel restoration techniques on the fracture resistance of teeth treated endodontically: An in vitro study. Dent. Mater. J. 2015, 34, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Hu, J.Y.; Marriot-Smith, C.S.; Heithersay, G.S. Splinting of teeth following trauma: A review and a new splinting recommendation. Aust. Dent. J. 2016, 61, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Sekhar, L.C.; Koganti, V.P.; Shankar, B.R.; Gopinath, A. A comparative study of temporary splints: Bonded polyethylene fiber reinforcement ribbon and stainless steel wire + composite resin splint in the treatment of chronic periodontitis. J. Contemp. Dent. Pract. 2011, 12, 343–349. [Google Scholar]
- Junior, G.; de Aquino, A.; Lopes, M.W.; Gaspar, G.D.; Braz, R. Comparative study of flexural strength and elasticity modulus in two types of direct fiber-reinforced systems. Braz. Oral. Res. 2009, 23, 236–240. [Google Scholar] [CrossRef]
- Juloski, J.; Beloicab, M.; Goraccic, C.; Chieffid, N.; Giovannettie, A.; Vichif, A. Shear bond strength to enamel and flexural strength of different fiber-reinforced composites. J. Adhes. Dent. 2012, 14, 1–8. [Google Scholar]
- Chaudhary, V.; Shrivastava, B.; Bhatia, H.P.; Aggarwal, A.; Singh, A.K.; Gupta, N. Multifunctional ribbond—A versatile tool. J. Clin. Pediatr. Dent. 2012, 325–328. [Google Scholar] [CrossRef]
- Foek, D.L.S.; Yetkiner, E.; Özcan, M. Fatigue resistance, debonding force, and failure type of fiber-reinforced composite, polyethylene ribbon-reinforced, and braided stainless steel wire lingual retainers in vitro. Korean J. Orthod. 2013, 43, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Purayil, T.P.; Chakravarthy, A.; Ginjupalli, K.; Ballal, N.V. Evaluation of bond strength of splinting materials to the teeth using three adhesive systems—An in vitro study. Saudi J. Oral. Sci. 2015, 2, 94–98. [Google Scholar] [CrossRef]
- Meiers, J.C.; Freilich, M.A. Conservative anterior tooth replacement using fiber-reinforced composite. Oper. Dent. 2000, 25, 239–243. [Google Scholar] [PubMed]
- Goldberg, A.J.; Burstone, C.J. Flexural properties and fiber architecture of commercial fiber reinforced composites. J. Dent. Res. 1998, 77, 226. [Google Scholar]
- Soares, P.B.; Fernandes, N.A.J.; Magalhães, D.; Versluis, A.; Soares, C.J. Effect of bone loss simulation and periodontal splinting on bone strain: Periodontal splints and bone strain. Arch. Oral. Biol. 2011, 56, 1373–1381. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tayab, T.; Shetty, A.; Kayalvizhi, G. The Clinical Applications of Fiber Reinforced Composites in all Specialties of Dentistry: An Overview. Int. J. Compos. Mater. 2015, 5, 18. [Google Scholar]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).