
Early Pupillometry Assessment in Traumatic Brain Injury Patients: A Retrospective Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Patients’ Management
2.3. Automated Pupillometry
2.4. Data Collection
2.5. Study Outcomes
2.6. Statistical Analyses
3. Results
3.1. Study Population
3.2. NPi and Neurological Outcome
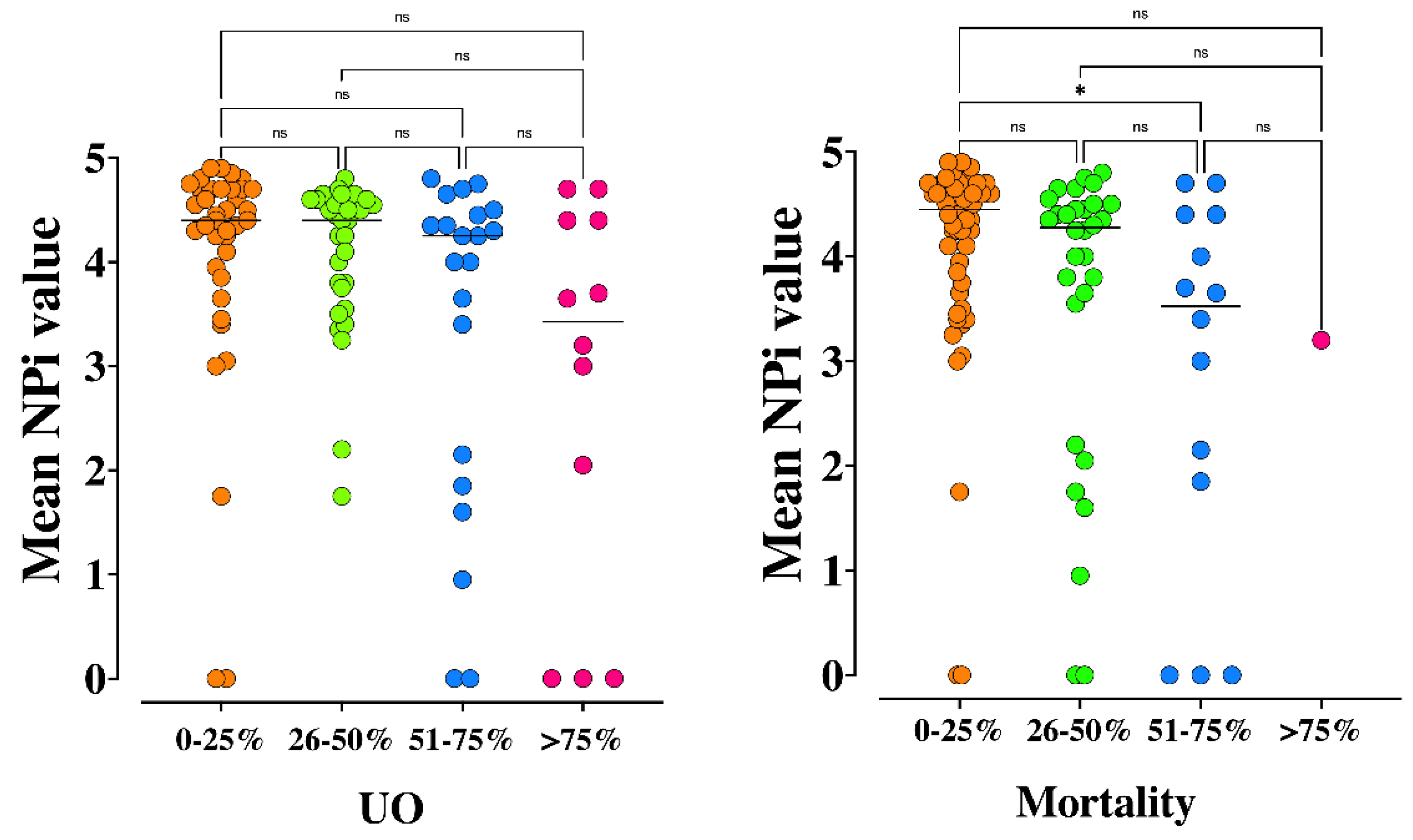
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brazinova, A.; Rehorcikova, V.; Taylor, M.S.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef] [Green Version]
- Stocchetti, N.; Roux, P.; Vespa, P.; Oddo, M.; Citerio, G.; Andrews, P.J.; Stevens, R.D.; Sharshar, T.; Taccone, F.S.; Vincent, Je. Clinical review: Neuromonitoring—An update. Crit. Care 2013, 17, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharshar, T.; Citerio, G.; Andrews, P.J.D.; Chieregato, A.; Latronico, N.; Menon, D.K.; Puybasset, L.; Sandroni, C.; Stevens, R.D. Neurological examination of critically ill patients: A pragmatic approach. Report of an ESICM expert panel. Intensive Care Med. 2014, 40, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Mader, M.M.D.; Rotermund, R.; Lefering, R.; Westphal, M.; Maegele, M.; Czorlich, P.; TraumaRegister DGU. The faster the better? Time to first CT scan after admission in moderate-to-severe traumatic brain injury and its association with mortality. Neurosurg. Rev. 2021, 44, 2697–2706. [Google Scholar] [CrossRef] [PubMed]
- Tien, H.C.; Cunha, J.R.F.; Wu, S.N.; Chughtai, T.; Tremblay, L.N.; Brenneman, F.D.; Rizoli, S.B. Do Trauma Patients with a Glasgow Coma Scale Score of 3 and Bilateral Fixed and Dilated Pupils Have Any Chance of Survival? J. Trauma 2006, 60, 5. [Google Scholar] [CrossRef]
- Marmarou, A.; Lu, J.; Butcher, I.; Mchugh, G.S.; Murray, G.D.; Steyerberg, E.W.; Mushkudiani, N.A.; Choi, S.; Maas, A.I.R. Prognostic Value of The Glasgow Coma Scale and Pupil Reactivity in Traumatic Brain Injury Assessed Pre-Hospital and on Enrollment: An IMPACT Analysis. J. Neurotrauma 2007, 24, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Mushkudiani, N.; Perel, P.; Butcher, I.; Lu, J.; McHugh, G.S.; Murray, G.D.; Marmarou, A.; Roberts, I.; Habbema, J.D.F.; et al. Predicting Outcome after Traumatic Brain Injury: Development and International Validation of Prognostic Scores Based on Admission Characteristics. PLoS Med. 2008, 5, e165. [Google Scholar] [CrossRef] [Green Version]
- Litvan, I.; Saposnik, G.; Maurino, J.; Gonzalez, L.; Saizar, R.; Sica, R.E.P.; Bartko, J.J. Pupillary diameter assessment: Need for a graded scale. Neurology 2000, 54, 530. [Google Scholar] [CrossRef] [PubMed]
- Morelli, P.; Oddo, M.; Ben-Hamouda, N. Role of automated pupillometry in critically ill patients. Minerva Anestesiol. 2019, 85, 995–1002. [Google Scholar] [CrossRef]
- Couret, D.; Boumaza, D.; Grisotto, C.; Triglia, T.; Pellegrini, L.; Ocquidant, P.; Bruder, N.J.; Velly, L.J. Reliability of standard pupillometry practice in neurocritical care: An observational, double-blinded study. Crit. Care 2016, 20, 99. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.W.; Vakil-Gilani, K.; Williamson, K.L.; Cecil, S. Infrared pupillometry, the Neurological Pupil index and unilateral pupillary dilation after traumatic brain injury: Implications for treatment paradigms. SpringerPlus 2014, 3, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oddo, M.; Sandroni, C.; Citerio, G.; Miroz, J.-P.; Horn, J.; Rundgren, M.; Cariou, A.; Payen, Je.; Storm, C.; Stammet, P.; et al. Quantitative versus standard pupillary light reflex for early prognostication in comatose cardiac arrest patients: An international prospective multicenter double-blinded study. Intensive Care Med. 2018, 44, 2102–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miroz, J.-P.; Ben-Hamouda, N.; Bernini, A.; Romagnosi, F.; Bongiovanni, F.; Roumy, A.; Kirsch, M.; Liaudet, L.; Eckert, P.; Oddo, M. Neurological Pupil index for Early Prognostication After Venoarterial Extracorporeal Membrane Oxygenation. Chest 2020, 157, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Jahns, F.-P.; Miroz, J.P.; Messerer, M.; Daniel, R.T.; Taccone, F.S.; Eckert, P.; Oddo, M. Quantitative pupillometry for the monitoring of intracranial hypertension in patients with severe traumatic brain injury. Crit. Care 2019, 23, 155. [Google Scholar] [CrossRef] [Green Version]
- El Ahmadieh, T.Y.; Bedros, N.; Stutzman, S.E.; Nyancho, D.; Venkatachalam, A.M.; MacAllister, M.; Ban, V.S.; Dahdaleh, N.S.; Aiyagari, V.; Figueroa, S.; et al. Automated Pupillometry as a Triage and Assessment Tool in Patients with Traumatic Brain Injury. World Neurosurg. 2021, 145, e163–e169. [Google Scholar] [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.J.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable Infrared Pupillometry: A Review. Anesth. Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Reith, F.C.M.; Van den Brande, R.; Synnot, A.; Gruen, R.; Maas, A.I.R. The reliability of the Glasgow Coma Scale: A systematic review. Intensive Care Med. 2016, 42, 3–15. [Google Scholar] [CrossRef]
- Marshall, L.F.; Marshall, S.B.; Klauber, M.R.; Van Berkum Clark, M.; Eisenberg, H.; Jane, J.A.; Luerssen, T.G.; Marmarou, A.; Foulkes, M.A. The diagnosis of head injury requires a classification based on computed axial tomography. J. Neurotrauma 1992, 9 (Suppl. 1), S287–292. [Google Scholar]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Zuercher, P.; Groen, J.L.; Aries, M.J.H.; Steyerberg, E.W.; Maas, A.I.R.; Ercole, A.; Menon, D.K. Reliability and Validity of the Therapy Intensity Level Scale: Analysis of Clinimetric Properties of a Novel Approach to Assess Management of Intracranial Pressure in Traumatic Brain Injury. J. Neurotrauma 2016, 33, 1768–1774. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, M.M.; Sweidan, A.J.; Xu, J.C.; Stern-Nezer, S.; Yu, W.; Groysman, L.I. Quantitative Pupillometry in the Intensive Care Unit. J. Intensive Care Med. 2019, 36. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.S.; Mueller, C.M.; Nogueira, R.G.; Khalifa, Y.M. A Systematic Review Assessing the Current State of Automated Pupillometry in the NeuroICU. Neurocrit. Care 2019, 31, 142–161. [Google Scholar] [CrossRef]
- Park, J.G.; Moon, C.T.; Park, D.S.; Song, S.W. Clinical Utility of an Automated Pupillometer in Patients with Acute Brain Lesion. J. Korean Neurosurg. Soc. 2015, 58, 363. [Google Scholar] [CrossRef]
- Chen, J.; Gombart, Z.; Rogers, S.; Gardiner, S.; Cecil, S.; Bullock, R. Pupillary reactivity as an early indicator of increased intracranial pressure: The introduction of the neurological pupil index. Surg. Neurol. Int. 2011, 2, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, K.E.; Wallen, T.E.; Jalbert, T.; Wakefield, D.; Spuzzillo, A.; Sharma, S.; Earnest, R.; Heh, V.; Foreman, B.; Goodman, M.D. Efficacy of Noninvasive Technologies in Triaging Traumatic Brain Injury and Correlating with Intracranial Pressure: A Prospective Study. J. Surg. Res. 2021, 262, 27–37. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | ALL (n = 100) | UO (n = 49) | FO (n = 51) | p-Value |
|---|---|---|---|---|
| Age, years | 48 (34–69) | 55 (39–75) | 45 (32–62) | 0.04 |
| Male Gender, n (%) | 73 (73) | 32 (65) | 41 (80) | 0.12 |
| Mechanism of Trauma n (%) | 0.02 | |||
| Fall * | 64 (64) | 38 (78) | 26 (51) | |
| Car accident | 24 (24) | 9 (18) | 15 (29) | |
| Aggression | 9 (9) | 1 (2) | 8 (16) | |
| Other | 3 (3) | 1 (2) | 2 (4) | |
| Polytrauma, n (%) | 38 (38) | 17 (35) | 21 (41) | 0.54 |
| Glasgow Coma Scale on admission | 11 (6–15) | 8 (4–13) | 14 (8–15) | <0.001 |
| SOFA Score on admission | 6 (2–8) | 9 (5–10) | 3 (1–6) | <0.001 |
| Marshall Score | 5 (2–5) | 5 (3–5) | 4 (2–5) | 0.35 |
| Neurological Pupil Index | ||||
| Worst NPi on admission | 4.2 (3.2–4.5) | 3.9 (1.7–4.4) | 4.4 (3.7–4.6) | 0.005 |
| Mean NPi on admission | 4.3 (3.4–4.6) | 4 (2.6–4.5) | 4.5 (3.9–4.7) | 0.002 |
| NPi < 3, n (%) | 20 (20) | 14 (29) | 6 (12) | 0.046 |
| NPi < 2, n (%) | 13 (13) | 11 (22) | 2 (4) | 0.007 |
| Worst size (max) on admission, mm | 3.1 (2.4–4.2) | 2.9 (2.3–4.1) | 3.2 (2.7–4.2) | 0.39 |
| Worst CH (min) on admission, % | 16 (9–26) | 12 (6–20) | 18 (11–31) | 0.008 |
| Comorbidities | ||||
| COPD, n (%) | 8 (8) | 4 (8) | 4 (8) | 1 |
| Chronic kidney disease, n (%) | 7 (7) | 6 (12) | 1 (2) | 0.06 |
| Liver Cirrhosis, n (%) | 5 (5) | 5 (10) | 0 | 0.02 |
| Heart disease, n (%) | 24 (24) | 16 (33) | 8 (16) | 0.06 |
| Immunosuppression, n (%) | 1 (1) | 1 (2) | 0 | 0.49 |
| Previous neurological disease, n (%) | 19 (19) | 13 (27) | 6 (12) | 0.08 |
| Cancer, n (%) | 5 (5) | 3 (6) | 2 (4) | 0.67 |
| Diabetes, n (%) | 12 (12) | 5 (10) | 7 (14) | 0.76 |
| Arterial Hypertension, n (%) | 25 (25) | 19 (39) | 6 (12) | 0.002 |
| Alcohol, n (%) | 40 (40) | 20 (41) | 20 (39) | 0.99 |
| Smoking, n (%) | 22 (22) | 8 (16) | 14 (28) | 0.23 |
| ICU Therapies | ||||
| Therapy Intensity Level (TIL-Basic) | 2 (1–4) | 4 (2–4) | 1 (1–2) | <0.001 |
| Sedative drugs, n (%) | 68 (68) | 45 (92) | 23 (45) | <0.001 |
| Analgesic drugs, n (%) | 81 (81) | 46 (94) | 35 (69) | 0.002 |
| Vasopressor drugs, n (%) | 56 (56) | 38 (77) | 18 (65) | <0.001 |
| Inotropes drugs, n (%) | 2 (2) | 2 (4) | 0.24 | |
| Mechanical ventilation, n (%) | 69 (69) | 44 (90) | 25 (49) | <0.001 |
| ECMO, n (%) | 1 (1) | 1 (2) | 0.49 | |
| ICP Monitoring, n (%) | 45 (45) | 32 (65) | 13 (26) | <0.001 |
| Osmotic drugs, n (%) | 46 (46) | 32 (65) | 14 (28) | <0.001 |
| Decompressive craniectomy, n (%) | 29 (29) | 22 (45) | 7 (14) | <0.001 |
| Barbiturates, n (%) | 17 (17) | 14 (29) | 3 (6) | 0.003 |
| Hypothermia, n (%) | 6 (6) | 6 (12) | 0.012 | |
| Outcome Variables | ||||
| ICU stay, days | 6 (3–17) | 12 (4–23) | 2 (3–7) | 0.01 |
| Hospital stay, days | 16 (8–43) | 22 (9–42) | 15 (8–43) | 0.61 |
| ICU death, n (%) | 27 (27) | 27 (55.1) | <0.001 | |
| Hospital death, n (%) | 29 (29) | 29 (59.2) | <0.001 | |
| IMPACT Mortality, % | 34 (15–50) | 44 (24–57) | 21 (12–37) | 0.011 |
| IMPACT Unfavourable Outcome, % | 50 (24–71) | 64 (36–75) | 37 (18–56) | 0.006 |
| Variables | AUC [IC 95%] | p-Value |
|---|---|---|
| Marshall score | 0.57 (0.41–0.73) | 0.37 |
| TIL | 0.63 (0.48–0.78) | 0.11 |
| IMPACT score | 0.72 (0.59–0.85) | 0.006 |
| GCS on admission | 0.70 (0.60–0.81) | <0.001 |
| Worst NPi on admission | 0.66 (0.58–0.77] | 0.005 |
| Mean NPi on admission | 0.68 (0.57–0.78) | 0.002 |
| Worst Pupil Size on admission | 0.45 (0.33–0.56) | 0.37 |
| Worst CH on admission | 0.65 (0.545–0.76) | 0.008 |
| UO | Mortality | |
|---|---|---|
| Coefficient | Coefficient | |
| (Intercept) | −0.009 | −2.62 |
| SOFA score on admission | 0.207 | 0.251 |
| Age | 0.767 | |
| Mean NPi | −0.627 | |
| Worst NPi | −0.468 | |
| Arterial Hypertension | 1.128 | 0.687 |
| Liver Cirrhosis | 0.524 | 0.898 |
| Vasopressors | 0.342 | 0.641 |
| Sedatives | 0.889 | 1.057 |
| Opioids | 1.328 | |
| Hypothermia | 1.059 | |
| TIL Score | 0.486 | 0.528 |
| Mechanism of trauma | 0.602 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luz Teixeira, T.; Peluso, L.; Banco, P.; Njimi, H.; Abi-Khalil, L.; Chanchay Pillajo, M.; Schuind, S.; Creteur, J.; Bouzat, P.; Taccone, F.S. Early Pupillometry Assessment in Traumatic Brain Injury Patients: A Retrospective Study. Brain Sci. 2021, 11, 1657. https://doi.org/10.3390/brainsci11121657
Luz Teixeira T, Peluso L, Banco P, Njimi H, Abi-Khalil L, Chanchay Pillajo M, Schuind S, Creteur J, Bouzat P, Taccone FS. Early Pupillometry Assessment in Traumatic Brain Injury Patients: A Retrospective Study. Brain Sciences. 2021; 11(12):1657. https://doi.org/10.3390/brainsci11121657
Chicago/Turabian StyleLuz Teixeira, Thomas, Lorenzo Peluso, Pierluigi Banco, Hassane Njimi, Layal Abi-Khalil, Mélanie Chanchay Pillajo, Sophie Schuind, Jacques Creteur, Pierre Bouzat, and Fabio Silvio Taccone. 2021. "Early Pupillometry Assessment in Traumatic Brain Injury Patients: A Retrospective Study" Brain Sciences 11, no. 12: 1657. https://doi.org/10.3390/brainsci11121657
APA StyleLuz Teixeira, T., Peluso, L., Banco, P., Njimi, H., Abi-Khalil, L., Chanchay Pillajo, M., Schuind, S., Creteur, J., Bouzat, P., & Taccone, F. S. (2021). Early Pupillometry Assessment in Traumatic Brain Injury Patients: A Retrospective Study. Brain Sciences, 11(12), 1657. https://doi.org/10.3390/brainsci11121657