

Repeated Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: A Double-Blinded Randomized Controlled Clinical Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Design
2.3. Transcranial Direct Current Stimulation Protocol
2.4. Evaluations
2.5. Statistical Analysis
3. Results
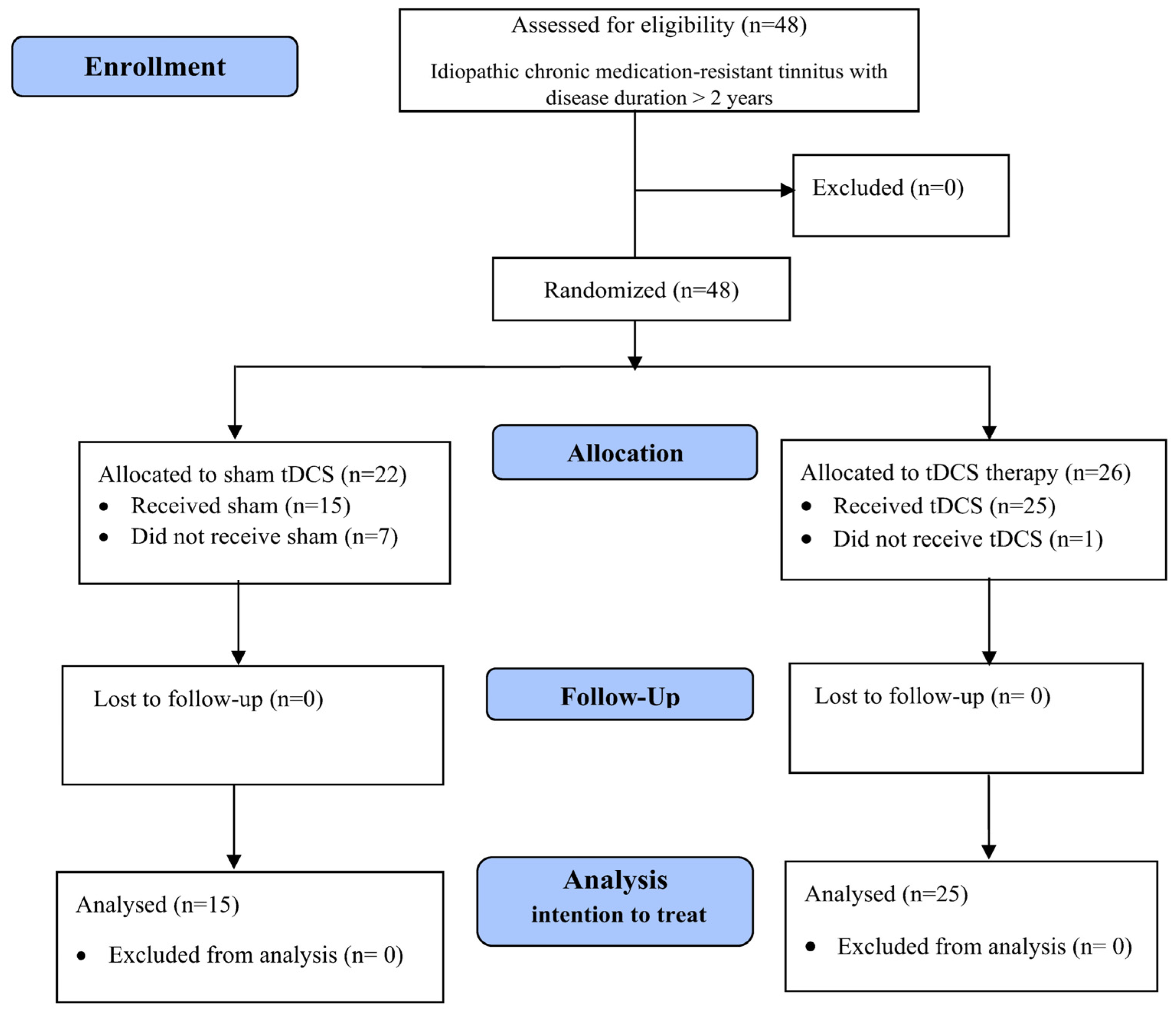
3.1. Participants
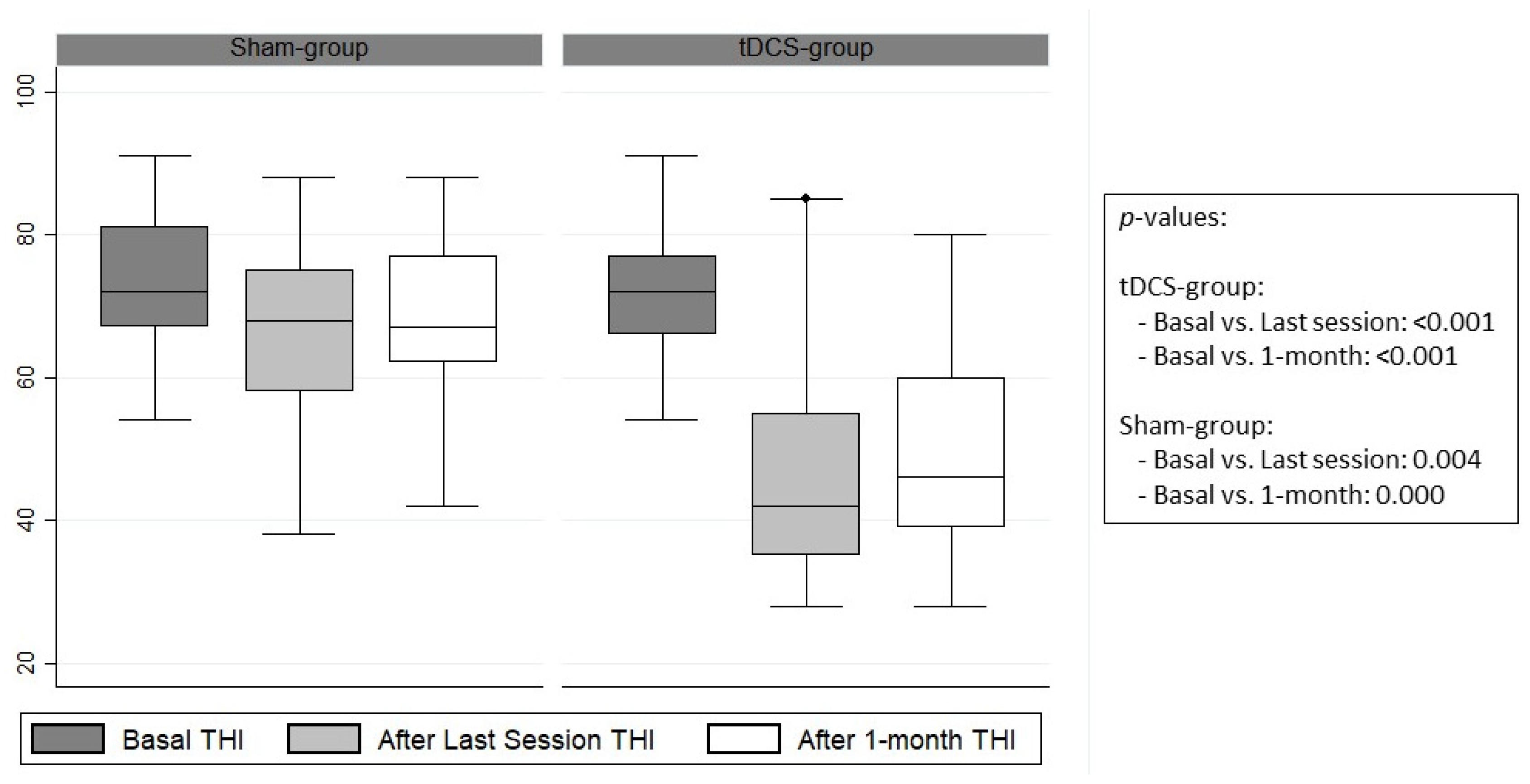
3.2. Response Variables
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.-J.; Lee, H.-J.; An, S.-Y.; Sim, S.; Park, B.; Kim, S.W.; Lee, J.S.; Hong, S.K.; Choi, H.G. Analysis of the Prevalence and Associated Risk Factors of Tinnitus in Adults. PLoS ONE 2015, 10, e0127578. [Google Scholar] [CrossRef] [PubMed]
- Smits, M.; Kovacs, S.; De Ridder, D.; Peeters, R.R.; Van Hecke, P.; Sunaert, S. Lateralization of Functional Magnetic Resonance Imaging (fMRI) Activation in the Auditory Pathway of Patients with Lateralized Tinnitus. Neuroradiology 2007, 49, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, J.J. Pathophysiology of Tinnitus. Prog. Brain Res. 2007, 166, 19–543. [Google Scholar] [PubMed]
- De Ridder, D.; Fransen, H.; Francois, O.; Sunaert, S.; Kovacs, S.; Van De Heyning, P. Amygdalohippocampal Involvement in Tinnitus and Auditory Memory. Acta Oto-Laryngol. 2006, 126, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; Plazier, M.; Ost, J.; van der Loo, E.; Van de Heyning, P.; De Ridder, D. Bilateral Dorsolateral Prefrontal Cortex Modulation for Tinnitus by Transcranial Direct Current Stimulation: A Preliminary Clinical Study. Exp. Brain Res. 2010, 202, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Weisz, N.; Müller, S.; Schlee, W.; Dohrmann, K.; Hartmann, T.; Elbert, T. The Neural Code of Auditory Phantom Perception. J. Neurosci. 2007, 27, 1479–1484. [Google Scholar] [CrossRef]
- Schlee, W.; Hartmann, T.; Langguth, B.; Weisz, N. Abnormal Resting-State Cortical Coupling in Chronic Tinnitus. BMC Neurosci. 2009, 10, 11. [Google Scholar] [CrossRef]
- Langguth, B.; Eichhammer, P.; Kreutzer, A.; Maenner, P.; Marienhagen, J.; Kleinjung, T.; Sand, P.; Hajak, G. The Impact of Auditory Cortex Activity on Characterizing and Treating Patients with Chronic Tinnitus—First Results from a PET Study. Acta Oto-Laryngol. 2006, 126, 84–88. [Google Scholar] [CrossRef]
- Van Der Loo, E.; Congedo, M.; Vanneste, S.; Van De Heyning, P.; De Ridder, D. Insular Lateralization in Tinnitus Distress. Auton. Neurosci. 2011, 165, 191–194. [Google Scholar] [CrossRef]
- Vanneste, S.; De Ridder, D. Bifrontal Transcranial Direct Current Stimulation Modulates Tinnitus Intensity and Tinnitus-distress-related Brain Activity. Eur. J. Neurosci. 2011, 34, 605–614. [Google Scholar] [CrossRef]
- Vanneste, S.; Van de Heyning, P.; De Ridder, D. Contralateral Parahippocampal Gamma-Band Activity Determines Noise-like Tinnitus Laterality: A Region of Interest Analysis. Neuroscience 2011, 199, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.W.; Beauchamp, M.S.; DeYoe, E.A. A Comparison of Visual and Auditory Motion Processing in Human Cerebral Cortex. Cereb. Cortex 2000, 10, 873–888. [Google Scholar] [CrossRef] [PubMed]
- Voisin, J.; Bidet-Caulet, A.; Bertrand, O.; Fonlupt, P. Listening in Silence Activates Auditory Areas: A Functional Magnetic Resonance Imaging Study. J. Neurosci. 2006, 26, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.E.; Eggermont, J.J.; Caspary, D.M.; Shore, S.E.; Melcher, J.R.; Kaltenbach, J.A. Ringing Ears: The Neuroscience of Tinnitus. J. Neurosci. 2010, 30, 14972–14979. [Google Scholar] [CrossRef]
- Nemholt, S.S.; Schmidt, J.H.; Wedderkopp, N.; Baguley, D.M. Prevalence of Tinnitus and/or Hyperacusis in Children and Adolescents: Study Protocol for a Systematic Review. BMJ Open 2015, 5, e006649. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, D.; Lee, J.-M.; Lee, S.K.; Kang, H.J.; Yeo, S.G. Review of Pharmacotherapy for Tinnitus. Healthcare 2021, 9, 779. [Google Scholar] [CrossRef] [PubMed]
- Rauschecker, J.P.; Leaver, A.M.; Mühlau, M. Tuning out the Noise: Limbic-Auditory Interactions in Tinnitus. Neuron 2010, 66, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Khoramzadeh, S.; Saki, N.; Davoodi, I.; Nosratabadi, M.; Yadollahpour, A. Investigating the Therapeutic Efficacy of Neurofeedback Treatment on the Severity of Symptoms and Quality of Life in Patients with Tinnitus. Int. J. Ment. Health Addict. 2016, 14, 982–992. [Google Scholar] [CrossRef]
- Mondino, M.; Haesebaert, F.; Poulet, E.; Saoud, M.; Brunelin, J. Efficacy of Cathodal Transcranial Direct Current Stimulation over the Left Orbitofrontal Cortex in a Patient with Treatment-Resistant Obsessive-Compulsive Disorder. J. ECT 2015, 31, 271–272. [Google Scholar] [CrossRef]
- Saunders, N.; Downham, R.; Turman, B.; Kropotov, J.; Clark, R.; Yumash, R.; Szatmary, A. Working Memory Training with tDCS Improves Behavioral and Neurophysiological Symptoms in Pilot Group with Post-Traumatic Stress Disorder (PTSD) and with Poor Working Memory. Neurocase 2015, 21, 271–278. [Google Scholar] [CrossRef]
- Baker, J.M.; Rorden, C.; Fridriksson, J. Using Transcranial Direct-Current Stimulation to Treat Stroke Patients with Aphasia. Stroke 2010, 41, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Yadollahpour, A.; Jalilifar, M.; Rashidi, S. Transcranial Direct Current Stimulation for the Treatment of Depression: A Comprehensive Review of the Recent Advances. Int. J. Ment. Health Addict. 2017, 15, 434–443. [Google Scholar] [CrossRef]
- Yadollahpour, A.; Asl, H.M.; Rashidi, S. Transcranial Direct Current Stimulation as a Non-Medication Modality for Attention Enhancement: A Review of the Literature. Res. J. Pharm. Technol. 2017, 10, 311–316. [Google Scholar] [CrossRef]
- Frank, E.; Schecklmann, M.; Landgrebe, M.; Burger, J.; Kreuzer, P.; Poeppl, T.B.; Kleinjung, T.; Hajak, G.; Langguth, B. Treatment of Chronic Tinnitus with Repeated Sessions of Prefrontal Transcranial Direct Current Stimulation: Outcomes from an Open-Label Pilot Study. J. Neurol. 2012, 259, 327–333. [Google Scholar] [CrossRef]
- De Ridder, D.; Vanneste, S. EEG Driven tDCS versus Bifrontal tDCS for Tinnitus. Front. Psychiatry 2012, 3, 84. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Marcondes, R.; Boggio, P.S.; Marcolin, M.A.; Rigonatti, S.P.; Sanchez, T.G.; Nitsche, M.A.; Pascual-Leone, A. Transient Tinnitus Suppression Induced by Repetitive Transcranial Magnetic Stimulation and Transcranial Direct Current Stimulation. Eur. J. Neurol. 2006, 13, 996–1001. [Google Scholar] [CrossRef]
- Stagg, C.J.; Nitsche, M.A. Physiological Basis of Transcranial Direct Current Stimulation. Neuroscientist 2011, 17, 37–53. [Google Scholar] [CrossRef]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Vanneste, S.; Congedo, M. The Distressed Brain: A Group Blind Source Separation Analysis on Tinnitus. PLoS ONE 2011, 6, e24273. [Google Scholar] [CrossRef]
- Yuan, T.; Yadollahpour, A.; Salgado-Ramírez, J.; Robles-Camarillo, D.; Ortega-Palacios, R. Transcranial Direct Current Stimulation for the Treatment of Tinnitus: A Review of Clinical Trials and Mechanisms of Action 11 Medical and Health Sciences 1103 Clinical Sciences. BMC Neurosci. 2018, 19, 66. [Google Scholar] [CrossRef]
- Wang, T.C.; Tyler, R.S.; Chang, T.Y.; Chen, J.C.; Lin, C.D.; Chung, H.K.; Tsou, Y.A. Effect of Transcranial Direct Current Stimulation in Patients with Tinnitus: A Meta-Analysis and Systematic Review. Ann. Otol. Rhinol. Laryngol. 2018, 127, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.L.; da Silva Souza, D.; Cavalcante, M.E.D.O.B.; Barboza, H.N.; de Medeiros, J.F.; dos Santos Andrade, S.M.M.; da Silva Machado, D.G.; da Rosa, M.R.D. Effect of Transcranial Direct Current Stimulation for Tinnitus Treatment: A Systematic Review and Meta-Analysis. Neurophysiol. Clin. 2022, 52, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, L.G.P.; Eisenman, D.J. Current Device-Based Clinical Treatments for Tinnitus. Otolaryngol. Clin. N. Am. 2020, 53, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Du, M.; Wang, Y.; Li, Y.; Tong, B.; Qiu, J.; Wu, F.; Liu, Y. State of the Art: Non-Invasive Electrical Stimulation for the Treatment of Chronic Tinnitus. Ther. Adv. Chronic Dis. 2023, 14, 20406223221148061. [Google Scholar] [CrossRef]
- Labree, B.; Hoare, D.J.; Gascoyne, L.E.; Scutt, P.; Del Giovane, C.; Sereda, M. Determining the Effects of Transcranial Direct Current Stimulation on Tinnitus, Depression, and Anxiety: A Systematic Review. Brain Sci. 2022, 12, 484. [Google Scholar] [CrossRef] [PubMed]
- Yadollahpour, A.; Rashidi, S.; Jaberzade, S. Single Session Anodal, Cathodal and Placebo Bifrontal tDCS for Treatment of Intractable Chronic Tinnitus: A Randomized Controlled Clinical Trial. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2019, 12, 406. [Google Scholar] [CrossRef]
- Forogh, B.; Mirshaki, Z.; Raissi, G.R.; Shirazi, A.; Mansoori, K.; Ahadi, T. Repeated Sessions of Transcranial Direct Current Stimulation for Treatment of Chronic Subjective Tinnitus: A Pilot Randomized Controlled Trial. Neurol. Sci. 2016, 37, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, S.; Yadollahpour, A. Three Weeks Bilateral tDCS over Auditory Cortex Significantly Improves Tinnitus: A Double Blinded Randomized Controlled Clinical Trial. Brain Stimul. 2023, 16, 403. [Google Scholar] [CrossRef]
- Garin, P.; Gilain, C.; Van Damme, J.P.; de Fays, K.; Jamart, J.; Ossemann, M.; Vandermeeren, Y. Short- and Long-Lasting Tinnitus Relief Induced by Transcranial Direct Current Stimulation. J. Neurol. 2011, 258, 1940–1948. [Google Scholar] [CrossRef]
- Shekhawat, G.S.; Searchfield, G.D.; Stinear, C.M. Randomized Trial of Transcranial Direct Current Stimulation and Hearing Aids for Tinnitus Management. Neurorehabilit. Neural Repair 2014, 28, 410–419. [Google Scholar] [CrossRef]
- Kikuta, S.; Matsumoto, Y.; Kuboki, A.; Nakayama, T.; Asaka, D.; Otori, N.; Kojima, H.; Sakamoto, T.; Akinori, K.; Kanaya, K.; et al. Longer Latency of Sensory Response to Intravenous Odor Injection Predicts Olfactory Neural Disorder. Sci. Rep. 2016, 6, 35361. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; De Ridder, D. Noninvasive and Invasive Neuromodulation for the Treatment of Tinnitus: An Overview. Neuromodulation Technol. Neural Interface 2012, 15, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Yadollahpour, A.; Mayo, M.; Saki, N.; Rashidi, S.; Bayat, A. A Chronic Protocol of Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: Dataset from a Double-Blinded Randomized Controlled Trial. F1000Research 2018, 7, 733. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-Based Guidelines on the Therapeutic Use of Transcranial Direct Current Stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Yadollahpour, A.; Bayat, A.; Rashidi, S.; Saki, N.; Karimi, M. Dataset of Acute Repeated Sessions of Bifrontal Transcranial Direct Current Stimulation for Treatment of Intractable Tinnitus: A Randomized Controlled Trial. Data Brief 2017, 15, 40–46. [Google Scholar] [CrossRef]
- Rashidi, S.; Yadollahpour, A.; Alkahtani, S.A.; Kunwar, P.S.; Robles-Camarillo, D.; Meneses-Flores, A.; Trejo-Macotela, F. The Effects of Acute Multisession Bifrontal Transcranial Direct Current Stimulation on Intractable Tinnitus and Comorbid Depression and Anxiety: A Study Protocol for Randomized Controlled Trial. Int. Tinnitus J. 2018, 22, 181–187. [Google Scholar] [CrossRef]
- Hyvärinen, P.; Mäkitie, A.; Aarnisalo, A.A. Self-Administered Domiciliary tDCS Treatment for Tinnitus: A Double-Blind Sham-Controlled Study. PLoS ONE 2016, 11, e0154286. [Google Scholar] [CrossRef] [PubMed]
- Mares, T.; Albrecht, J.; Buday, J.; Podgorna, G.; Le, T.H.; Magyarova, E.; Poshor, K.; Halik, J.; Buna, J.; Capek, V.; et al. Long-Term Effect of Transcranial Direct Current Stimulation in the Treatment of Chronic Tinnitus: A Randomized, Placebo-Controlled Trial. Front. Psychiatry 2022, 13, 969800. [Google Scholar] [CrossRef] [PubMed]
- Bayat, A.; Mayo, M.; Rashidi, S.; Saki, N.; Yadollahpour, A. Repeated Sessions of Bilateral Transcranial Direct Current Stimulation on Intractable Tinnitus: A Study Protocol for a Double-Blind Randomized Controlled Trial. F1000Research 2018, 7, 317. [Google Scholar] [CrossRef]
- Shekhawat, G.S.; Vanneste, S. Optimization of Transcranial Direct Current Stimulation of Dorsolateral Prefrontal Cortex for Tinnitus: A Non-Linear Dose-Response Effect. Sci. Rep. 2018, 8, 8311. [Google Scholar] [CrossRef]
- Vanneste, S.; Langguth, B.; De Ridder, D. Do tDCS and TMS Influence Tinnitus Transiently via a Direct Cortical and Indirect Somatosensory Modulating Effect? A Combined TMS-tDCS and TENS Study. Brain Stimul. 2011, 4, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Faber, M.; Vanneste, S.; Fregni, F.; De Ridder, D. Top down Prefrontal Affective Modulation of Tinnitus with Multiple Sessions of tDCS of Dorsolateral Prefrontal Cortex. Brain Stimul. 2012, 5, 492–498. [Google Scholar] [CrossRef]
- Shekhawat, G.S.; Sundram, F.; Bikson, M.; Truong, D.; De Ridder, D.; Stinear, C.M.; Welch, D.; Searchfield, G.D. Intensity, Duration, and Location of High-Definition Transcranial Direct Current Stimulation for Tinnitus Relief. Neurorehabilit. Neural Repair 2016, 30, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Cardon, E.; Jacquemin, L.; Vermeersch, H.; Joossen, I.; Moyaert, J.; Mertens, G.; Vanderveken, O.M.; Lammers, M.J.W.; Van De Heyning, P.; Van Rompaey, V.; et al. Dual-Site Transcranial Direct Current Stimulation to Treat Tinnitus: A Randomized Controlled Trial. Brain J. Neurol. 2022, 145, 4222–4231. [Google Scholar] [CrossRef]
- Elyssa Kok, T.; Schaette, R.; Shekhawat, G.S. Impact of tDCS and HD-tDCS on Tinnitus Perception: A Scoping Review. Prog. Brain Res. 2021, 262, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Teismann, H.; Wollbrink, A.; Okamoto, H.; Schlaug, G.; Rudack, C.; Pantev, C. Combining Transcranial Direct Current Stimulation and Tailor-Made Notched Music Training to Decrease Tinnitus-Related Distress—A Pilot Study. PLoS ONE 2014, 9, e89904. [Google Scholar] [CrossRef]
- McCombe, A.; Baguley, D.; Coles, R.; McKenna, L.; McKinney, C.; Windle-Taylor, P. Guidelines for the Grading of Tinnitus Severity: The Results of a Working Group Commissioned by the British Association of Otolaryngologists, Head and Neck Surgeons, 1999. Clin. Otolaryngol. Allied Sci. 2001, 26, 388–393. [Google Scholar] [CrossRef]
- Klem, G.H.; Lüders, H.O.; Jasper, H.H.; Elger, C. The Ten-Twenty Electrode System of the International Federation. The International Federation of Clinical Neurophysiology. Electroencephalogr. Clin. Neurophysiol. Suppl. 1999, 52, 3–6. [Google Scholar]
- Poreisz, C.; Boros, K.; Antal, A.; Paulus, W. Safety Aspects of Transcranial Direct Current Stimulation Concerning Healthy Subjects and Patients. Brain Res. Bull. 2007, 72, 208–214. [Google Scholar] [CrossRef]
- Paulus, W. Transcranial Direct Current Stimulation (tDCS). Suppl. Clin. Neurophysiol. 2003, 56, 249–254. [Google Scholar]
- Surr, R.K.; Kolb, J.A.; Cord, M.T.; Garrus, N.P. Tinnitus Handicap Inventory (THI) as a Hearing Aid Outcome Measure. J. Am. Acad. Audiol. 1999, 10, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Shekhawat, G.S.; Stinear, C.M.; Searchfield, G.D. Transcranial Direct Current Stimulation Intensity and Duration Effects on Tinnitus Suppression. Neurorehabilit. Neural Repair 2013, 27, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; Fregni, F.; De Ridder, D. Head-to-Head Comparison of Transcranial Random Noise Stimulation, Transcranial AC Stimulation, and Transcranial DC Stimulation for Tinnitus. Front. Psychiatry 2013, 4, 158. [Google Scholar] [CrossRef] [PubMed]
- Pal, N.; Maire, R.; Stephan, M.A.; Herrmann, F.R.; Benninger, D.H. Transcranial Direct Current Stimulation for the Treatment of Chronic Tinnitus: A Randomized Controlled Study. Brain Stimul. 2015, 8, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; Walsh, V.; Van De Heyning, P.; De Ridder, D. Comparing Immediate Transient Tinnitus Suppression Using tACS and tDCS: A Placebo-Controlled Study. Exp. Brain Res. 2013, 226, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Zeman, F.; Koller, M.; Figueiredo, R.; Aazevedo, A.; Rates, M.; Coelho, C.; Kleinjung, T.; de Ridder, D.; Langguth, B.; Landgrebe, M. Tinnitus Handicap Inventory for Evaluating Treatment Effects. Otolaryngol. Head. Neck Surg. 2011, 145, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for Tinnitus Patient Assessment and Treatment Outcome Measurement: Tinnitus Research Initiative Meeting, Regensburg, July 2006. Prog. Brain Res. 2007, 166, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, S.; Focquaert, F.; Van de Heyning, P.; De Ridder, D. Different Resting State Brain Activity and Functional Connectivity in Patients Who Respond and Not Respond to Bifrontal tDCS for Tinnitus Suppression. Exp. Brain Res. 2011, 210, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.-R.; Shi, J.; Hu, Z.-Y.; Lin, Y.-Y.; Lin, Y.-T.; Jiang, X.; Wang, R.; Wang, X.-Q.; Wang, Y.-L. Is Transcranial Direct Current Stimulation Beneficial for Treating Pain, Depression, and Anxiety Symptoms in Patients with Chronic Pain? A Systematic Review and Meta-Analysis. Front. Mol. Neurosci. 2022, 15, 1056966. [Google Scholar] [CrossRef]
- Le, B.; Alonzo, A.; Bull, M.; Kabourakis, M.; Martin, D.; Loo, C. A Clinical Case Series of Acute and Maintenance Home Administered Transcranial Direct Current Stimulation in Treatment-Resistant Depression. J. ECT 2022, 38, e11–e19. [Google Scholar] [CrossRef]
- Sharma, D.K.; Kaur, S.; Singh, J.; Kaur, I. Role of Acamprosate in Sensorineural Tinnitus. Indian J. Pharmacol. 2012, 44, 93–96. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| TDCS-Group | Placebo-Group | Total | |||
|---|---|---|---|---|---|
| Right ear | Normal | N | 10 | 5 | 15 |
| % | 40 | 33.3 | 37.5 | ||
| Mild | N | 7 | 5 | 12 | |
| % | 28 | 33.3 | 30 | ||
| Moderate | N | 5 | 4 | 9 | |
| % | 20 | 26.7 | 22.5 | ||
| Profound | N | 3 | 1 | 4 | |
| % | 12 | 6.7 | 10 | ||
| Left ear | Normal | N | 11 | 5 | 16 |
| % | 44 | 33.3 | 40 | ||
| Mild | N | 10 | 6 | 16 | |
| % | 40 | 40 | 40 | ||
| Moderate | N | 3 | 3 | 6 | |
| % | 12 | 20 | 15 | ||
| Profound | N | 1 | 1 | 2 | |
| % | 4 | 6.7 | 5 |
| N | % | |
|---|---|---|
| Ringing | 12 | 30 |
| Buzzing | 2 | 5 |
| Hissing | 7 | 17.5 |
| Ticking | 2 | 5 |
| High pitch whistling | 5 | 12 |
| Thumping | 2 | 5 |
| Cicadas | 5 | 12.5 |
| Pulsating | 5 | 12.5 |
| Mean ± SD | p-Value | ||
|---|---|---|---|
| tDCS Group | Placebo Group | ||
| Age | 47.52 ± 7.51 | 47.67 ± 7.96 | 0.954 |
| Tinnitus duration since its onset | 7.48 ± 3.99 | 7.60 ± 3.60 | 0.924 |
| Basal THI | 72.93 ± 10.11 | 71.90 ± 10.30 | 0.629 |
| THI post-intervention | 46.40 ± 15.36 | 66.73 ± 14.30 | <0.001 |
| THI 1-month post-intervention | 49.68 ± 14.49 | 66.73 ± 11.97 | <0.001 |
| Basal Loudness VAS | 7.36 ± 0.81 | 7.47 ± 0.91 | 0.708 |
| Loudness VAS immediate after last session | 5.60 ± 1.78 | 6.80 ± 1.52 | 0.036 |
| Loudness VAS 1-h post-last session | 5.56 ± 1.78 | 7.13 ± 1.40 | 0.006 |
| Loudness VAS 1-week post-last session | 5.68 ± 1.57 | 7.40 ± 1.05 | 0.001 |
| Loudness VAS 1-month post-last session | 6.64 ± 1.18 | 7.69 ± 0.85 | 0.010 |
| Basal Distress VAS | 7.68 ± 0.55 | 7.67 ± 0.61 | 0.971 |
| Distress VAS immediate after last session | 5.92 ± 1.25 | 7.07 ± 1.22 | 0.008 |
| Distress VAS 1-h post-last session | 5.92 ± 1.25 | 7.40 ± 1.12 | 0.001 |
| Distress VAS 1-week post-last session | 6.16 ± 1.24 | 7.47 ± 0.83 | 0.001 |
| Distress VAS 1-month post-last session | 6.92 ± 0.99 | 7.80 ± 0.56 | 0.003 |
| Improvement of ≥20 Points in the THI | |||||
|---|---|---|---|---|---|
| Yes | No | Total | Risk Ratio | ||
| Immediately after | tDCS treatment | 18 | 7 | 25 | 10.8 (IC 95%, 1.6–72.88) |
| Placebo group | 1 | 14 | 15 | ||
| Total | 19 | 21 | 40 | ||
| 1-month after | tDCS treatment | 14 | 11 | 25 | 2.36 (IC 95%, 1.51–3.7) |
| Placebo group | 0 | 15 | 15 | ||
| Total | 14 | 26 | 40 | ||
| Improvement ≥ 20 in THI Immediate after Last Session | |||||||
|---|---|---|---|---|---|---|---|
| Yes (N = 18) | No (N = 7) | Univariate Model | Multivariate Model | ||||
| p-Value | OR (IC 95%) | p-Value | OR Adjusted (IC 95%) | ||||
| Sex | Male | 7 (38.89) | 4 (57.14) | 0.413 | 0.48 (0.08–2.81) | 0.156 | 0.06 (0.00–2.89) |
| Female | 11 (61.11) | 3 (42.86) | 0.413 | 2.10 (0.36–12.32) | 0.156 | 16.33 (0.35–771.31) | |
| Mean ± SD | Mean ± SD | Univariate Model | Multivariate Model | ||||
| p-Value | OR (IC 95%) | p-Value | OR Adjusted (IC 95%) | ||||
| Age | 46.72 ± 7.68 | 49.57 ± 7.21 | 0.392 | 0.95 (0.84–1.07) | 0.325 | 0.325 (0.70–1.12) | |
| Tinnitus duration since its onset | 6.17 ± 3.40 | 10.86 ± 3.53 | 0.019 | 0.71 (0.53–0.95) | 0.064 | 0.64 (0.39–1.03) | |
| Basal THI | 70.94 ± 11.62 | 72.14 ± 7.95 | 0.795 | 0.99 (0.91–1.08) | 0.900 | 1.01 (0.88–1.16) | |
| Basal VAS Loudness | 7.17 ± 0.71 | 7.86 ± 0.90 | 0.071 | 0.29 (0.08–1.11) | 0.166 | 0.14 (0.01–2.26) | |
| Basal VAS Distress | 7.71 ± 6.49 | 7.67 ± 0.59 | 0.845 | 0.85 (0.16–4.43) | 0.556 | 3.36 (0.06–188.8) | |
| Improvement ≥ 20 in THI after 1-Month | |||||||
|---|---|---|---|---|---|---|---|
| Yes (N = 13) | No (N = 12) | Univariate Model | Multivariate Model | ||||
| p-Value | OR (IC 95%) | p-Value | OR Adjusted (IC 95%) | ||||
| Sex | Male | 4 (30.77) | 7 (58.33) | 0.171 | 0.32 (0.06–1.64) | 0.093 | 0.09 (0.01–1.50) |
| Female | 9 (69.23) | 5 (41.67) | 0.221 | 3.15 (0.61–16.31) | 0.093 | 11.17 (0.67–187.07) | |
| Mean ± SD | Mean ± SD | Univariate Model | Multivariate Model | ||||
| p-Value | OR (IC 95%) | p-Value | OR Adjusted (IC 95%) | ||||
| Age | 45.85 ± 8.63 | 49.34 ± 5.91 | 0.249 | 0.93 (0.83–1.05) | 0.694 | 0.97 (0.82–1.14) | |
| Tinnitus duration since its onset | 5.62 ± 2.99 | 9.5 ± 4.06 | 0.028 | 0.73 (0.55–0.97) | 0.027 | 0.60 (0.38–0.94) | |
| Basal THI | 72.54 ± 11.11 | 69.92 ± 10.26 | 0.529 | 1.03 (0.95–1.11) | 0.224 | 1.10 (0.94–1.28) | |
| Basal VAS Loudness | 7.15 ± 0.69 | 7.58 ± 0.90 | 0.191 | 0.48 (0.16–1.44) | 0.819 | 0.82 (0.16–4.30) | |
| Basal VAS Distress | 7.54 ± 0.66 | 7.83 ± 0.39 | 0.199 | 0.32 (0.06–1.81) | 0.120 | 0.08 (0.00–1.95) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yadollahpour, A.; Rashidi, S.; Saki, N.; Kunwar, P.S.; Mayo-Yáñez, M. Repeated Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: A Double-Blinded Randomized Controlled Clinical Trial. Brain Sci. 2024, 14, 373. https://doi.org/10.3390/brainsci14040373
Yadollahpour A, Rashidi S, Saki N, Kunwar PS, Mayo-Yáñez M. Repeated Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: A Double-Blinded Randomized Controlled Clinical Trial. Brain Sciences. 2024; 14(4):373. https://doi.org/10.3390/brainsci14040373
Chicago/Turabian StyleYadollahpour, Ali, Samaneh Rashidi, Nader Saki, Pramod Singh Kunwar, and Miguel Mayo-Yáñez. 2024. "Repeated Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: A Double-Blinded Randomized Controlled Clinical Trial" Brain Sciences 14, no. 4: 373. https://doi.org/10.3390/brainsci14040373
APA StyleYadollahpour, A., Rashidi, S., Saki, N., Kunwar, P. S., & Mayo-Yáñez, M. (2024). Repeated Bilateral Transcranial Direct Current Stimulation over Auditory Cortex for Tinnitus Treatment: A Double-Blinded Randomized Controlled Clinical Trial. Brain Sciences, 14(4), 373. https://doi.org/10.3390/brainsci14040373