


Exploring the Acute Effects of Immersive Virtual Reality Biking on Self-Efficacy and Attention of Individuals in the Treatment of Substance Use Disorders: A Feasibility Study

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
Research Questions and Hypotheses
2. Materials and Methods
2.1. Participants & Setting
2.2. Study Design
2.3. Ethics Approval and Consent to Participate
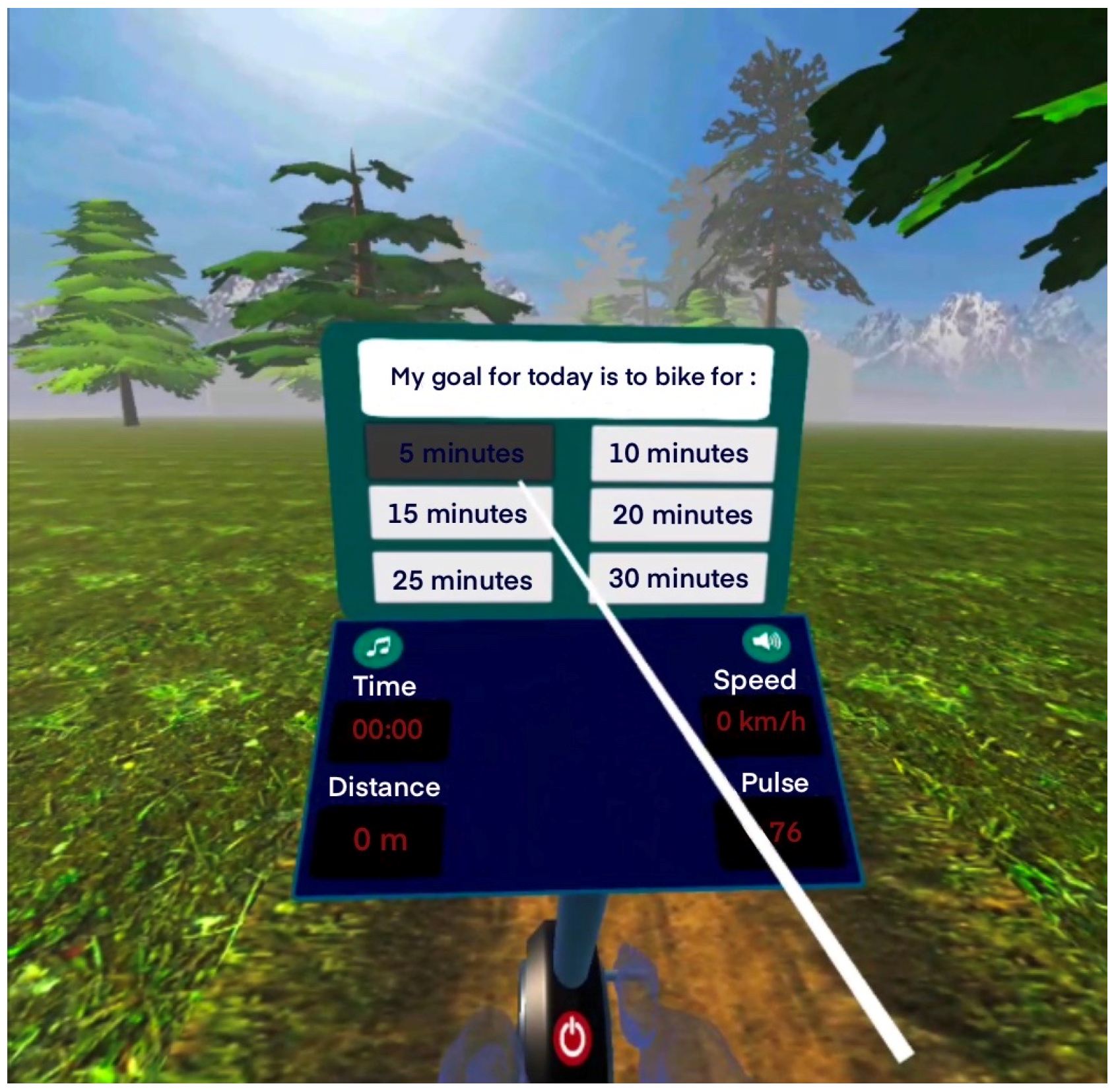
2.4. VR System
2.5. Procedure
2.6. Measures
2.7. Statistical Analysis
3. Results
3.1. Pre- and Post-VR Exercise Measures
3.1.1. Stroop Test
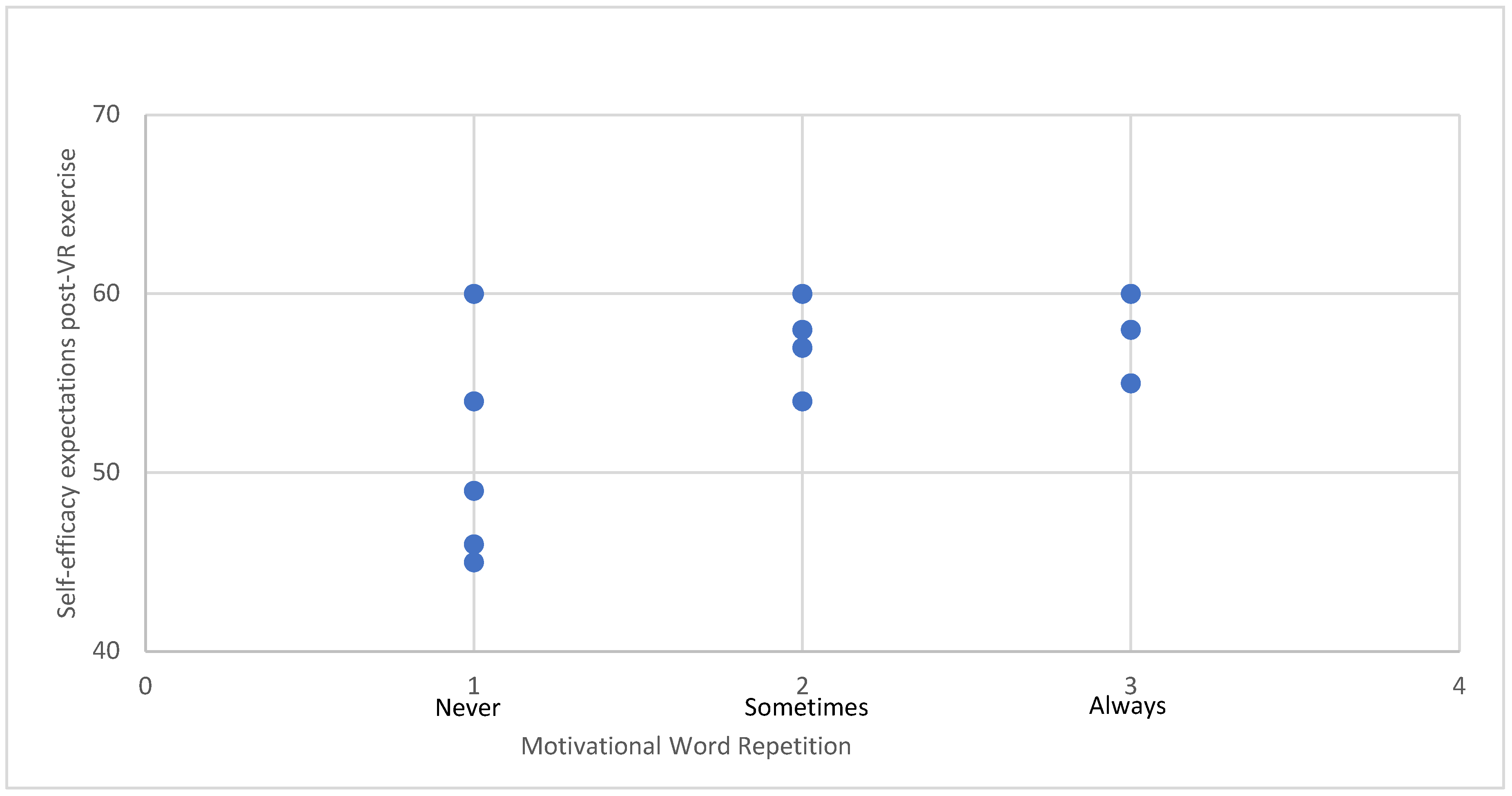
3.1.2. Self-Efficacy Expectations
3.2. Post-VR Exercise Measures
3.2.1. Attitudes, Intention for Future Use, Interest/Enjoyment
3.2.2. VR System Experience
3.2.3. VR Performance
3.3. Technical Functionality, User Experience, and Emotional Responses toward the VR Exercise System
4. Discussion
4.1. The Effects of VR Exercise on Self-Efficacy Expectations of Individuals in SUD Treatment
4.2. The Effects of VR Exercise on the Attentional Control of Individuals in SUD Treatment
4.3. The Attitudes, Intention for Future Use, and Interest/Enjoyment of Individuals in SUD Treatment toward VR Exercise
4.4. Practical Implications
4.5. Strengths & Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Office on Drugs and Crime. World Drug Report; United Nations Publication, Sales No. E.20.XI.6; United Nations: Vienna, Austria, 2020. [Google Scholar]
- Nestler, E.J. Cellular basis of memory for addiction. Dialogues Clin. Neurosci. 2013, 15, 431–443. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12, 652–669. [Google Scholar] [CrossRef]
- Gould, T.J. Addiction Science & Clinical Practice, Addiction and Cognition. Addict. Sci. Clin. Pract. 2010, 5, 4–14. [Google Scholar]
- Kutlu, M.G.; Gould, T.J. Effects of drugs of abuse on hippocampal plasticity and hippocampus-dependent learning and memory: Contributions to development and maintenance of addiction. Learn. Mem. 2016, 23, 515–533. [Google Scholar] [CrossRef]
- Ellingsen, M.M.; Johannesen, S.L.; Martinsen, E.W.; Dahl, S.R.; Hallgren, M. Effects of Acute Exercise on Drug Craving, Self-Esteem, Mood, and Affect in Adults with Polysubstance Use Disorder: Protocol for a Multicenter Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e18553. [Google Scholar] [CrossRef] [PubMed]
- Rethorst, C.D.; Henley, S.S.; Carmody, T.J.; Dela Cruz, A.; Greer, T.L.; Walker, R.; Trivedi, M. Moderators of treatment response to exercise in participants with stimulant use disorder: Results from the Stimulant Reduction Using Dosed Exercise (STRIDE) CTN0037 study. Ment. Health Phys. Act. 2021, 21, 100421. [Google Scholar] [CrossRef]
- Panagiotounis, F.; Hassandra, M.; Koutsoukou, A.; Theodorakis, Y. What about Sport and Physical Exercise in Substance Use Disorder Recovery? Perceptions of Individuals Undergoing SUD Recovery. Life Skills Development; RG Publishers: Athens, Greece, 2022. [Google Scholar] [CrossRef]
- Ding, K.; Li, H. Digital Addiction Intervention for Children and Adolescents: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 4777. [Google Scholar] [CrossRef]
- Piché, F.; Daneau, C.; Plourde, C.; Girard, S.; Romain, A.J. Characteristics and impact of physical activity interventions during substance use disorder treatment excluding tobacco: A systematic review. PLoS ONE 2023, 18, e0283861. [Google Scholar] [CrossRef] [PubMed]
- Caetano, T.; Pinho, M.S.; Ramadas, E.; Clara, C.; Areosa, T.; Dixe, M.d.A. Cognitive Training Effectiveness on Memory, Executive Functioning, and Processing Speed in Individuals with Substance Use Disorders: A Systematic Review. Front. Psychol. 2021, 12, 730165. [Google Scholar] [CrossRef] [PubMed]
- Brorson, H.H.; Arnevik, E.A.; Rand-Hendriksen, K.; Duckert, F. Drop-out from addiction treatment: A systematic review of risk factors. Clin. Psychol. Rev. 2013, 33, 1010–1024. [Google Scholar] [CrossRef]
- Lindsay, W.G. Attention in Psychology, Neuroscience, and Machine Learning. Front. Comput. Neurosci. 2020, 14, 29. [Google Scholar] [CrossRef]
- Chou, C.C.; Hsueh, M.C.; Chiu, Y.H.; Wang, W.Y.; Huang, M.Y.; Huang, C.J. Sustained Effects of Acute Resistance Exercise on Executive Function in Healthy Middle-Aged Adults. Front. Hum. Neurosci. 2021, 15, 684848. [Google Scholar] [CrossRef]
- Sanudo, B.; Abdi, E.; Bernardo-Filho, M.; Taiar, R. Aerobic Exercise with Superimposed Virtual Reality Improves Cognitive Flexibility and Selective Attention in Young Males. Appl. Sci. 2020, 10, 8029. [Google Scholar] [CrossRef]
- Haberstroh, C.; Weider, S.; Flemmen, G.; Loe, H.; Andersson, H.W.; Hallgren, M.; Mosti, M.P. The effect of high-intensity interval training on cognitive function in patients with substance use disorder: Study protocol for a two-armed randomized controlled trial. Front. Sports Act. Living 2022, 4, 954561. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Tao, W.; Peng, B.; Su, R.; Wang, D.; Hu, C.; Li, M.; Zhang, X.; Yang, Y.; Yu, S.; et al. Effects of a group-based aerobic exercise program on the cognitive functions and emotions of substance use disorder patients: A randomized controlled trial. Int. J. Ment. Health Addict. 2022, 20, 2349–2365. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Bonny-Noach, H.; Shapira, B.; Baumol, P.; Tadmor, N.; Rosca, P.; Shoshan, S.; Harel-Fisch, Y.; Caduri, A. Substance use, harm reduction attitudes and behaviors among attendees of nature rave parties in Israel. Harm Reduct. J. 2023, 20, 108. [Google Scholar] [CrossRef] [PubMed]
- Zemore, S.E.; Ajzen, I. Predicting substance abuse treatment completion using a new scale based on the theory of planned behavior. J. Subst. Abuse Treat. 2014, 46, 174–182. [Google Scholar] [CrossRef]
- Schwarzer, R. (Ed.) Self-Efficacy: Thought Control of Action; Routledge: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Kadden, R.M.; Litt, M.D. The role of self-efficacy in the treatment of substance use disorders. Addict. Behav. 2011, 36, 1120–1126. [Google Scholar] [CrossRef]
- Tate, S.R.; Wu, J.; McQuaid, J.R.; Cummins, K.; Shriver, C.; Krenek, M.; Brown, S.A. Comorbidity of substance dependence and depression: Role of life stress and self-efficacy in sustaining abstinence. Psychol. Addict. Behav. 2008, 22, 47–57. [Google Scholar] [CrossRef]
- Mohamed, S.M.; Hassan, S.S.; Abdelmonem, R.M. Relationship between Self-Efficacy, Social Support and Treatment Motivation among Addict Patients. Minia Sci. Nurs. J. 2022, 12, 106–113. [Google Scholar] [CrossRef]
- Nikmanesh, Z.; Baluchi, M.; Motlagh, A. The Role of Self-Efficacy Beliefs and Social Support on Prediction of Addiction Relapse. Int. J. High Risk Behav. Addict. 2017, 6, e21209. [Google Scholar] [CrossRef]
- Jia, D.; Zhang, K.; Xu, Y. The Relationship between Social Support and Relapse Tendency among Those Who Struggle with Drug Addiction: Multiple Mediators of Exercise Self-Efficacy and Health-Related Quality of Life. J. Drug Issues 2023, 54, 120–133. [Google Scholar] [CrossRef]
- Panagiotounis, F.; Hassandra, M.; Krommidas, C.; Theodorakis, Y. Effects of an exercise theory-based intervention program on craving during the early stage of adults’ SUD treatment. Ment. Health Phys. Act. 2022, 23, 100463. [Google Scholar] [CrossRef]
- VirtualSpeech. VR Applications. VirtualSpeech. Available online: https://virtualspeech.com/blog/vr-applications (accessed on 6 July 2024).
- Freina, L.; Ott, M. A Literature Review on Immersive Virtual Reality in Education: State of the Art and Perspectives. In the International Scientific Conference eLearning and Software for Education; “Carol I” National Defence University: București, Romania, 2015; Volume 1, pp. 133–141. [Google Scholar] [CrossRef]
- Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.; Zhu, Z.; Wu, B.; McConnell, E.S. Technology-based cognitive training and rehabilitation interventions for individuals with mild cognitive impairment: A systematic review. BMC Geriatr. 2018, 18, 213. [Google Scholar] [CrossRef] [PubMed]
- Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Mouzakidis, C.; Karathanasi, E.M.; Petridou, N.; Tsolaki, M.; Zikas, P.; Evangelou, G.; et al. A Virtual Reality App for Physical and Cognitive Training of Older People with Mild Cognitive Impairment: Mixed Methods Feasibility Study. JMIR Serious Games 2021, 9, e24170. [Google Scholar] [CrossRef] [PubMed]
- Krommidas, C.; Galanis, E.; Tzormpatzakis, E.; Hassandra, M.; Hatzigeorgiadis, A.; Morres, I.D.; Comoutos, N.; Theodorakis, Y. The Effects of Acute Exercise and Virtual Reality Tasks on Children’s Memory Function and Exercise Preference. Int. J. Kinesiol. Sports Sci. 2022, 10, 7–17. [Google Scholar] [CrossRef]
- Mazza, M.; Kammler-Sucker, K.; Lemenager, T.; Kiefer, F.; Lenz, B. Virtual reality: A powerful technology to provide novel insight into treatment mechanisms of addiction. Transl. Psychiatry 2021, 11, 617. [Google Scholar] [CrossRef]
- Touloudi, E.; Hassandra, M.; Galanis, E.; Goudas, M.; Theodorakis, Y. Applicability of an Immersive Virtual Reality Exercise Training System for Office Workers during Working Hours. Sports 2022, 10, 104. [Google Scholar] [CrossRef]
- Baldimtsi, E.; Mouzakidis, C.; Karathanasi, E.M.; Verykouki, E.; Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Zikas, P.; Evangelou, G.; et al. Effects of Virtual Reality Physical and Cognitive Training Intervention on Cognitive Abilities of Elders with Mild Cognitive Impairment. J. Alzheimers Dis. Rep. 2023, 7, 1475–1490. [Google Scholar] [CrossRef] [PubMed]
- Ochi, G.; Kuwamizu, R.; Fujimoto, T.; Ikarashi, K.; Yamashiro, K.; Sato, D. The Effects of Acute Virtual Reality Exergaming on Mood and Executive Function: Exploratory Crossover Trial. JMIR Serious Games 2022, 10, e38200. [Google Scholar] [CrossRef] [PubMed]
- Knight, K.; Simpson, D.D.; Hiller, M.L. Screening and referral for substance-abuse treatment in the criminal justice system. In Treatment of Drug Offenders: Policies and Issues; Leukefeld, C.G., Tims, F., Farabee, D., Eds.; Springer: New York, NY, USA, 2002; pp. 259–272. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Guide for constructing self-efficacy scales. In Self-Efficacy Beliefs of Adolescents; Pajares, F., Urdan, T., Eds.; Information Age Publishing: Charlotte, NC, USA, 2006; pp. 307–337. [Google Scholar]
- Theodorakis, Y. The influence of goals, commitment and self-efficacy on motor performance. J. Appl. Sport Psychol. 1996, 8, 171–182. [Google Scholar] [CrossRef]
- MacLeod, C.M. Half a century of research on the Stroop effect: An integrative review. Psychol. Bull. 1991, 109, 163–203. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. Constructing a TPB Questionnaire: Conceptual and Methodological Considerations; Department of Psychology, University of Amherst: Amherst, MA, USA, 2002; Archived by WebCite®; Available online: http://www.webcitation.org/66zom97zq (accessed on 15 March 2023).
- Goudas, M.; Dermitzaki, I.; Bagiatis, K. Predictors of student’s intrinsic motivation in school physical education. Eur. J. Psychol. Educ. 2000, 15, 271–280. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Panagiotounis, F.; Theodorakis, Y.; Hassandra, M.; Morres, I. Psychological effects of an adventure therapy program in the treatment of substance use disorders: A Greek pilot study. J. Subst. Use 2020, 26, 118–124. [Google Scholar] [CrossRef]
- Smith, A.L.; Jones, R.; Cooper, S.J.; Karageorghis, C.I.; Heather, N. Effects of a virtual reality exercise program on cognitive function and quality of life in individuals undergoing substance use disorder treatment. J. Subst. Abuse Treat. 2021, 128, 108410. [Google Scholar]
- Zimmer, P.; Stritt, C.; Bloch, W.; Schmidt, F.-P.; Hübner, S.T.; Binnebößel, S.; Schenk, A.; Oberste, M. The effects of different aerobic exercise intensities on serum serotonin concentrations and their association with Stroop task performance: A randomized controlled trial. Eur. J. Appl. Physiol. 2016, 116, 2025–2034. [Google Scholar] [CrossRef]
- Yin, Y.; Yang, S.; Xiao, K.; Wang, T.; Wang, J.; Schöllhorn, W.I.; Zhu, D.; Pang, X. Comparison of the acute effects of Tai chi versus high-intensity interval training on inhibitory control in individuals with substance use disorder. Front. Psychol. 2022, 13, 941719. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.C.; Woods, S.P.; Matt, G.E.; Meyer, R.A.; Heaton, R.K.; Atkinson, J.H.; Grant, I. Neurocognitive effects of methamphetamine: A critical review and meta-analysis. Neuropsychol. Rev. 2007, 17, 275–297. [Google Scholar] [CrossRef]
- Verdejo-García, A.; Pérez-García, M.; Bechara, A. Emotion, decision-making and substance dependence: A somatic-marker model of addiction. Curr. Neuropharmacol. 2006, 4, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, T. Cognitive consequences of cannabis use: Comparison with abuse of stimulants and heroin, with regard to attention, memory, and executive functions. Pharmacol. Biochem. Behav. 2005, 81, 319–330. [Google Scholar] [CrossRef]
- Teixeira, P.; Marques, M.M.; Hagger, M.S.; Silva, M.; Brunet, J.; Duda, J.; Haerens, L.; La Guardia, J.; Lindwall, M.; Lonsdale, C.; et al. Classification of Techniques Used in Self-Determination Theory-Based Interventions in Health Contexts: An Expert Consensus Study; Academic Bibliography: Ghent, Belgium, 2019. [Google Scholar] [CrossRef]
- Nesbitt, K.V.; Kolodziejczyk, K.; Hoelzle, J.B.; Bruening, D.A. Immersive exercise in substance use disorder treatment: The intersection of technology, health, and clinical care. Subst. Abus. 2020, 41, 174–179. [Google Scholar] [CrossRef]
- Fleming, T.M.; de Beurs, D.; Khazaal, Y.; Gaggioli, A.; Riva, G.; Botella, C.; Baños, R.M.; Aschieri, F.; Bavin, L.M.; Kleiboer, A.; et al. Maximizing the Impact of e-Therapy and Serious Gaming: Time for a Paradigm Shift. Front. Psychiatry 2016, 7, 65. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Keshavarz, M.; Bahrani, M.; Ardabili, H.E.; Habibi, D. The effect of virtual reality cognitive-motor exercises on executive functions in individuals with substance use disorder. J. Subst. Use 2020, 25, 174–179. [Google Scholar]
- Worley, J. Virtual Reality for Individuals with Substance Use Disorders. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 15–19. [Google Scholar] [CrossRef]
- Asadzadeh, A.; Samad-Soltani, T.; Salahzadeh, Z.; Rezaei-Hachesu, P. Effectiveness of virtual reality-based exercise therapy in rehabilitation: A scoping review. Inform. Med. Unlocked 2021, 24, 100562. [Google Scholar] [CrossRef]
- Furzer, B.; Rebar, A.; Dimmock, J.A.; More, A.; Thornton, A.L.; Wright, K.; Colthart, A.; Jackson, B. Exercise is medicine… when you enjoy it: Exercise enjoyment, relapse prevention efficacy, and health outcomes for youth within a drug and alcohol treatment service. Psychol. Sport Exerc. 2021, 52, 101800. [Google Scholar] [CrossRef]
- Verdejo-Garcia, A.; Garcia-Fernandez, G.; Dom, G. Cognition and addiction. Dialogues Clin. Neurosci. 2019, 21, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Abrantes, A.M.; Blevins, C.E. Exercise in the context of substance use treatment: Key issues and future directions. Curr. Opin. Psychol. 2019, 30, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.; Brice, C.; Craig, C.; Penri-Jones, R. Effects of caffeine, practice, and mode of presentation on Stroop task performance. Pharmacol. Biochem. Behav. 1996, 54, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Sibley, B.A.; Etnier, J.L.; Le Masurier, G.C. Effects of an Acute Bout of Exercise on Cognitive Aspects of Stroop Performance. J. Sport Exerc. Psychol. 2006, 28, 285–299. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 20 | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|
| Age | Years | 37.75 | 8.33 | 24 | 54 |
| Sex | Male, % | 90 | - | - | - |
| Educational level | Primary, % Secondary, % | 85% secondary 10% primary | - | - | - |
| Exercise during treatment | Yes, % | 50 | - | - | - |
| Current engagement in SUDs treatment | Days | 138.8 | 106.25 | 6 | 341 |
| Previous attempts | Times | 1.80 | 1.642 | 0 | 4 and more |
| Frequency (%) | Never 35% 1 time 15% 2 times 5% 3 times 25% 4 plus 20% | ||||
| Drug use | Years | 19.4 | 9.88 | 7 | 37 |
| Pre-VR Exercise | Post-VR Exercise | |
|---|---|---|
| Self-selected duration VR exercise |
|
| Stroop Test | Pre VR | Post VR | p Value, df | Cohen’s d | |
|---|---|---|---|---|---|
| Naming | Reaction time | 60.9 ± 13.1 | 51.9 ± 7.6 | t(19) = 4.178, p < 0.001 | 0.84 |
| Mistakes | 1.1 ± 1.2 | 0.6 ± 0.9 | t(19) = 1.308, p = 0.21 | ||
| Reading | Reaction time | 41.9 ± 5.4 | 40.2 ± 6.2 | t(19) = 3.202, p < 0.005 | 0.29 |
| Mistakes | 0.1 ± 0.2 | 0.1 ± 0.2 | t(19) = 0.152, p = 1.0 | ||
| Interference | Reaction time | 94.8 ± 22.9 | 78.0 ± 14.1 | t(19) = 6.242, p < 0.001 | 0.88 |
| Mistakes | 4.4 ± 4.1 | 2.6 ± 0.7 | t(19) = 1.966, p = 0.06. | ||
| Self-efficacy expectations | 49.8 ± 13.19 | 56.8 ± 4.87 | t(19) = −2.78, p < 0.01 | - | |
| Main Theme | Subthemes | N | (%) |
|---|---|---|---|
| Reasons to use VRADA | Why would you use VRADA? | ||
| It is pleasant | 14 | 70% | |
| It is relaxing | 8 | 40% | |
| It is motivating | 3 | 15% | |
| Usability or utilization | General difficulties | ||
| None | 16 | 80% | |
| Difficulty adjusting to the speed limits | 3 | 15% | |
| Technical issues | |||
| None | 20 | 100% | |
| Joystick use difficulty | |||
| No | 20 | 100% | |
| VR mask use difficulties | |||
| None | 16 | 80% | |
| It was a little heavy | 2 | 10% | |
| It was a little tight | 2 | 10% | |
| Usability or learning | Need more time to understand the system | ||
| No | 20 | 100% | |
| Usability or pleasantness | Most enjoyable parts | ||
| The VR environment (landscape) | 15 | 75% | |
| Music | 3 | 15% | |
| Peacefulness and relaxation | 3 | 15% | |
| Least enjoyable parts | |||
| Repeated virtual parts, monotonous | 9 | 45% | |
| Graphics | 8 | 40% | |
| Music | 5 | 25% | |
| Feel uncomfortable | |||
| No | 20 | 100% | |
| Sense of presence or engagement | Distraction of attention | ||
| No | 19 | 95% | |
| Yes | 1 | 5% | |
| Duration of the experience | |||
| It could be more | 10 | 50% | |
| It was enough | 7 | 35% | |
| It could be more but I did not have time because of our demanding schedule | 3 | 15% | |
| Sense of presence or realism | VR environment was realistic or artificial | ||
| Artificial | 20 | 100% | |
| Tolerability | Feel bad during training | ||
| Νο | 20 | 100% | |
| Thinking of weird things | |||
| Νο | 20 | 100% | |
| Nausea, dizziness or other physical symptoms | |||
| Νο | 19 | 95% | |
| A little for the first seconds | 1 | 5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Touloudi, E.; Hassandra, M.; Stavrou, V.T.; Panagiotounis, F.; Galanis, E.; Goudas, M.; Theodorakis, Y. Exploring the Acute Effects of Immersive Virtual Reality Biking on Self-Efficacy and Attention of Individuals in the Treatment of Substance Use Disorders: A Feasibility Study. Brain Sci. 2024, 14, 724. https://doi.org/10.3390/brainsci14070724
Touloudi E, Hassandra M, Stavrou VT, Panagiotounis F, Galanis E, Goudas M, Theodorakis Y. Exploring the Acute Effects of Immersive Virtual Reality Biking on Self-Efficacy and Attention of Individuals in the Treatment of Substance Use Disorders: A Feasibility Study. Brain Sciences. 2024; 14(7):724. https://doi.org/10.3390/brainsci14070724
Chicago/Turabian StyleTouloudi, Evlalia, Mary Hassandra, Vasileios T. Stavrou, Fotis Panagiotounis, Evangelos Galanis, Marios Goudas, and Yannis Theodorakis. 2024. "Exploring the Acute Effects of Immersive Virtual Reality Biking on Self-Efficacy and Attention of Individuals in the Treatment of Substance Use Disorders: A Feasibility Study" Brain Sciences 14, no. 7: 724. https://doi.org/10.3390/brainsci14070724
APA StyleTouloudi, E., Hassandra, M., Stavrou, V. T., Panagiotounis, F., Galanis, E., Goudas, M., & Theodorakis, Y. (2024). Exploring the Acute Effects of Immersive Virtual Reality Biking on Self-Efficacy and Attention of Individuals in the Treatment of Substance Use Disorders: A Feasibility Study. Brain Sciences, 14(7), 724. https://doi.org/10.3390/brainsci14070724