
Can a Two-Dose Influenza Vaccine Regimen Better Protect Older Adults? An Agent-Based Modeling Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Inputs
2.2. Model Structure
2.3. Vaccination Simulation Base Model Scenarios
2.4. Additional Scenario Analyses
2.5. Comparison to Prior Models
3. Results
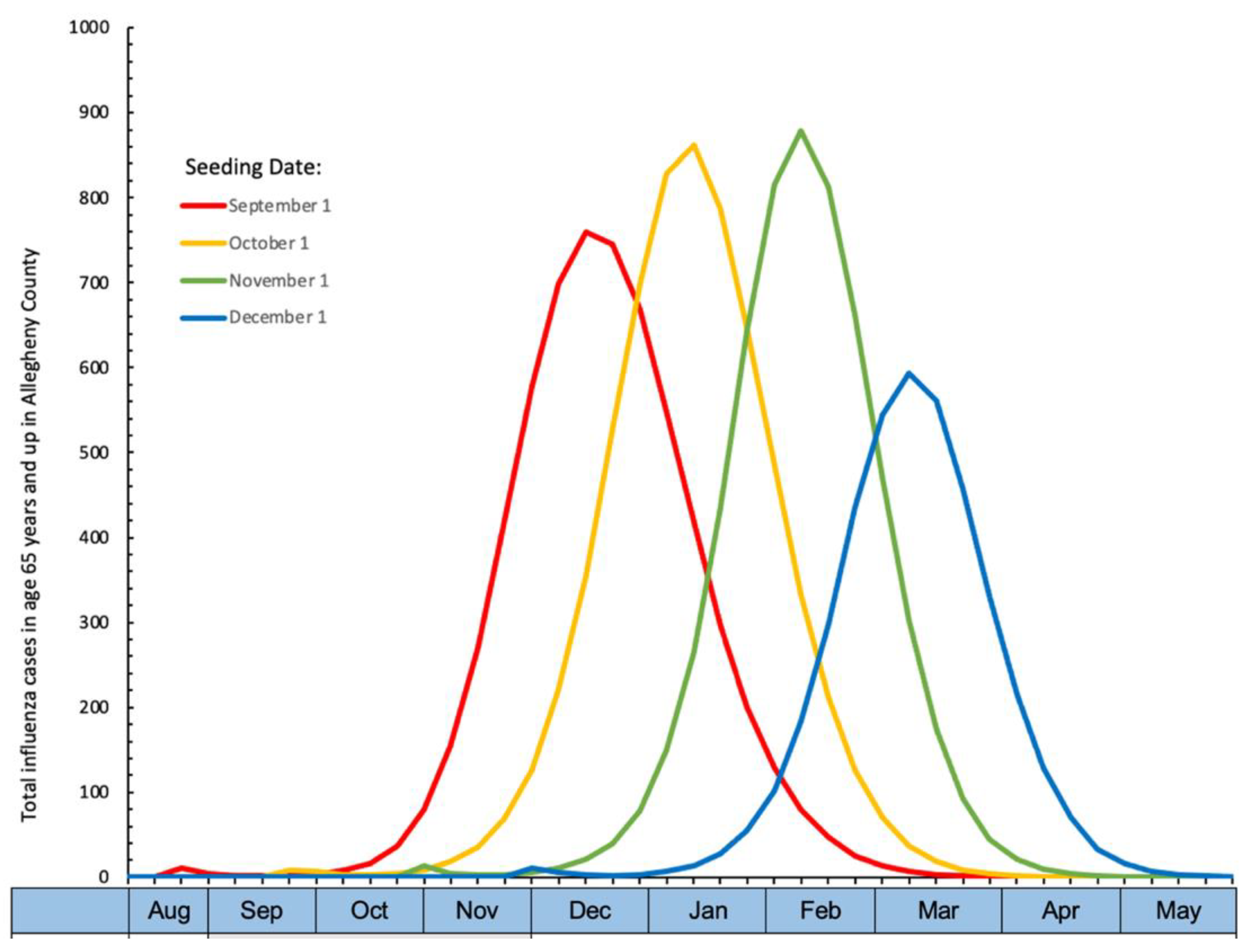
3.1. Base Model
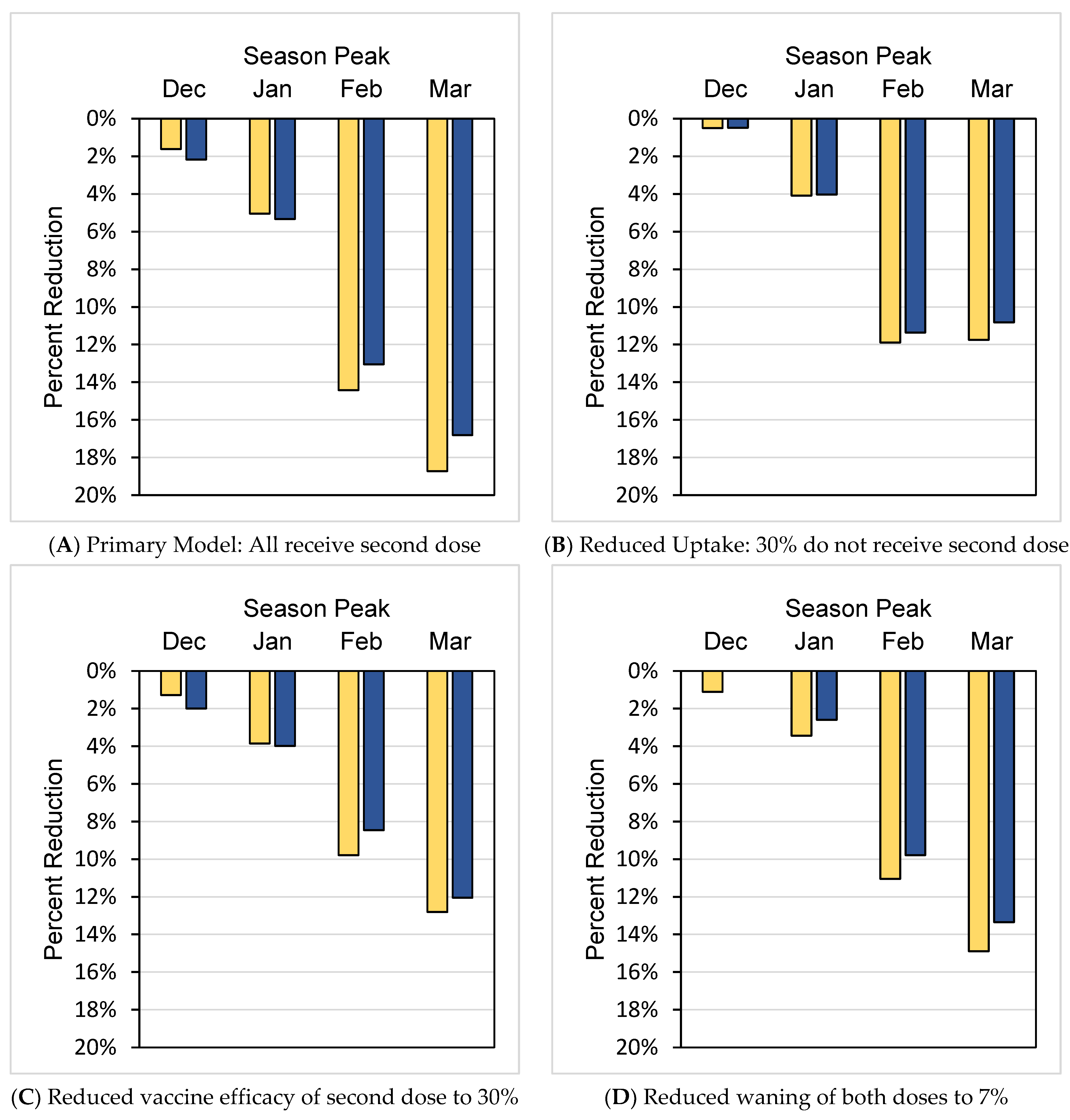
3.2. Scenario Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control. Flu Vaccination Coverage, United States, 2019–2020 Influenza Season. Available online: https://www.cdc.gov/flu/fluvaxview/coverage-1920estimates.htm (accessed on 25 May 2021).
- Centers for Disease Control and Prevention. Influenza (Flu), Adults 65 & Over. Available online: https://www.cdc.gov/flu/highrisk/65over.htm#:~:text=In%20recent%20years%2C%20for (accessed on 27 July 2022).
- Centers for Disease Control and Prevention. Influenza (Flu), When is Flu Season. Available online: https://www.cdc.gov/flu/about/season/flu-season.htm (accessed on 27 July 2022).
- Ferdinands, J.M.; Gaglani, M.; Martin, E.T.; Monto, A.S.; Middleton, D.; Silveira, F.; Talbot, H.K.; Zimmerman, R.; Patel, M. Waning Vaccine Effectiveness Against Influenza-Associated Hospitalizations Among Adults, 2015–2016 to 2018–2019, United States Hospitalized Adult Influenza Vaccine Effectiveness Network. Clin. Infect. Dis. 2021, 73, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Influenza Vaccination Coverage for Persons 6 Months and Older. Available online: https://www.cdc.gov/flu/fluvaxview/interactive-general-population.htm (accessed on 27 July 2022).
- Ferdinands, J.M.; Fry, A.M.; Reynolds, S.; Petrie, J.; Flannery, B.; Jackson, M.L.; Belongia, E.A. Intraseason waning of influenza vaccine protection: Evidence from the US Influenza Vaccine Effectiveness Network, 2011–2012 through 2014–2015. Clin. Infect. Dis. 2017, 64, 544–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauland, M.G.; Galloway, D.D.; Raviotta, J.M.; Zimmerman, R.K.; Roberts, M.S. Impact of Low Rates of Influenza on Next-Season Influenza Infections. Am. J. Prev. Med. 2022, 62, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Grefenstette, J.J.; Galloway, D.; Albert, S.M.; Burke, D.S. Policies to reduce influenza in the workplace: Impact assessments using an agent-based model. Am. J. Public Health 2013, 103, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Piper, K.; Galloway, D.D.; Hadler, J.L.; Grefenstette, J.J. Is population structure sufficient to generate area-level inequalities in influenza rates? An examination using agent-based models. BMC Public Health 2015, 15, 947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grefenstette, J.J.; Brown, S.T.; Rosenfeld, R.; DePasse, J.; Stone, N.T.; Cooley, P.C.; Wheaton, W.D.; Fyshe, A.; Galloway, D.D.; Sriram, A.; et al. FRED (a Framework for Reconstructing Epidemic Dynamics): An open-source software system for modeling infectious diseases and control strategies using census-based populations. BMC Public Health 2013, 13, 940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, S.J.; Miller, J.C.; Meyers, L.A. Seasonality in risk of pandemic influenza emergence. PLoS Comput. Biol. 2017, 13, e1005749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Lofgren, E.; Fefferman, N.H.; Naumov, Y.N.; Gorski, J.; Naumova, E.N. Influenza seasonality: Underlying causes and modeling theories. J. Virol. 2007, 81, 5429–5436. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Estimated Influenza Disease Burden, by Season. Available online: https://www.cdc.gov/flu/about/burden/past-seasons.html (accessed on 28 July 2022).
- Centers for Disease Control and Prevention. FLUVIEW Interactive, Laboratory-Confirmed Influenza Hospitalizations. Available online: https://gis.cdc.gov/GRASP/Fluview/FluHospRates.html (accessed on 28 July 2022).
- Czaja, C.A.; Miller, L.; Alden, N.; Wald, H.L.; Cummings, C.N.; Rolfes, M.A.; Anderson, E.J.; Bennett, N.M.; Billing, L.M.; Chai, S.J.; et al. Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes among Older Adults Hospitalized with Influenza-U.S. Influenza Hospitalization Surveillance Network (FluSurv-NET). Open Forum Infect. Dis. 2019, 6, ofz225. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Past Seasons Vaccine Effectiveness Estimates. Available online: https://www.cdc.gov/flu/vaccines-work/past-seasons-estimates.html (accessed on 28 July 2022).
- Ferdinands, J.M.; Alyanak, E.; Reed, C.; Fry, A.M. Waning of Influenza Vaccine Protection: Exploring the Trade-offs of Changes in Vaccination Timing among Older Adults. Clin. Infect. Dis. 2020, 70, 1550–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.J.; France, G.; Nowalk, M.P.; Raviotta, J.M.; DePasse, J.; Wateska, A.; Shim, E.; Zimmerman, R.K. Compressed Influenza Vaccination in U.S. Older Adults: A Decision Analysis. Am. J. Prev. Med. 2019, 56, e135–e141. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Estimated Flu Disease Burden, by Age Group—United States, 2019–2020 Flu Season. Available online: https://www.cdc.gov/flu/about/burden/2019-2020.html (accessed on 28 July 2022).
- Centers for Disease Control and Prevention. Influenza (Flu), General Population Vaccination Coverage. Available online: https://www.cdc.gov/flu/fluvaxview/coverage-1920estimates.htm#figure7 (accessed on 27 July 2022).
- Centers for Disease Control and Prevention. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States, 2021–2022. Available online: https://www.cdc.gov/flu/professionals/acip/summary/summary-recommendations.htm (accessed on 22 September 2021).
- Belongia, E.A.; Skowronski, D.M.; McLean, H.Q.; Chambers, C.; Sundaram, M.E.; De Serres, G. Repeated annual influenza vaccination and vaccine effectiveness: Review of evidence. Expert Rev. Vaccines 2017, 16, 723–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellebedy, A.H. Immunizing the Immune: Can We Overcome Influenza’s Most Formidable Challenge? Vaccines 2018, 6, 68. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control. Disease Burden of Influenza. Available online: https://www.cdc.gov/flu/about/burden/index.html (accessed on 30 June 2021).
- Centers for Disease Control and Prevention. CDC Director Adopts Preference for Specific Flu Vaccines for Seniors. Available online: https://www.cdc.gov/media/releases/2022/s0630-seniors-flu.html (accessed on 17 August 2022).

{kind=link}
{kind=link}
| Model | Aug | Sep | Oct | Nov | Dec | Jan | Feb | Mar | Apr | May |
|---|---|---|---|---|---|---|---|---|---|---|
| Range of Season Peaks | ||||||||||
| Single Dose | Dose 1, normal distribution starts 1 Sep | |||||||||
| Two Dose | Dose 1, normal distribution starts 1 Sep | Dose 2, 90 days after dose 1 | ||||||||
| Season Peak | Age 65–74 Years | Age 75–84 Years | Age 85 and up | Overall: Age 65 and up |
|---|---|---|---|---|
| December | ||||
| One dose | 4006 (3787, 4259) | 2394 (2251, 2511) | 1568 (1398, 1729) | 3010 (2860, 3156) |
| Two doses | 3936 (3745, 3931) | 2375 (2215, 2508) | 1542 (1381, 1717) | 2962 (2849, 3116) |
| January | ||||
| One dose | 4221 (4024, 4416) | 2477 (2337, 2689) | 1585 (1449, 1789) | 3144 (3021, 3293) |
| Two doses | 3985 (3791, 4191) | 2373 (2193, 2548) | 1523 (1398, 1701) | 2985 (2836, 3108) |
| February | ||||
| One dose | 3932 (3629, 4190) | 2215 (1956, 2326) | 1391 (1220, 1608) | 2880 (2644, 3094) |
| Two doses | 3312 (2850, 3670) | 1938 (1648, 2165) | 1242 (1033, 1422) | 2465 (2104, 2735) |
| March | ||||
| One dose | 2751 (2194, 3305) | 1493 (1099, 1804) | 916 (686, 1132) | 1985 (1577, 2382) |
| Two doses | 2190 (1691, 2617) | 1249 (942, 1519) | 793 (587, 1024) | 1613 (1242, 1931) |
| Season Peak | Age 65–74 Years | Age 75–84 Years | Age 85 and up | Overall: Age 65 and up |
|---|---|---|---|---|
| December | ||||
| One dose | 247 (212, 283) | 297 (261, 334) | 473 (393, 554) | 302 (296, 311) |
| Two doses | 240 (209, 268) | 291 (254, 335) | 466 (375, 545) | 295 (270, 31,937) |
| January | ||||
| One dose | 260 (225, 299) | 307 (270, 354) | 480 (396, 572) | 313 (285, 341) |
| Two doses | 244 (210, 278) | 291 (256, 330) | 457 (377, 555) | 296 (273, 323) |
| February | ||||
| One dose | 243 (200, 279) | 277 (230, 327) | 416 (342, 500) | 283 (249, 315) |
| Two doses | 207 (169, 254) | 243 (190, 290) | 370 (275, 443) | 246 (198, 283) |
| March | ||||
| One dose | 171 (126, 216) | 186 (133, 250) | 277 (183, 381) | 194 (145, 246) |
| Two doses | 137 (95, 169) | 159 (110, 214) | 237 (165, 311) | 161 (118, 196) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams, K.V.; Krauland, M.G.; Harrison, L.H.; Williams, J.V.; Roberts, M.S.; Zimmerman, R.K. Can a Two-Dose Influenza Vaccine Regimen Better Protect Older Adults? An Agent-Based Modeling Study. Vaccines 2022, 10, 1799. https://doi.org/10.3390/vaccines10111799
Williams KV, Krauland MG, Harrison LH, Williams JV, Roberts MS, Zimmerman RK. Can a Two-Dose Influenza Vaccine Regimen Better Protect Older Adults? An Agent-Based Modeling Study. Vaccines. 2022; 10(11):1799. https://doi.org/10.3390/vaccines10111799
Chicago/Turabian StyleWilliams, Katherine V., Mary G. Krauland, Lee H. Harrison, John V. Williams, Mark S. Roberts, and Richard K. Zimmerman. 2022. "Can a Two-Dose Influenza Vaccine Regimen Better Protect Older Adults? An Agent-Based Modeling Study" Vaccines 10, no. 11: 1799. https://doi.org/10.3390/vaccines10111799
APA StyleWilliams, K. V., Krauland, M. G., Harrison, L. H., Williams, J. V., Roberts, M. S., & Zimmerman, R. K. (2022). Can a Two-Dose Influenza Vaccine Regimen Better Protect Older Adults? An Agent-Based Modeling Study. Vaccines, 10(11), 1799. https://doi.org/10.3390/vaccines10111799