Abstract
(1) Background: We describe a case of a 58-year-old Chinese woman, without obvious cause of immunosuppression, who developed cytomegalovirus (CMV) proctitis three days after a second COVID-19 vaccination. Electronic colonoscopy revealed a new lesion that was circumferential at the anorectal junction, with an uneven surface and ulceration, which mimicked rectal carcinoma. This is the first case of CMV proctitis following vaccination since the invention of the COVID-19 vaccine, suggesting that the COVID-19 vaccine may cause disorders of immune homeostasis, including not only immune hyperactivity but also immune deficiency. We report this case to increase readers’ awareness of the risks after COVID-19 vaccination and to provide new ideas for the diagnosis and treatment of similar cases. (2) Methods: In this case, we used laboratory biochemical examinations, colonoscopy, immunohistochemistry, and a biochemical index to confirm the existence of CMV proctitis. (3) Results: In this case, the vaccine-induced CMV proctitis had a similar endoscopic appearance to rectal neoplastic lesions, which could be confirmed by biopsy and quickly relieved by ganciclovir treatment. Ganciclovir was used to treat the patient, and a good effect was observed. (4) Conclusions: COVID-19 vaccination may cause immune disorders, not just immune hyperactivity as previously reported, but also immune deficiency, such as CMV proctitis in this case. The clinical course of CMV proctitis secondary to COVID-19 vaccination was favorable with ganciclovir therapy.
1. Introduction
The COVID-19 epidemic is still raging over the globe, and vaccination is supposed to help us overcome it. The Chinese Center for Disease Control and Prevention (CCDC) has approved three forms of COVID-19 vaccines: inactivated vaccines (Sinopharm, Sinovac, etc.), recombinant vaccines (Chinese hamster ovary cells), and viral vector vaccines (adenovirus type 5 vector). Although the vaccinations’ efficacy is undeniable, their safety is still a concern. The advent of novel vaccines currently seems to be altering the course of events in a favorable direction. Along with the clear benefits stemming from the vaccination programs in many countries, side effects of these vaccines remain a concern that must be addressed. Hence, the recent reports of effective and safe vaccines were welcomed with great joy [1]. There have been a number of previous reports suggesting that COVID-19 vaccines may cause damage to multiple systems, most of which is caused by immune hyperactivity. A variety of mechanisms have been proposed to contribute to the rise in acute autoimmune responses [2]. As recently shown by Vorjani et al., molecular mimicry, i.e., antibodies against SARS-CoV-2 spike glycoproteins cross-reacting with structurally similar host peptide protein sequences, could play an important role in this response [3]. However, there are still some reports of immune-deficiency diseases such as herpes zoster virus and herpes simplex virus reactivation [4,5,6,7,8,9]. Although the mechanism of herpes zoster virus reactivation is elusive, the idea that some adjuvants in the vaccine may result in T-cell dysfunction is a reasonable guess. We reported a case of a 58-year-old Chinese woman, without obvious cause of immunosuppression, who developed persistent constipation three days after the second COVID-19 vaccination, and was eventually diagnosed with CMV proctitis that mimicked a rectal tumor under colonoscopy, which is the first case of post-vaccination immune-deficiency disease found in the digestive system. However, since its treatment with ganciclovir is highly effective, this should not distract us from the overwhelming benefits of COVID-19 vaccination.
2. Case Presentation
A 57-year-old Chinese woman suffered from constipation for several weeks after receiving her second dose of the CoronaVac COVID-19 vaccine. She was previously healthy. Further examination of the medical history revealed that the patient had difficulty defecating three days after the second injection of the COVID-19 vaccine in the community two weeks ago, accompanied by a feeling of perianal discomfort and abdominal distention. There was no obvious bloody stool or melena, and a colonoscopy at the local hospital indicated a chronic inflammatory reaction of the rectal mucosa. She denied any previous history of blood transfusion or anal intercourse. No diseases were recorded in her past medical history.
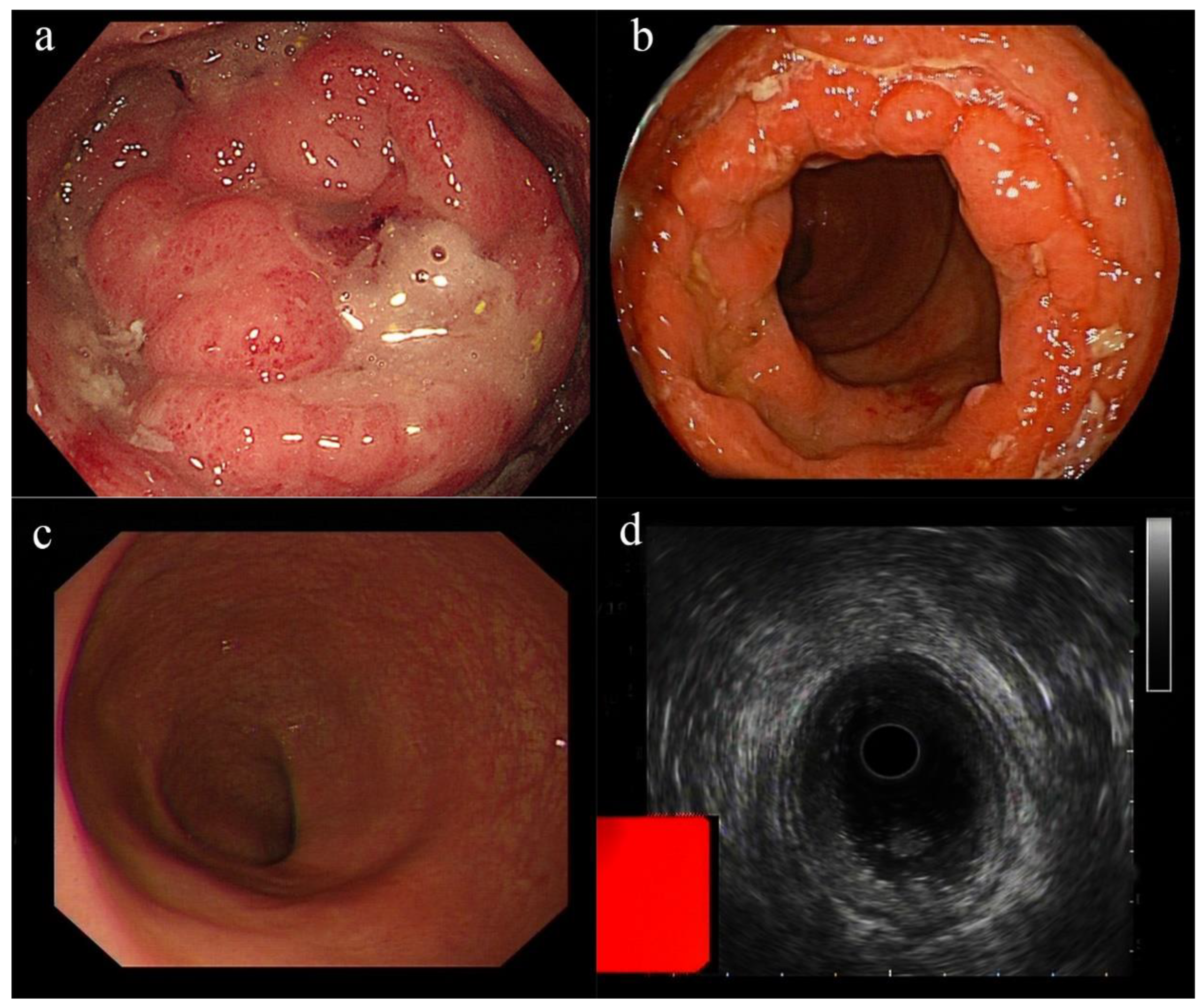
A digital examination revealed a firm deformity over the posterior rectal wall. The ESR, CRP, and WBC were all within the normal limits. A stool routine examination showed a positive occult blood test (+). An anti-HIV and PCR test for COVID-19 were negative. We performed a colonoscopy on the second day of admission, revealing a new lesion that was circumferential at the anorectal junction, with an uneven surface and ulceration, which mimicked rectal carcinoma (Figure 1a). Further tests for tumor markers such as CEA, CA199, and CA125 were performed and found no abnormalities. Several biopsies were removed for further pathological examination. Pelvic enhanced rectal MRI revealed diffuse mucosal thickening in the middle and lower rectum, with limited diffusion of the contrast agent. Ultrasound colonoscopy showed that the lesion was confined to the mucosal layer, with intact mucosal muscular tissue and without invasion of the muscularis propria (Figure 1d). Subsequent liver MRI was performed to rule out the presence of tumor metastases, demonstrating a hepatic hemangioma of the lower right posterior lobe and liver cyst.
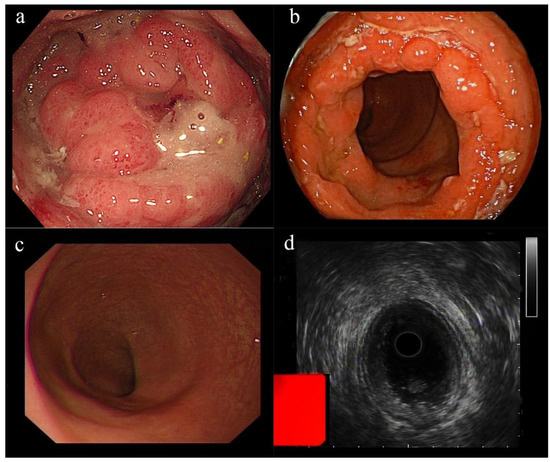
Figure 1.
Proctosigmoidoscopy appearance: (a) A new lesion that mimicked rectal carcinoma at the anorectal junction. The surrounding mucosa was edemic and ulcerated. (b) Colonoscopy after treatment with ganciclovir showed shrinkage of the lesion. (c) A follow-up colonoscopy performed after 28 days of ganciclovir treatment revealed that the lesion had completely recovered. (d) Ultrasound colonoscopy revealed the lesion was confined to the mucosal layer, without extending beyond the mucosal muscular tissue, as the muscularis propria appeared to be intact.
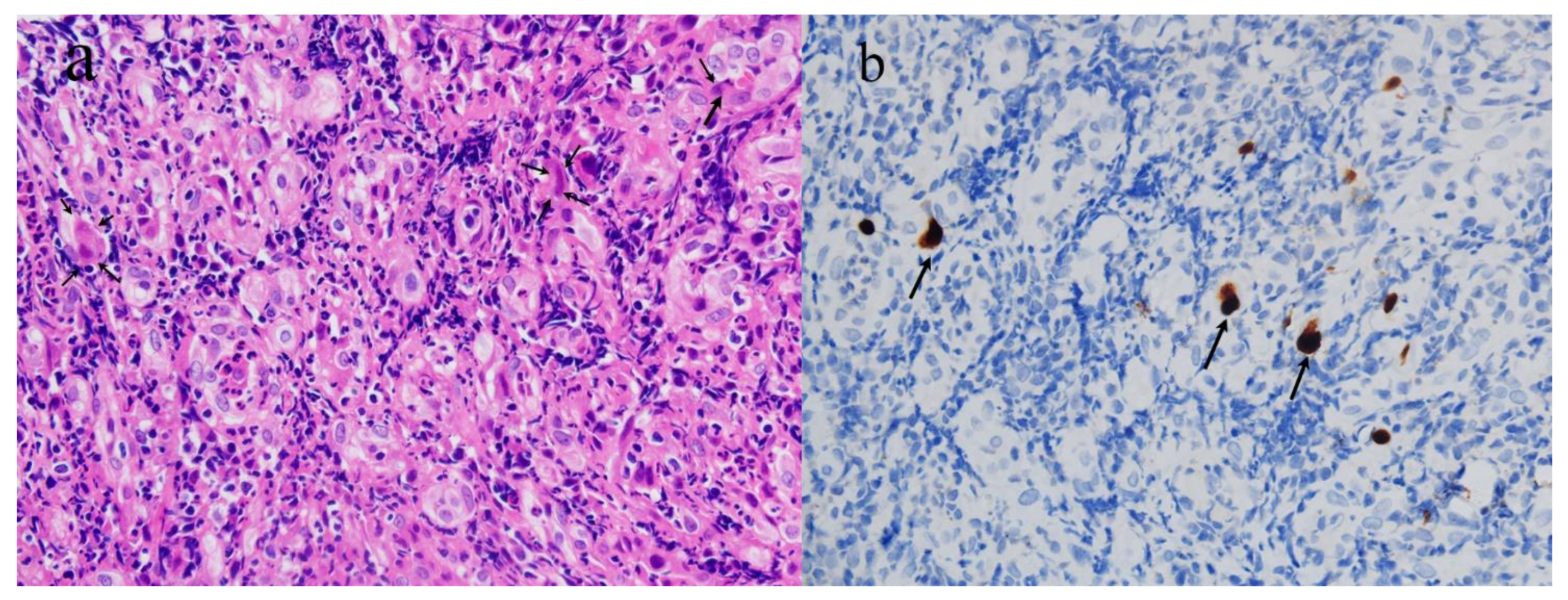
Two days after the colonoscopy, the biopsy revealed moderately active chronic proctitis with CMV infection (Figure 2). Microscopic findings showed a colorectal ulcer with fibrinoid necrotic debris, granulation tissue formation, and acute and chronic inflammatory cell infiltration. Intranuclear viral inclusions were seen in some infected cells. Immunohistochemical (IHC) staining with monoclonal antibodies for CMV confirmed CMV infections. CMV proctitis was diagnosed clinically.
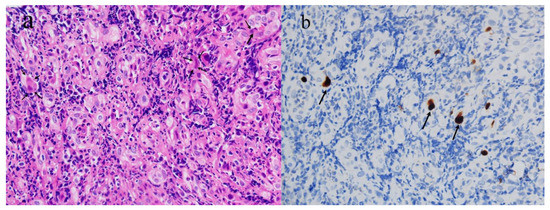
Figure 2.
(a) Microscopic examination of rectal biopsy (×400, H&E stain). The large, infected cell showed an intranuclear viral inclusion with a perinuclear halo. (b) Immunohistochemical staining with monoclonal antibodies for CMV (×400) demonstrated positive uptake in inclusion bodies (arrow).
The patient received 250 mg of ganciclovir intravenously twice daily for 5 days, and her intestinal discomfort, including abdominal pain and constipation, were completely resolved. A re-examination of the colonoscopy revealed that the rectal inflammation had subsided significantly, and the lesion had shrunk and no longer had a tumor-like appearance (Figure 1b). She was discharged in a stable condition after her symptoms resolved. After discharge, the patient was instructed to take 0.25 g ganciclovir capsules orally twice a day, one pill each time, reduced to one pill per day after one week. A follow-up colonoscopy performed after 28 days of ganciclovir treatment revealed that the lesion had completely recovered, with newly grown mucosal tissue, and a biopsy (Figure 1c) for CMV IHC staining was negative. Although we cannot prove whether the COVID-19 vaccine was the trigger of a new bout of CMV proctitis or whether it was just a contingent association, the brief duration of the symptoms and the timing of the COVID-19 vaccination administration led to the increased likelihood of the vaccine as a plausible culprit for her acute bout of constipation.
3. Discussion
There are several points of concern about this case: 1. This is a case of opportunistic disease caused by an immune disorder triggered by the injection of the COVID-19 vaccine. Previously reported diseases associated with COVID-19 vaccinations are usually attributed to immune hyperactivity, such as diseases of the digestive system [10,11,12,13,14,15,16]. The reactivation of herpes zoster virus in the skin has been reported as an immunodeficiency disease caused by immune disorders. Until now, no immune-deficiency diseases in the digestive system, such as CMV proctitis, had been reported. 2. The presentation of proctitis in this case was special, showing an appearance similar to that of a rectal tumor. We hope that this case will serve as a reminder to readers about whether proctitis following COVID-19 vaccination has a comparable appearance and performance, in order to avoid overdiagnosis and therapy. 3. CMV proctitis produced by the COVID-19 vaccine responds well to conservative medical treatment with ganciclovir, indicating that prompt identification and treatment do not hinder vaccination. The purpose of our report on this case is to enable readers to quickly identify, diagnose, and treat similar cases in a timely manner.
CMV disease rarely develops in immunocompetent patients, and reported cases often present with a mild, self-limiting course, without severe life-threatening sequelae [17]. According to a recent review of 290 cases of CMV disease in immunocompetent patients, the most frequently affected site was the gastrointestinal tract, but the rectum was rarely involved [17]. CMV proctitis can present in two distinct forms: primary and reactivated. It is pathognomonic for primary CMV proctitis for young patients to experience mononucleosis-like illness with rectal bleeding within several days to two weeks of unprotected anal intercourse. Reactivated CMV proctitis occurs mainly in elderly patients, without exposure to anal intercourse, who have poor underlying physical conditions, multiple comorbidities such as diabetes mellitus (DM), inflammatory bowel disease, and multiple organ failure, or who have immunodeficiency disease [18]. Obviously, in our case, the patient did not meet the criteria for primary CMV proctitis. Moreover, she was healthy, without a history of immune-deficiency disease, and was not receiving immunosuppressive drugs, which also contradicted the criteria for reactivated CMV proctitis. When the lesion involves the rectum, most patients present with diarrhea and tenesmus [19]. Meanwhile, in our report, the main symptom of the patient was constipation, because we observed a new tumor-like lesion under endoscopy. Although CMV proctitis with a tumor-like appearance has been reported before [20,21], it is still peculiar.
Due to their ability to reduce COVID-19-related disease’s severity and mortality [22], COVID-19 vaccines are being used worldwide. There have been some concerns regarding the possibility of COVID-19-vaccine-induced autoimmunity [23]. Indeed, antibodies against the spike protein S1 of SARS-CoV-2 have a high affinity for some human tissue proteins, suggesting that molecular mimicry may be responsible for this association [3]. Recently, some cases of multiple diseases that developed after COVID-19 vaccination have been reported, such as autoimmune hepatitis [10,11], myocarditis [24], thrombotic thrombocytopenia [25], and other diseases. There are some similarities between the previously described cases and the present case; one of them is a short interval between vaccination and symptom onset [11,26,27,28]. Most vaccine-related diseases are autoimmune, but there are still some reports of immune-deficiency diseases such as herpes zoster virus and herpes simplex virus reactivation (Table 1) [4,5,6,7,8,9]. Although a definitive theoretical elucidation of the underlying causes for herpes zoster virus reactivation remains elusive, there are still some conjectures. Psichogiou et al. [9] theorize that, following vaccination, a massive shift in the host’s T-cell response following vaccination may render the host’s zoster virus-specific adaptive immune cells momentarily incapable of managing latent zoster virus infection, which could be the underlying mechanism of virus reactivation. W.-H. Wang et al. [6] thought that it was possible that the vaccine caused certain immunomodulation that allowed the virus to awaken from latency. A review of 40 cases in an International Dermatology Registry reported 40 cases of varicella-zoster virus (VZV) and herpes simplex virus (HSV) reactivation, most of which occurred after the first vaccine dose [8]. Fathy, R.A. et al. [8] thought that herpesvirus reactivation may occur due to innate or cell-mediated immune-defense failures initiated by the host response to vaccination, although the precise mechanism is not known.

Table 1.
Summary of some reported cases of COVID-19-vaccine-related diseases.
A literature search on PubMed for reports of cases following COVID-19 vaccination using the search terms (“COVID-19 vaccin*” [Title]) AND (case reports [Filter]) retrieved a total of 554 articles. The reports included in our review were limited to those written in English. The reference lists of relevant articles retrieved by the searches were also reviewed. We then screened out six COVID-19-vaccine-related diseases of the digestive system, as shown in the table below (Table 1).
As seen above, the majority of COVID-19-vaccine-related digestive diseases are autoimmune diseases due to immune hyperactivity. However, in our report, this is the first case of CMV proctitis in the digestive system following vaccination with the COVID-19 vaccine, further demonstrating that the COVID-19 vaccine may cause immune disorders rather than immune hyperactivity. A search of the Vaccine Adverse Event Reporting System (VAERS) database on 27 February 2022 yielded no events associated with COVID-19 vaccination and cytomegalovirus infection, suggesting this is a very interesting and rare case. VAERS accepts reports of adverse events and reactions that occur following vaccination. Most of the reports to VAERS are voluntary, which means they are subject to biases, whereas, to some extent, it proves that vaccine-related CMV infections are rare.
However, there have been some recent reports of COVID-19-related CMV proctitis [30,31,32]. Maillet, F. et al. [30] described a case of reactivated biopsy-proven cytomegalovirus proctitis complicating the course of severe COVID-19 pneumonia treated with dexamethasone, anakinra, and lopinavir/ritonavir. Treatment with ganciclovir led to a favorable outcome. They theorize that the dysregulation of the immune system during COVID-19 pneumonia may cause a specific decrease in CD4+ T cells as in HIV patients, which leads to the development of CMV proctitis. On the other hand, some immunosuppressive agents used to combat COVID-19 inflammatory cytokine storm syndrome may lead to potential infectious adverse events. On the other hand, Plüß, M. et al. [29] reported a case of CMV reactivation after SARS-CoV-2 vaccination, which was thought to have a mechanism similar to immune reconstitution inflammatory syndrome (IRIS) because vaccination is a strong stimulator of the immune system. Therefore, we speculated that, in our case, the vaccine-induced CMV proctitis might have been related to abnormal lymphocyte function caused by immune-homeostasis disruption.
To sum up, we report a case of a 58-year-old Chinese woman who was previously healthy and had no underlying ailments, and developed CMV proctitis after receiving a second dose of the COVID-19 vaccine, which usually occurs in immunocompromised populations. A vaccine-induced immune disorder remains a highly suspected possibility, which may be confirmed by more similar examples.
4. Conclusions
The outcomes of this case scenario confirm CMV proctitis as a probable complication of COVID-19 vaccines. The clinical course was favorable with ganciclovir therapy. Immune disorders are more likely than immune hyperactivity to be involved in vaccine-related disease processes. Nevertheless, it should not distract healthcare providers from the overwhelming benefits of mass COVID-19 vaccination.
Author Contributions
Y.L. wrote the manuscript; Y.C. revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by [National Natural Science Foundation of China] grant number [No.81670554].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Zhongnan Hospital of Wuhan University (protocol code 2022093K and date of approval: 4 May 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeld, M.; Tincani, A.; Andreoli, L.; Cattalini, M.; Greenbaum, A.; Kanduc, D.; Alijotas-Reig, J.; Zinserling, V.; Semenova, N.; Amital, H. Covid-19 and autoimmunity. Autoimmun. Rev. 2020, 19, 102597. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. [Google Scholar] [CrossRef]
- Eid, E.; Abdullah, L.; Kurban, M.; Abbas, O. Herpes zoster emergence following mRNA COVID-19 vaccine. J. Med. Virol. 2021, 93, 5231–5232. [Google Scholar] [CrossRef] [PubMed]
- David, E.; Landriscina, A. Herpes Zoster Following COVID-19 Vaccination. J. Drugs Dermatol. 2021, 20, 898–900. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Wei, K.C.; Chen, A.; Wang, W.H. Herpes zoster following COVID-19 vaccine: A report of three cases. Qjm 2021, 114, 531–532. [Google Scholar] [CrossRef]
- Maruki, T.; Ishikane, M.; Suzuki, T.; Ujiie, M.; Katano, H.; Ohmagari, N. A case of varicella zoster virus meningitis following BNT162b2 mRNA COVID-19 vaccination in an immunocompetent patient. Int. J. Infect. Dis. 2021, 113, 55–57. [Google Scholar] [CrossRef]
- Fathy, R.A.; McMahon, D.E.; Lee, C.; Chamberlin, G.C.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W. Varicella-zoster and herpes simplex virus reactivation post-COVID-19 vaccination: A review of 40 cases in an International Dermatology Registry. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e6–e9. [Google Scholar] [CrossRef]
- Psichogiou, M.; Samarkos, M.; Mikos, N.; Hatzakis, A. Reactivation of Varicella Zoster Virus after Vaccination for SARS-CoV-2. Vaccines 2021, 9, 572. [Google Scholar] [CrossRef]
- Garrido, I.; Lopes, S.; Simões, M.S.; Liberal, R.; Lopes, J.; Carneiro, F.; Macedo, G. Autoimmune hepatitis after COVID-19 vaccine—more than a coincidence. J. Autoimmun. 2021, 125, 102741. [Google Scholar] [CrossRef]
- Bril, F.; Al Diffalha, S.; Dean, M.; Fettig, D.M. Autoimmune hepatitis developing after coronavirus disease 2019 (COVID-19) vaccine: Causality or casualty? J. Hepatol. 2021, 75, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Cieślewicz, A.; Dudek, M.; Krela-Kaźmierczak, I.; Jabłecka, A.; Lesiak, M.; Korzeniowska, K. Pancreatic Injury after COVID-19 Vaccine-A Case Report. Vaccines 2021, 9, 576. [Google Scholar] [CrossRef] [PubMed]
- Parkash, O.; Sharko, A.; Farooqi, A.; Ying, G.W.; Sura, P. Acute Pancreatitis: A Possible Side Effect of COVID-19 Vaccine. Cureus 2021, 13, e14741. [Google Scholar] [CrossRef]
- Torrente, S.; Castiella, A.; Garmendia, M.; Zapata, E. Probable autoimmune hepatitis reactivated after COVID-19 vaccination. Gastroenterol Hepatol. 2021, 45, 115–116. [Google Scholar] [CrossRef] [PubMed]
- Hines, A.; Shen, J.G.; Olazagasti, C.; Shams, S. Immune thrombocytopenic purpura and acute liver injury after COVID-19 vaccine. BMJ Case Rep. 2021, 14, e242678. [Google Scholar] [CrossRef] [PubMed]
- Lensen, R.; Netea, M.G.; Rosendaal, F.R. Hepatitis C Virus Reactivation Following COVID-19 Vaccination—A Case Report. Int. Med. Case Rep. J. 2021, 14, 573–576. [Google Scholar] [CrossRef]
- Rafailidis, P.I.; Mourtzoukou, E.G.; Varbobitis, I.C.; Falagas, M.E. Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review. Virol. J. 2008, 5, 47. [Google Scholar] [CrossRef]
- Studemeister, A. Cytomegalovirus proctitis: A rare and disregarded sexually transmitted disease. Sex. Transm. Dis. 2011, 38, 876–878. [Google Scholar] [CrossRef]
- Ng, F.H.; Chau, T.N.; Cheung, T.C.; Kng, C.; Wong, S.Y.; Ng, W.F.; Lee, K.C.; Chan, E.; Lai, S.T.; Yuen, W.C. Cytomegalovirus colitis in individuals without apparent cause of immunodeficiency. Dig. Dis Sci. 1999, 44, 945–952. [Google Scholar] [CrossRef]
- Macaigne, G.; Auriault, M.L.; Boivin, J.F.; Chayette, C.; Cheaib, S.; Deplus, R. Acute cytomegalovirus (CMV) recto-colitis mimicking rectal carcinoma without apparent cause of immunodeficiency. Gastroenterol. Clin. Biol. 2004, 28, 73–76. [Google Scholar] [CrossRef]
- Subbarao, S.; O’Sullivan, A.; Adesina, T.; Gwozdz, A.M.; Rees, J.; Satta, G. Cytomegalovirus proctitis mimicking rectal cancer in an immunocompetent elderly patient: A case report. BMC Res. Notes 2014, 7, 799. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Lee, E.J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am. J. Hematol. 2021, 96, 534–537. [Google Scholar] [CrossRef]
- Salah, H.M.; Mehta, J.L. COVID-19 Vaccine and Myocarditis. Am. J. Cardiol. 2021, 157, 146–148. [Google Scholar] [CrossRef]
- Fanni, D.; Saba, L.; Demontis, R.; Gerosa, C.; Chighine, A.; Nioi, M.; Suri, J.S.; Ravarino, A.; Cau, F.; Barcellona, D. Vaccine-induced severe thrombotic thrombocytopenia following COVID-19 vaccination: A report of an autoptic case and review of the literature. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5063–5069. [Google Scholar]
- Yoshifuji, A.; Ishioka, K.; Masuzawa, Y.; Suda, S.; Murata, S.; Uwamino, Y.; Fujino, M.; Miyahara, H.; Hasegawa, N.; Ryuzaki, M. COVID-19 vaccine induced interstitial lung disease. J. Infect. Chemother. 2022, 28, 95–98. [Google Scholar] [CrossRef]
- Al-Mashdali, A.F.; Ata, Y.M.; Sadik, N. Post-COVID-19 vaccine acute hyperactive encephalopathy with dramatic response to methylprednisolone: A case report. Ann. Med. Surg. 2021, 69, 102803. [Google Scholar] [CrossRef]
- Lee, C.Y.; Chen, Y.H.; Lu, P.L. Reactivated cytomegalovirus proctitis in an immunocompetent patient presenting as nosocomial diarrhea: A case report and literature review. BMC Infect. Dis. 2017, 17, 113. [Google Scholar] [CrossRef]
- Plüß, M.; Mese, K.; Kowallick, J.T.; Schuster, A.; Tampe, D.; Tampe, B. Case Report: Cytomegalovirus Reactivation and Pericarditis Following ChAdOx1 nCoV-19 Vaccination Against SARS-CoV-2. Front. Immunol. 2021, 12, 784145. [Google Scholar] [CrossRef]
- Maillet, F.; Pourbaix, A.; le Pluart, D.; Sirmai, L.; Postolache, S.A.; Couvelard, A.; Houhou-Fidouh, N.; Males, L.; Deconinck, L.; Lescure, F. Cytomegalovirus proctitis as a complication of COVID-19 with immunosuppressive treatments. IDCases 2021, 24, e01111. [Google Scholar] [CrossRef]
- Geisen, W.R.; Berger, J.; Schwartz, C.; Reddy, A.; Rai, B.; Wadih, G.; Peck, J. Cytomegalovirus Enterocolitis secondary to experimental COVID-19 therapy. IDCases 2020, 22, e00962. [Google Scholar] [CrossRef] [PubMed]
- Marchi, G.; Vianello, A.; Crisafulli, E.; Maroccia, A.; Crinò, S.F.; Pecori, S.; Zamboni, G.A.; Mazzaferri, F.; Tacconelli, E.; Girelli, D. Cytomegalovirus-Induced Gastrointestinal Bleeding and Pancreatitis Complicating Severe Covid-19 Pneumonia: A Paradigmatic Case. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020060. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).