
Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Classification
2.3. Clinical Data
2.4. Laboratory Data
2.5. Machine Learning Analysis
2.6. Statistics
3. Results
3.1. Baseline Characteristics among the Four Groups
3.2. Identification of an Appropriate Classification for Prediction Using Machine Learning Analysis
3.3. Identification of an Appropriate ML Algorithm for the Prediction of DSPN and Analysis of Predictive Values
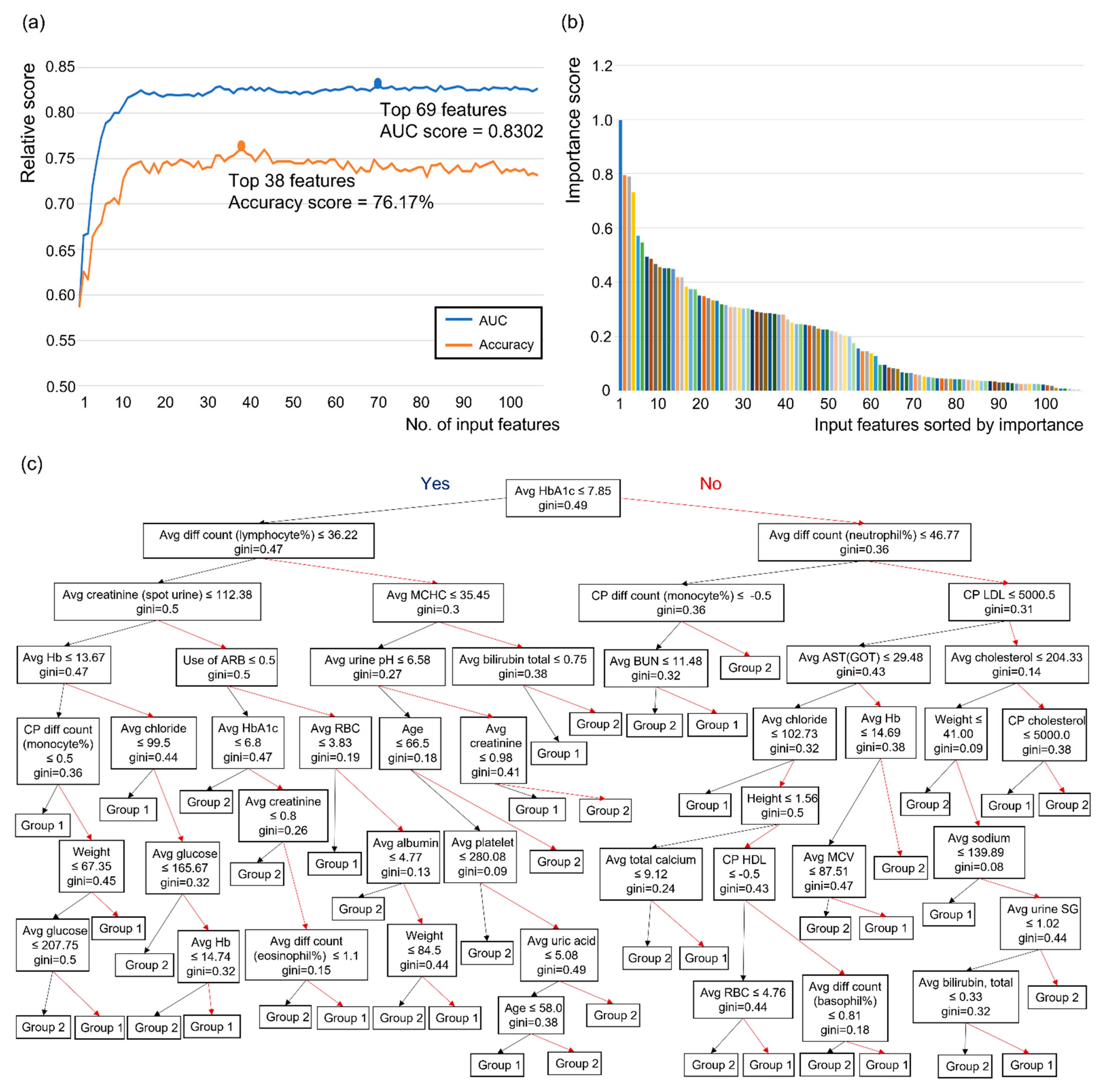
3.4. Development of a Decision-Making Model Using Influential Features from the RF Algorithm
3.5. ML Analysis of the Confirmed Group to Identify Demyelinated and Mixed Types of DSPN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center for Disease Control and Prevention. National diabetes statistics report, 2020. In Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; Center for Disease Control and Prevention: Atlanta, GA, USA, 2020; pp. 12–15. [Google Scholar]
- Mohamadi, A.; Cooke, D.W. Type 2 diabetes mellitus in children and adolescents. Adolesc. Med. State Art Rev. 2010, 21, 103–119. [Google Scholar] [PubMed]
- Russell, J.W.; Zilliox, L.A. Diabetic neuropathies. Continuum 2014, 20, 1226–1240. [Google Scholar] [CrossRef] [Green Version]
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R.; Zochodne, D.W.; Wright, D.E.; Bennett, D.L.; Bril, V.; Russell, J.W.; Viswanathan, V. Diabetic neuropathy. Nat. Rev. Dis. Primers 2019, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Sloan, G.; Selvarajah, D.; Tesfaye, S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat. Rev. Endocrinol. 2021, 17, 400–420. [Google Scholar] [CrossRef]
- Kaku, M.; Vinik, A.; Simpson, D.M. Pathways in the diagnosis and management of diabetic polyneuropathy. Curr. Diabetes Rep. 2015, 15, 609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: Update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [Green Version]
- Thomas, P.K. Classification, differential diagnosis, and staging of diabetic peripheral neuropathy. Diabetes 1997, 46, S54–S57. [Google Scholar] [CrossRef]
- Boulton, A.J.; Vinik, A.I.; Arezzo, J.C.; Bril, V.; Feldman, E.L.; Freeman, R.; Malik, R.A.; Maser, R.E.; Sosenko, J.M.; Ziegler, D.; et al. Diabetic neuropathies: A statement by the American Diabetes Association. Diabetes Care 2005, 28, 956–962. [Google Scholar] [CrossRef] [Green Version]
- England, J.D.; Gronseth, G.S.; Franklin, G.; Miller, R.G.; Asbury, A.K.; Carter, G.T.; Cohen, J.A.; Fisher, M.A.; Howard, J.F.; Kinsella, L.J.; et al. Distal symmetrical polyneuropathy: A definition for clinical research. A report of the American Academy of Neurology, the American Association of Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Arch. Phys. Med. Rehabil. 2005, 86, 167–174. [Google Scholar] [CrossRef]
- Dyck, P.J.; Kratz, K.M.; Karnes, J.L.; Litchy, W.J.; Klein, R.; Pach, J.M.; Wilson, D.M.; O’Brien, P.C.; Melton, L.J., 3rd. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology 1993, 43, 817–824. [Google Scholar] [CrossRef]
- Meijer, J.W.; Bosma, E.; Lefrandt, J.D.; Links, T.P.; Smit, A.J.; Stewart, R.E.; van der Hoeven, J.H.; Hoogenberg, K. Clinical diagnosis of diabetic polyneuropathy with the diabetic neuropathy symptom and diabetic neuropathy examination scores. Diabetes Care 2003, 26, 697–701. [Google Scholar] [CrossRef] [Green Version]
- Himeno, T.; Kamiya, H.; Nakamura, J. Lumos for the long trail: Strategies for clinical diagnosis and severity staging for diabetic polyneuropathy and future directions. J. Diabetes Investig. 2020, 11, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Bril, V.; Perkins, B.A. Validation of the Toronto clinical scoring system for diabetic polyneuropathy. Diabetes Care 2002, 25, 2048–2052. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Standards of medical care in diabetes—2016 abridged for primary care providers. Clin. Diabetes A Publ. Am. Diabetes Assoc. 2016, 34, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- England, J.D.; Gronseth, G.S.; Franklin, G.; Miller, R.G.; Asbury, A.K.; Carter, G.T.; Cohen, J.A.; Fisher, M.A.; Howard, J.F.; Kinsella, L.J.; et al. Distal symmetric polyneuropathy: A definition for clinical research: Report of the American Academy of Neurology, the American Association of Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 2005, 64, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasnoor, M.; Dimachkie, M.M.; Kluding, P.; Barohn, R.J. Diabetic neuropathy part 1: Overview and symmetric phenotypes. Neurol. Clin. 2013, 31, 425–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tesfaye, S.; Stevens, L.K.; Stephenson, J.M.; Fuller, J.H.; Plater, M.; Ionescu-Tirgoviste, C.; Nuber, A.; Pozza, G.; Ward, J.D. Prevalence of diabetic peripheral neuropathy and its relation to glycaemic control and potential risk factors: The EURODIAB IDDM Complications Study. Diabetologia 1996, 39, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.I.; Boyko, E.J.; Ahroni, J.H.; Stensel, V.; Forsberg, R.C.; Smith, D.G. Risk factors for diabetic peripheral sensory neuropathy. Results of the Seattle Prospective Diabetic Foot Study. Diabetes Care 1997, 20, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Adler, A. Risk factors for diabetic neuropathy and foot ulceration. Curr. Diabetes Rep. 2001, 1, 202–207. [Google Scholar] [CrossRef]
- Tesfaye, S.; Chaturvedi, N.; Eaton, S.E.; Ward, J.D.; Manes, C.; Ionescu-Tirgoviste, C.; Witte, D.R.; Fuller, J.H.; EURODIAB Prospective Complications Study Group. Vascular risk factors and diabetic neuropathy. N. Engl. J. Med. 2005, 352, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bzdok, D.; Altman, N.; Krzywinski, M. Statistics versus machine learning. Nat. Methods 2018, 15, 233–234. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, M.; Moghimbeigi, A.; Kiani, J.; Mahjub, H.; Faradmal, J. Diabetic peripheral neuropathy class prediction by multicategory support vector machine model: A cross-sectional study. Epidemiol. Health 2016, 38, e2016011. [Google Scholar] [CrossRef] [PubMed]
- Dagliati, A.; Marini, S.; Sacchi, L.; Cogni, G.; Teliti, M.; Tibollo, V.; de Cata, P.; Chiovato, L.; Bellazzi, R. Machine learning methods to predict diabetes complications. J. Diabetes Sci. Technol. 2018, 12, 295–302. [Google Scholar] [CrossRef]
- Tsao, H.Y.; Chan, P.Y.; Su, E.C.Y. Predicting diabetic retinopathy and identifying interpretable biomedical features using machine learning algorithms. BMC Bioinform. 2018, 19, 283. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Long, E.; Cai, L.; Cao, Q.; Wu, X.; Tong, R. Machine learning approaches to predict risks of diabetic complications and poor glycemic control in nonadherent type 2 diabetes. Front. Pharmacol. 2021, 12, 665951. [Google Scholar] [CrossRef] [PubMed]
- Schafer, Z.; Mathisen, A.; Svendsen, K.; Engberg, S.; Rolighed Thomsen, T.; Kirketerp-Moller, K. Toward machine-learning-based decision support in diabetes care: A risk stratification study on diabetic foot ulcer and amputation. Front. Med. 2020, 7, 601602. [Google Scholar] [CrossRef] [PubMed]
- Haque, F.; Bin Ibne Reaz, M.; Chowdhury, M.E.H.; Srivastava, G.; Md Ali, S.H.; Bakar, A.A.A.; Bhuiyan, M.A.S. Performance analysis of conventional machine learning algorithms for diabetic sensorimotor polyneuropathy severity classification. Diagnostics 2021, 11, 801. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. In IJCAI; Morgan Kaufmann: Burlington, MA, USA, 1995; pp. 1137–1145. [Google Scholar]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; Association for Computing Machinery: New York, NY, USA; pp. 785–794. [Google Scholar]
- Hearst, M.A.; Dumais, S.T.; Osuna, E.; Platt, J.; Scholkopf, B. Support vector machines. IEEE Intell. Syst. Appl. 1998, 13, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Sagi, O.; Rokach, L. Ensemble learning: A survey. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2018, 8, e1249. [Google Scholar] [CrossRef]
- Drummond, C.; Holte, R.C. Severe class imbalance: Why better algorithms aren’t the answer. In European Conference on Machine Learning; Springer: Berlin, Germany, 2005; pp. 539–546. [Google Scholar]
- Ravi, D.; Wong, C.; Deligianni, F.; Berthelot, M.; Andreu-Perez, J.; Lo, B.; Yang, G.Z. Deep learning for health informatics. IEEE J. Biomed. Health Inform. 2017, 21, 4–21. [Google Scholar] [CrossRef] [Green Version]
- Kavakiotis, I.; Tsave, O.; Salifoglou, A.; Maglaveras, N.; Vlahavas, I.; Chouvarda, I. Machine learning and data mining methods in diabetes research. Comput. Struct. Biotechnol. J. 2017, 15, 104–116. [Google Scholar] [CrossRef]
- Maeda-Gutierrez, V.; Galvan-Tejada, C.E.; Cruz, M.; Valladares-Salgado, A.; Galvan-Tejada, J.I.; Gamboa-Rosales, H.; Garcia-Hernandez, A.; Luna-Garcia, H.; Gonzalez-Curiel, I.; Martinez-Acuna, M. Distal symmetric polyneuropathy identification in type 2 diabetes subjects: A random forest approach. Healthcare 2021, 9, 138. [Google Scholar] [CrossRef]
- Meijer, J.W.; Smit, A.J.; Sonderen, E.V.; Groothoff, J.W.; Eisma, W.H.; Links, T.P. Symptom scoring systems to diagnose distal polyneuropathy in diabetes: The diabetic neuropathy symptom score. Diabet. Med. 2002, 19, 962–965. [Google Scholar] [CrossRef] [Green Version]
- Feldman, E.L.; Stevens, M.J.; Thomas, P.K.; Brown, M.B.; Canal, N.; Greene, D.A. A practical two-step quantitative clinical and electrophysiological assessment for the diagnosis and staging of diabetic neuropathy. Diabetes Care 1994, 17, 1281–1289. [Google Scholar] [CrossRef]
- Perkins, B.A.; Olaleye, D.; Zinman, B.; Bril, V. Simple screening tests for peripheral neuropathy in the diabetes clinic. Diabetes Care 2001, 24, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, A.; Alabdali, M.; Alsulaiman, A.; Albulaihe, H.; Breiner, A.; Katzberg, H.D.; Aljaafari, D.; Lovblom, L.E.; Bril, V. The sensitivity and specificity of the neurological examination in polyneuropathy patients with clinical and electrophysiological correlations. PLoS ONE 2017, 12, e0171597. [Google Scholar] [CrossRef] [PubMed]
- Franse, L.V.; Valk, G.D.; Dekker, J.H.; Heine, R.J.; van Eijk, J.T. ‘Numbness of the feet’ is a poor indicator for polyneuropathy in Type 2 diabetic patients. Diabet. Med. 2000, 17, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Overland, C.J.; Low, P.A.; Litchy, W.J.; Davies, J.L.; Dyck, P.J.; O’Brien, P.C.; Cl vs. NPhys Trial Investigators; Albers, J.W.; Andersen, H.; et al. Signs and symptoms versus nerve conduction studies to diagnose diabetic sensorimotor polyneuropathy: Cl vs. NPhys. trial. Muscle Nerve 2010, 42, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Graham, J.; Dabbah, M.A.; Petropoulos, I.N.; Ponirakis, G.; Asghar, O.; Alam, U.; Marshall, A.; Fadavi, H.; Ferdousi, M.; et al. Small nerve fiber quantification in the diagnosis of diabetic sensorimotor polyneuropathy: Comparing corneal confocal microscopy with intraepidermal nerve fiber density. Diabetes Care 2015, 38, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javed, S.; Petropoulos, I.N.; Tavakoli, M.; Malik, R.A. Clinical and diagnostic features of small fiber damage in diabetic polyneuropathy. Handb. Clin. Neurol. 2014, 126, 275–290. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Lais, A.; Karnes, J.L.; O’Brien, P.; Rizza, R. Fiber loss is primary and multifocal in sural nerves in diabetic polyneuropathy. Ann. Neurol. 1986, 19, 425–439. [Google Scholar] [CrossRef]
- Galiero, R.; Ricciardi, D.; Pafundi, P.C.; Todisco, V.; Tedeschi, G.; Cirillo, G.; Sasso, F.C. Whole plantar nerve conduction study: A new tool for early diagnosis of peripheral diabetic neuropathy. Diabetes Res. Clin. Pract. 2021, 176, 108856. [Google Scholar] [CrossRef]
- Petropoulos, I.N.; Ponirakis, G.; Khan, A.; Almuhannadi, H.; Gad, H.; Malik, R.A. Diagnosing diabetic neuropathy: Something old, something new. Diabetes Metab. J. 2018, 42, 255–269. [Google Scholar] [CrossRef]
- Perkins, B.; Bril, V. Electrophysiologic testing in diabetic neuropathy. Handb. Clin. Neurol. 2014, 126, 235–248. [Google Scholar] [CrossRef]
- Sima, A.A.; Zhang, W. Mechanisms of diabetic neuropathy: Axon dysfunction. Handb. Clin. Neurol. 2014, 126, 429–442. [Google Scholar] [CrossRef]
- Sima, A.A.; Kamiya, H. Diabetic neuropathy differs in type 1 and type 2 diabetes. Ann. N. Y. Acad. Sci. 2006, 1084, 235–249. [Google Scholar] [CrossRef]
- Elhadd, T.; Mall, R.; Bashir, M.; Palotti, J.; Fernandez-Luque, L.; Farooq, F.; Mohanadi, D.A.; Dabbous, Z.; Malik, R.A.; Abou-Samra, A.B.; et al. Artificial Intelligence (AI) based machine learning models predict glucose variability and hypoglycaemia risk in patients with type 2 diabetes on a multiple drug regimen who fast during ramadan (The PROFAST—IT Ramadan study). Diabetes Res. Clin. Pract. 2020, 169, 108388. [Google Scholar] [CrossRef]
- Kleinbaum, D.G.; Klein, M. Introduction to logistic regression. In Logistic Regression; Springer: New York, NY, USA, 2010; pp. 1–39. [Google Scholar] [CrossRef]
- Panesar, S.S.; D’Souza, R.N.; Yeh, F.C.; Fernandez-Miranda, J.C. Machine learning versus logistic regression methods for 2-year mortality prognostication in a small, heterogeneous glioma database. World Neurosurg. X 2019, 2, 100012. [Google Scholar] [CrossRef] [PubMed]
- Lynam, A.L.; Dennis, J.M.; Owen, K.R.; Oram, R.A.; Jones, A.G.; Shields, B.M.; Ferrat, L.A. Logistic regression has similar performance to optimised machine learning algorithms in a clinical setting: Application to the discrimination between type 1 and type 2 diabetes in young adults. Diagn. Progn. Res. 2020, 4, 6. [Google Scholar] [CrossRef]
- Levy, J.J.; O’Malley, A.J. Don’t dismiss logistic regression: The case for sensible extraction of interactions in the era of machine learning. BMC Med. Res. Methodol. 2020, 20, 171. [Google Scholar] [CrossRef]
- Liu, X.; Xu, Y.; An, M.; Zeng, Q. The risk factors for diabetic peripheral neuropathy: A meta-analysis. PLoS ONE 2019, 14, e0212574. [Google Scholar] [CrossRef]
- Andersen, S.T.; Witte, D.R.; Dalsgaard, E.M.; Andersen, H.; Nawroth, P.; Fleming, T.; Jensen, T.M.; Finnerup, N.B.; Jensen, T.S.; Lauritzen, T.; et al. Risk factors for incident diabetic polyneuropathy in a cohort with screen-detected type 2 diabetes followed for 13 years: ADDITION-Denmark. Diabetes Care 2018, 41, 1068–1075. [Google Scholar] [CrossRef] [Green Version]
- Callaghan, B.C.; Gao, L.; Li, Y.; Zhou, X.; Reynolds, E.; Banerjee, M.; Pop-Busui, R.; Feldman, E.L.; Ji, L. Diabetes and obesity are the main metabolic drivers of peripheral neuropathy. Ann. Clin. Transl. Neurol. 2018, 5, 397–405. [Google Scholar] [CrossRef]
- Callaghan, B.C.; Price, R.S.; Feldman, E.L. Distal symmetric polyneuropathy: A review. JAMA 2015, 314, 2172–2181. [Google Scholar] [CrossRef]
- Li, L.; Liu, B.; Lu, J.; Jiang, L.; Zhang, Y.; Shen, Y.; Wang, C.; Jia, W. Serum albumin is associated with peripheral nerve function in patients with type 2 diabetes. Endocrine 2015, 50, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Yan, P.; Tang, Q.; Wu, Y.; Wan, Q.; Zhang, Z.; Xu, Y.; Zhu, J.; Miao, Y. Serum albumin was negatively associated with diabetic peripheral neuropathy in Chinese population: A cross-sectional study. Diabetol. Metab. Syndr. 2021, 13, 100. [Google Scholar] [CrossRef] [PubMed]
- Su, J.B.; Zhao, L.H.; Zhang, X.L.; Cai, H.L.; Huang, H.Y.; Xu, F.; Chen, T.; Wang, X.Q. HbA1c variability and diabetic peripheral neuropathy in type 2 diabetic patients. Cardiovasc. Diabetol. 2018, 17, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azab, B.; Chainani, V.; Shah, N.; McGinn, J.T. Neutrophil-lymphocyte ratio as a predictor of major adverse cardiac events among diabetic population: A 4-year follow-up study. Angiology 2013, 64, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Altay, F.A.; Kuzi, S.; Altay, M.; Ates, I.; Gurbuz, Y.; Tutuncu, E.E.; Senturk, G.C.; Altin, N.; Sencan, I. Predicting diabetic foot ulcer infection using the neutrophil-to-lymphocyte ratio: A prospective study. J. Wound Care 2019, 28, 601–607. [Google Scholar] [CrossRef]
- Metsker, O.; Magoev, K.; Yakovlev, A.; Yanishevskiy, S.; Kopanitsa, G.; Kovalchuk, S.; Krzhizhanovskaya, V.V. Identification of risk factors for patients with diabetes: Diabetic polyneuropathy case study. BMC Med. Inform. Decis. Mak. 2020, 20, 201. [Google Scholar] [CrossRef]
- Liu, S.; Zheng, H.; Zhu, X.; Mao, F.; Zhang, S.; Shi, H.; Li, Y.; Lu, B. Neutrophil-to-lymphocyte ratio is associated with diabetic peripheral neuropathy in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2017, 130, 90–97. [Google Scholar] [CrossRef]
- Combrisson, E.; Jerbi, K. Exceeding chance level by chance: The caveat of theoretical chance levels in brain signal classification and statistical assessment of decoding accuracy. J. Neurosci. Methods 2015, 250, 126–136. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature Set Used | Lab Feature Extraction Method | Feature Counts | AUC | Accuracy (%) |
|---|---|---|---|---|
| Laboratory data only | Method 1 | 39 | 0.7954 | 73.74 |
| Method 2 | 39 | 0.7790 | 71.53 | |
| Method 3 | 36 | 0.7226 | 65.32 | |
| Method 1 + 3 | 75 | 0.8095 | 73.83 | |
| Method 2 + 3 | 75 | 0.7950 | 72.26 | |
| Method 1 + 2 + 3 | 114 | 0.8012 | 73.06 | |
| Clinical data only | - | 30 | 0.7493 | 69.79 |
| Laboratory and clinical data | Method 1 | 69 | 0.8284 | 76.09 |
| Method 2 | 69 | 0.8096 | 72.68 | |
| Method 3 | 66 | 0.8100 | 72.98 | |
| Method 1 + 3 | 105 | 0.8350 | 74.85 | |
| Method 2 + 3 | 105 | 0.8141 | 73.02 | |
| Method 1 + 2 + 3 | 144 | 0.8219 | 74.21 |
| Normal (A) (n = 93) | Possible (B) (n = 91) | Probable (C) (n = 13) | Confirmed (D) (n = 273) | p-Value | Post Hoc | |
|---|---|---|---|---|---|---|
| Disease duration (days) | 4543.18 ± 2849.75 | 4464.03 ± 2934.87 | 4933.46 ± 3463.31 | 5686.67 ± 3648.57 | 0.004 | A<>D, B<>D |
| Age (years) | 51.33 ± 12.30 | 49.74 ± 11.51 | 53.85 ± 8.92 | 51.32 ± 14.91 | 0.676 | |
| Sex (male) | 48 (51.6) | 48 (52.7) | 5 (38.5) | 176 (64.5) | 0.027 | |
| Height (m) | 1.61 ± 0.09 | 1.62 ± 0.09 | 1.59 ± 0.09 | 1.64 ± 0.09 | 0.006 | A<>D |
| Weight (kg) | 66.10 ± 11.76 | 66.26 ± 11.14 | 62.21 ± 11.41 | 64.29 ± 11.92 | 0.308 | |
| BMI (kg/m2) | 25.33 ± 3.81 | 25.26 ± 3.48 | 24.65 ± 4.07 | 23.82 ± 3.66 | 0.001 | A<>D, B<>D |
| Initial BST | 211.78 ± 98.75 | 196.51 ± 87.62 | 178.21 ± 104.57 | 249.06 ± 117.68 | 0.000 | A<>D, B<>D |
| Initial HbA1c | 8.69 ± 2.18 | 8.72 ± 2.06 | 9.03 ± 3.09 | 9.59 ± 2.54 | 0.002 | A<>D, B<>D |
| DM retinopathy | 25 (26.9) | 26 (28.6) | 3 (23.1) | 141 (51.6) | 0.000 | |
| Hypertension | 54 (58.1) | 56 (61.5) | 8 (61.5) | 186 (68.1) | 0.304 | |
| Dyslipidemia | 76 (81.7) | 70 (76.9) | 10 (76.9) | 197 (72.2) | 0.29 | |
| Smoking | ||||||
| No | 61 (65.6) | 57 (62.6) | 12 (92.3) | 163 (59.7) | 0.172 | |
| Current | 18 (19.4) | 19 (20.9) | 1 (7.7) | 57 (20.9) | ||
| Past smoking | 14 (15.1) | 15 (16.5) | 0 (0.0) | 53 (19.4) | ||
| Family history of DM | 28 (30.1) | 51 (56.0) | 4 (30.8) | 106 (38.8) | 0.003 | |
| CAD Hx | 25 (26.9) | 24 (26.4) | 6 (46.2) | 93 (34.1) | 0.248 | |
| CVD Hx | 43 (46.2) | 33 (36.3) | 6 (46.2) | 134 (49.1) | 0.205 | |
| Stroke Hx | 25 (26.9) | 16 (17.6) | 2 (15.4) | 63 (23.1) | 0.427 | |
| Diabetes education | 43 (46.2) | 36 (39.6) | 8 (61.5) | 128 (46.9) | 0.412 | |
| Medications | ||||||
| Metformin | 83 (89.2) | 86 (94.5) | 11 (84.6) | 201 (73.6) | 0.000 | |
| Sulfonylureas | 64 (68.8) | 62 (68.1) | 5 (38.5) | 159 (58.2) | 0.048 | |
| TZDs | 11 (11.8) | 5 (5.5) | 1 (7.7) | 3 (13.6) | 0.158 | |
| DPP4is | 62 (66.7) | 65 (71.4) | 8 (61.5) | 147 (53.8) | 0.011 | |
| SGLT2is | 16 (17.2) | 19 (20.9) | 1 (7.7) | 21 (7.7) | 0.004 | |
| Insulin | 37 (39.8) | 32 (35.2) | 8 (61.5) | 179 (65.6) | 0.000 | |
| CCBs | 32 (34.4) | 26 (28.6) | 7 (53.8) | 104 (38.1) | 0.204 | |
| ACEis | 10 (10.8) | 10 (11.0) | 1 (7.7) | 32 (11.7) | 0.965 | |
| ARBs | 51 (54.8) | 54 (59.3) | 7 (53.8) | 156 (57.1) | 0.933 | |
| BBs | 21 (22.6) | 24 (26.4) | 6 (46.2) | 76 (27.8) | 0.355 | |
| Thiazides | 15 (16.1) | 20 (22.0) | 2 (15.4) | 47 (17.2) | 0.723 | |
| Statins | 78 (83.9) | 70 (76.9) | 10 (76.9) | 192 (70.3) | 0.058 |
| Classification | ML Model Which Showed the Best Result | AUC | Accuracy (%) |
|---|---|---|---|
| A vs. B vs. C vs. D | XGB + RF | 0.8546 | 60.85 |
| A vs. B vs. C + D | RF | 0.8105 | 62.34 |
| A vs. B + C vs. D | RF | 0.8075 | 61.32 |
| A + B vs. C vs. D | XGB + RF | 0.8925 | 73.40 |
| A + B vs. C + D | RF | 0.8103 | 72.68 |
| A + B + C vs. D | RF | 0.8250 | 74.47 |
| Model | AUC | Accuracy (%) | Sensitivity | Specificity |
|---|---|---|---|---|
| XGB | 0.7604 | 69.83 | 0.7708 | 0.5899 |
| SVM | 0.7535 | 66.81 | 0.6643 | 0.6721 |
| RF | 0.8250 | 74.47 | 0.7940 | 0.6720 |
| XGB + SVM | 0.7822 | 71.28 | 0.7712 | 0.6363 |
| XGB + RF | 0.8235 | 74.47 | 0.7927 | 0.6743 |
| SVM + RF | 0.8070 | 73.19 | 0.7957 | 0.6478 |
| XGB + RF + SVM | 0.8105 | 73.62 | 0.8103 | 0.6342 |
| Logistic regression | 0.6620 | 84.76 | 0.9721 | 0.3519 |
| Ranking | Feature Name | Importance Score | Ranking | Feature Name | Importance Score |
|---|---|---|---|---|---|
| 1 | Avg glucose | 0.997768 | 36 | Avg WBC | 0.280162 |
| 2 | Avg IFCC | 0.794161 | 37 | Avg PLT | 0.262754 |
| 3 | Avg HbA1c | 0.789265 | 38 | Avg chloride | 0.250326 |
| 4 | Avg albumin | 0.731579 | 39 | Avg uric acid | 0.246706 |
| 5 | Height | 0.57069 | 40 | CP IFCC | 0.246499 |
| 6 | Avg Diff count (lymphocyte %) | 0.546759 | 41 | CP creatinine (spot urine) | 0.242497 |
| 7 | Avg creatinine (spot urine) | 0.493981 | 42 | Avg MCV | 0.240183 |
| 8 | Avg Diff count (neutrophil %) | 0.486409 | 43 | Avg Diff count (eosinophil%) | 0.237532 |
| 9 | Disease duration | 0.467576 | 44 | Avg MCH | 0.229848 |
| 10 | Avg sodium | 0.455435 | 45 | Avg Diff count (monocyte %) | 0.225926 |
| 11 | Avg HCT | 0.451166 | 46 | CP HbA1c | 0.225847 |
| 12 | Avg ALT (GPT) | 0.450865 | 47 | Avg MCHC | 0.222184 |
| 13 | Avg RBC | 0.417525 | 48 | Avg bilirubin | 0.217108 |
| 14 | Avg Hb | 0.383685 | 49 | Avg free T4 | 0.208568 |
| 15 | BMI | 0.375055 | 50 | CP urine SG | 0.204239 |
| 16 | Avg HDL | 0.374211 | 51 | Avg Diff count (basophil %) | 0.201151 |
| 17 | Avg BUN | 0.351033 | 52 | Diabetic retinopathy | 0.176286 |
| 18 | Avg AST (GOT) | 0.348776 | 53 | CP TG | 0.155261 |
| 19 | Avg ALP | 0.342055 | 54 | Use of insulin | 0.14617 |
| 20 | Avg BST | 0.33438 | 55 | CP HDL | 0.146164 |
| 21 | Avg creatinine | 0.332449 | 56 | CP cholesterol | 0.127665 |
| 22 | Age | 0.319338 | 57 | CP WBC | 0.096003 |
| 23 | Avg urine pH | 0.31512 | 58 | CP PLT | 0.09567 |
| 24 | Avg calcium | 0.309396 | 59 | Sex | 0.084762 |
| 25 | Avg TG | 0.307935 | 60 | CP BST | 0.083089 |
| 26 | Avg LDL | 0.305571 | 61 | CP ALP | 0.080399 |
| 27 | Avg TSH | 0.303504 | 62 | Smoking | 0.068729 |
| 28 | Avg protein | 0.302998 | 63 | CP creatinine | 0.065407 |
| 29 | CP glucose | 0.297945 | 64 | CP Diff count (lymphocyte %) | 0.065285 |
| 30 | CP urine pH | 0.290718 | 65 | CP bilirubin | 0.060325 |
| 31 | Avg cholesterol | 0.287416 | 66 | Use of sulfonylurea | 0.05838 |
| 32 | Avg potassium | 0.286635 | 67 | CP AST (GOT) | 0.052956 |
| 33 | Weight | 0.285151 | 68 | CP ALT (GPT) | 0.050693 |
| 34 | Avg urine SG | 0.282845 | 69 | Use of metformin | 0.048544 |
| 35 | CP LDL | 0.280875 |
| Model | AUC | Accuracy (%) | Sensitivity | Specificity |
|---|---|---|---|---|
| XGB | 0.5492 | 62.39 | 0.8329 | 0.1797 |
| SVM | 0.5105 | 68.15 | 1.0000 | 0.0000 |
| RF | 0.5426 | 64.25 | 0.9245 | 0.0436 |
| XGB + SVM | 0.5698 | 67.78 | 0.9947 | 0.0000 |
| XGB + RF | 0.5579 | 64.52 | 0.9317 | 0.0378 |
| SVM + RF | 0.5457 | 67.41 | 0.9889 | 0.0000 |
| XGB + RF + SVM | 0.5601 | 67.41 | 0.9897 | 0.0000 |
| Logistic regression | 0.6350 | 70.97 | 0.8812 | 0.3889 |
| References | Criteria to Diagnose DSPN | Suggested ML Models | AUC/Accuracy | Laboratory Data Processing | Providing Decision-Making Tool |
|---|---|---|---|---|---|
| Kazemi et al., 2016 [24] | clinical (T1DM and T2DM) | MSVM | UC/0.76 | UC | N |
| Dagliati et al., 2018 [25] | UC | LR | 0.726/0.746 | UC | nomogram |
| Fan et al., 2021 [27] | UC | EM | 0.847/0.783 | UC | N |
| Maeda-Gutierrez et al., 2021 [38] | clinical | RF | 0.65/UC | UC | N |
| Current study | electrophysiological | RF | 0.825/0.7447 | average/change pattern | decision tree |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.Y.; Lee, B.; Yoo, W.S.; Park, J.W.; Hyun, J.K. Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques. J. Clin. Med. 2021, 10, 4576. https://doi.org/10.3390/jcm10194576
Shin DY, Lee B, Yoo WS, Park JW, Hyun JK. Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques. Journal of Clinical Medicine. 2021; 10(19):4576. https://doi.org/10.3390/jcm10194576
Chicago/Turabian StyleShin, Dae Youp, Bora Lee, Won Sang Yoo, Joo Won Park, and Jung Keun Hyun. 2021. "Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques" Journal of Clinical Medicine 10, no. 19: 4576. https://doi.org/10.3390/jcm10194576
APA StyleShin, D. Y., Lee, B., Yoo, W. S., Park, J. W., & Hyun, J. K. (2021). Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques. Journal of Clinical Medicine, 10(19), 4576. https://doi.org/10.3390/jcm10194576