Abstract
Background: Primary lack or secondary loss of response to therapy with infliximab is a significant problem. This study aimed to evaluate the response to treatment in patients with Crohn’s disease (CD) and ulcerative colitis (UC) achieving therapeutic and sub-therapeutic trough levels of biosimilar infliximab (CT-P13). Results: A total of 65 patients (32 with CD and 33 with UC) were recruited. The overall response rate in both CD and UC patients exceeded 80%. There were no significant differences in treatment response and CT-P13 levels for patients with CD or UC. We did not find significant differences in the percentage of patients achieving drug levels of 3 μg/mL at week 6, 10, or 12; a significant decrease was observed at week 14. Up to 55.5% of patients with CD and 64.3% of patients with UC with sub-therapeutic CT-P13 levels at week 14 primarily responded to treatment. Conclusions: Intermediate measurements of drug levels at weeks 10 and 12 did not capture any pronounced decrease in infliximab concentrations below therapeutic levels in either group, thus suggesting no clinical usefulness. A significant percentage of patients primarily responded to treatment despite sub-therapeutic drug levels after the induction phase.
1. Introduction
Ulcerative colitis (UC) and Crohn’s disease (CD) are classified as immune-mediated, chronic inflammatory bowel diseases (IBD) [1]. Severe and moderate courses of these diseases, lack of response to standard treatment, and presence of poor prognostic factors are indications for use of biological drugs that inhibit chronic inflammatory response [2,3]. Tumor necrosis factor alpha (TNF-α) is one of the most important factors that maintain chronic inflammation. Three classes of biologics are available for the treatment of IBD: TNF inhibitors, adhesion molecule inhibitors, and anti-interleukin (IL) drugs. Among this type of drug, anti-IL-23 and anti-TNF alpha seem to secure the best results in the management of these conditions [4,5]. In addition to the original TNF inhibitors, biosimilar products are available [6]. Biosimilar infliximab (CT-P13) is a chimeric human–mouse monoclonal antibody against TNF-α. CT-P13 is frequently used as an effective and safe alternative for original infliximab (IFX) [7,8,9,10]. While it is an important drug in IBD treatment, a significant problem may be the primary lack or secondary loss of response (LOR) to therapy. Therefore, their prevention is an important subject addressed in clinical trials [11,12,13]. There is evidence to suggest that combination therapy or/and optimization of the dosing regimen can improve overall treatment efficacy [6,12].
Reactive monitoring of drug levels is a recommended practice in cases of decreased response or LOR. There are significant differences in drug requirements during maintenance treatment, as reflected by the dosage of 5 to 10 mg/kg every four to eight weeks [14,15]. The standard dosage of IFX in induction is 5 mg/kg; treatment monitoring during this period of therapy is not performed routinely and a therapeutic window has not been established for it [16]. In many studies, IFX levels were measured just before or after subsequent infusions of the drug at induction. However, little is known about the possible utility of intermediate measurements at weeks 10 and 12 and comparison between patients with CD and UC [17,18,19].
The aim of this study was to comparatively evaluate the response to treatment and the frequency of achieving and maintaining adequate (3 μg/mL) levels of CT-P13 during the induction phase at week 6 (before the third induction dose) and in the maintenance phase at weeks 10, 12, and 14 in patients with CD and UC. Furthermore, risk factors, the relationship between the level of drug and the response to induction therapy, as well as the occurrence of secondary LOR were analyzed.
2. Materials and Methods
2.1. Patients
Patients with CD and UC who qualified for the biosimilar infliximab (CT-P13, Remsima) [20] treatment within drug programs were consecutively enrolled between 2017 and 2019 at the tertiary IBD center in Rzeszow, Poland. The inclusion criterion for patients with CD was disease activity on the Crohn’s Disease Activity Index (CDAI) scale above 300 points or less, but with the presence of perianal fistulas. For patients with UC the inclusion crterion was disease activity above six points on the Mayo scale.
In both groups, CT-P13 was administered intravenously at a dose of 5 mg/kg according to the induction schedule at week 0, week 2, and week 6. In the maintenance phase, the drug was administered every four or eight weeks. The patients were monitored for 12 months.
The study was approved by the Ethics Committee of the University of Rzeszów (No 9 October 2016). Each participant read and signed an informed consent form.
2.2. CT-P13 Concentrations
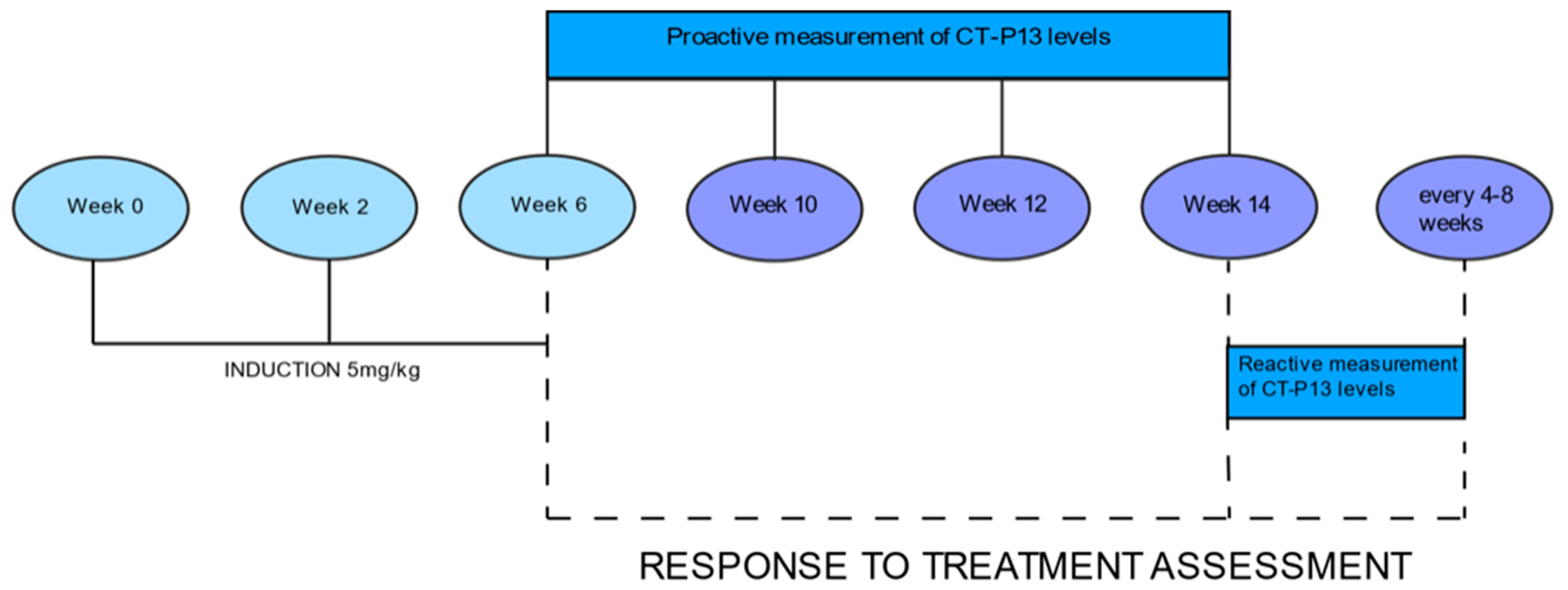
Drug levels were measured at week 6, just before the third induction dose, then at weeks 10, 12, and 14, just before the first maintenance dose (Figure 1). Serum levels of CT-P13 were evaluated using validated ELISA methods (Matriks Biotek, Ankara, Turkey). The detection range of the CT-P13 test was 0.4 μg/mL to 20 μg/mL, while the therapeutic range was established at 3 to 7 μg/mL [21]. We calculated the percentage of patients achieving CT-P13 levels equal to or greater than 3 μg/mL at each measurement.
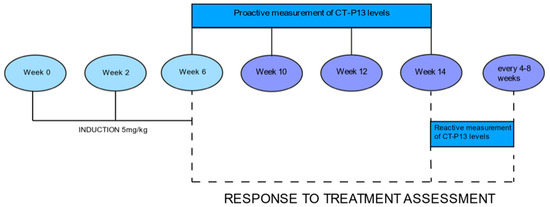
Figure 1.
3 Response to treatment.
Response to treatment was assessed at week 6, week 14, and then during maintenance treatment before each drug infusion (every four or eight weeks) for 12 months. In UC patients, the response to treatment was defined as reduction in disease activity by at least three points on the full Mayo scale and at least 30%, with decrease on the rectal bleeding subscale by at least one point [22]. In CD patients, the response to treatment was defined as reduction by at least 70 points and by at least 25% on the CDAI scale from baseline.
Primary lack of response in both groups was defined as none or little response, or deterioration after at least two infusions of infliximab. Response to treatment was analyzed at weeks 6 and 14 after three induction infusions of infliximab [23].
Secondary LOR was defined as deterioration after primary response to CT-P13 that resulted in terminating treatment or increasing dosage [24]. Response to treatment was assessed for all patients but was analyzed separately for patients who achieved drug levels of 3 μg/mL and for those with drug levels below 3 μg/mL at week 6. The same criteria were used for the assessment at week 14.
In addition, among patients with UC and CD, we analyzed the subgroups of patients who achieved the highest levels of CT-P13 (over the detection limit of 20 μg/mL) at week 6 and compared them with the patients who achieved lower drug levels.
2.3. Statistical Methods
Nominal data was presented by counts (n) and frequency of occurrence (%). Comparison of frequencies between groups was performed using the chi squared test. When group sizes did not allow for the use of the chi-squared test we performed Fisher’ s exact test. Furthermore, the ROC curves were prepared, and the optimal cut-off point for infliximab levels was determined as a diagnostic test for the response to treatment and the subsequent absence of secondary loss of response. The Youden index was used in determining the optimal cut-off point. All statistical tests were performed using R v. 4.0.5. software (The R Foundation for Statistical Computing, Wien, Austria) at a significance level of α = 0.05.
3. Results
3.1. Baseline Characteristics
The study group included 65 patients (32 with CD and 33 with UC). Patients with UC scored 7–12 points on the Mayo scale (moderate to severe disease) and CD activity ranged from 150 to 435 CDAI points. Most of the patients (86.2%) received concomitant treatment with thiopurines. Seventy-five percent of patients received additional mesalzine, and 55.4% of patients were also treated with glucocorticosteroids. Patient baseline characteristics are shown in Table 1.

Table 1.
Patient baseline characteristics.
3.2. Response to Treatment
Twenty-six of 32 (81.2%) CD patients responded to induction therapy. Primary lack of response was observed in six of 32 patients (18.8%). Loss of response was observed in 14 of 26 (53.8%) patients and could have been associated with insufficient drug levels. Subsequently, the dosage was increased to 5–10 mg/kg every four to eight weeks.
Twenty-seven of 33 (81.8%) UC patients responded to induction therapy. Primary lack of response was observed in six of 32 patients (18.2%). Loss of response was observed in 10 of 27 (37%) patients and was caused by non-therapeutic levels of infliximab (Table 2 and Table 3).
Table 2.
Number of patients with CD and UC who achieved CT-P13 level of 3 μg/mL.
Table 3.
Comparison of treatment response in both groups according to CT-P13 levels at weeks 6 and 14.
3.3. Levels of CT-P13
Additional measurements at weeks 10 and 12 did not capture a significant decrease in the percentage of patients achieving therapeutic drug concentrations compared to baseline (Table 2). A significant decrease was observed between weeks 6 and 14 in patients with UC (p = 0.014). In patients with CD, drug concentrations of 3 μg/mL were observed in 84.4% of patients at week 6, in 84.0% at week 10, in 80.0% at week 12, and in 68.7% at week 14 (Table 2). In the UC subgroup, drug levels of 3 μg/mL were found in 84.8% of patients at week 6, in 88.5% at weeks 10 and 12, and in 57.6% at week 14.
3.4. Comparative Evaluation for Patients with Crohn’s Disease and Ulcerative Colitis
3.4.1. Response to Treatment
A comparable number of patients with CD and UC (81.2% vs. 81.8%) achieved a response to induction (p > 0.999). A similar number of patients with CD (84.4%) and UC (84.8%) achieved trough levels of CT-P13 of 3 μg/mL at week 6 (p > 0.999). Some differences, although not statistically significant, were observed at week 14 when the therapeutic levels of CT-P13 were found in 68.8% patients with CD and in 57.6% patients with UC (p = 0.499) (Table 3).
In the CD subgroup, response to treatment was observed in 88.9% of patients who achieved CT-P13 levels of 3 μg/mL at week 6 and in 40% of patients whose drug levels were lower (p = 0.034). At week 14, response to treatment was found in 90.9% of patients with therapeutic drug levels and in 55.5% of patients with non-therapeutic levels of CT-P13 (p = 0.043).
In patients with UC, response to treatment was observed in 92.8% of patients with levels of CT-P13 equal to or above 3 μg/mL and in 20% of patients who did not achieve the trough drug level of 3 μg/mL at week 6 (p = 0.002). At week 14, response to treatment was found in 94.7% of patients with therapeutic drug levels and in 64.3% of patients with non-therapeutic levels of CT-P13 (p = 0.062) (Table 3). Analysis showed a statistically significant association between minimum therapeutic drug levels at week 6 and response to treatment in patients with CD and UC. At week 14, the significant relationship was found only in patients with CD.
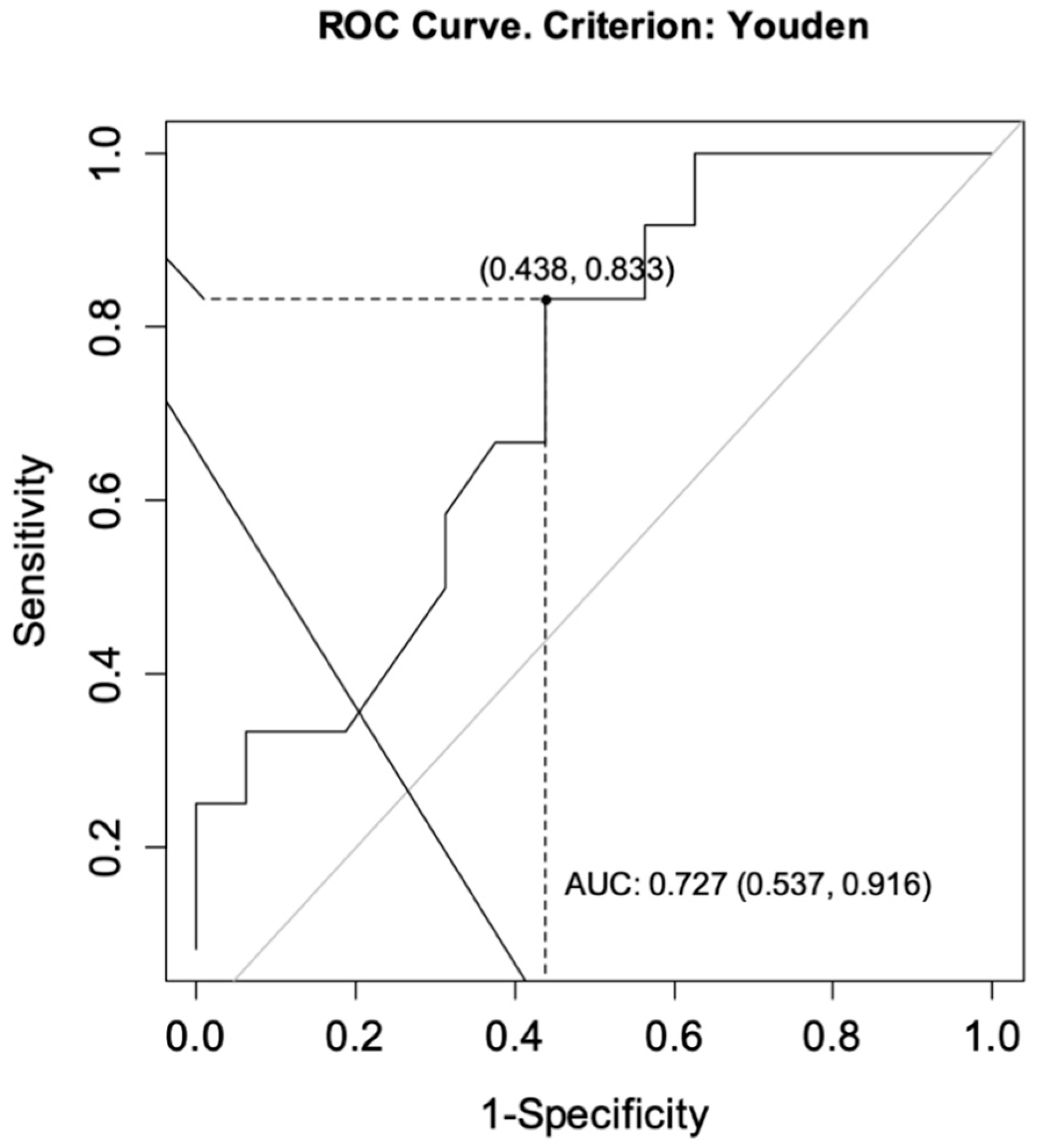
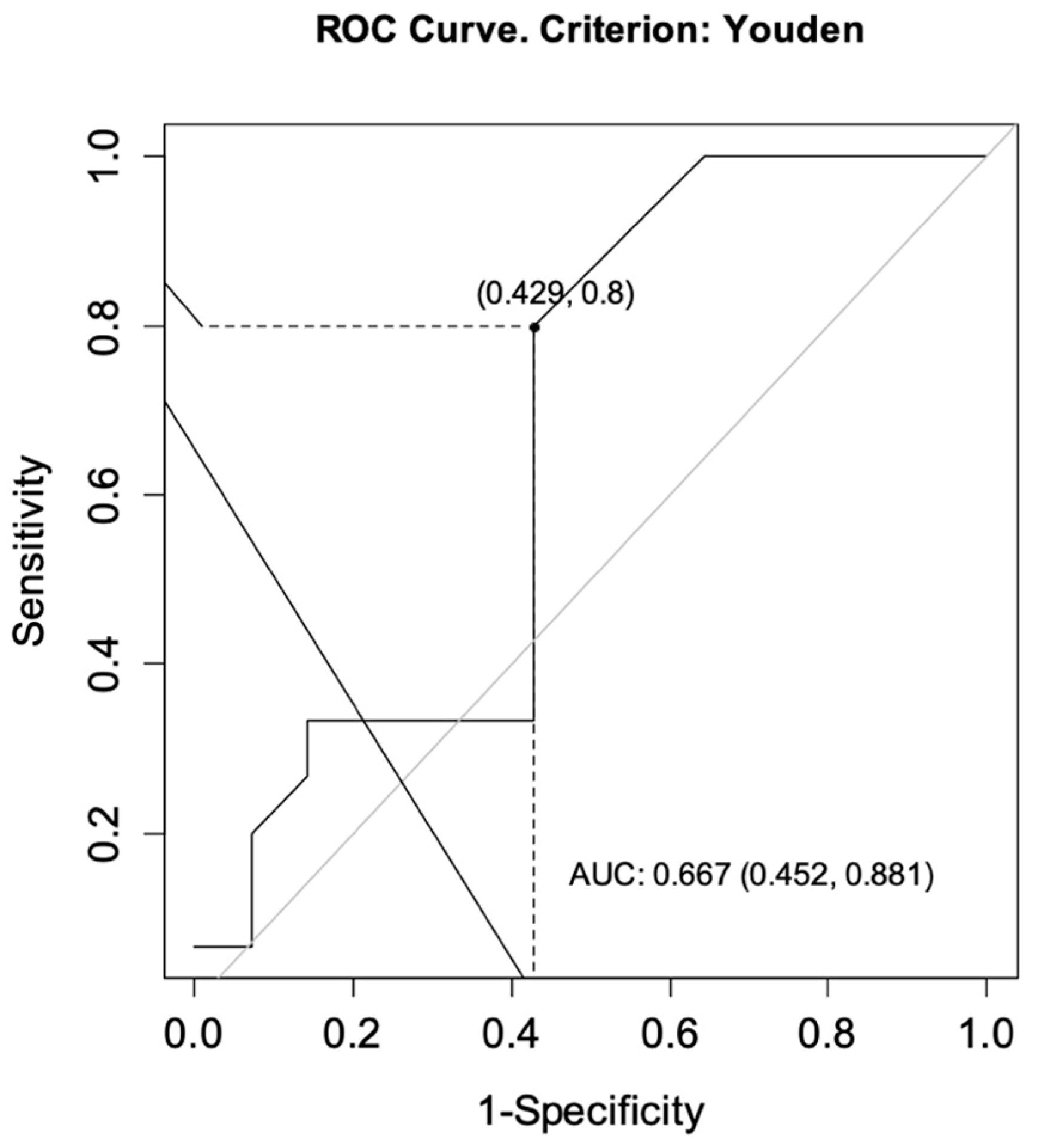
The ROC curves were drawn for each group to determine the optimal cut-off points for CT-P13 level as predictors of achieving a primary response while ensuring no secondary loss of response. For CD, the analysis showed an area under the curve (AUC) = 0.727, CI95 [0.537; 0.916] indicating satisfactory differentiation of patients by the selected diagnostic test. The optimal cut-off point for infliximab at week 14 was calculated to be 4.60 μg/mL. The sensitivity of the analysis was 83%, specificity 56%, and test accuracy 68% (Figure 2). For UC patients, the same analysis showed AUC = 0.667, CI95 [0.452; 0.881] and the optimal cut-off point for CT-P13 at week 14 was calculated to be 3.10 μg/mL. The sensitivity of the analysis was 80%, specificity 57%, and test accuracy 69% (Figure 3).
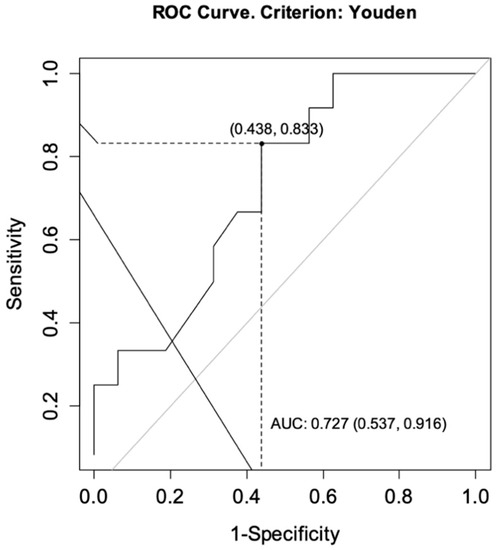
Figure 2.
ROC curve for infliximab levels as a predictor of achieving a primary response while ensuring no secondary loss of response in patients with Crohn’s disease. AUC, area under the curve.
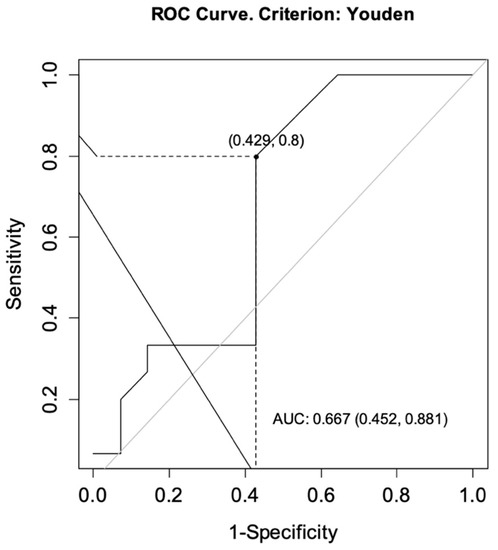
Figure 3.
ROC curve for infliximab levels as a predictor of achieving a primary response while ensuring no secondary loss of response in patients with ulcerative colitis. AUC, area under the curve.
3.4.2. Secondary Loss of Response
We observed a higher incidence of LOR in patients with CD (53.8%) compared to UC (37.0%). The difference between groups was not statistically significant (p = 0.341). Patients with CD who achieved the minimum therapeutical levels of CT-P13 at week 14 lost response more often than those with UC (45.0% vs. 27.8%), but again, the difference was not statistically significant (p = 0.272). Among patients who did not reach the therapeutic minimum of the drug at week 14, all the patients with CD versus 55.5% of patients with UC lost their response to infliximab treatment. The differences were not statistically significant (p = 0.272) (Table 3).
3.4.3. Risk Factors
A higher incidence of primary non-response or LOR was not confirmed for any of the potential risk factors (sex, lack of thiopurine use, history of infliximab treatment) (Table 4 and Table 5).
Table 4.
Primary lack of response.
Table 5.
Secondary loss of response.
3.4.4. Highest CT-P13 Levels
An additional focus of the analysis was to evaluate patients with the highest CT-P13 levels (>20 μg/mL, above the assay detection level) found at weeks 6 and 10 in both groups for any advantage in achieving a response to induction therapy compared to the other patients. The results are shown in Table 6.
Table 6.
CT-P13 levels >20 μg/mL and < 20 μg/mL at weeks 6 and 10 in patients with CD and UC and response to treatment.
In both groups, similar numbers of patients achieved CT-P13 levels greater than 20 μg/mL at weeks 6 and 10 (43.7% in CD and 39.4% in UC). In these patients, a high induction response rate was achieved (85.8% in CD and 92.3% in UC). The results were compared with a 66.6% response rate in CD and a 70% response rate in UC for patients who had lower CT-P13 levels at weeks 6 and 10, but the difference was not statistically significant. No association was confirmed between drug levels greater than 20 μg/mL at weeks 6 and 10 and response to induction (p = 0.412 in CD, p = 0.202 in UC). All patients with CD and only 76.9% of patients with UC who achieved CT-P13 levels above 20 μg/mL at weeks 6 and 10 maintained minimal therapeutic drug levels at week 14 (p = 0.098). There was also a high rate of LOR among patients with the highest drug levels: 50% in CD and 25% in UC (p = 0.400).
4. Discussion
Monitoring of biologic therapy with anti-TNF-α drugs can be proactive or reactive and is most often performed during the maintenance phase to optimize therapy. The benefits of reactive monitoring during maintenance treatment have been demonstrated [24,25]. Proactive monitoring and monitoring during induction analyzed in studies give different and sometimes contradictory results [26,27,28,29]. Many studies show that IFX levels in adult and pediatric patients responding to induction are significantly higher than in non-responding patients [30,31,32,33].
We found similar results in our previous study where the mean drug concentration in responders was 16.7 μg/mL, while in the group with no response it was 0.95 μg/mL [34]. In the current study, we attempted to determine the drug level that was associated with clinical response and with no LOR during one year of treatment. We identified a cut-off point for biosimilar IFX at week 14 of 4.6 μg/mL for CD and of 3.1 μg/mL for UC. Post-hoc analysis of the ACCENT I trial showed that sustained clinical response in patients with CD was associated with IFX levels equal to or greater than 3.5 μg/mL at week 14 [35]. A much higher IFX level of 7 µg/mL was found to be optimal and associated with remission at weeks 14 and 54 in the British PANTS trial, which included patients with CD treated with original and biosimilar IFX [31]. For UC patients, mucosal healing was associated with infliximab concentrations ≥5.1 μg/mL at week 14 and ≥2.3 μg/mL at week 30. Endoscopic remission was observed with IFX concentrations ≥6.7 μg/mL at week 14 and ≥3.8 μg/mL at week 30 [36]. These differences seem to suggest that the optimal level of IFX to ensure response or remission may be highly individual and dependent on many factors, including disease severity, as demonstrated in a group of children with UC treated at a dose of 5 or 10 mg/kg in induction [37].
However, recent studies show that monitoring of treatment at induction and dose selection based on drug concentration to achieve appropriately high post-induction levels of IFX may not be beneficial in IBD or other autoimmune diseases [38]. In our study, we also assessed a group of patients who had the highest (over the test detection level of 20 µg/mL) CT-P13 concentrations at week 6 and 10 and we compared them with the rest of the patients. Twenty-seven of 65 patients had the highest drug levels; however, we did not observe a statistically higher number of patients experiencing primary response nor decreased risk LOR in this subgroup. In patients with UC, the highest CT-P13 levels before last induction dose and four weeks later resulted in therapeutic drug levels (3 μg/mL) at week 14 (before the first maintenance dose) in only 75% of patients.
Despite these results, the data we analyzed on biosimilar IFX levels in association with treatment response support the benefit of proactive monitoring. The results suggest that proactive monitoring at weeks 6 and 14 provides important information because, as our previous study showed, indeterminate levels of biosimilar IFX at week 6 were associated with a high risk of immunization and nonresponse to therapy [34]. These results are in line with other research [34,39]. As for the intermediate measurements at weeks 10 and 12, our data did not confirm their usefulness in either CD or UC because IFX concentrations in more than 80% of patients were still within therapeutic limits. A significant deficiency of the drug was seen only at week 14; nevertheless, a decreasing trend could be detected at week 12 in some patients.
An interesting observation that suggests the utility of proactive monitoring is that primary response was achieved by more than 81% of patients in both groups but much fewer patients, only 68.8% of CD patients and 57.6% of UC patients, achieved the minimum therapeutic levels of CT-P13 at the end of induction. This shows that a considerable group of patients responded to induction treatment despite non-therapeutic drug levels. This was more evident in the UC group, as the non-therapeutic drug levels at week 14 were shown to be unrelated to non-response. This might have been caused by the influence of corticosteroids, which were used in more than 60% of UC patients at the start of treatment and may have masked both clinical and endoscopic response. At follow-up, all patients with CD and more than half of the patients with UC in this subgroup had lost response to treatment. This suggests that patients with non-therapeutic drug levels at week 14 require further monitoring and surveillance as the risk of LOR is significant in these patients. In our study, this was particularly evident in the CD group.
A limitation of this study is a relatively small patient group, which means that statistical differences between subgroups were not apparent. It would probably be worth continuing similar studies on a larger group of patients with IBD to verify the initial findings.
5. Conclusions
There is an unmet clinical need to establish IFX values predictive of treatment response for early identification of the subgroup of IBD patients that have the highest probability of non-response for potential IFX dosage adjustment. In our study, we have shown that overall response rate in both CD and UC exceeded 80% and there were no significant differences in primary response and biosimilar IFX levels across measurement points for both CD and UC groups. Intermediate measurements of drug levels at weeks 10 and 12 did not capture any pronounced decrease in IFX concentrations below therapeutic levels in either group.
The study also showed that the group of patients who achieved the highest levels of CT-P13 before the third induction dose was not significantly different from the other patients in terms of response to induction and LOR. A significant number of patients who achieved a primary response presented subtherapeutic levels of CT-P13 at week 14.
Author Contributions
Conceptualization, A.P. and R.F.; methodology, A.P.; software, A.P; validation, A.P. and R.F.; formal analysis, A.P. and R.F.; investigation, A.P. and R.F.; resources, R.F.; data curation, A.P. and R.F.; writing—original draft preparation, A.P. and R.F.; writing—review and editing, A.P. and R.F.; visualization, A.P. and R.F.; supervision, R.F.; project administration, R.F. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received to assist with the preparation of this manuscript.
Institutional Review Board Statement
The study protocol was approved by the Ethics Committee of the University of Rzeszów (No. 9 October 2016).
Informed Consent Statement
Each participant read and signed an informed consent form.
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhang, Y.Z.; Li, Y.Y. Inflammatory bowel disease: Pathogenesis. World J. Gastroenterol. 2014, 20, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.R.; Colombel, J.F.; Ungaro, R. The Role of Early Biologic Therapy in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 1896–1905. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohns Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef]
- Roberti, R.; Iannone, L.F.; Palleria, C.; De Sarro, C.; Spagnuolo, R.; Barbieri, M.A.; Vero, A.; Manti, A.; Pisana, V.; Fries, W.; et al. Safety profiles of biologic agents for inflammatory bowel diseases: A prospective pharmacovigilance study in Southern Italy. Curr. Med. Res. Opin. 2020, 36, 1457–1463. [Google Scholar] [CrossRef]
- Spagnuolo, R.; Dastoli, S.; Silvestri, M.; Cosco, C.; Garieri, P.; Bennardo, L.; Nisticò, S.P. Anti-interleukin 12/23 in the treatment of erythema nodosum and Crohn disease: A case report. Dermatol. Ther. 2019, 32, 12811. [Google Scholar] [CrossRef]
- Papamichael, K.; Vogelzang, E.H.; Lambert, J.; Wolbink, G.; Cheifetz, A.S. Therapeutic drug monitoring with biologic agents in immune mediated inflammatory diseases. Expert Rev. Clin. Immunol. 2019, 15, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Lee, J.H.; Hong, S.N.; Yoon, H.; Kang, H.W.; Lee, S.H.; Im, J.P.; Cha, J.M.; Eun, C.S.; Kim, J.W.; et al. Long-term efficacy and safety of CT-P13, a biosimilar of infliximab, in patients with inflammatory bowel disease: A retrospective multicenter study. J. Gastroenterol. Hepatol. 2019, 34, 1523–1532. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, Y.H.; Lee, J.H.; Kwon, H.J.; Lee, S.H.; Park, D.I.; Kim, H.K.; Cheon, J.H.; Im, J.P.; Kim, Y.S.; et al. Post-marketing study of biosimilar infliximab (CT-P13) to evaluate its safety and efficacy in Korea. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H.; Park, J.C.; Lukas, M.; Kolar, M.; Loftus, E.V. Biosimilars: Concept, current status, and future perspectives in inflammatory bowel diseases. Intest. Res. 2020, 18, 34–44. [Google Scholar] [CrossRef] [Green Version]
- van Deventer, S.J. Review article: Targeting TNF alpha as a key cytokine in the inflammatory processes of Crohn’s disease—The mechanisms of action of infliximab. Aliment. Pharmacol. Ther. 1999, 13, 3–8; discussion 38. [Google Scholar] [CrossRef]
- Guerbau, L.; Gerard, R.; Duveau, N.; Staumont-Salle, D.; Branche, J.; Maunoury, V.; Cattan, S.; Wils, P.; Boualit, M.; Libier, L.; et al. Patients with Crohn’s Disease with High Body Mass Index Present More Frequent and Rapid Loss of Response to Infliximab. Inflamm. Bowel Dis. 2017, 23, 1853–1859. [Google Scholar] [CrossRef] [Green Version]
- Roblin, X.; Williet, N.; Boschetti, G.; Phelip, J.M.; Del Tedesco, E.; Berger, A.E.; Vedrines, P.; Duru, G.; Peyrin-Biroulet, L.; Nancey, S.; et al. Addition of azathioprine to the switch of anti-TNF in patients with IBD in clinical relapse with undetectable anti-TNF trough levels and antidrug antibodies: A prospective randomised trial. Gut 2020, 69, 1206–1212. [Google Scholar] [CrossRef]
- Viazis, N.; Koukouratos, T.; Anastasiou, J.; Giakoumis, M.; Triantos, C.; Tsolias, C.; Theocharis, G.; Karamanolis, D.G. Azathioprine discontinuation earlier than 6 months in Crohn’s disease patients started on anti-TNF therapy is associated with loss of response and the need for anti-TNF dose escalation. Eur. J. Gastroenterol. Hepatol. 2015, 27, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Chen, B.L.; Mao, R.; Zhang, S.H.; He, Y.; Zeng, Z.R.; Ben-Horin, S.; Chen, M.H. Systematic review with meta-analysis: Loss of response and requirement of anti-TNFalpha dose intensification in Crohn’s disease. J. Gastroenterol. 2017, 52, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Taxonera, C.; Olivares, D.; Mendoza, J.L.; Diaz-Rubio, M.; Rey, E. Need for infliximab dose intensification in Crohn’s disease and ulcerative colitis. World J. Gastroenterol. 2014, 20, 9170–9177. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Casteele, N.V.; Ferrante, M.; Gils, A.; Cheifetz, A.S. Therapeutic Drug Monitoring during Induction of Anti-Tumor Necrosis Factor Therapy in Inflammatory Bowel Disease: Defining a Therapeutic Drug Window. Inflamm. Bowel Dis. 2017, 23, 1510–1515. [Google Scholar] [CrossRef] [Green Version]
- Beltran, B.; Iborra, M.; Saez-Gonzalez, E.; Marques-Minana, M.R.; Moret, I.; Cerrillo, E.; Tortosa, L.; Bastida, G.; Hinojosa, J.; Poveda-Andres, J.L.; et al. Fecal Calprotectin Pretreatment and Induction Infliximab Levels for Prediction of Primary Nonresponse to Infliximab Therapy in Crohn’s Disease. Dig. Dis. 2019, 37, 108–115. [Google Scholar] [CrossRef]
- Clarkston, K.; Tsai, Y.T.; Jackson, K.; Rosen, M.J.; Denson, L.A.; Minar, P. Development of Infliximab Target Concentrations during Induction in Pediatric Crohn Disease Patients. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 68–74. [Google Scholar] [CrossRef] [PubMed]
- van Hoeve, K.; Dreesen, E.; Hoffman, I.; Van Assche, G.; Ferrante, M.; Gils, A.; Vermeire, S. Adequate Infliximab Exposure during Induction Predicts Remission in Paediatric Patients with Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 847–853. [Google Scholar] [CrossRef]
- Ilias, A.; Gonczi, L.; Kurti, Z.; Lakatos, P.L. Biosimilars in ulcerative colitis: When and for who? Best Pract. Res. Clin. Gastroenterol. 2018, 32–33, 35–42. [Google Scholar] [CrossRef]
- Novakovic, V.; Abdija, S.; Larsen, P.B.; Fenger, M.; Gredal, L.; Jacobsen, K.K. Comparison of the Quantum Blue(R) reader Point-of-Care system versus ELISA technique for therapeutic drug monitoring of Infliximab levels. Clin. Biochem. 2019, 74, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Mei, W.Q.; Hu, H.Z.; Liu, Y.; Li, Z.C.; Wang, W.G. Infliximab is superior to other biological agents for treatment of active ulcerative colitis: A meta-analysis. World J. Gastroenterol. 2015, 21, 6044–6051. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Hanauer, S.B. Assessing response and loss of response to biological therapies in IBD. Am. J. Gastroenterol. 2011, 106, 685–698. [Google Scholar] [CrossRef]
- Negoescu, D.M.; Enns, E.A.; Swanhorst, B.; Baumgartner, B.; Campbell, J.P.; Osterman, M.T.; Papamichael, K.; Cheifetz, A.S.; Vaughn, B.P. Proactive vs Reactive Therapeutic Drug Monitoring of Infliximab in Crohn’s Disease: A Cost-Effectiveness Analysis in a Simulated Cohort. Inflamm. Bowel Dis. 2020, 26, 103–111. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S.; Melmed, G.Y.; Irving, P.M.; Casteele, N.V.; Kozuch, P.L.; Raffals, L.E.; Baidoo, L.; Bressler, B.; Devlin, S.M.; et al. Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2019, 17, 1655–1668. [Google Scholar] [CrossRef] [Green Version]
- Casteele, N.V.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. Trough concentrations of infliximab guide dosing for patients with inflammatory bowel disease. Gastroenterology 2015, 148, 1320–1329. [Google Scholar] [CrossRef]
- D’Haens, G.; Vermeire, S.; Lambrecht, G.; Baert, F.; Bossuyt, P.; Pariente, B.; Buisson, A.; Bouhnik, Y.; Filippi, J.; Woude, J.V.; et al. Increasing Infliximab dose Based on Symptoms, Biomarkers, and Serum Drug Concentrations does not Increase Clinical, Endoscopic, and Corticosteroid-Free Remission in Patients with Active Luminal Crohn’s Disease. Gastroenterology 2018, 154, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Chachu, K.A.; Vajravelu, R.K.; Vaughn, B.P.; Ni, J.; Osterman, M.T.; Cheifetz, A.S. Improved Long-term Outcomes of Patients with Inflammatory Bowel Disease Receiving Proactive Compared with Reactive Monitoring of Serum Concentrations of Infliximab. Clin. Gastroenterol. Hepatol. 2017, 15, 1580–1588. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S. Therapeutic Drug Monitoring in IBD: The New Standard-of-Care for Anti-TNF Therapy. Am. J. Gastroenterol. 2017, 112, 673–676. [Google Scholar] [CrossRef]
- Dreesen, E.; Baert, F.; Laharie, D.; Bossuyt, P.; Bouhnik, Y.; Buisson, A.; Lambrecht, G.; Louis, E.; Oldenburg, B.; Pariente, B.; et al. Monitoring a Combination of Calprotectin and Infliximab Identifies Patients with Mucosal Healing of Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 637–646. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Heap, G.A.; Green, H.D.; Hamilton, B.; Bewshea, C.; Walker, G.J.; Thomas, A.; Nice, R.; Perry, M.H.; Bouri, S.; et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: A prospective, multicentre, cohort study. Lancet Gastroenterol. Hepatol. 2019, 4, 341–353. [Google Scholar] [CrossRef] [Green Version]
- Papamichael, K.; Van Stappen, T.; Casteele, N.V.; Gils, A.; Billiet, T.; Tops, S.; Claes, K.; Van Assche, G.; Rutgeerts, P.; Vermeire, S.; et al. Infliximab Concentration Thresholds during Induction Therapy Are Associated with Short-term Mucosal Healing in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2016, 14, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Casteele, N.V.; Papamichael, K.; Jeyarajah, J.; Osterman, M.T.; Cheifetz, A.S. DOP45 Adequate infliximab exposure during the induction phase is associated with early complete fistula response in patients with fistulizing Crohn’s disease: A post-hoc analysis of the ACCENT-2 trial. J. Crohns Colitis 2019, 13, S053–S054. [Google Scholar] [CrossRef]
- Pekala, A.; Filip, R.; Aebisher, D. Anti-Drug Antibodies in Patients with Inflammatory Bowel Diseases Treated with Biosimilar Infliximab: A Prospective Cohort Study. J. Clin. Med. 2021, 10, 2653. [Google Scholar] [CrossRef] [PubMed]
- Cornillie, F.; Hanauer, S.B.; Diamond, R.H.; Wang, J.; Tang, K.L.; Xu, Z.; Rutgeerts, P.; Vermeire, S. Postinduction serum infliximab trough level and decrease of C-reactive protein level are associated with durable sustained response to infliximab: A retrospective analysis of the ACCENT I trial. Gut 2014, 63, 1721–1727. [Google Scholar] [CrossRef] [PubMed]
- Casteele, N.V.; Jeyarajah, J.; Jairath, V.; Feagan, B.G.; Sandborn, W.J. Infliximab Exposure-Response Relationship and Thresholds Associated with Endoscopic Healing in Patients with Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2019, 17, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.; Dolce, P.; Devas, N.; Baldassano, R.; Martinelli, M. Post-induction infliximab trough levels and disease activity in the clinical evolution of pediatric ulcerative colitis. United Eur. Gastroenterol. J. 2020, 8, 425–435. [Google Scholar] [CrossRef]
- Syversen, S.W.; Goll, G.L.; Jorgensen, K.K.; Sandanger, O.; Sexton, J.; Olsen, I.C.; Gehin, J.E.; Warren, D.J.; Brun, M.K.; Klaasen, R.A.; et al. Effect of Therapeutic Drug Monitoring vs Standard Therapy during Infliximab Induction on Disease Remission in Patients with Chronic Immune-Mediated Inflammatory Diseases: A Randomized Clinical Trial. JAMA 2021, 325, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Brandse, J.F.; Mathot, R.A.; van der Kleij, D.; Rispens, T.; Ashruf, Y.; Jansen, J.M.; Rietdijk, S.; Lowenberg, M.; Ponsioen, C.Y.; Singh, S.; et al. Pharmacokinetic Features and Presence of Antidrug Antibodies Associate with Response to Infliximab Induction Therapy in Patients with Moderate to Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2016, 14, 251–258. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).