
Defining the Normal Growth Curve of Fetal Fractional Limb Volume in a Japanese Population

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Prenatal Ultrasonography
2.3. Birth Outcomes
2.4. Pre-Pregnancy Body Mass Index and Gestational Weight Gain
2.5. Statistical Analysis
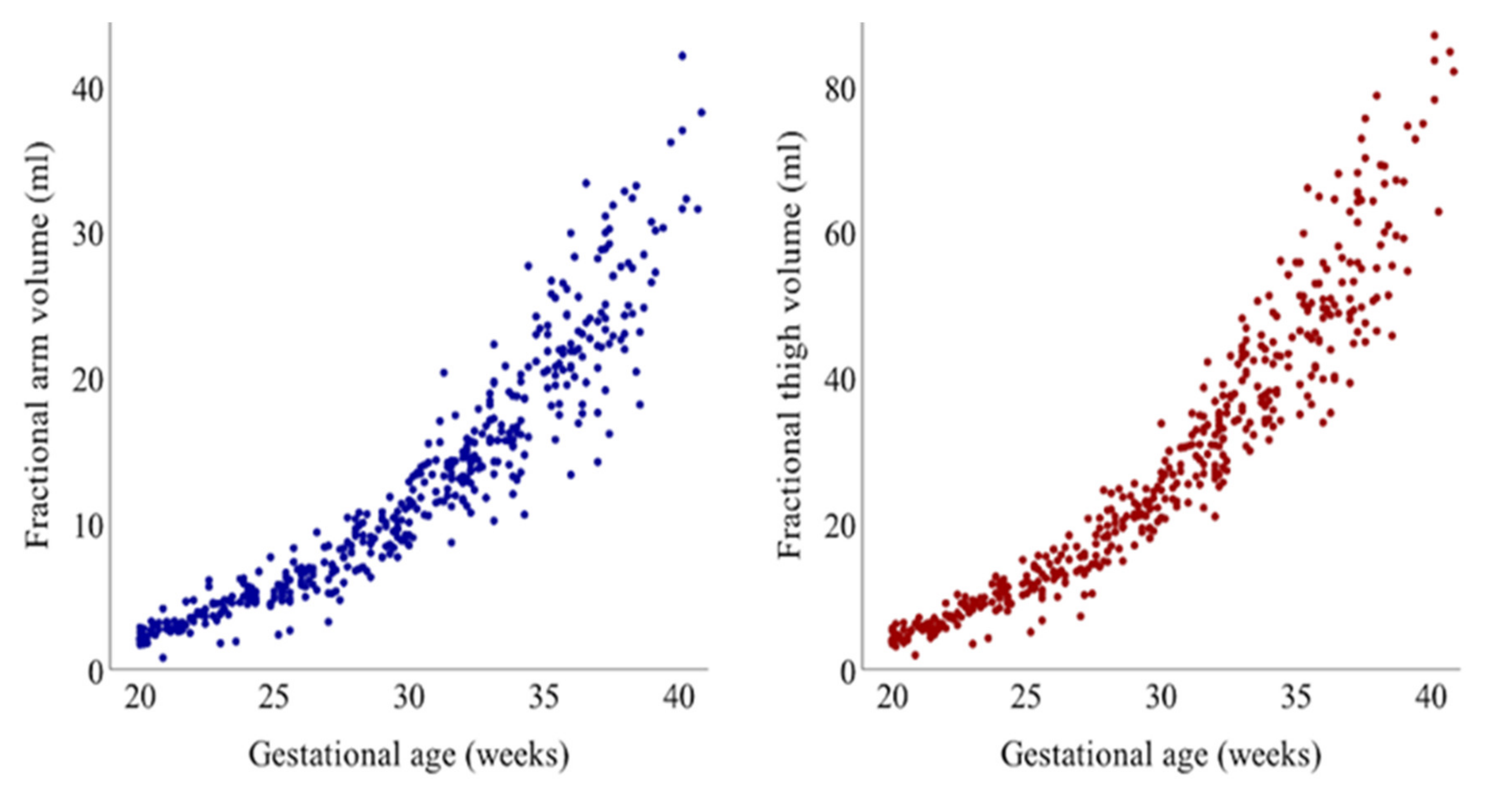
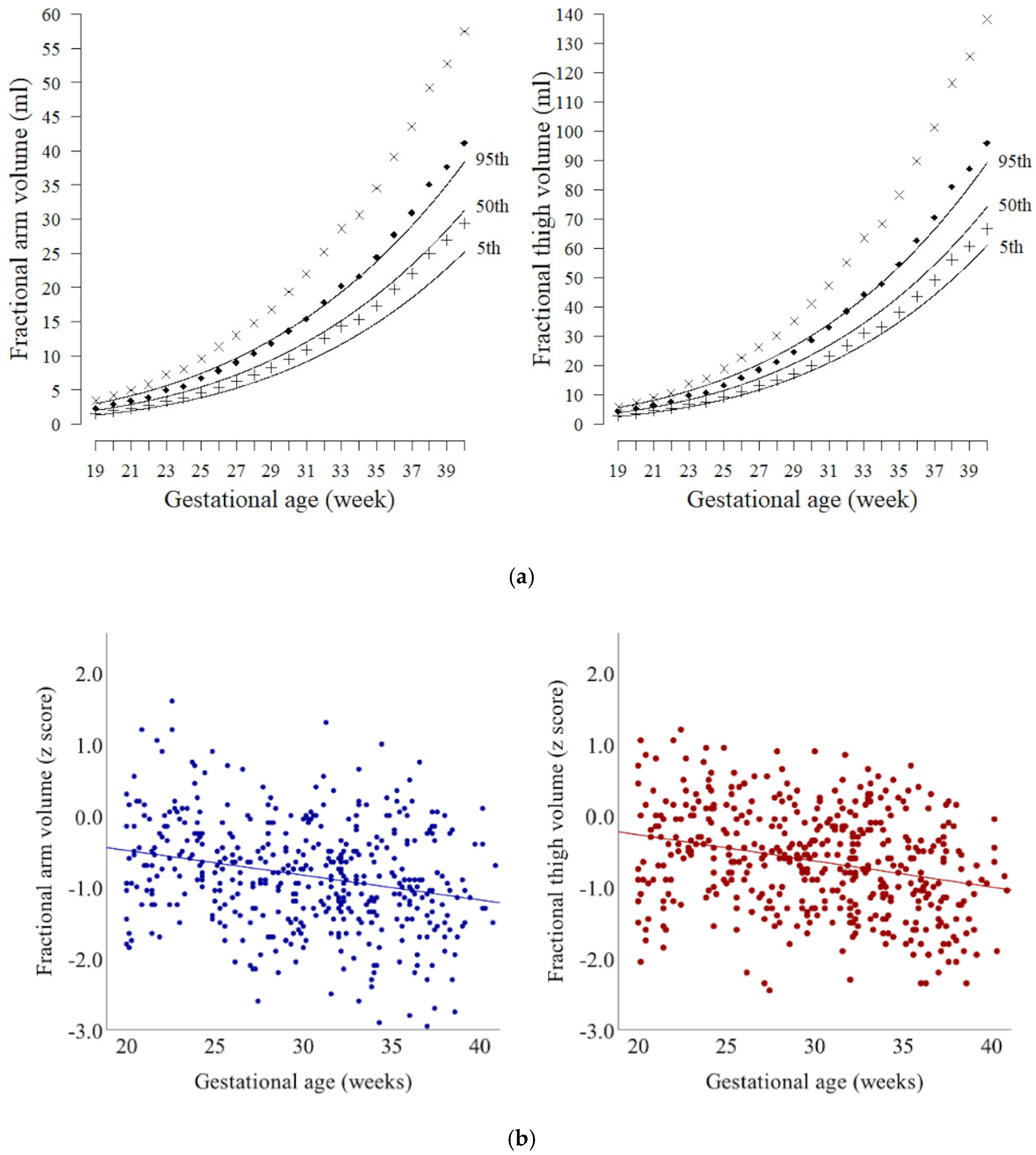
3. Results
4. Discussion
4.1. Principal Findings
4.2. Clinical Implications
4.3. Research Implications
4.4. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| AVol | fractional arm volume |
| TVol | fractional thigh volume |
References
- Committee on Practice Bulletins—Obstetrics. Macrosomia: ACOG Practice Bulletin, Number 216. Obstet. Gynecol. 2020, 135, e18–e35. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics and the Society for Maternal-Fetal Medicin. ACOG Practice Bulletin No. 204: Fetal Growth Restriction. Obstet. Gynecol. 2019, 133, e97–e109. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Winter, P.D.; Osmond, C.; Margetts, B.; Simmonds, S.J. Weight in infancy and death from ischaemic heart disease. Lancet 1989, 2, 577–580. [Google Scholar] [CrossRef]
- Lee, W.; Mack, L.M.; Sangi-Haghpeykar, H.; Gandhi, R.; Wu, Q.; Kang, L.; Canavan, T.P.; Gatina, R.; Schild, R.L. Fetal weight estimation using automated fractional limb volume with 2-dimensional size parameters: A multicenter study. J. Ultrasound Med. 2020, 39, 1317–1324. [Google Scholar] [CrossRef]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements—A prospective study. Am. J. Obstet. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef]
- Lee, W.; Deter, R.L.; Ebersole, J.D.; Huang, R.; Blanckaert, K.; Romero, R. Birth weight prediction by three-dimensional ultrasonography: Fractional limb volume. J. Ultrasound Med. 2001, 20, 1283–1292. [Google Scholar] [CrossRef]
- Miller, J.M., Jr.; Kissling, G.A.; Brown, H.L.; Gabert, H.A. Estimated fetal weight: Applicability to small- and large-for-gestational-age fetus. J. Clin. Ultrasound 1988, 16, 95–97. [Google Scholar] [CrossRef]
- Sparks, J.W. Human intrauterine growth and nutrient accretion. Semin. Perinatol. 1984, 8, 74–93. [Google Scholar]
- Salomon, L.J.; Alfirevic, Z.; Da Silva Costa, F.; Deter, R.L.; Figueras, F.; Ghi, T.; Glanc, P.; Khalil, A.; Lee, W.; Napolitano, R.; et al. ISUOG Practice Guidelines: Ultrasound assessment of fetal biometry and growth. Ultrasound Obstet. Gynecol. 2019, 53, 715–723. [Google Scholar] [CrossRef]
- Simcox, L.E.; Myers, J.E.; Cole, T.J.; Johnstone, E.D. Fractional fetal thigh volume in the prediction of normal and abnormal fetal growth during the third trimester of pregnancy. Am. J. Obstet. Gynecol. 2017, 217, 453.e1–453.e12. [Google Scholar] [CrossRef]
- Lee, W.; Balasubramaniam, M.; Deter, R.L.; Hassan, S.S.; Gotsch, F.; Kusanovic, J.P.; Goncalves, L.F.; Romero, R. Fetal growth parameters and birth weight: Their relationship to neonatal body composition. Ultrasound Obstet. Gynecol. 2009, 33, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.; Balasubramaniam, M.; Deter, R.L.; Hassan, S.S.; Gotsch, F.; Kusanovic, J.P.; Goncalves, L.F.; Romero, R. Fractional limb volume—A soft tissue parameter of fetal body composition: Validation, technical considerations and normal ranges during pregnancy. Ultrasound Obstet. Gynecol. 2009, 33, 427–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morisaki, N.; Kawachi, I.; Oken, E.; Fujiwara, T. Social and anthropometric factors explaining racial/ethnical differences in birth weight in the United States. Sci. Rep. 2017, 7, 46657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, G.R. Nutritional Assessment. In Fetal and Neonatal Physiology, 4th ed.; Polin, R.A., Fox, W.W., Abman, S.H., Eds.; Elsevier: Philadelphia, PA, USA, 2011; pp. 341–351. [Google Scholar]
- Akiba, Y.; Ikenoue, S.; Endo, T.; Kasuga, Y.; Ochiai, D.; Miyakoshi, K.; Ishii, R.; Yakubo, K.; Tanaka, M. Differences in fetal fractional limb volume changes in normal and gestational diabetic pregnancies: An exploratory observational study. BJOG 2021, 128, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Itabashi, K.; Miura, F.; Uehara, R.; Nakamura, Y. New Japanese neonatal anthropometric charts for gestational age at birth. Pediatr. Int. 2014, 56, 702–708. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists, American Institute of Ultrasound in Medicine, and Society for Maternal-Fetal Medicine. Committee opinion no 611: Method for estimating due date. Obstet. Gynecol. 2014, 124, 863–866. [Google Scholar] [CrossRef]
- Japan Society of Ultrasound in Medicine. Ultrasound Fetal measurement standardization and Japanese standard. J. Med. Ultrason. 2003, 30, 416–440. [Google Scholar]
- Spong, C.Y. Defining “term” pregnancy: Recommendations from the Defining “Term” Pregnancy Workgroup. JAMA 2013, 309, 2445–2446. [Google Scholar] [CrossRef]
- Lee, W.; Deter, R.L.; McNie, B.; Goncalves, L.F.; Espinoza, J.; Chaiworapongsa, T.; Balasubramaniam, M.; Romero, R. The fetal arm: Individualized growth assessment in normal pregnancies. J. Ultrasound Med. 2005, 24, 817–828. [Google Scholar] [CrossRef]
- Lee, W.; Deter, R.L.; McNie, B.; Goncalves, L.F.; Espinoza, J.; Chaiworapongsa, T.; Romero, R. Individualized growth assessment of fetal soft tissue using fractional thigh volume. Ultrasound Obstet. Gynecol. 2004, 24, 766–774. [Google Scholar] [CrossRef]
- Poissonnet, C.M.; Burdi, A.R.; Garn, S.M. The chronology of adipose tissue appearance and distribution in the human fetus. Early Hum. Dev. 1984, 10, 1–11. [Google Scholar] [CrossRef]
- Kuzawa, C.W. Adipose tissue in human infancy and childhood: An evolutionary perspective. Am. J. Phys. Anthropol. 1998, (Suppl. 27), 177–209. [Google Scholar] [CrossRef]
- Kuzawa, C.W.; Chugani, H.T.; Grossman, L.I.; Lipovich, L.; Muzik, O.; Hof, P.R.; Wildman, D.E.; Sherwood, C.C.; Leonard, W.R.; Lange, N. Metabolic costs and evolutionary implications of human brain development. Proc. Natl. Acad. Sci. USA 2014, 111, 13010–13015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bougneres, P.F.; Lemmel, C.; Ferre, P.; Bier, D.M. Ketone body transport in the human neonate and infant. J. Clin. Investig. 1986, 77, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Sparks, J.W.; Girard, J.R.; Battaglia, F.C. An estimate of the caloric requirements of the human fetus. Biol. Neonate 1980, 38, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Pagani, G.; Palai, N.; Zatti, S.; Fratelli, N.; Prefumo, F.; Frusca, T. Fetal weight estimation in gestational diabetic pregnancies: Comparison between conventional and three-dimensional fractional thigh volume methods using gestation-adjusted projection. Ultrasound Obstet. Gynecol. 2014, 43, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Deter, R.L.; Lee, W.; Yeo, L.; Erez, O.; Ramamurthy, U.; Naik, M.; Romero, R. Individualized growth assessment: Conceptual framework and practical implementation for the evaluation of fetal growth and neonatal growth outcome. Am. J. Obstet. Gynecol. 2018, 218, S656–S678. [Google Scholar] [CrossRef] [Green Version]
- Catalano, P.M.; Kirwan, J.P. Maternal factors that determine neonatal size and body fat. Curr. Diab. Rep. 2001, 1, 71–77. [Google Scholar] [CrossRef]
- Waters, T.P.; Huston-Presley, L.; Catalano, P.M. Neonatal body composition according to the revised institute of medicine recommendations for maternal weight gain. J. Clin. Endocrinol. Metab. 2012, 97, 3648–3654. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | n (%) or Mean ± SD |
|---|---|
| Maternal Characteristics | |
| Age, years | 32.5 ± 5.7 |
| Pre-pregnancy BMI, kg/m2 | 21.7 ± 3.2 |
| Underweight (BMI < 18.5) | 27 (11%) |
| Normal weight (18.5 ≤ BMI < 25) | 188 (76%) |
| Overweight/Obese (BMI ≥ 25.0) | 32 (13%) |
| Gestational weight gain, kg | 9.1 ± 4.5 |
| Primiparous | 128 (52%) |
| Newborn Characteristics | |
| Gestational age at birth, weeks | 38.0 ± 2.3 |
| Birth weight, g | 2841 ± 503 |
| Birth weight percentile, % | 53.2 ± 27.5 |
| Small for gestational age (birth weight < 10th centile) | 19 (8%) |
| Appropriate for gestational age | 205 (83%) |
| Large for gestational age (birth weight ≥ 90th centile) | 23 (9%) |
| Infant sex (female) | 122 (49%) |
| Gestational Age (Weeks) | n | Fractional Arm Volume | Fractional Thigh Volume | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5th | 10th | 25th | 50th | 75th | 90th | 95th | 5th | 10th | 25th | 50th | 75th | 90th | 95th | ||
| 20 | 23 | 1.7 | 1.8 | 2.0 | 2.4 | 2.8 | 3.1 | 3.3 | 3.4 | 3.6 | 4.0 | 4.6 | 5.2 | 5.9 | 6.2 |
| 21 | 20 | 2.0 | 2.1 | 2.4 | 2.8 | 3.3 | 3.7 | 3.9 | 4.2 | 4.4 | 4.9 | 5.6 | 6.3 | 7.1 | 7.5 |
| 22 | 17 | 2.5 | 2.6 | 2.9 | 3.4 | 3.8 | 4.3 | 4.5 | 5.1 | 5.4 | 6.0 | 6.8 | 7.6 | 8.4 | 8.8 |
| 23 | 16 | 2.9 | 3.0 | 3.4 | 3.9 | 4.5 | 5.0 | 5.3 | 6.2 | 6.5 | 7.2 | 8.1 | 9.1 | 10.0 | 10.5 |
| 24 | 20 | 3.4 | 3.6 | 4.0 | 4.6 | 5.2 | 5.8 | 6.1 | 7.4 | 7.8 | 8.6 | 9.6 | 10.7 | 11.8 | 12.4 |
| 25 | 22 | 4.0 | 4.2 | 4.7 | 5.4 | 6.1 | 6.7 | 7.0 | 8.8 | 9.3 | 10.2 | 11.3 | 12.6 | 13.8 | 14.5 |
| 26 | 18 | 4.7 | 4.9 | 5.5 | 6.2 | 7.0 | 7.7 | 8.1 | 10.4 | 10.9 | 12.0 | 13.3 | 14.7 | 16.0 | 16.8 |
| 27 | 22 | 5.4 | 5.7 | 6.3 | 7.1 | 8.0 | 8.8 | 9.2 | 12.2 | 12.8 | 14.0 | 15.5 | 17.0 | 18.5 | 19.4 |
| 28 | 22 | 6.3 | 6.6 | 7.3 | 8.2 | 9.1 | 10.0 | 10.5 | 14.2 | 14.9 | 16.3 | 17.9 | 19.6 | 21.3 | 22.4 |
| 29 | 29 | 7.1 | 7.5 | 8.3 | 9.3 | 10.3 | 11.4 | 12.0 | 16.4 | 17.3 | 18.8 | 20.6 | 22.5 | 24.4 | 25.6 |
| 30 | 23 | 8.2 | 8.6 | 9.5 | 10.6 | 11.7 | 12.8 | 13.4 | 19.0 | 20.0 | 21.7 | 23.6 | 25.8 | 27.8 | 29.2 |
| 31 | 24 | 9.3 | 9.8 | 10.8 | 11.9 | 13.2 | 14.4 | 15.1 | 21.8 | 22.9 | 24.8 | 27.0 | 29.3 | 31.5 | 33.1 |
| 32 | 37 | 10.5 | 11.1 | 12.2 | 13.5 | 14.8 | 16.1 | 16.9 | 24.9 | 26.2 | 28.2 | 30.6 | 33.2 | 35.7 | 37.5 |
| 33 | 31 | 11.9 | 12.5 | 13.7 | 15.1 | 16.6 | 18.0 | 18.9 | 28.3 | 29.8 | 32.0 | 34.7 | 37.5 | 40.2 | 42.2 |
| 34 | 23 | 13.4 | 14.1 | 15.4 | 16.9 | 18.5 | 20.1 | 21.1 | 32.0 | 33.7 | 36.2 | 39.1 | 42.2 | 45.1 | 47.4 |
| 35 | 26 | 15.0 | 15.8 | 17.2 | 18.9 | 20.6 | 22.3 | 23.4 | 36.2 | 38.1 | 40.8 | 44.0 | 47.3 | 50.5 | 53.0 |
| 36 | 24 | 16.8 | 17.7 | 19.2 | 21.0 | 22.9 | 24.7 | 25.9 | 40.7 | 42.8 | 45.8 | 49.2 | 52.9 | 56.3 | 59.1 |
| 37 | 26 | 18.7 | 19.7 | 21.3 | 23.3 | 25.3 | 27.3 | 28.7 | 45.6 | 48.0 | 51.2 | 55.0 | 58.9 | 62.7 | 65.8 |
| 38 | 17 | 20.8 | 21.9 | 23.7 | 25.7 | 28.0 | 30.1 | 31.6 | 50.9 | 53.6 | 57.1 | 61.2 | 65.5 | 69.5 | 73.0 |
| 39 | 7 | 23.1 | 24.3 | 26.2 | 28.4 | 30.8 | 33.1 | 34.8 | 56.7 | 59.7 | 63.5 | 67.9 | 72.6 | 76.9 | 80.7 |
| 40 | 6 | 25.5 | 26.8 | 28.9 | 31.3 | 33.8 | 36.3 | 38.1 | 63.0 | 66.3 | 70.4 | 75.2 | 80.2 | 84.9 | 89.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikenoue, S.; Akiba, Y.; Endo, T.; Kasuga, Y.; Yakubo, K.; Ishii, R.; Tanaka, M.; Ochiai, D. Defining the Normal Growth Curve of Fetal Fractional Limb Volume in a Japanese Population. J. Clin. Med. 2021, 10, 485. https://doi.org/10.3390/jcm10030485
Ikenoue S, Akiba Y, Endo T, Kasuga Y, Yakubo K, Ishii R, Tanaka M, Ochiai D. Defining the Normal Growth Curve of Fetal Fractional Limb Volume in a Japanese Population. Journal of Clinical Medicine. 2021; 10(3):485. https://doi.org/10.3390/jcm10030485
Chicago/Turabian StyleIkenoue, Satoru, Yohei Akiba, Toyohide Endo, Yoshifumi Kasuga, Kazumi Yakubo, Ryota Ishii, Mamoru Tanaka, and Daigo Ochiai. 2021. "Defining the Normal Growth Curve of Fetal Fractional Limb Volume in a Japanese Population" Journal of Clinical Medicine 10, no. 3: 485. https://doi.org/10.3390/jcm10030485
APA StyleIkenoue, S., Akiba, Y., Endo, T., Kasuga, Y., Yakubo, K., Ishii, R., Tanaka, M., & Ochiai, D. (2021). Defining the Normal Growth Curve of Fetal Fractional Limb Volume in a Japanese Population. Journal of Clinical Medicine, 10(3), 485. https://doi.org/10.3390/jcm10030485