
Endoglin Expression and Microvessel Density as Prognostic Factors in Pediatric Rhabdomyosarcoma


 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Analyzed Clinical Parameters
2.3. Immunohistochemistry
2.4. Microvessel Density Assessment
2.5. Statistical Analysis
3. Results
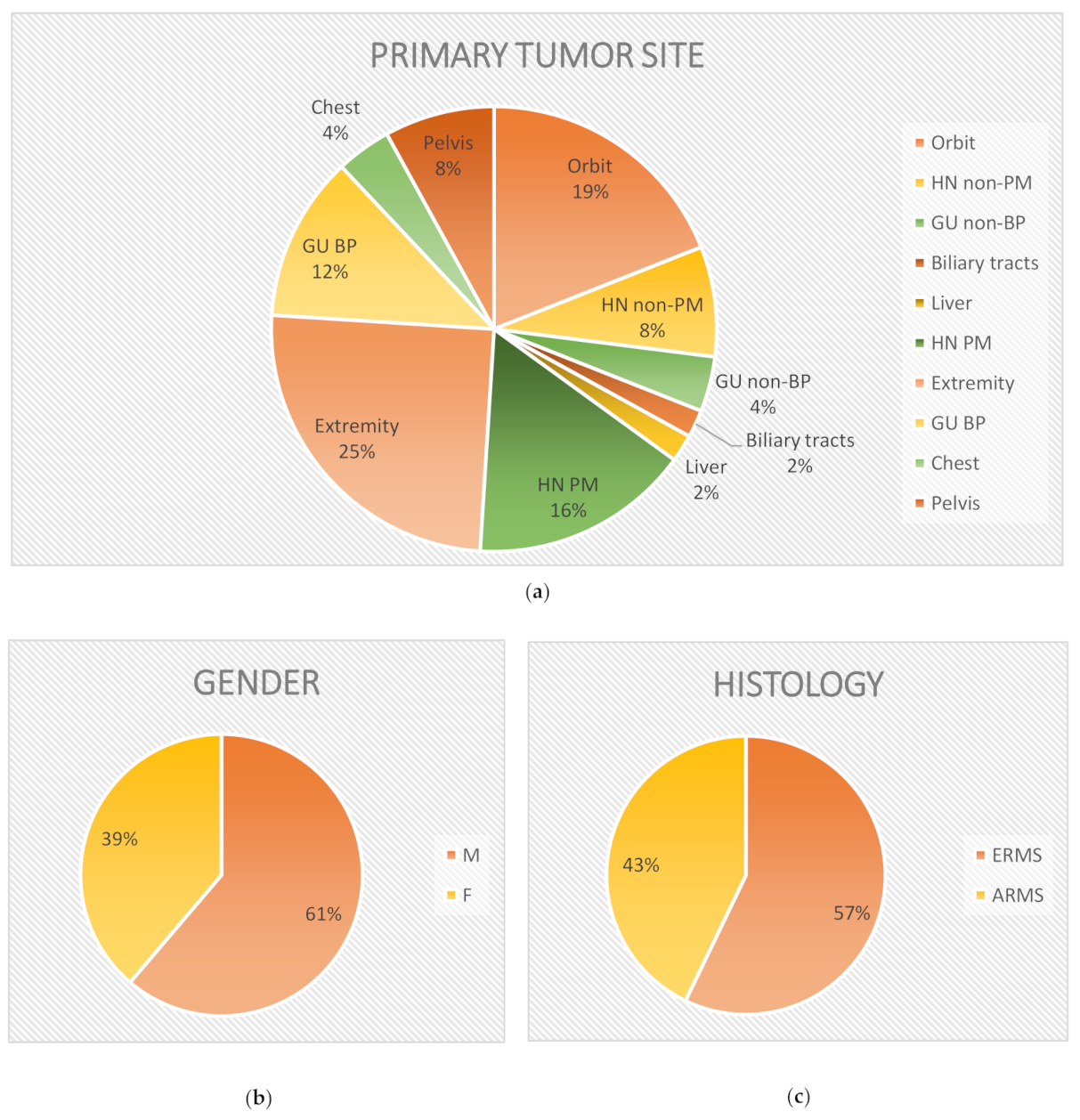
3.1. Study Population
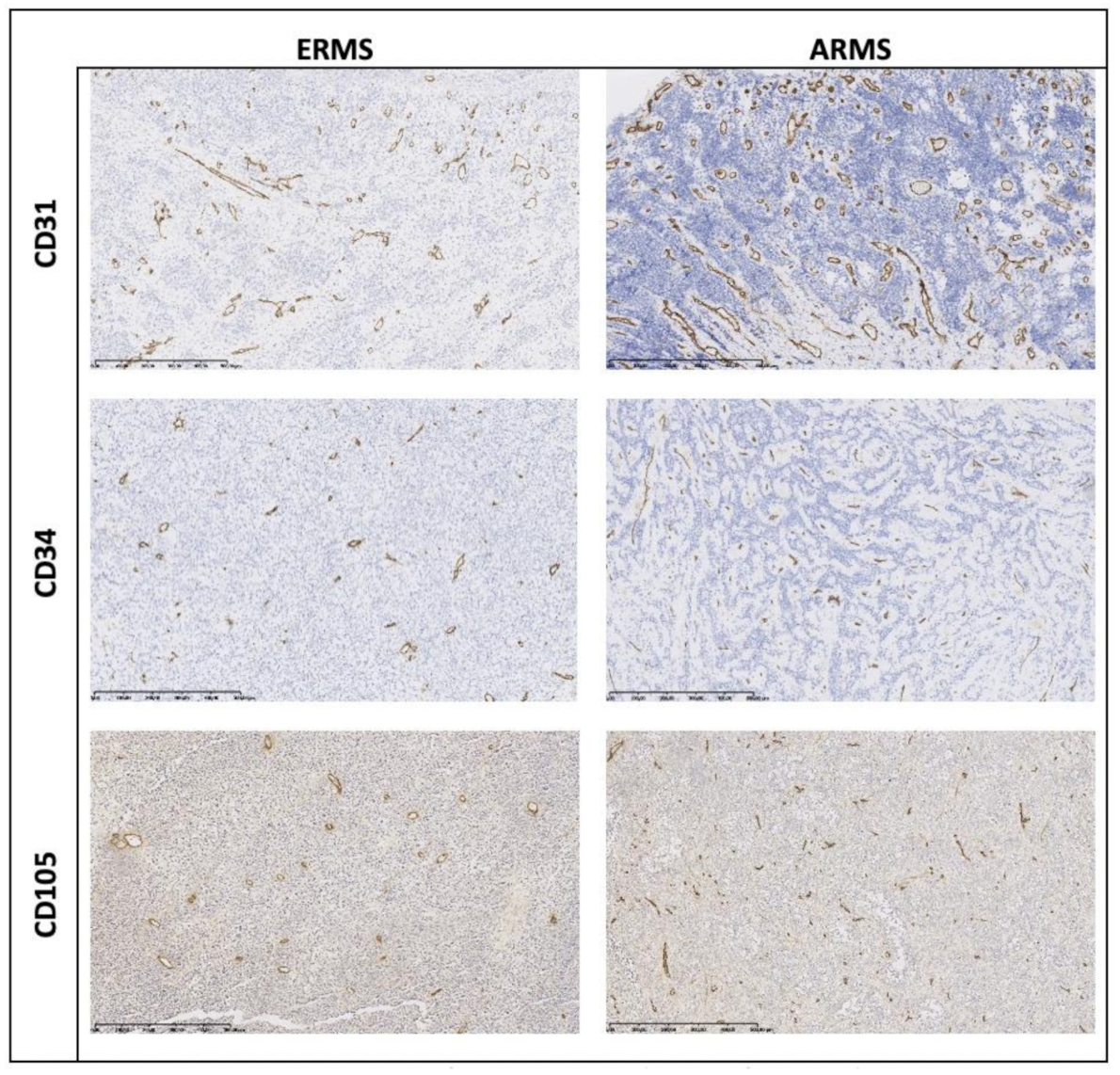
3.2. CD105, CD34, and CD 31 Expression
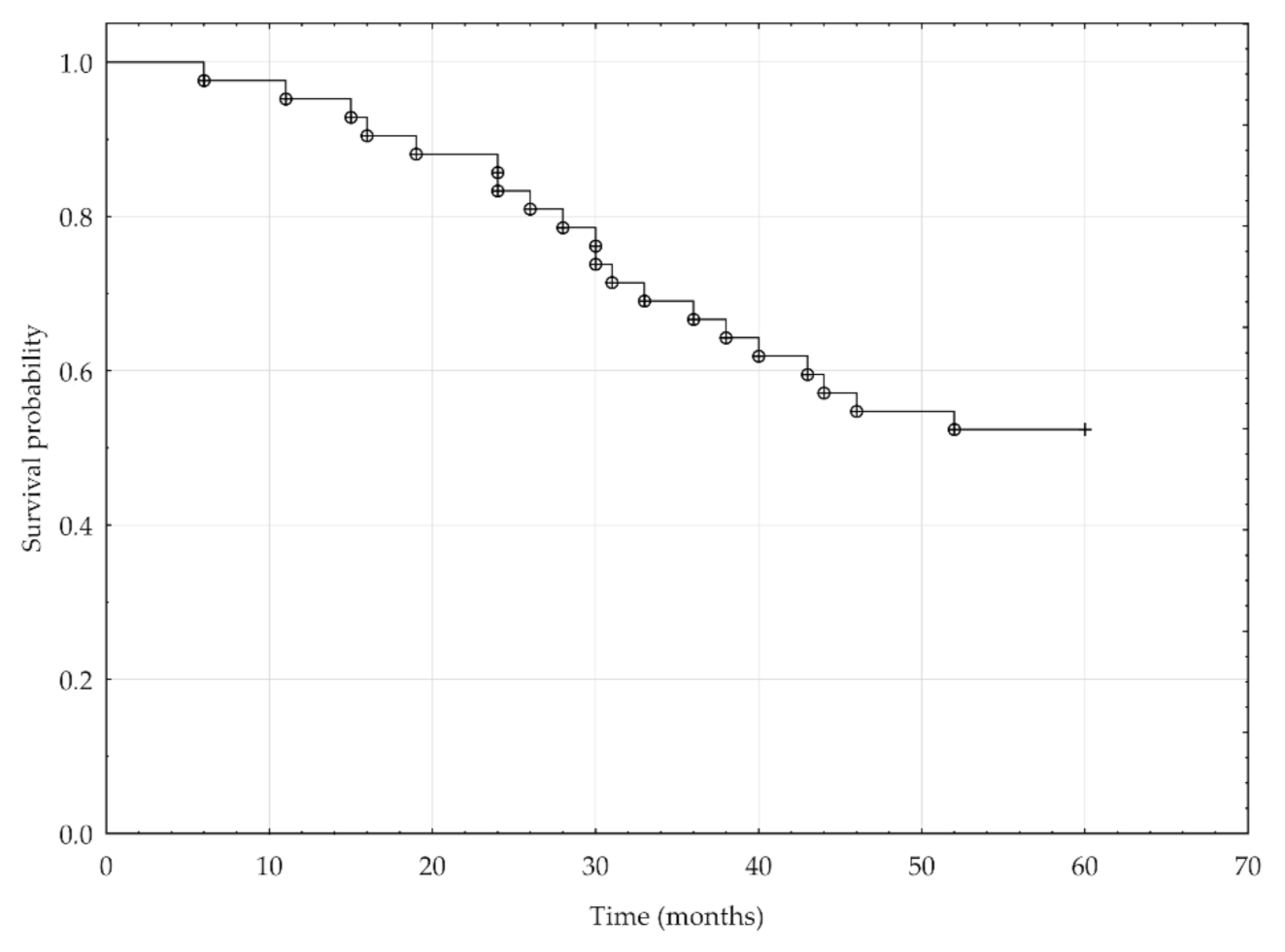
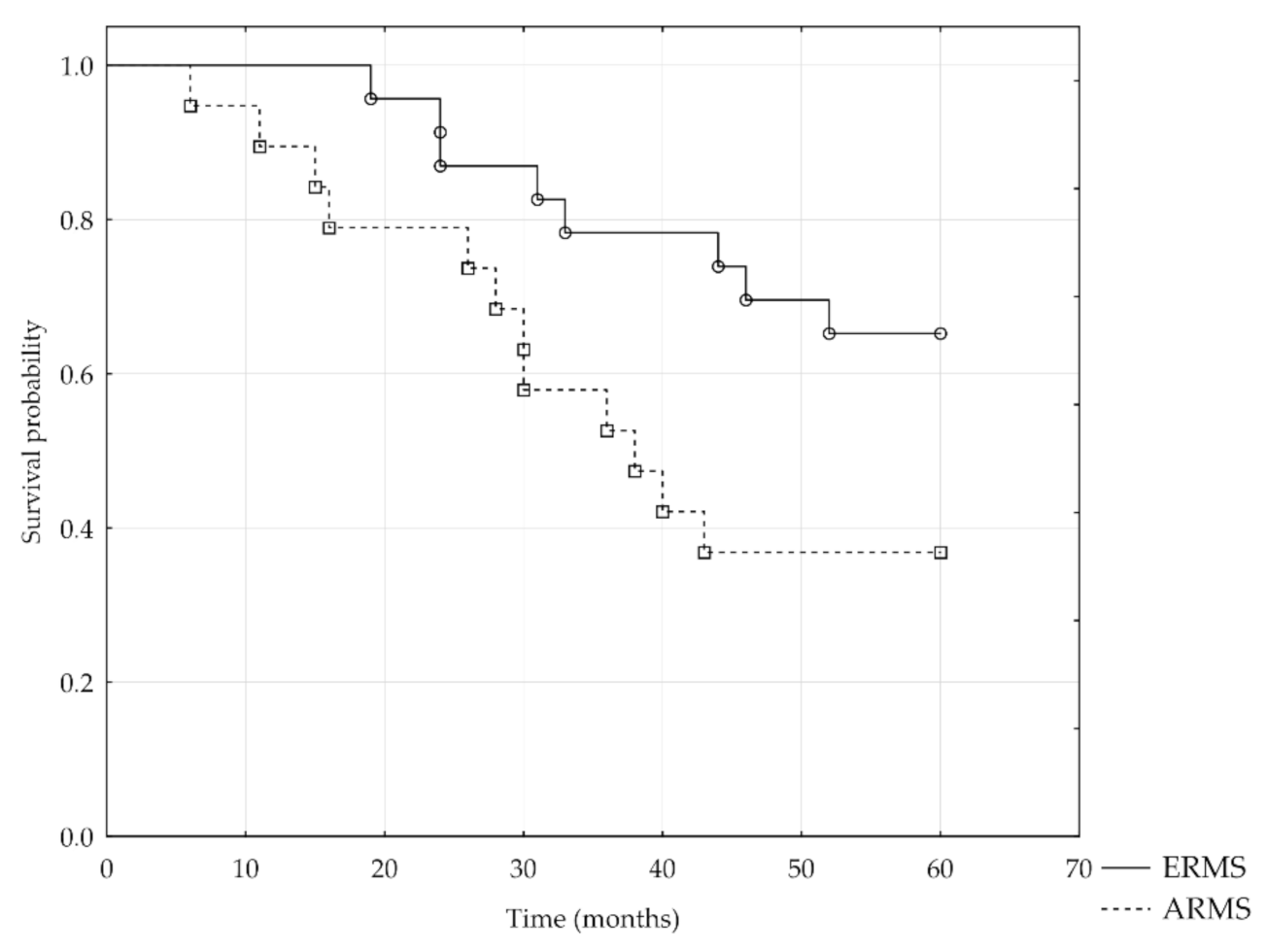
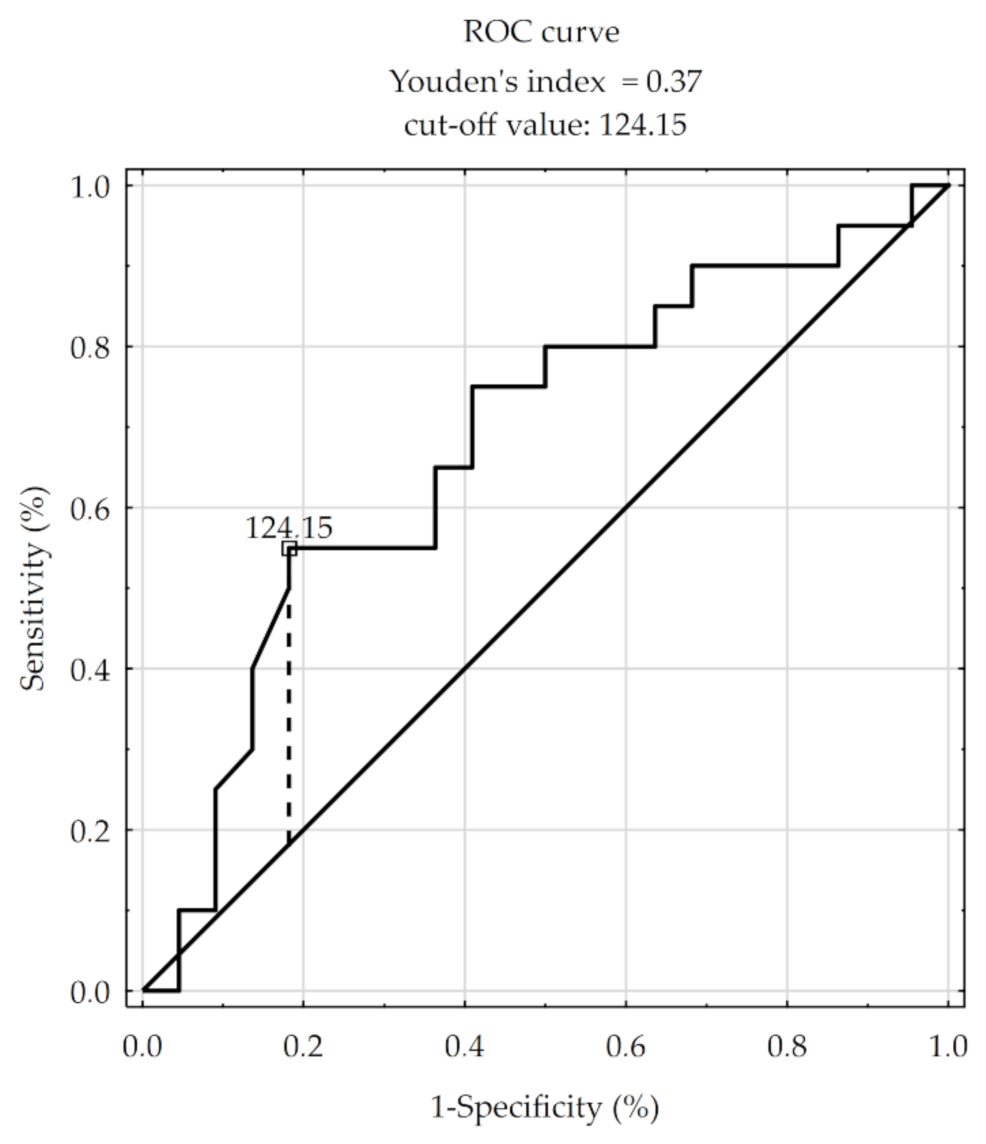
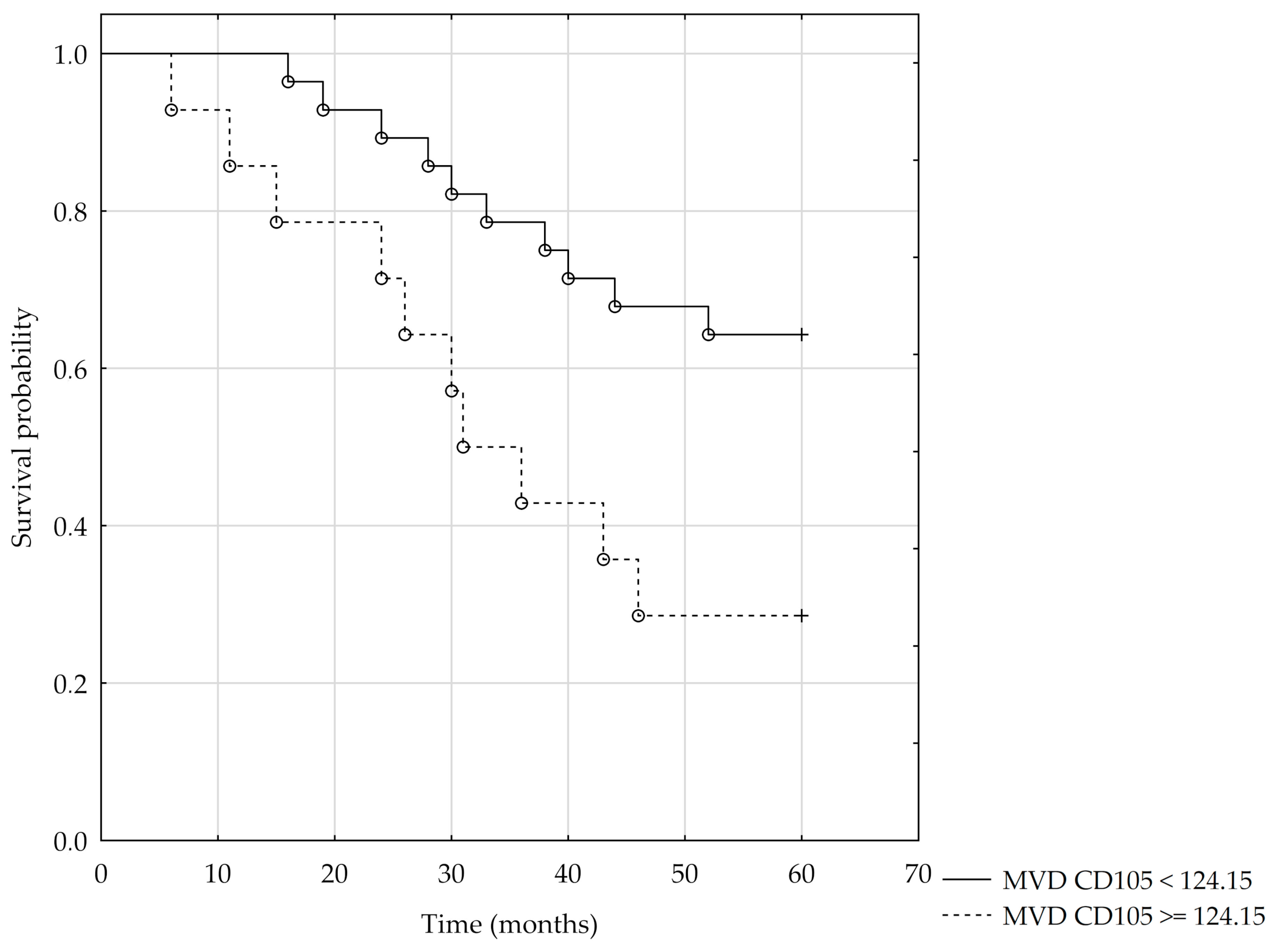
3.3. Clinical and Pathological Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, X.; Guo, W.; Shen, J.K.; Mankin, H.J.; Hornicek, F.J.; Duan, Z. Rhabdomyosarcoma: Advances in Molecular and Cellular Biology. Sarcoma 2015, 2015, 232010. [Google Scholar] [CrossRef] [PubMed]
- Linet, M.S.; Ries, L.A.G.; Smith, M.A.; Tarone, R.E.; Devesa, S.S. Cancer Surveillance Series: Recent Trends in Childhood Cancer Incidence and Mortality in the United States. J. Natl. Cancer Inst. 1999, 91, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Styczynski, J.; Balwierz, W.; Dembowska-Baginska, B.; Kazanowska, B.; Wachowiak, J.; Matysiak, M.; Klukowska, A.; Krawczuk-Rybak, M.; Adamkiewicz-Drozynska, E.; Młynarski, W.; et al. Paediatric oncology and haematology in Poland: Position paper. Pol. J. Paediatr. 2018, 93, 451–461. [Google Scholar] [CrossRef]
- Dasgupta, R.; Fuchs, J.; Rodeberg, D. Rhabdomyosarcoma. Semin Pediatr. Surg. 2016, 25, 276–283. [Google Scholar] [CrossRef]
- Tarnowski, M.; Grymula, K.; Tkacz, M.; Czerewaty, M.; Poniewierska-Baran, A.; Ratajczak, M.Z. Molecular mechanisms regulating metastasis of cancer cells with special emphasis on rhabdomyosarcoma. Postepy Hig. Med. Dosw. 2014, 68, 258–270. [Google Scholar] [CrossRef]
- Barr, F.G. Molecular genetics and pathogenesis of rhabdomyosarcoma. J. Pediatr. Hematol. Oncol. 1997, 19, 483–491. [Google Scholar] [CrossRef]
- Diller, L.; Sexsmith, E.; Gottlieb, A.; Li, F.P.; Malkin, D. Germline p53 mutations are frequently detected in young children with rhabdomyosarcoma. J. Clin. Investig. 1995, 95, 1606–1611. [Google Scholar] [CrossRef]
- Iolascon, A.; Faienza, M.F.; Coppola, B.; Rosolen, A.; Basso, G.; Della Ragione, F.; Schettini, F. Analysis of cyclin-dependent kinase inhibitor genes (CDKN2A, CDKN2B, and CDKN2C) in childhood rhabdomyosarcoma. Genes Chromosomes Cancer 1996, 15, 217–222. [Google Scholar] [CrossRef]
- Knudsen, E.S.; Pazzagli, C.; Born, T.L.; Bertolaet, B.L.; Knudsen, K.E.; Arden, K.C.; Henry, R.R.; Feramisco, J.R. Elevated cyclins and cyclin-dependent kinase activity in the rhabdomyosarcoma cell line RD. Cancer Res. 1998, 58, 2042–2049. [Google Scholar]
- Mauro, A.; Ciccarelli, C.; De Cesaris, P.; Scoglio, A.; Bouche, M.; Molinaro, M.; Aquino, A.; Zani, B.M. PKCalpha-mediated ERK, JNK and p38 activation regulates the myogenic program in human rhabdomyosarcoma cells. J. Cell Sci. 2002, 115, 3587–3599. [Google Scholar] [CrossRef]
- Marcinowska, A. Rhabdomyosaroma—Genetic changes in tumor pathogenesis. Nowotw. J. Oncol. 2003, 53, 286–292. [Google Scholar]
- Raney, R.B.; Anderson, J.R.; Barr, F.G.; Donaldson, S.S.; Pappo, A.S.; Qualman, S.J.; Wiener, E.S.; Maurer, H.M.; Crist, W.M. Rhabdomyosarcoma and undifferentiated sarcoma in the first two decades of life: A selective review of intergroup rhabdomyosarcoma study group experience and rationale for Intergroup Rhabdomyosarcoma Study V. J. Pediatr. Hematol. Oncol. 2001, 23, 215–220. [Google Scholar] [CrossRef]
- Di Paolo, V.; Russo, I.; Boldrini, R.; Rava, L.; Pezzullo, M.; Benedetti, M.C.; Galardi, A.; Colletti, M.; Rota, R.; Orlando, D.; et al. Evaluation of Endoglin (CD105) expression in pediatric rhabdomyosarcoma. BMC Cancer 2018, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Miyata, Y.; Sakai, H. Reconsideration of the clinical and histopathological significance of angiogenesis in prostate cancer: Usefulness and limitations of microvessel density measurement. Int. J. Urol. 2015, 22, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Rosen, L.S.; Gordon, M.S.; Robert, F.; Matei, D.E. Endoglin for targeted cancer treatment. Curr. Oncol. Rep. 2014, 16, 365. [Google Scholar] [CrossRef] [PubMed]
- Fonsatti, E.; Altomonte, M.; Nicotra, M.R.; Natali, P.G.; Maio, M. Endoglin (CD105): A powerful therapeutic target on tumor-associated angiogenetic blood vessels. Oncogene 2003, 22, 6557–6563. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Ghellal, A.; Li, C.; Byrne, G.; Haboubi, N.; Wang, J.M.; Bundred, N. Breast carcinoma: Vascular density determined using CD105 antibody correlates with tumor prognosis. Cancer Res. 1999, 59, 856–861. [Google Scholar]
- Tanaka, F.; Otake, Y.; Yanagihara, K.; Kawano, Y.; Miyahara, R.; Li, M.; Yamada, T.; Hanaoka, N.; Inui, K.; Wada, H. Evaluation of angiogenesis in non-small cell lung cancer: Comparison between anti-CD34 antibody and anti-CD105 antibody. Clin. Cancer Res. 2001, 7, 3410–3415. [Google Scholar]
- El-Gohary, Y.M.; Silverman, J.F.; Olson, P.R.; Liu, Y.L.; Cohen, J.K.; Miller, R.; Saad, R.S. Endoglin (CD105) and vascular endothelial growth factor as prognostic markers in prostatic adenocarcinoma. Am. J. Clin. Pathol. 2007, 127, 572–579. [Google Scholar] [CrossRef]
- Li, C.; Gardy, R.; Seon, B.K.; Duff, S.E.; Abdalla, S.; Renehan, A.; O’Dwyer, S.T.; Haboubi, N.; Kumar, S. Both high intratumoral microvessel density determined using CD105 antibody and elevated plasma levels of CD105 in colorectal cancer patients correlate with poor prognosis. Br. J. Cancer 2003, 88, 1424–1431. [Google Scholar] [CrossRef]
- Rubatt, J.M.; Darcy, K.M.; Hutson, A.; Bean, S.M.; Havrilesky, L.J.; Grace, L.A.; Berchuck, A.; Secord, A.A. Independent prognostic relevance of microvessel density in advanced epithelial ovarian cancer and associations between CD31, CD105, p53 status, and angiogenic marker expression: A Gynecologic Oncology Group study. Gynecol. Oncol. 2009, 112, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Li, C.; Lin, S.; Yang, Y.; Liu, D.; Han, Y.; Zhang, Y.; Li, L.; Zhou, L.; Kumar, S. Comparative evaluation of microvessel density determined by CD34 or CD105 in benign and malignant gastric lesions. Hum. Pathol. 2006, 37, 861–866. [Google Scholar] [CrossRef]
- Yang, L.Y.; Lu, W.Q.; Huang, G.W.; Wang, W. Correlation between CD105 expression and postoperative recurrence and metastasis of hepatocellular carcinoma. BMC Cancer 2006, 6, 110. [Google Scholar] [CrossRef] [PubMed]
- Saad, R.S.; El-Gohary, Y.; Memari, E.; Liu, Y.L.; Silverman, J.F. Endoglin (CD105) and vascular endothelial growth factor as prognostic markers in esophageal adenocarcinoma. Hum. Pathol. 2005, 36, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Kyzas, P.A.; Agnantis, N.J.; Stefanou, D. Endoglin (CD105) as a prognostic factor in head and neck squamous cell carcinoma. Virchows Arch. 2006, 448, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Dubinski, W.; Gabril, M.; Iakovlev, V.V.; Scorilas, A.; Youssef, Y.M.; Faragalla, H.; Kovacs, K.; Rotondo, F.; Metias, S.; Arsanious, A.; et al. Assessment of the prognostic significance of endoglin (CD105) in clear cell renal cell carcinoma using automated image analysis. Hum. Pathol. 2012, 43, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Attia, S.; Sankhala, K.K.; Riedel, R.F.; Robinson, S.I.; Conry, R.M.; Boland, P.M.; Barve, M.A.; Fritchie, K.; Seon, B.K.; Alvarez, D.; et al. A phase 1B/phase 2A study of TRC105 (Endoglin Antibody) in combination with pazopanib (P) in patients (pts) with advanced soft tissue sarcoma (STS). J. Clin. Oncol. 2016, 34, 11016. [Google Scholar] [CrossRef]
- Puerto-Camacho, P.; Amaral, A.T.; Lamhamedi-Cherradi, S.-E.; Menegaz, B.A.; Castillo-Ecija, H.; Ordóñez, J.L.; Domínguez, S.; Jordan-Perez, C.; Diaz-Martin, J.; Romero-Pérez, L.; et al. Preclinical Efficacy of Endoglin-Targeting Antibody–Drug Conjugates for the Treatment of Ewing Sarcoma. Clin. Cancer Res. 2019, 25, 2228–2240. [Google Scholar] [CrossRef]
- Fritchie, K.; Attia, S.; Okuno, S.; Arndt, C.; Robinson, S. Abstract B237: CD105: A therapeutic target for sarcomas. Mol. Cancer Ther. 2013, 12, B237. [Google Scholar] [CrossRef]
- Lawrence, W., Jr.; Anderson, J.R.; Gehan, E.A.; Maurer, H. Pretreatment TNM staging of childhood rhabdomyosarcoma: A report of the Intergroup Rhabdomyosarcoma Study Group. Children’s Cancer Study Group. Pediatric Oncology Group. Cancer 1997, 80, 1165–1170. [Google Scholar] [CrossRef]
- Weidner, N.; Semple, J.P.; Welch, W.R.; Folkman, J. Tumor angiogenesis and metastasis--correlation in invasive breast carcinoma. N. Engl. J. Med. 1991, 324, 1–8. [Google Scholar] [CrossRef]
- Rocchi, L.; Caraffi, S.; Perris, R.; Mangieri, D. The angiogenic asset of soft tissue sarcomas: A new tool to discover new therapeutic targets. Biosci. Rep. 2014, 34, e00147. [Google Scholar] [CrossRef] [PubMed]
- Miyata, Y.; Mitsunari, K.; Asai, A.; Takehara, K.; Mochizuki, Y.; Sakai, H. Pathological significance and prognostic role of microvessel density, evaluated using CD31, CD34, and CD105 in prostate cancer patients after radical prostatectomy with neoadjuvant therapy. Prostate 2015, 75, 84–91. [Google Scholar] [CrossRef]
- Cheng, S.H.; Liu, J.M.; Liu, Q.Y.; Luo, D.Y.; Liao, B.H.; Li, H.; Wang, K.J. Prognostic role of microvessel density in patients with renal cell carcinoma: A meta-analysis. Int. J. Clin. Exp. Pathol. 2014, 7, 5855–5863. [Google Scholar] [PubMed]
- Ma, G.; Zhang, J.; Jiang, H.; Zhang, N.; Zhu, Y.; Deng, Y.; Zhou, Q. Microvessel density as a prognostic factor in esophageal squamous cell cancer patients: A meta-analysis. Medicine (Baltimore) 2017, 96, e7600. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, J.; Barsky, S.H.; Nelson, S.; Singer, S.; Pezeshki, B.; Lee, M.C.; Eilber, F.; Nguyen, M. Different patterns of angiogenesis in sarcomas and carcinomas. Clin. Cancer Res. 1999, 5, 3516–3522. [Google Scholar] [PubMed]
- West, C.C.; Brown, N.J.; Mangham, D.C.; Grimer, R.J.; Reed, M.W. Microvessel density does not predict outcome in high grade soft tissue sarcoma. Eur. J. Surg. Oncol. 2005, 31, 1198–1205. [Google Scholar] [CrossRef]
- Pavlakovic, H.; Von Schutz, V.; Rossler, J.; Koscielniak, E.; Havers, W.; Schweigerer, L. Quantification of angiogenesis stimulators in children with solid malignancies. Int. J. Cancer 2001, 92, 756–760. [Google Scholar] [CrossRef]
- Yudoh, K.; Kanamori, M.; Ohmori, K.; Yasuda, T.; Aoki, M.; Kimura, T. Concentration of vascular endothelial growth factor in the tumour tissue as a prognostic factor of soft tissue sarcomas. Br. J. Cancer 2001, 84, 1610–1615. [Google Scholar] [CrossRef]
- Kreuter, M.; Bieker, R.; Bielack, S.S.; Auras, T.; Buerger, H.; Gosheger, G.; Jurgens, H.; Berdel, W.E.; Mesters, R.M. Prognostic relevance of increased angiogenesis in osteosarcoma. Clin. Cancer Res. 2004, 10, 8531–8537. [Google Scholar] [CrossRef]
- Kubo, T.; Shimose, S.; Fujimori, J.; Arihiro, K.; Ochi, M. Diversity of angiogenesis among malignant bone tumors. Mol. Clin. Oncol. 2013, 1, 131–136. [Google Scholar] [CrossRef]
- Mantadakis, E.; Kim, G.; Reisch, J.; McHard, K.; Maale, G.; Leavey, P.J.; Timmons, C. Lack of prognostic significance of intratumoral angiogenesis in nonmetastatic osteosarcoma. J. Pediatr. Hematol. Oncol. 2001, 23, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Saenz, N.C.; Heslin, M.J.; Adsay, V.; Lewis, J.J.; Leung, D.H.; LaQuaglia, M.P.; Brennan, M.F. Neovascularity and clinical outcome in high-grade extremity soft tissue sarcomas. Ann. Surg. Oncol. 1998, 5, 48–53. [Google Scholar] [CrossRef]
- Mikulic, D.; Ilic, I.; Cepulic, M.; Orlic, D.; Giljevic, J.S.; Fattorini, I.; Seiwerth, S. Tumor angiogenesis and outcome in osteosarcoma. Pediatr. Hematol. Oncol. 2004, 21, 611–619. [Google Scholar] [CrossRef]
- Ohsawa, M.; Tomita, Y.; Kuratsu, S.; Kanno, H.; Aozasa, K. Angiogenesis in malignant fibrous histiocytoma. Oncology 1995, 52, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Basilio-de-Oliveira, R.P.; Pannain, V.L. Prognostic angiogenic markers (endoglin, VEGF, CD31) and tumor cell proliferation (Ki67) for gastrointestinal stromal tumors. World J. Gastroenterol. 2015, 21, 6924–6930. [Google Scholar] [CrossRef] [PubMed]
- Ollauri-Ibanez, C.; Lopez-Novoa, J.M.; Pericacho, M. Endoglin-based biological therapy in the treatment of angiogenesis-dependent pathologies. Expert Opin. Biol. Ther. 2017, 17, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Nico, B.; Benagiano, V.; Mangieri, D.; Maruotti, N.; Vacca, A.; Ribatti, D. Evaluation of microvascular density in tumors: Pro and contra. Histol. Histopathol. 2008, 23, 601–607. [Google Scholar] [CrossRef]
- Gordon, M.S.; Robert, F.; Matei, D.; Mendelson, D.S.; Goldman, J.W.; Chiorean, E.G.; Strother, R.M.; Seon, B.K.; Figg, W.D.; Peer, C.J.; et al. An open-label phase Ib dose-escalation study of TRC105 (anti-endoglin antibody) with bevacizumab in patients with advanced cancer. Clin. Cancer Res. 2014, 20, 5918–5926. [Google Scholar] [CrossRef]
- Attia, S.; Okuno, S.H.; Robinson, S.I.; Webber, N.P.; Indelicato, D.J.; Jones, R.L.; Bagaria, S.P.; Jones, R.L.; Sherman, C.; Kozak, K.R.; et al. Clinical Activity of Pazopanib in Metastatic Extraosseous Ewing Sarcoma. Rare Tumors 2015, 7, 5992. [Google Scholar] [CrossRef]
- Newman, P.J. The biology of PECAM-1. J. Clin. Investig. 1997, 100, S25–S29. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, O.; Rey, A.; Lyden, E.; Bisogno, G.; Stevens, M.C.; Meyer, W.H.; Carli, M.; Anderson, J.R. Prognostic factors in metastatic rhabdomyosarcomas: Results of a pooled analysis from United States and European cooperative groups. J. Clin. Oncol. 2008, 26, 2384–2389. [Google Scholar] [CrossRef] [PubMed]
- Hasan, J.; Byers, R.; Jayson, G.C. Intra-tumoural microvessel density in human solid tumours. Br. J. Cancer 2002, 86, 1566–1577. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pt | Age (Years) | Gender | Histology | Primary Site | Primary Size (cm) | T | N | M | TNM Stage | Follow Up | MVD CD31 | MVD CD34 | MVD CD105 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | DOD | 56.1 | 88.4 | 40.8 |
| 2 | 1 mos | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | ALV | 156.5 | 156.5 | 90.1 |
| 3 | 3 | M | ERMS | Favorable | ≤5 | 2 | 0 | 0 | 1 | TSF | 137.8 | 44.2 | 22.1 |
| 4 | 6 mos | F | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | TSF | 236.4 | 340.1 | 96.9 |
| 5 | 9 mos | M | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | DOD | 335.0 | 190.5 | 136.1 |
| 6 | 4 | F | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | DOD | 363.9 | 362.2 | 124.1 |
| 7 | 12 | F | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | DOD | 161.6 | 197.3 | 95.2 |
| 8 | 4 | F | ERMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | DOD | 137.8 | 250.0 | 127.6 |
| 9 | 11 | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | ALV | 136.1 | 154.8 | 56.1 |
| 10 | 3 mos | F | ARMS | Favorable | ≤5 | 2 | 0 | 0 | 1 | DOD | 173.5 | 73.1 | 125.9 |
| 11 | 9 | M | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 83.3 | 113.9 | 76.5 |
| 12 | 4 | F | ERMS | Favorable | ≤5 | 2 | 0 | 0 | 1 | ALV | 132.7 | 176.9 | 115.6 |
| 13 | 3 | M | ERMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | DOD | 236.4 | 85.0 | 112.2 |
| 14 | 17 | M | ARMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | DOD | 309.5 | 199.0 | 176.9 |
| 15 | 7 | M | ERMS | Unfavorable | >5 | 2 | 1 | 0 | 3 | DOD | 124.1 | 202.4 | 81.6 |
| 16 | 16 | F | ARMS | Favorable | >5 | 2 | 0 | 1 | 4 | DOD | 462.6 | 188.8 | 200.7 |
| 17 | 5 | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | TSF | 91.8 | 107.1 | 73.1 |
| 18 | 4 | M | ERMS | Unfavorable | >5 | 2 | 1 | 0 | 3 | ALV | 15.3 | 20.4 | 15.3 |
| 19 | 4 | F | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | ALV | 129.3 | 107.1 | 120.7 |
| 20 | 8 | F | ARMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | DOD | 127.6 | 142.9 | 74.8 |
| 21 | 6 | F | ERMS | Favorable | >5 | 2 | 1 | 0 | 1 | TSF | 219.4 | 204.1 | 91.8 |
| 22 | 3 | F | ERMS | Unfavorable | >5 | 1 | 0 | 0 | 3 | ALV | 54.4 | 88.4 | 37.4 |
| 23 | 19 mos | M | ERMS | Unfavorable | ≤5 | 2 | 0 | 0 | 2 | ALV | 124.1 | 120.7 | 68.0 |
| 24 | 2 | F | ARMS | Unfavorable | ≤5 | 1 | 0 | 0 | 2 | ALV | 142.9 | 176.9 | 115.6 |
| 25 | 15 | M | ERMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | DOD | 90.1 | 209.2 | 34.0 |
| 26 | 15 mos | M | ARMS | Unfavorable | >5 | 2 | 1 | 1 | 4 | ALV | 100.3 | 79.9 | 39.1 |
| 27 | 2 | M | ARMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 127.6 | 243.2 | 76.5 |
| 28 | 21 mos | M | ERMS | Favorable | >5 | 2 | 1 | 0 | 1 | DOD | 161.6 | 171.8 | 125.9 |
| 29 | 15 | F | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | ALV | 132.7 | 338.4 | 153.1 |
| 30 | 9 | M | ARMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | TSF | 318.0 | 88.4 | 122.4 |
| 31 | 3 | F | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 125.9 | 102.0 | 83.3 |
| 32 | 2 | M | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | ALV | 219.4 | 363.9 | 54.4 |
| 33 | 2 | M | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | AVL | 91.8 | 56.1 | 47.6 |
| 34 | 8 | M | ERMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | DOD | 363.9 | 511.9 | 233.0 |
| 35 | 2 | M | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 136.1 | 136.1 | 76.5 |
| 36 | 11 | F | ERMS | Unfavorable | >5 | 1 | 0 | 1 | 4 | TSF | 227.9 | 227.9 | 188.8 |
| 37 | 3 | M | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 71.4 | 112.2 | 62.9 |
| 38 | 5 | M | ARMS | Unfavorable | ≤5 | 1 | 0 | 1 | 4 | DOD | 353.7 | 295.9 | 277.2 |
| 39 | 14 mos | M | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | DOD | 212.6 | 216.0 | 229.6 |
| 40 | 5 | F | ERMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | ALV | 205.8 | 144.6 | 107.1 |
| 41 | 3 | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | ALV | 227.9 | 263.6 | 117.3 |
| 42 | 15 | F | ARMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | DOD | 93.5 | 132.7 | 66.3 |
| 43 | 7 | M | ARMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | ALV | 120.7 | 170.1 | 125.9 |
| 44 | 2 | M | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | DOD | 622.4 | 1052.7 | 294.2 |
| 45 | 15 | M | ARMS | Unfavorable | >5 | 2 | 0 | 1 | 4 | DOD | 216.0 | 251.7 | 159.9 |
| 46 | 5 | M | ERMS | Favorable | ≤5 | 1 | 0 | 0 | 1 | TSF | 227.9 | 168.4 | 108.8 |
| 47 | 8 | F | ARMS | Unfavorable | >5 | 1 | 0 | 0 | 3 | DOD | 214.3 | 110.5 | 100.3 |
| 48 | 5 | M | ERMS | Favorable | >5 | 2 | 0 | 1 | 4 | DOD | 120.7 | 127.6 | 108.8 |
| 49 | 13 | F | ARMS | Unfavorable | >5 | 2 | 0 | 0 | 3 | DOD | 142.9 | 159.9 | 153.1 |
| Pt | Age (Years) | Gender | Surgical Procedure |
|---|---|---|---|
| 1 | 11 | F | Tonsillectomy |
| 2 | 11 | F | Tonsillectomy |
| 3 | 18 mos | F | TGDC excision |
| 4 | 6 | F | TGDC excision |
| 5 | 5 | M | TGDC excision |
| 6 | 8 | M | TGDC excision |
| 7 | 15 | M | TGDC excision |
| 8 | 15 | F | Tonsillectomy |
| 9 | 15 | F | Tonsillectomy |
| 10 | 6 | M | Tonsillectomy |
| 11 | 15 | F | Tonsillectomy |
| 12 | 17 | F | Tonsillectomy |
| 13 | 17 | F | Tonsillectomy |
| 14 | 13 | F | Tonsillectomy |
| 15 | 17 | F | Tonsillectomy |
| 16 | 8 | M | Tonsillectomy |
| 17 | 15 | M | Tonsillectomy |
| 18 | 15 | F | Tonsillectomy |
| Variables | Study Group | Control Group | Mann-Whitney U Test (Z) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Mean | SD | Median | |||
| MVD/CD31 | 185.17 | 112.69 | 142.86 | 352.04 | 186.40 | 322.28 | −3.68 | p < 0.001 |
| MVD/CD34 | 194.40 | 156.83 | 168.37 | 711.73 | 205.48 | 770.41 | −5.83 | p < 0.001 |
| MVD/CD105 | 110.65 | 61.36 | 107.14 | 74.07 | 107.52 | 9.35 | 2.75 | p = 0.006 |
| Cox Regression Analysis—5 Years. Model Chi-Square = 22.25, p = 0.0002 | ||||
|---|---|---|---|---|
| Parameter | Parameter Estimate | Chi-Square | p-Value | Hazard Ratio (HR) |
| Age < 1 | 2.07 | 5.75 | 0.016 | 7.97 |
| Age ≥ 10 | 1.82 | 11.07 | 0.001 | 6.22 |
| N1 | 2.44 | 13.65 | 0.0002 | 11.51 |
| MVD/CD105 | 0.01 | 6.19 | 0.013 | 1.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radzikowska, J.; Krzeski, A.; Czarnecka, A.M.; Klepacka, T.; Rychlowska-Pruszynska, M.; Raciborska, A.; Dembowska-Baginska, B.; Pronicki, M.; Kukwa, A.; Sierdzinski, J.; et al. Endoglin Expression and Microvessel Density as Prognostic Factors in Pediatric Rhabdomyosarcoma. J. Clin. Med. 2021, 10, 512. https://doi.org/10.3390/jcm10030512
Radzikowska J, Krzeski A, Czarnecka AM, Klepacka T, Rychlowska-Pruszynska M, Raciborska A, Dembowska-Baginska B, Pronicki M, Kukwa A, Sierdzinski J, et al. Endoglin Expression and Microvessel Density as Prognostic Factors in Pediatric Rhabdomyosarcoma. Journal of Clinical Medicine. 2021; 10(3):512. https://doi.org/10.3390/jcm10030512
Chicago/Turabian StyleRadzikowska, Joanna, Antoni Krzeski, Anna M. Czarnecka, Teresa Klepacka, Magdalena Rychlowska-Pruszynska, Anna Raciborska, Bozenna Dembowska-Baginska, Maciej Pronicki, Andrzej Kukwa, Janusz Sierdzinski, and et al. 2021. "Endoglin Expression and Microvessel Density as Prognostic Factors in Pediatric Rhabdomyosarcoma" Journal of Clinical Medicine 10, no. 3: 512. https://doi.org/10.3390/jcm10030512
APA StyleRadzikowska, J., Krzeski, A., Czarnecka, A. M., Klepacka, T., Rychlowska-Pruszynska, M., Raciborska, A., Dembowska-Baginska, B., Pronicki, M., Kukwa, A., Sierdzinski, J., & Kukwa, W. (2021). Endoglin Expression and Microvessel Density as Prognostic Factors in Pediatric Rhabdomyosarcoma. Journal of Clinical Medicine, 10(3), 512. https://doi.org/10.3390/jcm10030512