4. Discussion
To the best of our knowledge, our study is the largest to evaluate the impact of prolonged fluoroscopy time on procedural outcomes in both CTO and non-CTO PCI. Our major findings are as follows: (1) Prolonged fluoroscopy time is strongly associated with procedural failure. (2) The relation between fluoroscopy time and procedural failure differs significantly between non-CTO and CTO PCI, with a shift towards longer fluoroscopy times in CTO–PCI. (3) In non-CTO PCI, the decrease in procedural success with increasing fluoroscopy time is largely driven by MACCE, whereas with CTO PCI, it is driven by technical failure.
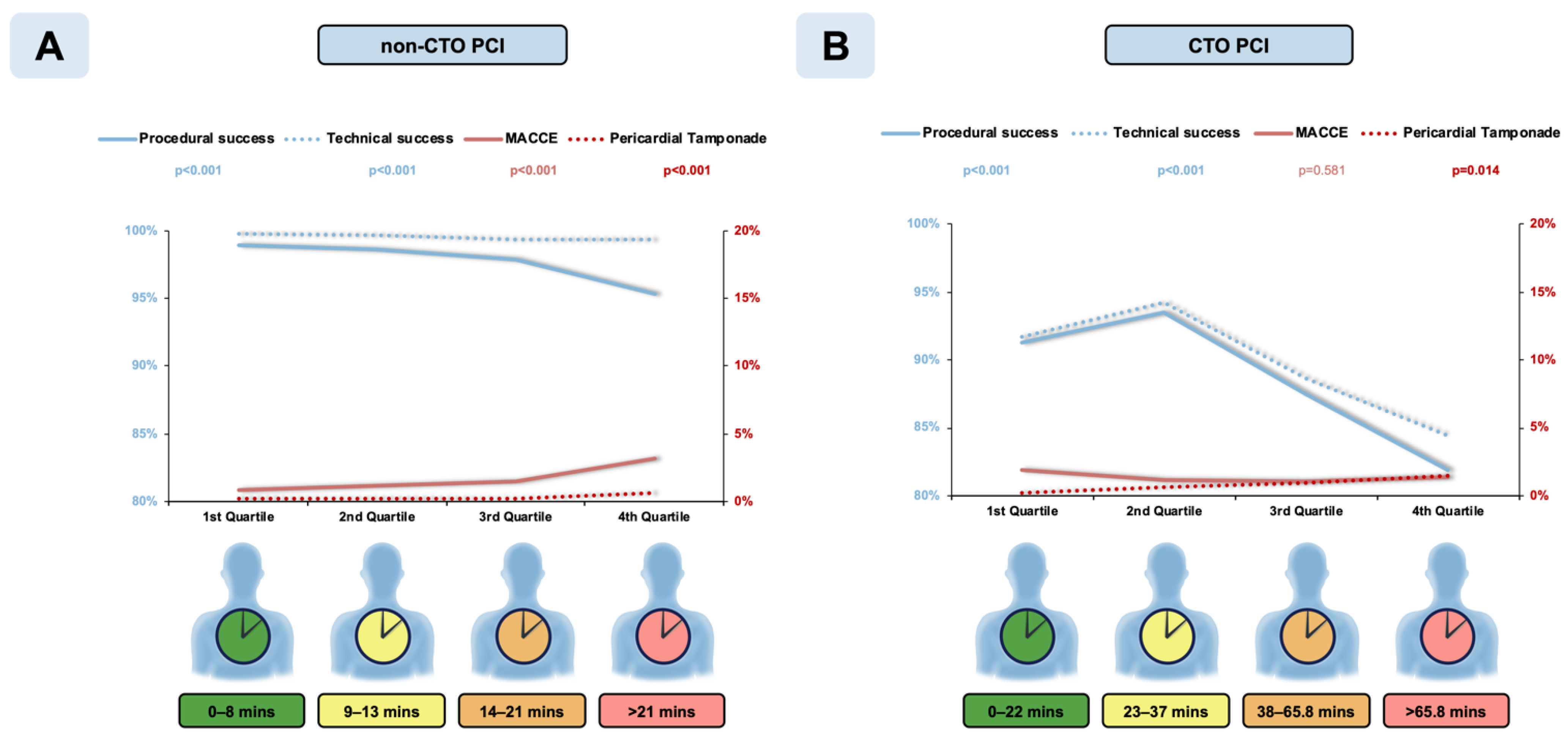
The procedural success significantly decreased with increasing fluoroscopy time in both CTO and non-CTO PCI. However, the optimal cut-off time for prediction of procedural failure in CTO PCI was about twice that in CTO PCI. Even an uncomplicated CTO PCI is inherently more time consuming than a non-CTO PCI, whereas in non-CTO PCI, prolongation of the procedure may be caused by the number of lesions treated or intraprocedural problems.
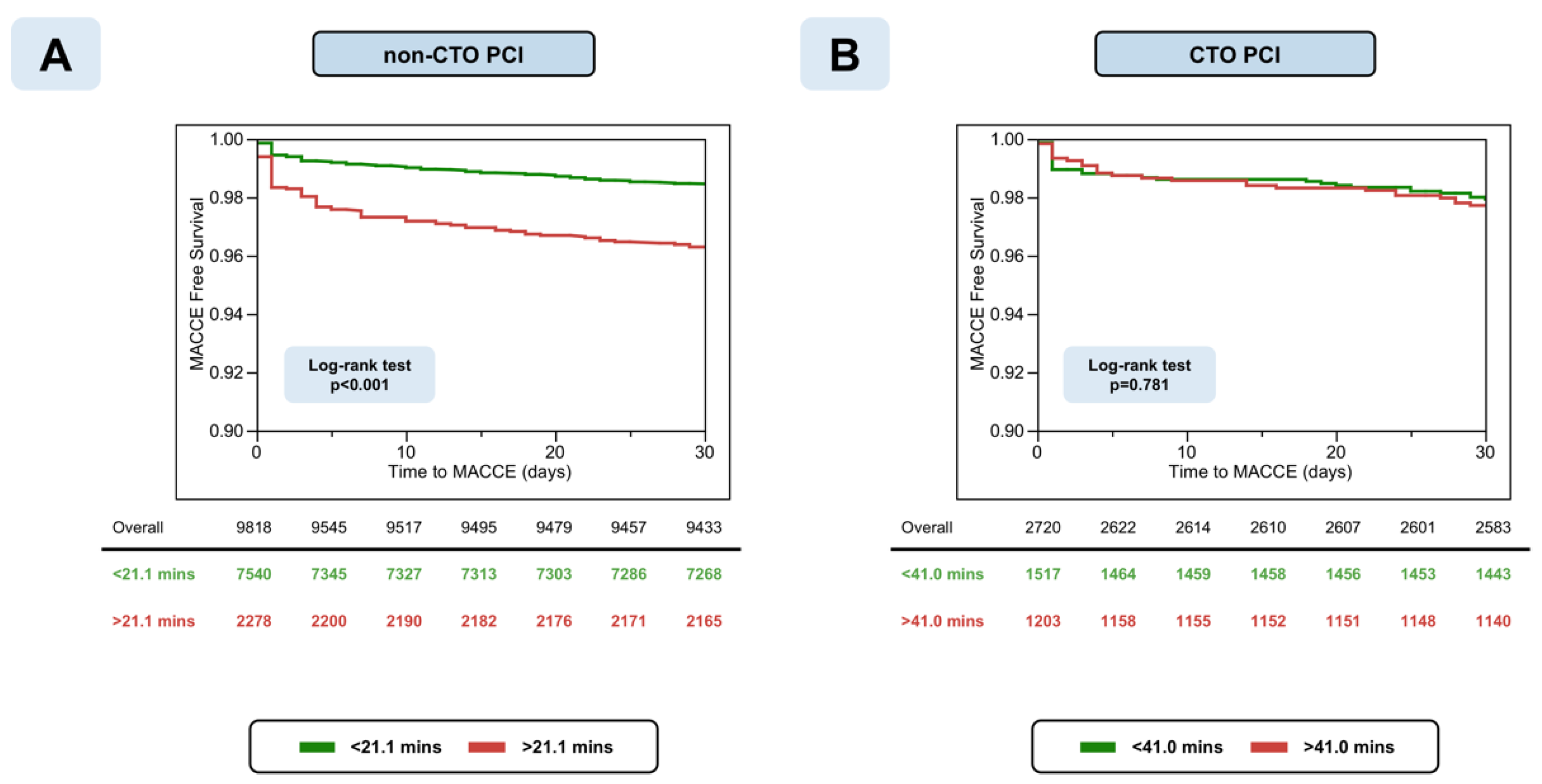
The mechanism of procedural failure differed substantially between the two types of PCI. Although the chance of technical failure increased significantly with fluoroscopy time in both modalities, the increment was small with non-CTO PCI—0.4% between first and fourth quartile of fluoroscopy time—but substantially larger with CTO PCI—7.3% between first and fourth quartile of fluoroscopy time. Likewise, the statistically significant increment in the risk of perforation with tamponade with fluoroscopy time was larger with CTO PCI than with non-CTO PCI (1.47% versus 0.49% for the difference between first and fourth quartile of fluoroscopy time). On the other side, the increase in procedural failure with FT in non-CTO PCI was driven by a significant increase in MACCE (2.37% increase between first and fourth quartile) that was not found in CTO PCI. The difference in MACCE depending on fluoroscopy time in the non-CTO group prevailed during 30-day follow-up, whereas in the CTO group, 30-day survival without MACCE was similar irrespective of procedure prolongation. Thus, in CTO PCI, the risk of MACCE was low and largely independent of fluoroscopy time. Possible explanations for this include the following: (a) a presumably higher level of tolerance for transient ischemia in patients undergoing PCI with a well-developed collateral system, (b) the predominant restriction of the procedure to one lesion, (c) a lower clinical impact of technical failure or early reocclusion, and (d) CTO operators’ advanced skillset for hindering procedure-related complications. Additionally, bleeding complications significantly increase in both longer CTO and non-CTO PCI. This may be caused by the cumulated dosage of unfractionated heparin, which is critical to maintain an appropriate activated clotting time (ACT). Other potential explanations include a higher rate of femoral access, larger sheath size, and potential blood loss via the Y-connectors caused by more frequent device exchange in lengthened PCI.
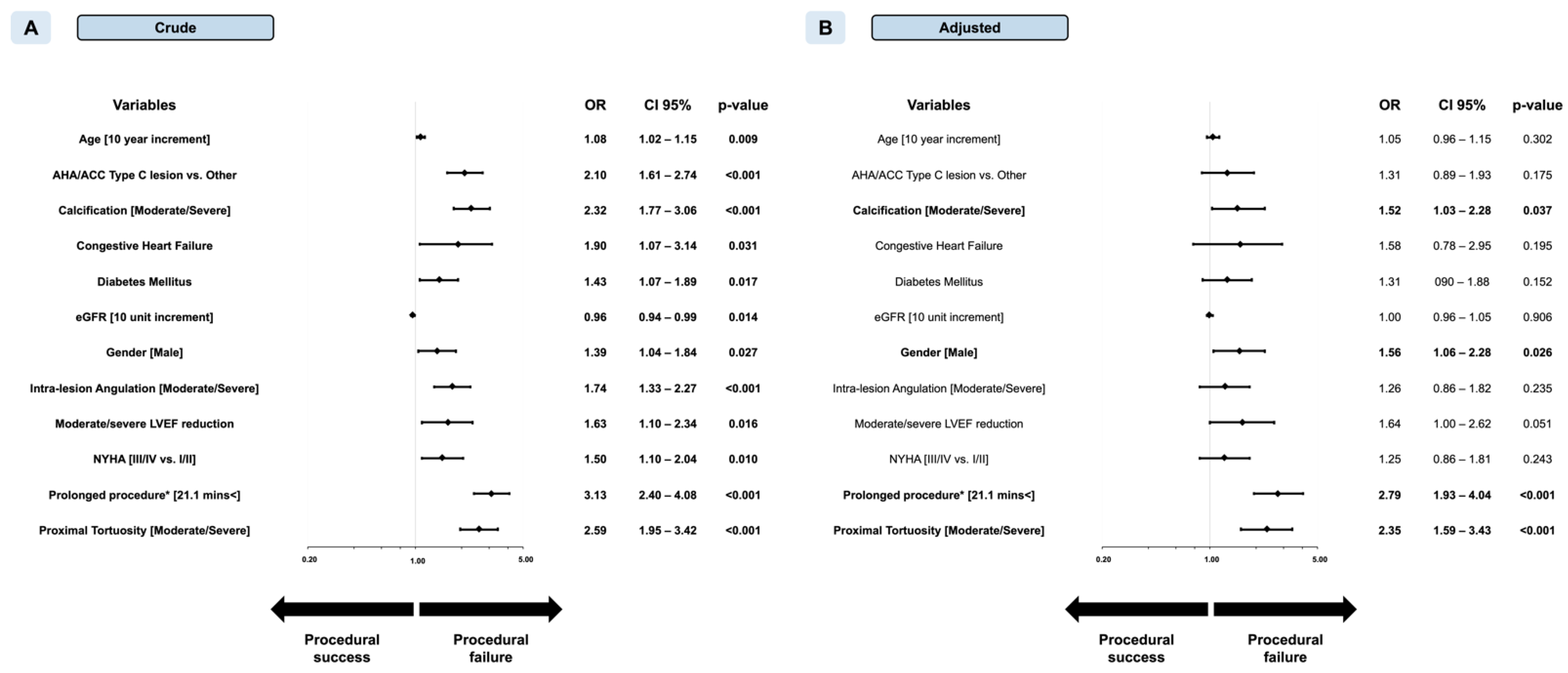
In the dichotomized analyses, fluoroscopy time above the cut-off was a strongly associated with procedural failure, roughly indicating a 2-fold increase in risk with CTO PCI and 3-fold increase with non-CTO PCI. Nevertheless, the discrimination was poor with AUCs of 0.665 (p < 0.001) and 0.613 (p < 0.001), respectively.
In prior studies, target lesion complexity has been associated with increasing need for PCI resources, such as contrast volume, radiation, and fluoroscopy time [
7]. However, the reverse association between PCI prolongation and procedural outcomes—preferably using fluoroscopy time as indicator—has been rarely studied. Nikolsky et al. examined the relation between fluoroscopy time and short-term PCI prognosis in 9650 consecutive PCIs, in which 75th percentile threshold was utilized (18.3 ± 12.2 min) (2) as prolonged fluoroscopy time. Procedure prolongation was associated with an increased risk of in-hospital mortality (3.3% vs. 0.3%,
p < 0.0001) emergent surgery (2.1% vs. 0.3%,
p = 0.0001), and contrast-induced nephropathy (6.7% vs. 4.5%,
p = 0.03). In a report from the United States National Cardiovascular Data Registry, Fazel et al. also analyzed the fluoroscopy time factor during invasive coronary angiography and percutaneous coronary intervention; however, they sought to evaluate the determinants of fluoroscopy time elongation but not its effect on procedural success and incidence of major complications related to PCI [
8].
In previous studies, thresholds for defining procedure prolongation were simply selected as fluoroscopy time exceeding >75th percentile in the entire cohort (2,7). However, various procedures, such as CTO and non-CTO PCI, substantially differ in terms of techniques and clinical consequences. We, therefore, addressed the interaction of type of PCI (CTO versus non-CTO) with the impact of fluoroscopy time on procedural success in our multivariable logistic regression model. Based on a highly significant interaction as revealed by this model, we were able to calculate different cut-off values of procedure prolongation for CTO and non-CTO PCI. In a sensitivity analysis, we also confirmed that our findings were robust with respect to the definition of myocardial infarction. A similar association between fluoroscopy time and procedural success was present when implementing the SCAI definition instead of the fourth Universal Definition [
9].
Our study has limitations. First, it has a retrospective, observational design without core laboratory assessment of the study angiograms or independent clinical event adjudication. Second, procedural complications, such as perforation, are self-reported; however, the occurrence of MACCE underwent a quality check performed by the dedicated independent committee of our institution. Third, study procedures were performed in a dedicated, high-volume CTO referral center. Fluoroscopy time thresholds and their effect on in-hospital outcomes may differ numerically in other cohorts. Fourth, our study was not designed to elucidate the underlying mechanism of the observed association between procedural failure and fluoroscopy time. To a large extent, prolonged fluoroscopy times are a reflection of the number and complexity of lesions treated, which both impact the risk of complications and technical failure. Therefore, this association is an epiphenomenon rather than responsible for success or failure of a procedure. On the other hand, excessive procedure duration may be detrimental in itself due to exhaustion of patients, toxic effects of contrast media, and operator fatigue.




 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}