
What Are the Biomechanical Properties of an Aortic Aneurysm Associated with Quadricuspid Aortic Valve?

 , , ,
, , ,  and
and
Abstract
:
1. Introduction
2. Population
3. Method
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANT | Anterior |
| AsAA | ascending aortic aneurysms |
| BAV | bicuspid aortic valve |
| CIR | circumferential |
| LAT | lateral |
| LON | longitudinal |
| MED | medial |
| POST | posterior |
| QAV | quadricuspid aortic valve |
| TAV | tricuspid aortic valve |
References
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. Corrigendum to: 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur. Heart J. 2015, 36, 2779. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Siu, S.C. Aortic Dilatation in Patients with Bicuspid Aortic Valve. N. Engl. J. Med. 2014, 370, 1920–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, S.-M. Quadricuspid Aortic Valve: A Comprehensive Review. Braz. J. Cardiovasc. Surg. 2016, 31, 454–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigaeva, T.; Sommer, G.; Holzapfel, G.A.; Di Martino, E. Anisotropic residual stresses in arteries. J. R. Soc. Interface 2019, 16, 20190029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.; Morgant, M.C.; Marín-Castrillón, D.M.; Walker, P.M.; Glélé, L.S.A.; Boucher, A.; Presles, B.; Bouchot, O.; Lalande, A. Aortic local biomechanical properties in ascending aortic aneurysms. Acta Biomater. 2022, 149, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, A.; Totaro, P.; Morganti, S.; Auricchio, F. Effects of clinico-pathological risk factors on in-vitro mechanical properties of human dilated ascending aorta. J. Mech. Behav. Biomed. Mater. 2018, 77, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Morgant, M.; Lalande, A.; Cochet, A.; Bouchot, O. Local ex-vivo evaluation of the biomechanical properties of the ascending aortic aneurysms. Arch. Cardiovasc. Dis. Suppl. 2020, 12, 145. [Google Scholar] [CrossRef]
- Bersi, M.R.; Bellini, C.; Humphrey, J.D.; Avril, S. Local variations in material and structural properties characterize murine thoracic aortic aneurysm mechanics. Biomech. Model. Mechanobiol. 2019, 18, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Shahmansouri, N.; Alreshidan, M.; Emmott, A.; Lachapelle, K.; El-Hamamsy, I.; Cartier, R.; Leask, R.L.; Mongrain, R. Investigation on the Regional Loss Factor and Its Anisotropy for Aortic Aneurysms. Materials 2016, 9, 867. [Google Scholar] [CrossRef]
- Hosoda, Y.; Kawano, K.; Yamasawa, F.; Ishii, T.; Shibata, T.; Inayama, S. Age-Dependent Changes of Collagen and Elastin Content in Human Aorta and Pulmonary Artery. Angiology 1984, 35, 615–621. [Google Scholar] [CrossRef]
- Tsamis, A.; Krawiec, J.T.; Vorp, D.A. Elastin and collagen fibre microstructure of the human aorta in ageing and disease: A review. J. R. Soc. Interface 2013, 10, 20121004. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AsAA-QAV | AsAA-TAV | AsAA-BAV | |
|---|---|---|---|
| Aortic diameter (mm) | 52 | 53 | 53 |
| Age (years) | 63 | 44 | 58 |
| Gender | Female | Male | Male |
| Tobacco use | − | − | − |
| Dyslipidemia | − | − | − |
| Hypertension | + | + | − |
| Obesity | − | + | + |
| Diabetes | − | − | − |
| Coronary arterial disease | − | − | − |
| Aortic insufficiency | + | − | − |
| Aortic stenosis | − | − | + |
| AsAA-QAV | AsAA-TAV | AsAA-BAV | |||
|---|---|---|---|---|---|
| MED | Failure stiffness (MPa) | LON | 0.579 | 0.630 | 0.661 |
| CIR | 0.676 | 0.891 | 0.717 | ||
| Thickness (mm) | 2.41 | 2.256 | 1.714 | ||
| ANT | Failure stiffness (MPa) | LON | 0.698 | 0.775 | 0.667 |
| CIR | 0.889 | 0.941 | 0.932 | ||
| Thickness (mm) | 2.06 | 1.64 | 1.498 | ||
| LAT | Failure stiffness (MPa) | LON | 1.034 | 1.145 | 1.087 |
| CIR | 0.911 | 1.250 | 0.905 | ||
| Thickness (mm) | 2.212 | 1.78 | 1.306 | ||
| POST | Failure stiffness (MPa) | LON | 0.913 | 0.667 | 1.083 |
| CIR | 1.509 | 0.814 | 1.384 | ||
| Thickness (mm) | 2.064 | 1.574 | 1.586 |
| AsAA-QAV | AsAA-TAV | AsAA-BAV | ||
|---|---|---|---|---|
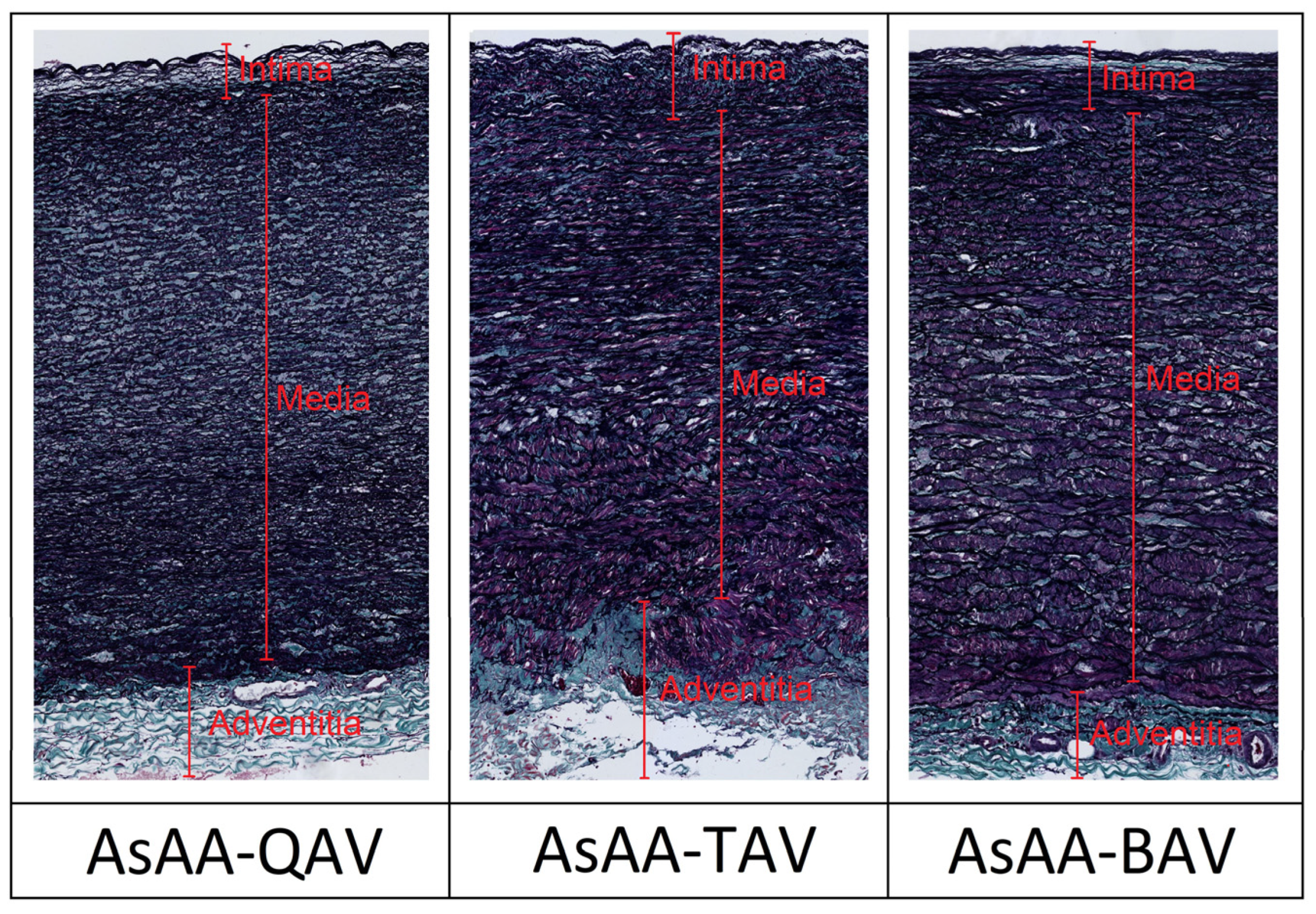
| Collagen (%) | Intima | 15.925 | 23.227 | 18.119 |
| Media | 17.29 | 20.689 | 20.878 | |
| Adventitia | 34.612 | 43.273 | 43.985 | |
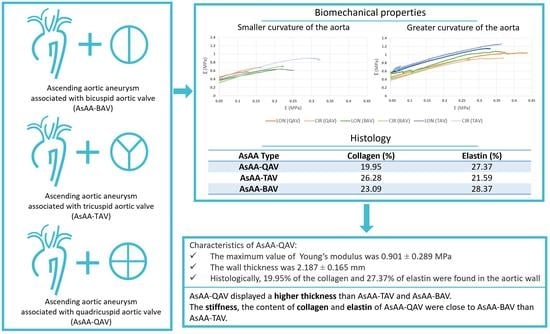
| Total | 19.95 | 26.28 | 23.09 | |
| Elastin (%) | Intima | 24.337 | 19.297 | 34.682 |
| Media | 31.681 | 28.83 | 31.142 | |
| Adventitia | 7.175 | 4.96 | 9.995 | |
| Total | 27.37 | 21.59 | 28.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.; Morgant, M.-C.; Marín-Castrillón, D.M.; Bernard, C.; Boucher, A.; Presles, B.; Lalande, A.; Bouchot, O. What Are the Biomechanical Properties of an Aortic Aneurysm Associated with Quadricuspid Aortic Valve? J. Clin. Med. 2022, 11, 4897. https://doi.org/10.3390/jcm11164897
Lin S, Morgant M-C, Marín-Castrillón DM, Bernard C, Boucher A, Presles B, Lalande A, Bouchot O. What Are the Biomechanical Properties of an Aortic Aneurysm Associated with Quadricuspid Aortic Valve? Journal of Clinical Medicine. 2022; 11(16):4897. https://doi.org/10.3390/jcm11164897
Chicago/Turabian StyleLin, Siyu, Marie-Catherine Morgant, Diana M. Marín-Castrillón, Chloé Bernard, Arnaud Boucher, Benoît Presles, Alain Lalande, and Olivier Bouchot. 2022. "What Are the Biomechanical Properties of an Aortic Aneurysm Associated with Quadricuspid Aortic Valve?" Journal of Clinical Medicine 11, no. 16: 4897. https://doi.org/10.3390/jcm11164897
APA StyleLin, S., Morgant, M.-C., Marín-Castrillón, D. M., Bernard, C., Boucher, A., Presles, B., Lalande, A., & Bouchot, O. (2022). What Are the Biomechanical Properties of an Aortic Aneurysm Associated with Quadricuspid Aortic Valve? Journal of Clinical Medicine, 11(16), 4897. https://doi.org/10.3390/jcm11164897