
Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Searches
2.2. Study Selection and Outcomes
2.3. Data Extraction and Quality Appraisal
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
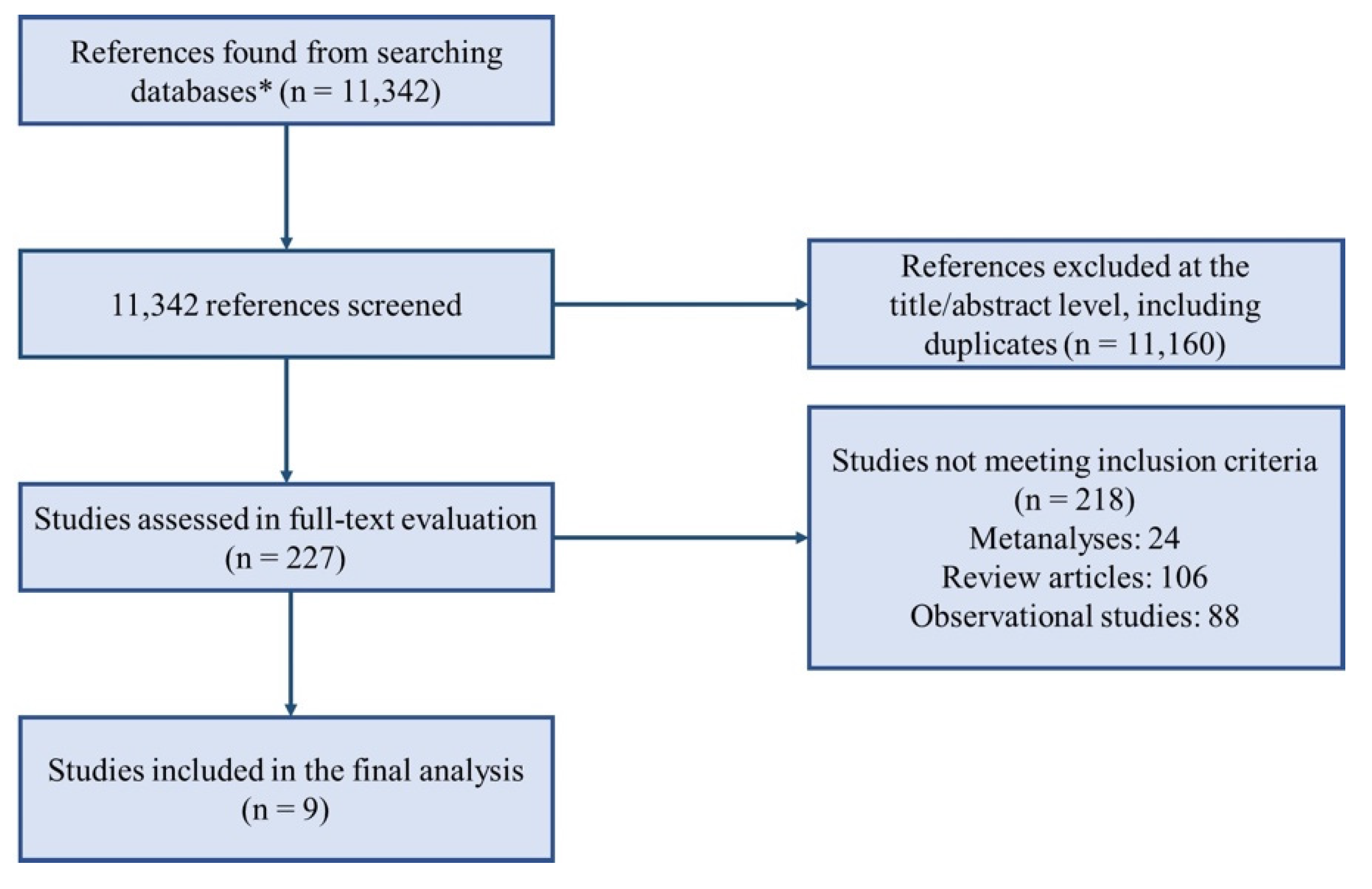
3.1. Study Selection
3.2. Baseline Characteristics
3.3. Composite Endpoint, All-Cause Mortality, HF Hospitalizations
3.4. Other Secondary Endpoints
3.5. Safety Endpoints
3.6. Sensitivity Analyses
- -
- Catheter Ablation vs. Rate Control
- -
- LVEF ≤ 50%
- -
- Persistent AF
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AATAC | Ablation versus Amiodarone for Treatment of Atrial Fibrillation in Patients with Congestive Heart Failure and an Implanted ICD |
| AF | Atrial Fibrillation |
| AMICA | Atrial Fibrillation Management in Congestive Heart Failure with Ablation |
| ARC-HF | A Randomized Trial to Assess Catheter Ablation Versus Rate Control in the Management of Persistent Atrial Fibrillation in Chronic Heart Failure |
| BNP | Brain Natriuretic Peptide |
| CA | Catheter Ablation |
| CABANA | Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation |
| CAD | Coronary Artery Disease |
| CAMERA-MRI | Catheter Ablation Versus Medical Rate Control in Atrial Fibrillation and Systolic Dysfunction |
| CAMTAF | A Randomized Controlled Trial of Catheter Ablation Versus Medical Treatment of Atrial Fibrillation in Heart Failure |
| CASTLE-AF | Catheter Ablation versus Standard Conventional Therapy in Patients with Left Ventricular Dysfunction and Atrial Fibrillation |
| CIED | Cardiac Implantable Electronic Device |
| CRT-D | Cardiac Resynchronization Therapy Defibrillator |
| CV | Cardiovascular |
| ECG | Electrocardiogram |
| HF | Heart Failure |
| LVEF | Left Ventricular Ejection Fraction |
| MLHFQ | Minnesota Living with Heart Failure Questionnaire |
| MT | Medical Therapy |
| MRI | Magnetic Resonance Imaging |
| NYHA | New York Heart Association |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PVI | Pulmonary Vein Isolation |
| RAFT | Randomized Ablation-Based Rhythm-Control Versus Rate-Control |
| RCT | Randomized Controlled Trial |
| RR | Risk Ratio |
| SVC | Superior Vena Cava |
| VO2 max | Peak Oxygen Consumption |
| 6MWT | 6-Min Walk Test |
References
- Sanders, P.; Morton, J.B.; Davidson, N.C.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrical remodeling of the atria in congestive heart failure: Electrophysiological and electroanatomic mapping in humans. Circulation 2003, 108, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.A.; Lambiase, P.D. Pathophysiology, diagnosis and treatment of tachycardiomyopathy. Heart 2017, 103, 1543. [Google Scholar] [CrossRef]
- Della Rocca, D.G.; Santini, L.; Forleo, G.B.; Sanniti, A.; Del Prete, A.; Lavalle, C.; Di Biase, L.; Natale, A.; Romeo, F. Novel Perspectives on Arrhythmia-Induced Cardiomyopathy: Pathophysiology, Clinical Manifestations and an Update on Invasive Management Strategies. Cardiol. Rev. 2015, 23, 135–141. [Google Scholar] [CrossRef]
- Della Rocca, D.G.; Tarantino, N.; Trivedi, C.; Mohanty, S.; Anannab, A.; Salwan, A.S.; Gianni, C.; Bassiouny, M.; Al-Ahmad, A.; Romero, J.; et al. Non-pulmonary vein triggers in nonparoxysmal atrial fibrillation: Implications of pathophysiology for catheter ablation. J. Cardiovasc. Electrophysiol. 2020, 31, 2154–2167. [Google Scholar] [CrossRef] [PubMed]
- Maisel, W.H.; Stevenson, L.W. Atrial fibrillation in heart failure: Epidemiology, pathophysiology, and rationale for therapy. Am. J. Cardiol. 2003, 91, 2D–8D. [Google Scholar] [CrossRef]
- Dries, D.L.; Exner, D.V.; Gersh, B.J.; Domanski, M.J.; Waclawiw, M.A.; Stevenson, L.W. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: A retrospective analysis of the SOLVD trials. Studies of Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 1998, 32, 695–703. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Vasan, R.S.; Leip, E.P.; Wolf, P.A.; D’Agostino, R.B.; Murabito, J.M.; Kannel, W.B.; Benjamin, E.J. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: The Framingham Heart Study. Circulation 2003, 107, 2920–2925. [Google Scholar] [CrossRef] [PubMed]
- The Stroke Prevention in Atrial Fibrillation Investigators. Predictors of thromboembolism in atrial fibrillation: I. Clinical features of patients at risk. Ann. Intern. Med. 1992, 116, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bardy, G.H.; Lee, K.L.; Mark, D.B.; Poole, J.E.; Packer, D.L.; Boineau, R.; Domanski, M.; Troutman, C.; Anderson, J.; Johnson, G.; et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N. Engl. J. Med. 2005, 352, 225–237. [Google Scholar] [CrossRef]
- Flaker, G.C.; Blackshear, J.L.; McBride, R.; Kronmal, R.A.; Halperin, J.L.; Hart, R.G. Antiarrhythmic drug therapy and cardiac mortality in atrial fibrillation. The Stroke Prevention in Atrial Fibrillation Investigators. J. Am. Coll. Cardiol. 1992, 20, 527–532. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, E.S.; Zimmermann, P.A.; Wang, T.; Dennish, G.W., 3rd; Barrell, P.D.; Chandler, M.L.; Greene, H.L. Risk of proarrhythmic events in the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study: A multivariate analysis. J. Am. Coll. Cardiol. 2004, 44, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.-H.; Merkely, B.; Zahn, R.; Arentz, T.; Seidl, K.; Schlüter, M.; Tilz, R.R.; Piorkowski, C.; Gellér, L.; Kleemann, T.; et al. Catheter Ablation Versus Best Medical Therapy in Patients With Persistent Atrial Fibrillation and Congestive Heart Failure. Circ. Arrhythmia Electrophysiol. 2019, 12, e007731. [Google Scholar] [CrossRef]
- Parkash, R.; Wells, G.A.; Rouleau, J.; Talajic, M.; Essebag, V.; Skanes, A.; Wilton, S.B.; Verma, A.; Healey, J.S.; Sterns, L.; et al. Randomized Ablation-Based Rhythm-Control Versus Rate-Control Trial in Patients With Heart Failure and Atrial Fibrillation: Results from the RAFT-AF trial. Circulation 2022, 145, 1693–1704. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Packer, D.L.; Piccini, J.P.; Monahan, K.H.; Al-Khalidi, H.R.; Silverstein, A.P.; Noseworthy, P.A.; Poole, J.E.; Bahnson, T.D.; Lee, K.L.; Mark, D.B.; et al. Ablation Versus Drug Therapy for Atrial Fibrillation in Heart Failure. Circulation 2021, 143, 1377–1390. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Di Biase, L.; Mohanty, P.; Mohanty, S.; Santangeli, P.; Trivedi, C.; Lakkireddy, D.; Reddy, M.; Jais, P.; Themistoclakis, S.; Dello Russo, A.; et al. Ablation Versus Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients With Congestive Heart Failure and an Implanted Device. Circulation 2016, 133, 1637–1644. [Google Scholar] [CrossRef]
- Hunter, R.J.; Berriman, T.J.; Diab, I.; Kamdar, R.; Richmond, L.; Baker, V.; Goromonzi, F.; Sawhney, V.; Duncan, E.; Page, S.P.; et al. A Randomized Controlled Trial of Catheter Ablation Versus Medical Treatment of Atrial Fibrillation in Heart Failure (The CAMTAF Trial). Circ. Arrhythmia Electrophysiol. 2014, 7, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Jones, D.G.; Haldar, S.K.; Hussain, W.; Sharma, R.; Francis, D.P.; Rahman-Haley, S.L.; McDonagh, T.A.; Underwood, S.R.; Markides, V.; Wong, T. A Randomized Trial to Assess Catheter Ablation Versus Rate Control in the Management of Persistent Atrial Fibrillation in Heart Failure. J. Am. Coll. Cardiol. 2013, 61, 1894–1903. [Google Scholar] [CrossRef] [PubMed]
- Sugumar, H.; Prabhu, S.; Costello, B.; Chieng, D.; Azzopardi, S.; Voskoboinik, A.; Parameswaran, R.; Wong, G.R.; Anderson, R.; Al-Kaisey, A.M.; et al. Catheter Ablation Versus Medication in Atrial Fibrillation and Systolic Dysfunction: Late Outcomes of CAMERA-MRI Study. JACC Clin. Electrophysiol. 2020, 6, 1721–1731. [Google Scholar] [CrossRef]
- MacDonald, M.R.; Connelly, D.T.; Hawkins, N.M.; Steedman, T.; Payne, J.; Shaw, M.; Denvir, M.; Bhagra, S.; Small, S.; Martin, W.; et al. Radiofrequency ablation for persistent atrial fibrillation in patients with advanced heart failure and severe left ventricular systolic dysfunction: A randomised controlled trial. Heart 2011, 97, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, S.; Taylor, A.J.; Costello, B.T.; Kaye, D.M.; McLellan, A.J.A.; Voskoboinik, A.; Sugumar, H.; Lockwood, S.M.; Stokes, M.B.; Pathik, B.; et al. Catheter Ablation Versus Medical Rate Control in Atrial Fibrillation and Systolic Dysfunction: The CAMERA-MRI Study. J. Am. Coll. Cardiol. 2017, 70, 1949–1961. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Mohanty, P.; Trivedi, C.; Gianni, C.; Della Rocca, D.G.; Di Biase, L.; Natale, A. Long-Term Outcome of Pulmonary Vein Isolation With and Without Focal Impulse and Rotor Modulation Mapping: Insights From a Meta-Analysis. Circ. Arrhythmia Electrophysiol. 2018, 11, e005789. [Google Scholar] [CrossRef]
- Della Rocca, D.G.; Di Biase, L.; Mohanty, S.; Trivedi, C.; Gianni, C.; Romero, J.; Tarantino, N.; Magnocavallo, M.; Bassiouny, M.; Natale, V.N.; et al. Targeting non-pulmonary vein triggers in persistent atrial fibrillation: Results from a prospective, multicentre, observational registry. EP Eur. 2021, 23, 1939–1949. [Google Scholar] [CrossRef]
- Mohanty, S.; Trivedi, C.; Horton, P.; Della Rocca, D.G.; Gianni, C.; MacDonald, B.; Mayedo, A.; Sanchez, J.; Gallinghouse, G.J.; Al-Ahmad, A.; et al. Natural History of Arrhythmia After Successful Isolation of Pulmonary Veins, Left Atrial Posterior Wall, and Superior Vena Cava in Patients With Paroxysmal Atrial Fibrillation: A Multi-Center Experience. JAHA 2021, 10, e020563. [Google Scholar] [CrossRef]
- Turagam, M.K.; Garg, J.; Whang, W.; Sartori, S.; Koruth, J.S.; Miller, M.A.; Langan, N.; Sofi, A.; Gomes, A.; Choudry, S.; et al. Catheter Ablation of Atrial Fibrillation in Patients With Heart Failure. Ann. Intern. Med. 2019, 170, 41–50. [Google Scholar] [CrossRef]
- Briceño, D.F.; Markman, T.M.; Lupercio, F.; Romero, J.; Liang, J.J.; Villablanca, P.A.; Birati, E.Y.; Garcia, F.C.; Di Biase, L.; Natale, A.; et al. Catheter ablation versus conventional treatment of atrial fibrillation in patients with heart failure with reduced ejection fraction: A systematic review and meta-analysis of randomized controlled trials. J. Interv. Card. Electrophysiol. 2018, 53, 19–29. [Google Scholar] [CrossRef]
- Andrade, J.G.; Wells, G.A.; Deyell, M.W.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.-F.; Yung, D.; Skanes, A.; Khaykin, Y.; et al. Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 305–315. [Google Scholar] [CrossRef]
- Della Rocca, D.G.; Mohanty, S.; Mohanty, P.; Trivedi, C.; Gianni, C.; Al-Ahmad, A.; Burkhardt, J.D.; Gallinghouse, G.J.; Hranitzky, P.; Sanchez, J.E.; et al. Long-term outcomes of catheter ablation in patients with longstanding persistent atrial fibrillation lasting less than 2 years. J. Cardiovasc. Electrophysiol. 2018, 29, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Trivedi, C.; Gianni, C.; Della Rocca, D.G.; Morris, E.H.; Burkhardt, J.D.; Sanchez, J.E.; Horton, R.; Gallinghouse, G.J.; Hongo, R.; et al. Procedural findings and ablation outcome in patients with atrial fibrillation referred after two or more failed catheter ablations. J. Cardiovasc. Electrophysiol. 2017, 28, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Natale, V.; Mohanty, S.; Trivedi, C.; Baqai, F.M.; Gallinghouse, J.; Della Rocca, D.G.; Gianni, C.; MacDonald, B.; Mayedo, A.; Burkhardt, J.D.; et al. Arrhythmia profile and ablation-outcome in elderly women with atrial fibrillation undergoing first catheter ablation. Pacing Clin. Electrophysiol. 2021, 44, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.N.; Jaïs, P.; Cummings, J.; Di Biase, L.; Sanders, P.; Martin, D.O.; Kautzner, J.; Hao, S.; Themistoclakis, S.; Fanelli, R.; et al. Pulmonary-Vein Isolation for Atrial Fibrillation in Patients with Heart Failure. N. Engl. J. Med. 2008, 359, 1778–1785. [Google Scholar] [CrossRef]
- Della Rocca, D.G.; Magnocavallo, M.; Natale, V.N.; Gianni, C.; Mohanty, S.; Trivedi, C.; Lavalle, C.; Forleo, G.B.; Tarantino, N.; Romero, J.; et al. Clinical presentation, diagnosis, and treatment of atrioesophageal fistula resulting from atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2021, 32, 2441–2450. [Google Scholar] [CrossRef]
- Mohanty, S.; Trivedi, C.; Della Rocca, D.G.; Gianni, C.; MacDonald, B.; Quintero Mayedo, A.; Al-Ahmad, A.; Burkhardt, J.D.; Bassiouny, M.; Gallinghouse, G.J.; et al. Recovery of Conduction Following High-Power Short-Duration Ablation in Patients With Atrial Fibrillation: A Single-Center Experience. Circ. Arrhythmia Electrophysiol. 2021, 14, e010096. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | MacDonald et al., 2011 [23] | ARC-HF, 2013 [21] | CAMTAF, 2014 [20] | AATAC, 2016 [19] | CAMERA-MRI, 2017 [24] | CASTLE-AF, 2018 [18] | AMICA, 2019 [13] | CAMERA LATE OUTCOMES, 2020 [22] | CABANA, 2021 [17] | RAFT-AF, 2022 [14] | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Monocentric or multicentric | Multicentric | Multicentric | Monocentric | Multicentric | Multicentric | Multicentric | Multicentric | Multicentric | Multicentric | Multicentric | |
| Comparison | Ablation vs. medical rate control | Ablation vs. medical rate control | Ablation vs. medical rate control | Ablation vs. amiodarone | Ablation vs. medical rate control | Ablation vs. medical rhythm and rate control | Ablation vs. medical rhythm and rate control | Ablation vs. medical rate control | Ablation vs. medical rhythm and rate control | Ablation vs. medical rate control | |
| HF inclusion criteria | NYHA class II or greater and optimal HF treatment for at least 3 months | NYHA class II or greater and optimal HF treatment for at least 1 month | NYHA class II or greater and optimal HF treatment for at least 3 months | NYHA class II to III | NYHA class ≥ II | NYHA class ≥ II | NYHA class II or greater and optimal HF treatment for at least 1 months | NYHA class ≥ II | NYHA class ≥ II | NYHA class II/III HF on optimal guideline directedmedical therapy and elevated NT-proBNP | |
| LVEF inclusion criterion | ≤35% (RNVG) | ≤35% | <50% | <40% | ≤45% | ≤35% | ≤35% | ≤45% | No LVEF inclusion criterion | No LVEF inclusion criterion | |
| Type of AF | Persistent | Persistent | Persistent | Persistent | Persistent | Paroxysmal or persistent | Persistent | Persistent | Paroxysmal or persistent | Paroxysmal or persistent | |
| Patients at randomization, n | Ablation | 22 | 26 | 26 | 102 | 34 | 200 | 104 | 34 | 378 | 214 |
| Drug | 19 | 26 | 24 | 101 | 34 | 197 | 98 | 34 | 400 | 197 | |
| Mean age, years (SD or IQR) | Ablation | 62.3 ± 6.7 | 64 ± 10 | 55 ± 12 | 62 ± 10 | 59 ± 11 | 64 (56–71) | 65 ± 8 | 60.5 ± 10.7 | 68 (62, 73) | 65.9 ± 8.6 |
| Drug | 64.4 ± 8.3 | 62 ± 9 | 60 ± 10 | 60 ± 11 | 62 ± 9.4 | 64 (56–73.5) | 65 ± 8 | 65.5 ± 7.2 | 67 (62, 73) | 67.5 ± 8.0 | |
| LVEF Baseline (SD or IQR), % | Ablation | 36.1 ± 11.9 (MRI) 16.1 ± 7.1 (RNVG) | 22 ± 8 (RNVG) | 31.8 ± 7.7 | 29 ± 5 | 35 ± 9.8 (MRI) | 32.5 (25.0–38.0) | 27.8 ± 9.5 | 36.1 ± 9.6 (MRI) | 55 (50-60) | EF ≤ 45%: 30.1 ± 8.5 EF > 45%: 55.9 ± 6.7 |
| Drug | 42.9 ± 9.6 (MRI) 19.6 ± 5.5 (RNVG) | 25 ± 7 (RNVG) | 33.7 ± 12.1 | 30 ± 8 | 35 ± 9.3 (MRI) | 31.5 (27.0–37.0) | 24.8 ± 8 | 34.6 ± 9.1 (MRI) | 56 (50-62) | EF ≤ 45%: 30.3 ± 9.2 EF > 45%: 54.6 ± 7.3 | |
| Mean baseline 6MWT (SD), meters | Ablation | 317.5 ± 125.8 | 416 ± 78 | NA | 348 ± 111 | 491 ± 147 | NA | NA | NA | NA | 363.1 ± 101.4 |
| Drug | 351.8 ± 117.1 | 411 ± 109 | NA | 350 ± 130 | 489 ± 132 | NA | NA | NA | NA | 344.4 ± 107.1 | |
| Mean baseline VO2 max (SD), mL/kg per min | Ablation | NA | 16.3 ± 5.3 | 22 | NA | NA | NA | NA | NA | NA | NA |
| Drug | NA | 18.2 ± 4.8 | 19.5 | NA | NA | NA | NA | NA | NA | NA | |
| Mean baseline MLHFQ score (SD) | Ablation | 55.8 ± 19.8 | 42 ± 23 | 42 | 52 ± 24 | NA | NA | NA | NA | NA | NA |
| Drug | 59.2 ± 22.4 | 49 ± 21 | 48 | 50 ± 27 | NA | NA | NA | NA | NA | NA | |
| Mean baseline BNP(SD or IQR), pg/mL | Ablation | NA | 412 ± 324 | NA | NA | 266 ± 210 | NA | NA | NA | NA | NA |
| Drug | NA | 283 ± 285 | NA | NA | 256 ± 208 | NA | NA | NA | NA | NA | |
| Follow-up | 6 mo | 12 mo | 6 and 12 mo | 24 mo | 6 mo | 60 mo | 12 mo | 4.0 ± 0.9 years | 48.5 mo | 24 mo |
| A. Periprocedural Complications | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study | Access Site Complications, n | Pericardial Effusion/tamponade, n | Esophageal Complications, n | Systemic Embolism, n | Pulmonary Stenosis, n | |||
| MacDonald et al., 2011 [23] | 0 | 2 | 0 | 0 | 0 | |||
| ARC-HF, 2013 [21] | 1 | 1 | 0 | 0 | 0 | |||
| CAMTAF, 2014 [20] | 0 | 1 | 0 | 1 | 0 | |||
| AATAC, 2016 [19] | 2 | 1 | 0 | 0 | 0 | |||
| CAMERA-MRI, 2017 [24] | 1 | 0 | 0 | 0 | 0 | |||
| CASTLE-AF, 2018 [18] | 3 | 3 | 0 | 0 | 1 | |||
| AMICA, 2019 [13] | 2 | 1 | 1 | 0 | 0 | |||
| CABANA, 2021 [17] | 15 | 2 | 4 | 0 | 0 | |||
| RAFT-AF, 2022 [14] | 9 | 6 | 1 | 4 | 0 | |||
| OVERALL, % | 2.37% | 0.8% | 0.07% | 0.01% | 0.001% | |||
| B. Antiarrhythmic Drug Adverse Events | ||||||||
| Study | Thyroid toxicity, n | Liver and Pulmonary toxicity, n | Proarrhythmic effect, n | Unspecified toxicity, n | ||||
| AATAC, 2016 [19] | 4 | 3 | ||||||
| CABANA, 2021 [17] | 9 | 2 | 3 | 5 | ||||
| RAFT-AF, 2022 [14] | 4 | 1 | ||||||
| OVERALL, % | 1.38% | 0.48% | 0.8% | 0.7% | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magnocavallo, M.; Parlavecchio, A.; Vetta, G.; Gianni, C.; Polselli, M.; De Vuono, F.; Pannone, L.; Mohanty, S.; Cauti, F.M.; Caminiti, R.; et al. Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2022, 11, 5530. https://doi.org/10.3390/jcm11195530
Magnocavallo M, Parlavecchio A, Vetta G, Gianni C, Polselli M, De Vuono F, Pannone L, Mohanty S, Cauti FM, Caminiti R, et al. Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2022; 11(19):5530. https://doi.org/10.3390/jcm11195530
Chicago/Turabian StyleMagnocavallo, Michele, Antonio Parlavecchio, Giampaolo Vetta, Carola Gianni, Marco Polselli, Francesco De Vuono, Luigi Pannone, Sanghamitra Mohanty, Filippo Maria Cauti, Rodolfo Caminiti, and et al. 2022. "Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 11, no. 19: 5530. https://doi.org/10.3390/jcm11195530