
Lesion-to-Liver SUVmax Ratio to Improve the Prognostic Value of the End of Treatment PET/CT in Diffuse Large B-Cell Lymphoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PET/CT Acquisition
2.3. PET/CT Analyses
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
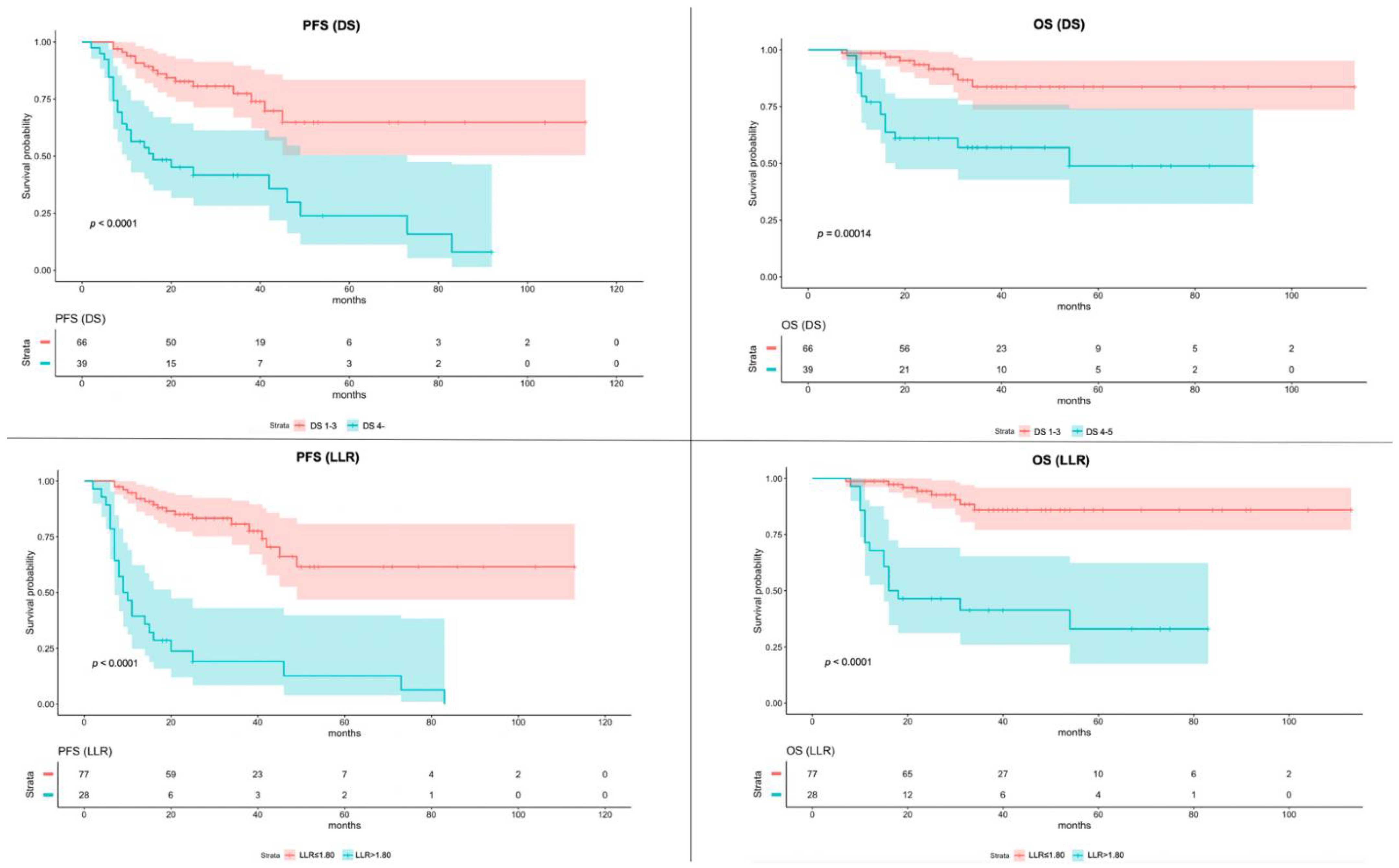
3.2. Survival Analyses Based on DS vs. LLR
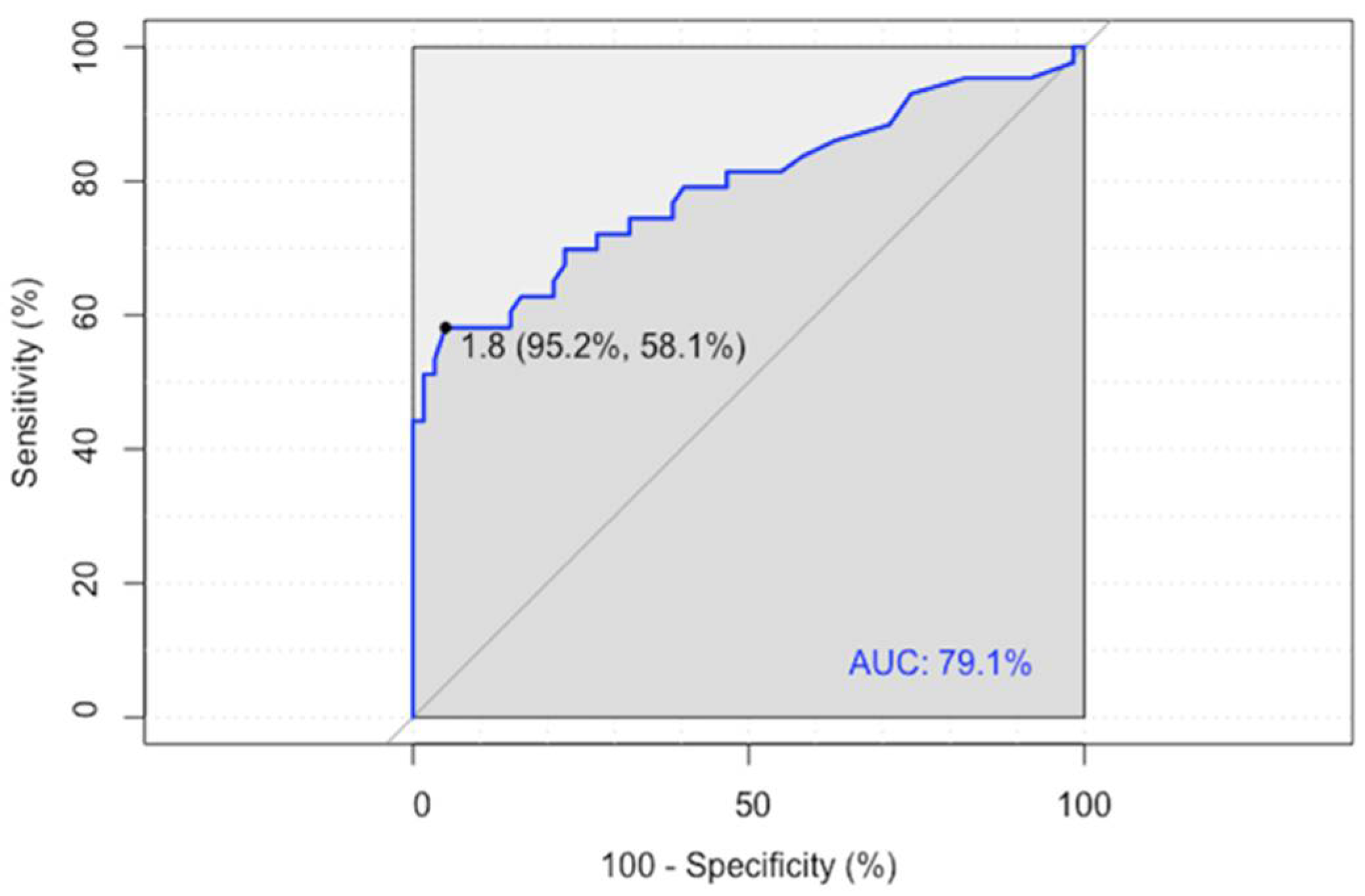
3.3. Diagnostic Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raut, L.; Chakrabarti, P. Management of Relapsed-Refractory Diffuse Large B Cell Lymphoma. South Asian J. Cancer 2014, 3, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Crump, M.; Neelapu, S.S.; Farooq, U.; van den Neste, E.; Kuruvilla, J.; Westin, J.; Link, B.K.; Hay, A.; Cerhan, J.R.; Zhu, L.; et al. Outcomes in Refractory Diffuse Large B-Cell Lymphoma: Results from the International SCHOLAR-1 Study. Blood 2017, 130, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Sawalha, Y. Relapsed/Refractory Diffuse Large B-Cell Lymphoma: A Look at the Approved and Emerging Therapies. J. Pers. Med. 2021, 11, 1345. [Google Scholar] [CrossRef]
- Pilkington, P.; Lopci, E.; Adam, J.A.; Kobe, C.; Goffin, K.; Herrmann, K. FDG-PET/CT Variants and Pitfalls in Haematological Malignancies. Semin. Nucl. Med. 2021, 51, 554–571. [Google Scholar] [CrossRef]
- Weiler-Sagie, M.; Bushelev, O.; Epelbaum, R.; Dann, E.J.; Haim, N.; Avivi, I.; Ben-Barak, A.; Ben-Arie, Y.; Bar-Shalom, R.; Israel, O. 18F-FDG Avidity in Lymphoma Readdressed: A Study of 766 Patients. J. Nucl. Med. 2010, 51, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Barrington, S. FDG-PET for the Early Treatment Monitoring, for Final Response and Follow-up Evaluation in Lymphoma. Clin. Transl. Imaging 2015, 3, 271–281. [Google Scholar] [CrossRef]
- Ferrari, C.; Asabella, N.; Merenda, N.; Altini, C.; Fanelli, M.; Muggeo, P.; de Leonardis, F.; Perillo, T.; Santoro, N.; Rubini, G. Pediatric Hodgkin Lymphoma Predictive Value of Interim 18 F-FDG PET/CT in Therapy Response Assessment. Medicine 2017, 96, e5973. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef]
- Ferrari, C.; Maggialetti, N.; Masi, T.; Nappi, A.G.; Santo, G.; Asabella, A.N.; Rubini, G. Early Evaluation of Immunotherapy Response in Lymphoma Patients by 18F-FDG PET/CT: A Literature Overview. J. Pers. Med. 2021, 11, 217. [Google Scholar] [CrossRef]
- Mamot, C.; Klingbiel, D.; Hitz, F.; Renner, C.; Pabst, T.; Driessen, C.; Mey, U.; Pless, M.; Bargetzi, M.; Krasniqi, F.; et al. Final Results of a Prospective Evaluation of the Predictive Value of Interim Positron Emission Tomography in Patients with Diffuse Large B-Cell Lymphoma Treated With R-CHOP-14 (SAKK 38/07). J. Clin. Oncol. 2015, 33, 2523–2529. [Google Scholar] [CrossRef]
- Voltin, C.A.; Mettler, J.; Grosse, J.; Dietlein, M.; Baues, C.; Schmitz, C.; Borchmann, P.; Kobe, C.; Hellwig, D. FDG-PET Imaging for Hodgkin and Diffuse Large B-Cell Lymphoma-An Updated Overview. Cancers 2020, 12, 601. [Google Scholar] [CrossRef] [PubMed]
- Juweid, M.E.; Mueller, M.; Alhouri, A.; A-Risheq, M.Z.; Mottaghy, F.M. Positron Emission Tomography/Computed Tomography in the Management of Hodgkin and B-Cell Non-Hodgkin Lymphoma: An Update. Cancer 2021, 127, 3727–3741. [Google Scholar] [CrossRef] [PubMed]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Cheson, B.D.; Meignan, M. Current Role of Functional Imaging in the Management of Lymphoma. Curr. Oncol. Rep. 2021, 23, 144. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Fan, Y.; Ying, Z.; Song, Y.; Zhu, J.; Yang, Z.; Wang, X. Can the SUV Max-Liver-Based Interpretation Improve Prognostic Accuracy of Interim and Posttreatment 18 F-FDG PET/CT in Patients with Diffuse Large B-Cell Lymphoma? Leuk. Lymphoma 2018, 59, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, S.; Pelliccioni, A.; Hohaus, S.; Maiolo, E.; Cuccaro, A.; Giordano, A. The Prognostic Role of End-of-Treatment FDG-PET/CT in Diffuse Large B Cell Lymphoma: A Pilot Study Application of Neural Networks to Predict Time-to-Event. Ann. Nucl. Med. 2021, 35, 102–110. [Google Scholar] [CrossRef]
- Li, Y.H.; Zhao, Y.M.; Jiang, Y.L.; Tang, S.; Chen, M.T.; Xiao, Z.Z.; Fan, W.; Hu, Y.Y.; Zhang, X. The Prognostic Value of End-of-Treatment FDG-PET/CT in Diffuse Large B Cell Lymphoma: Comparison of Visual Deauville Criteria and a Lesion-to-Liver SUV Max Ratio-Based Evaluation System. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1311–1321. [Google Scholar] [CrossRef]
- Teras, L.R.; DeSantis, C.E.; Cerhan, J.R.; Morton, L.M.; Jemal, A.; Flowers, C.R. 2016 US Lymphoid Malignancy Statistics by World Health Organization Subtypes. CA Cancer J. Clin. 2016, 66, 443–459. [Google Scholar] [CrossRef]
- Li, C.; Yu, H.; Chen, X.; Han, S.; Peng, S.; Lei, T.; Yang, H. The Prognostic Utility of 18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography-Based Analyses of Metabolic Response Rates in Newly Diagnosed Diffuse Large B Cell Lymphoma Patients. Front. Oncol. 2022, 12, 772773. [Google Scholar] [CrossRef]
- Lee, J.W.; Oh, D.; Eom, K.Y.; Kim, J.H.; Kim, W.C.; Chung, M.J.; Lee, J.H. The Prognostic Value of PET/CT Evaluation with Deauville Score on the Recurrence and Survival in Diffuse Large B-Cell Lymphoma: A Multi-Institutional Study of KROG 17-02. Clin. Exp. Metastasis 2020, 37, 125–131. [Google Scholar] [CrossRef]
- Burggraaff, C.N.; Cornelisse, A.C.; Hoekstra, O.S.; Lugtenburg, P.J.; de Keizer, B.; Arens, A.I.J.; Celik, F.; Huijbregts, J.E.; de Vet, H.C.W.; Zijlstra, J.M. Interobserver Agreement of Interim and End-of-Treatment 18F-FDG PET/CT in Diffuse Large B-Cell Lymphoma: Impact on Clinical Practice and Trials. J. Nucl. Med. 2018, 59, 1831–1836. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.N.; Vera, P.; Tilly, H.; Jardin, F.; Becker, S. Comparison of Therapeutic Evaluation Criteria in FDG-PET/CT in Patients with Diffuse Large-Cell B-Cell Lymphoma: Prognostic Impact of Tumor/Liver Ratio. PLoS ONE 2019, 14, e0211649. [Google Scholar] [CrossRef] [PubMed]
- Texte, E.; Lequesne, J.; Tilly, H.; Jardin, F.; Vera, P.; Stamatoullas, A.; Becker, S. SUVmax-Based Assessment of PET Response Shows a Superior Specificity to Deauville Criteria for Predicting Recurrence in Hodgkin’s Lymphoma. Leuk. Lymphoma 2020, 62, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, S.; Cuccaro, A.; Calcagni, M.L.; Hohaus, S.; Giordano, A.; Rufini, V. Interim FDG-PET/CT in Hodgkin Lymphoma: The Prognostic Role of the Ratio between Target Lesion and Liver SUVmax (RPET). Ann. Nucl. Med. 2016, 30, 588–592. [Google Scholar] [CrossRef]
- Eskian, M.; Alavi, A.; Khorasanizadeh, M.; Viglianti, B.L.; Jacobsson, H.; Barwick, T.D.; Meysamie, A.; Yi, S.K.; Iwano, S.; Bybel, B.; et al. Effect of Blood Glucose Level on Standardized Uptake Value (SUV) in 18 F-FDG PET-Scan: A Systematic Review and Meta-Analysis of 20,807 Individual SUV Measurements. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 224–237. [Google Scholar] [CrossRef]
- Sarikaya, I.; Sarikaya, A.; Sharma, P. Assessing the Effect of Various Blood Glucose Levels on 18 F-FDG Activity in the Brain, Liver, and Blood Pool. J. Nucl. Med. Technol. 2019, 47, 313–318. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients | 105 (100%) |
|---|---|
| Gender | |
| Male | 62 (59%) |
| Female | 43 (41%) |
| Age at diagnosis | |
| Median (range) | 61 (18–88) |
| Follow-up | |
| Median (range) | 30 (17–113) |
| Chemotherapy | |
| R-CHOP | 85 (81%) |
| R-COMP | 12 (11%) |
| EPOCH-R | 5 (5%) |
| R-MACOP-B | 3 (3%) |
| Ann Arbor Stage | |
| Stage I-II | 36 (34%) |
| Stage III-IV | 69 (66%) |
| Bulky | |
| Yes | 16 (15%) |
| No | 89 (85%) |
| Extranodal Involvement | |
| Yes | 55 (52%) |
| No | 50 (48%) |
| Variable | PFS | OS | ||
|---|---|---|---|---|
| p Value | HR (95% CI for exp(b)) | p Value | HR (95% CI for exp(b)) | |
| Age | 0.969 | 0.999 (0.980–1.020) | 0.0154 | 1.040 × 100 (1.0075–1.073) |
| Diabetes | 0.529 | 0.732 (0.277–1.935) | 0.2897 | 1.696 × 100 (0.6380–4.507) |
| Sex | 0.757 | 0.898 (0.455–1.773) | 0.0421 | 3.400 × 10−1 (0.1202–0.962) |
| Stage | 0.828 | 0.917 (0.419–2.005) | 0.6733 | 8.056 × 10−1 (0.2948–2.201) |
| Extranodal sites | 0.753 | 0.894 (0.446–1.795) | 0.1930 | 1.923 × 100 (0.7186–5.144) |
| Bulky disease | 0.734 | 0.851 (0.336–2.154) | 0.2572 | 4.707 × 10−1 (0.1278–1.733) |
| DS | 0.574 | 0.650 (0.145–2.920) | 0.9979 | 1.413 × 10−8 (0–inf) |
| LLR | 0.00178 | 10.939 (2.4401–49.037) | 0.9976 | 7.581 × 108 (0–inf) |
| Sensitivity | Specificity | PPV | NPV | Accuracy | ||
|---|---|---|---|---|---|---|
| Progression/Relapse | DS | 62.8 | 80.7 | 69.2 | 75.8 | 73.3 |
| LLR | 58.1 | 95.2 | 89.3 | 76.6 | 80.0 | |
| Survival | DS | 68.0 | 72.5 | 43.6 | 87.9 | 71.4 |
| LLR | 68.0 | 86.3 | 60.7 | 89.6 | 81.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, C.; Pisani, A.R.; Masi, T.; Santo, G.; Mammucci, P.; Rubini, D.; Sardaro, A.; Rubini, G. Lesion-to-Liver SUVmax Ratio to Improve the Prognostic Value of the End of Treatment PET/CT in Diffuse Large B-Cell Lymphoma. J. Clin. Med. 2022, 11, 5541. https://doi.org/10.3390/jcm11195541
Ferrari C, Pisani AR, Masi T, Santo G, Mammucci P, Rubini D, Sardaro A, Rubini G. Lesion-to-Liver SUVmax Ratio to Improve the Prognostic Value of the End of Treatment PET/CT in Diffuse Large B-Cell Lymphoma. Journal of Clinical Medicine. 2022; 11(19):5541. https://doi.org/10.3390/jcm11195541
Chicago/Turabian StyleFerrari, Cristina, Antonio Rosario Pisani, Tamara Masi, Giulia Santo, Paolo Mammucci, Dino Rubini, Angela Sardaro, and Giuseppe Rubini. 2022. "Lesion-to-Liver SUVmax Ratio to Improve the Prognostic Value of the End of Treatment PET/CT in Diffuse Large B-Cell Lymphoma" Journal of Clinical Medicine 11, no. 19: 5541. https://doi.org/10.3390/jcm11195541
APA StyleFerrari, C., Pisani, A. R., Masi, T., Santo, G., Mammucci, P., Rubini, D., Sardaro, A., & Rubini, G. (2022). Lesion-to-Liver SUVmax Ratio to Improve the Prognostic Value of the End of Treatment PET/CT in Diffuse Large B-Cell Lymphoma. Journal of Clinical Medicine, 11(19), 5541. https://doi.org/10.3390/jcm11195541