
Association of Body Mass Index, Blood Pressure, and Interictal Serum Levels of Cytokines in Migraine with and without Aura


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Laboratory Assays
2.3. Statistical Analysis
3. Results
3.1. Association of BMI, BP, and Cytokines Regarding Migraine Type–Migraine with or without Aura
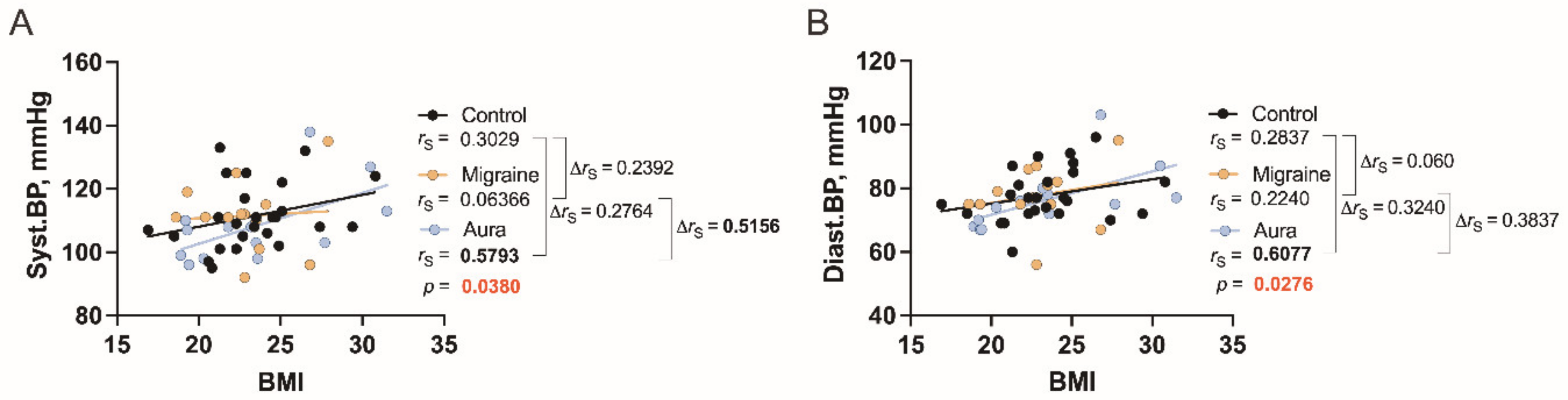
3.2. Correlations between BMI and BP in the Study Groups
3.3. Correlations between BMI and Cytokines Levels in the Study Groups
3.4. Correlations between BP and Cytokines Levels in the Study Groups
3.5. Covariances of the Investigated Cytokines in the Study Groups
4. Discussion
4.1. Cytokine Levels in Blood Serum Including Migraine Patients with and without Aura
4.2. Correlates of BMI and BP, Including Cytokines, in Migraineurs with and without Aura
4.3. Cytokine Intercorrelations in Migraineurs with and without Aura
4.4. Potential Biomarkers to Distinguish Migraine Patients from Healthy Individuals
5. Conclusions
- Migraine patients have elevated levels of IL-8, but decreased serum levels of PAI-1 and sICAM-1 during the interictal period, regardless of aura;
- Pronounced association of BMI with BP (both systolic and diastolic), and also with IFN-γ and MMP-9 is observed only in patients with aura;
- In patients with aura, only diastolic BP correlates with sICAM-1 (and inversely compared to control) and sVCAM-1, but in patients without aura, both systolic and diastolic BP correlates with MCP-1, and these associations are opposite compared to the control;
- Regarding cytokine intercorrelations, there are three correlations in migraine patients with aura that are absent in patients without aura: between IL-8 and PAI-1; MMP-9 and IL-8; and IL-8 and sICAM-1;
- Migraine patients without aura, on the other hand, have correlations that patients with aura do not: between PAI-1 and MCP-1, sICAM-1; between MMP-9 and sICAM-1, MCP-1; between TGF-α and PAI-1, MMP-9, and sICAM-1; between sICAM-1 and MMP-9, PAI-1, and MCP-1; as well as between sVCAM-1 and MCP-1;
- There are also correlations that are present in all migraine patients, but are more pronounced in patients without aura: between PAI-1 and MMP-9, TGF-α; between MMP-9 and PAI-1, TGF-α; between TGF-α and PAI-1, MMP-9, and sICAM-1; as well as between sVCAM-1 and IL-8;
- PAI-1, TGF, and MMP-9 could be used as potential biomarkers to distinguish migraine patients from healthy individuals.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Togha, M.; Haghdoost, F.; Khorsha, F.; Jahromi, S.R.; Zeinab Ghorbani, Z. Body mass index and its association with migraine characteristics in female patients. Arch. Iran. Med. 2019, 22, 554–559. Available online: http://www.aimjournal.ir/Article/aim-5516 (accessed on 26 September 2022). [PubMed]
- Danese, E.; Montagnana, M.; Lippi, G. Platelets and migraine. Thromb. Res. 2014, 134, 17–22. Available online: https://scholar.google.lv/scholar?q=doi:+10.1016/j.thromres.2014.03.055&hl=en&as_sdt=0&as_vis=1&oi=scholart (accessed on 26 September 2022). [CrossRef] [PubMed]
- Han, D. Association of serum levels of calcitonin gene-related peptide and cytokines during migraine attacks. Ann. Indian Acad. Neurol. 2019, 22, 277–281. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6613407/ (accessed on 26 September 2022). [CrossRef] [PubMed]
- Munno, I.; Centonze, V.; Marinaro, M.; Bassi, A.; Lacedra, G.; Causarano, V.; Nardelli, P.; Cassiano, M.A.; Albano, O. Cytokines and migraine: Increase of IL-5 and IL-4 plasma levels. Headache 1998, 38, 465–467. [Google Scholar] [CrossRef] [PubMed]
- Bruno, P.P.; Carpino, F.; Carpino, G.; Zicari, A. An overview on immune system and migraine. Eur. Rev. Med. Pharmacol. Sci. 2007, 11, 245–248. Available online: http://europeanreview.org/wp/wp-content/uploads/446.pdf (accessed on 26 September 2022). [PubMed]
- Ornello, R.; Ripa, P.; Pistoia, F.; Degan, D.; Tiseo, C.; Carolei, A.; Sacco, S. Migraine and body mass index categories: A systematic review and meta-analysis of observational studies. J. Headache Pain 2015, 16, 27. Available online: https://thejournalofheadacheandpain.biomedcentral.com/articles/10.1186/s10194-015-0510-z (accessed on 26 September 2022). [CrossRef] [PubMed]
- Seçil, Y.; Unde, C.; Beckmann, Y.Y.; Bozkaya, Y.T.; Ozerkan, F.; Başoğlu, M. Blood pressure changes in migraine patients before, during and after migraine attacks. Pain Pract. 2010, 10, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Rist, P.M.; Winter, A.C.; Buring, J.B.; Sesso, H.D.; Kurth, T. Migraine and the risk of incident hypertension among women. Cephalalgia 2018, 38, 1817–1824. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6026578/ (accessed on 26 September 2022). [CrossRef] [PubMed]
- Fagernæs, C.F.; Heuch, I.I.; Zwart, J.-A.; Winsvold, B.S.; Linde, M.; Hagen, K. Blood pressure as a risk factor for headache and migraine: A prospective population-based study. Eur. J. Neurol. 2015, 22, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Arca, K.N.; Singh, R.B.H. The hypertensive headache: A review. Curr. Pain Headache Rep. 2019, 23, 30. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. Available online: https://journals.sagepub.com/doi/epub/10.1177/0333102417738202 (accessed on 26 September 2022). [CrossRef]
- Sarchielli, P.; Alberti, A.; Vaianella, L.; Pierguidi, L.; Floridi, A.; Mazzotta, G.; Floridi, A.; Gallai, V. Chemokine levels in the jugular venous blood of migraine without aura patients during attacks. Headache 2004, 44, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Duarte, H.; Teixeira, A.L.; Rocha, N.P.; Domingues, R.B. Increased interictal serum levels of CXCL8/IL-8 and CCL3/MIP-1α in migraine. Neurol. Sci. 2015, 36, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A.; Pitari, G.; Amenta, V.; Giuliano, F.; Gallina, M.; Costa, R.; Ferlito, S. Endothelial, haemostatic and haemorheological modifications in migraineurs. Artery 1996, 22, 93–100. [Google Scholar] [PubMed]
- Martelletti, P.; Stirparo, G.; Morrone, S.; Rinaldi, C.; Giacovazzo, M. Inhibition of intercellular adhesion molecule-1 (ICAM-1), soluble ICAM-1 and interleukin-4 by nitric oxide expression in migraine patients. J. Mol. Med. 1997, 75, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Kursun, O.; Yemisci, M.; van den Maagdenberg, A.M.J.M.; Karatas, H. Migraine and neuroinflammation: The inflammasome perspective. J. Headache Pain 2021, 22, 55. Available online: https://thejournalofheadacheandpain.biomedcentral.com/articles/10.1186/s10194-021-01271-1 (accessed on 26 September 2022). [CrossRef] [PubMed]
- Taheri, M.; Nicknafs, F.; Hesami, O.; Javadi, A.; Arsang-Jang, S.; Sayad, A.; Ghafouri-Fard, S. Differential expression of cytokine-coding genes among migraine patients with and without aura and normal subjects. J. Mol. Neurosci. 2021, 71, 1197–1204. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group n = 25 | Migraine Patients’ Group without Aura n = 12 | Migraine Patients’ Group with Aura n = 14 | p Value (Ordinary One-Way ANOVA) | |
|---|---|---|---|---|
| Age, years | 34.6 (1.3) | 39.7 (1.5) | 34.5 (2.3) | 0.08 |
| BMI, kg/m2 | 23.4 (0.6) | 23.2 (0.8) | 22.8 (1.0) | 0.72 |
| Systolic blood pressure, mm Hg | 112 (2) | 112 (3) | 108 (3) | 0.43 |
| Diastolic blood pressure, mm Hg | 78 (29) | 78 (3) | 77 (3) | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plinta, A.; Tretjakovs, P.; Svirskis, S.; Logina, I.; Gersone, G.; Jurka, A.; Mikelsone, I.; Blumfelds, L.; Mackevics, V.; Bahs, G. Association of Body Mass Index, Blood Pressure, and Interictal Serum Levels of Cytokines in Migraine with and without Aura. J. Clin. Med. 2022, 11, 5696. https://doi.org/10.3390/jcm11195696
Plinta A, Tretjakovs P, Svirskis S, Logina I, Gersone G, Jurka A, Mikelsone I, Blumfelds L, Mackevics V, Bahs G. Association of Body Mass Index, Blood Pressure, and Interictal Serum Levels of Cytokines in Migraine with and without Aura. Journal of Clinical Medicine. 2022; 11(19):5696. https://doi.org/10.3390/jcm11195696
Chicago/Turabian StylePlinta, Aelita, Peteris Tretjakovs, Simons Svirskis, Inara Logina, Gita Gersone, Antra Jurka, Indra Mikelsone, Leons Blumfelds, Vitolds Mackevics, and Guntis Bahs. 2022. "Association of Body Mass Index, Blood Pressure, and Interictal Serum Levels of Cytokines in Migraine with and without Aura" Journal of Clinical Medicine 11, no. 19: 5696. https://doi.org/10.3390/jcm11195696
APA StylePlinta, A., Tretjakovs, P., Svirskis, S., Logina, I., Gersone, G., Jurka, A., Mikelsone, I., Blumfelds, L., Mackevics, V., & Bahs, G. (2022). Association of Body Mass Index, Blood Pressure, and Interictal Serum Levels of Cytokines in Migraine with and without Aura. Journal of Clinical Medicine, 11(19), 5696. https://doi.org/10.3390/jcm11195696