
Neuromodulation Applied to Diseases: The Case of HRV Biofeedback


{kind=link}
Abstract
:1. Introduction
2. Heart Rate Variability—The Heart’s Eye to the Vagus
3. The Role of HRV in Health and Diseases
4. Activating the Vagal Nerve by Heart Rate Variability Biofeedback
5. Resonance Frequency Breathing
6. The Role of the Vagus Nerve and HRV-B in Diseases
7. Heart Diseases
8. Hypertension
9. Pain
10. Cancer
11. Diabetes
12. Cognitive Impairment and Dementia
13. Summary and Future Directions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Godin, P.J.; Buchman, T.G. Uncoupling of biological oscillators: A complementary hypothesis concerning the pathogenesis of multiple organ dysfunction syndrome. Crit. Care Med. 1996, 24, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Gidron, Y.; De Couck, M.; Reynders, T.; Marechal, R.; Engelborghs, S.; D’Hooghe, M. Stronger Correlations between Neurophysiological and Peripheral Disease Biomarkers Predict Better Prognosis in Two Severe Diseases. J. Clin. Med. 2019, 9, 26. [Google Scholar] [CrossRef] [Green Version]
- Kenney, M.J.; Ganta, C.K. Autonomic Nervous System and Immune System Interactions. Compr. Physiol. 2014, 4, 1177–1200. [Google Scholar] [CrossRef] [Green Version]
- Câmara, R.; Griessenauer, C.J. Anatomy of the vagus nerve. In Nerves and Nerve Injuries; Academic Press: Cambridge, MA, USA, 2015; pp. 385–397. [Google Scholar]
- Wink, J.; van Delft, R.; Notenboom, R.; Wouters, P.; DeRuiter, M.; Plevier, J.; Jongbloed, M. Human adult cardiac autonomic innervation: Controversies in anatomical knowledge and relevance for cardiac neuromodulation. Auton. Neurosci. 2020, 227, 102674. [Google Scholar] [CrossRef]
- Khan, I.; Bhardwaj, G.; Malla, N.; Wattal, C.; Agarwal, S. Effect of Serotonin on T Lymphocyte Proliferation in vitro in Healthy Individuals. Int. Arch. Allergy Immunol. 1986, 81, 378–380. [Google Scholar] [CrossRef]
- Madden, K.; Felten, D.L. Experimental basis for neural-immune interactions. Physiol. Rev. 1995, 75, 77–106. [Google Scholar] [CrossRef]
- Goehler, L.E.; Gaykema, R.P.; Hansen, M.K.; Anderson, K.; Maier, S.F.; Watkins, L.R. Vagal immune-to-brain communication: A visceral chemosensory pathway. Auton. Neurosci. 2000, 85, 49–59. [Google Scholar] [CrossRef]
- Tracey, K.J. Reflex control of immunity. Nat. Rev. Immunol. 2009, 9, 418–428. [Google Scholar] [CrossRef]
- Rosas-Ballina, M.; Olofsson, P.S.; Ochani, M.; Valdés-Ferrer, S.I.; Levine, Y.A.; Reardon, C.; Tusche, M.W.; Pavlov, V.A.; Andersson, U.; Chavan, S.; et al. Acetylcholine-Synthesizing T Cells Relay Neural Signals in a Vagus Nerve Circuit. Science 2011, 334, 98–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feliciano, L.; Henning, R.J. Vagal nerve stimulation releases vasoactive intestinal peptide which significantly increases coronary artery blood flow. Cardiovasc. Res. 1998, 40, 45–55. [Google Scholar] [CrossRef] [Green Version]
- Vaupel, P.; Mayer, A. Hypoxia in cancer: Significance and impact on clinical outcome. Cancer Metastasis Rev. 2007, 26, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P. How Does Heart Rate Variability Biofeedback Work? Resonance, the Baroreflex, and Other Mechanisms. Biofeedback 2013, 41, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Barthel, P.; Wensel, R.; Bauer, A.; Müller, A.; Wolf, P.; Ulm, K.; Huster, K.M.; Francis, D.P.; Malik, M.; Schmidt, G. Respiratory rate predicts outcome after acute myocardial infarction: A prospective cohort study. Eur. Heart J. 2012, 34, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar]
- Kuo, T.B.J.; Lai, C.J.; Huang, Y.-T.; Yang, C.C.H. Regression Analysis Between Heart Rate Variability and Baroreflex-Related Vagus Nerve Activity in Rats. J. Cardiovasc. Electrophysiol. 2005, 16, 864–869. [Google Scholar] [CrossRef]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research–recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar]
- Shaffer, F.; McCraty, R. Heart rate variability anatomy and physiology. Biofeedback 2013, 41, 13–25. [Google Scholar]
- Ackermann, S.; Laborde, S.; Borges, U.; Mosley, E. Commentary: Photoplethysmography for Quantitative Assessment of Sympathetic Nerve Activity (SNA) during Cold Stress. Front. Physiol. 2021, 12, 602745. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heathers, J.A.J. Sympathovagal balance from heart rate variability: An obituary. Exp. Physiol. 2012, 97, 556. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Bentho, O.; Park, M.-Y.; Sharabi, Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Rahman, F.; Pechnik, S.; Gross, D.; Sewell, L.; Goldstein, D.S. Low frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Clin. Auton. Res. 2011, 21, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- del Paso, G.A.R.; Langewitz, W.; Mulder, L.J.M.; Van Roon, A.; Duschek, S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: A review with emphasis on a reanalysis of previous studies. Psychophysiology 2013, 50, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Munoz, M.L.; van Roon, A.; Riese, H.; Thio, C.; Oostenbroek, E.; Westrik, I.; de Geus, E.J.C.; Gansevoort, R.; Lefrandt, J.; Nolte, I.M.; et al. Validity of (Ultra-)Short Recordings for Heart Rate Variability Measurements. PLoS ONE 2015, 10, e0138921. [Google Scholar] [CrossRef] [Green Version]
- Rautaharju, P.M.; Kooperberg, C.; Larson, J.C.; LaCroix, A. Electrocardiographic predictors of incident congestive heart failure and all-cause mortality in postmenopausal women: The Women’s Health Initiative. Circulation 2006, 113, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Dekker, J.M.; Schouten, E.G.; Klootwijk, P.; Pool, J.; Swenne, C.A.; Kromhout, D. Heart Rate Variability from Short Electrocardiographic Recordings Predicts Mortality from All Causes in Middle-aged and Elderly Men: The Zutphen Study. Am. J. Epidemiol. 1997, 145, 899–908. [Google Scholar] [CrossRef] [Green Version]
- De Couck, M.; Maréchal, R.; Moorthamers, S.; Van Laethem, J.-L.; Gidron, Y. Vagal nerve activity predicts overall survival in metastatic pancreatic cancer, mediated by inflammation. Cancer Epidemiol. 2016, 40, 47–51. [Google Scholar] [CrossRef]
- Weber, C.S.; Thayer, J.F.; Rudat, M.; Wirtz, P.H.; Zimmermann-Viehoff, F.; Thomas, A.; Perschel, F.H.; Arck, P.C.; Deter, H.C. Low vagal tone is associated with impaired post stress recovery of cardiovascular, endocrine, and immune markers. Eur. J. Appl. Physiol. 2010, 109, 201–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-G.; Cheon, E.-J.; Bai, D.-S.; Lee, Y.H.; Koo, B.-H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchaine, T.P.; Thayer, J.F. Heart rate variability as a transdiagnostic biomarker of psychopathology. Int. J. Psychophysiol. 2015, 98, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Frank, E.; Doyle, W.J.; Skoner, D.P.; Rabin, B.S.; Gwaltney, J.M., Jr. Types of stressors that increase susceptibility to the common cold in healthy adults. Health Psychol. 1998, 17, 214. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.A.; Sudlow, C.L.; Mishra, G.D. Psychological distress and risk of myocardial infarction and stroke in the 45 and up study: A prospective cohort study. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004500. [Google Scholar] [CrossRef] [Green Version]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart Rate Variability, Prefrontal Neural Function, and Cognitive Performance: The Neurovisceral Integration Perspective on Self-regulation, Adaptation, and Health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef]
- Thayer, J.F.; Åhs, F.; Fredrikson, M.; Sollers, J.J., III; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef]
- Otzenberger, H.; Gronfier, C.; Simon, C.; Charloux, A.; Ehrhart, J.; Piquard, F.; Brandenberger, G. Dynamic heart rate variability: A tool for exploring sympathovagal balance continuously during sleep in men. Am. J. Physiol. Circ. Physiol. 1998, 275, H946–H950. [Google Scholar] [CrossRef]
- Kleiger, R.E.; Stein, P.K.; Bigger, J.T., Jr. Heart rate variability: Measurement and clinical utility. Ann. Noninvasive Electrocardiol. 2005, 10, 88–101. [Google Scholar] [CrossRef]
- Penttilä, J.; Helminen, A.; Jartti, T.; Kuusela, T.; Huikuri, H.V.; Tulppo, M.; Coffeng, R.; Scheinin, H. Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clin. Physiol. 2001, 21, 365–376. [Google Scholar] [CrossRef]
- Berntson, G.G.; Lozano, D.L.; Chen, Y.-J. Filter properties of root mean square successive difference (RMSSD) for heart rate. Psychophysiology 2005, 42, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, H.; Venditti, F.J.; Manders, E.S.; Evans, J.C.; Larson, M.G.; Feldman, C.L.; Levy, D. Reduced heart rate variability and mortality risk in an elderly cohort. The Framingham Heart Study. Circulation 1994, 90, 878–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccelletti, E.; Gilardi, E.; Scaini, E.; Galiuto, L.; Persiani, R.; Biondi, A.; Basile, F.; Silveri, N.G. Heart rate variability and myocardial infarction: Systematic literature review and meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 299–307. [Google Scholar] [PubMed]
- De Couck, M.; Gidron, Y. Norms of vagal nerve activity, indexed by Heart Rate Variability, in cancer patients. Cancer Epidemiol. 2013, 37, 737–741. [Google Scholar] [CrossRef]
- Zhou, X.; Ma, Z.; Zhang, L.; Zhou, S.; Wang, J.; Wang, B.; Fu, W. Heart rate variability in the prediction of survival in patients with cancer: A systematic review and meta-analysis. J. Psychosom. Res. 2016, 89, 20–25. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Pikkujämsä, S.M.; Airaksinen, K.E.; Ikäheimo, M.J.; Rantala, A.O.; Kauma, H.; Lilja, M.; Kesäniemi, Y.A. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 1996, 94, 122–125. [Google Scholar] [CrossRef]
- Singh, J.P.; Larson, M.G.; Tsuji, H.; Evans, J.C.; O’Donnell, C.J.; Levy, D. Reduced heart rate variability and new-onset hypertension: Insights into pathogenesis of hypertension: The Framingham Heart Study. Hypertension 1998, 32, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Huston, J.M.; Tracey, K.J. The pulse of inflammation: Heart rate variability, the cholinergic anti-inflammatory pathway and implications for therapy. J. Intern. Med. 2011, 269, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Sajadieh, A.; Nielsen, O.W.; Rasmussen, V.; Hein, H.O.; Abedini, S.; Hansen, J.F. Increased heart rate and reduced heart-rate variability are associated with subclinical inflammation in middle-aged and elderly subjects with no apparent heart disease. Eur. Heart J. 2004, 25, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Benichou, T.; Pereira, B.; Mermillod, M.; Tauveron, I.; Pfabigan, D.; Maqdasy, S.; Dutheil, F. Heart rate variability in type 2 diabetes mellitus: A systematic review and meta–analysis. PLoS ONE 2018, 13, e0195166. [Google Scholar] [CrossRef] [Green Version]
- Gidron, Y.; Deschepper, R.; De Couck, M.; Thayer, J.F.; Velkeniers, B. The Vagus Nerve Can Predict and Possibly Modulate Non-Communicable Chronic Diseases: Introducing a Neuroimmunological Paradigm to Public Health. J. Clin. Med. 2018, 7, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Aeschbacher, S.; Schön, T.; Dörig, L.; Kreuzmann, R.; Neuhauser, C.; Schmidt-Trucksäss, A.; Probst-Hensch, N.M.; Risch, M.; Risch, L.; Conen, D. Heart rate, heart rate variability and inflammatory biomarkers among young and healthy adults. Ann. Med. 2016, 49, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.; Antelmi, I.; Pereira, A.C.; Latorre, M.D.R.D.; Grupi, C.J.; Krieger, J.E.; Mansur, A.J. Lower heart rate variability is associated with higher serum high-sensitivity C-reactive protein concentration in healthy individuals aged 46 years or more. Int. J. Cardiol. 2006, 107, 333–337. [Google Scholar] [CrossRef]
- Lampert, R.; Bremner, J.D.; Su, S.; Miller, A.; Lee, F.; Cheema, F.; Goldberg, J.; Vaccarino, V. Decreased heart rate variability is associated with higher levels of inflammation in middle-aged men. Am. Heart J. 2008, 156, 759.e1–759.e7. [Google Scholar] [CrossRef] [Green Version]
- Jarczok, M.N.; Koenig, J.; Mauss, D.; Fischer, J.E.; Thayer, J.F. Lower heart rate variability predicts increased level of C-reactive protein 4 years later in healthy, nonsmoking adults. J. Intern. Med. 2014, 276, 667–671. [Google Scholar] [CrossRef]
- Nunan, D.; Sandercock, G.R.H.; Brodie, D.A. A Quantitative Systematic Review of Normal Values for Short-Term Heart Rate Variability in Healthy Adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef]
- O’Neal, W.T.; Chen, L.Y.; Nazarian, S.; Soliman, E.Z. Reference ranges for short-term heart rate variability measures in individuals free of cardiovascular disease: The Multi-Ethnic Study of Atherosclerosis (MESA). J. Electrocardiol. 2016, 49, 686–690. [Google Scholar] [CrossRef] [Green Version]
- Berg, M.E.V.D.; Rijnbeek, P.R.; Niemeijer, M.N.; Hofman, A.; Van Herpen, G.; Bots, M.L.; Hillege, H.; Swenne, C.A.; Eijgelsheim, M.; Stricker, B.H.; et al. Normal Values of Corrected Heart-Rate Variability in 10-Second Electrocardiograms for All Ages. Front. Physiol. 2018, 9, 424. [Google Scholar] [CrossRef]
- Nussinovitch, U.; Elishkevitz, K.P.; Kaminer, K.; Nussinovitch, M.; Segev, S.; Volovitz, B.; Nussinovitch, N. The Efficiency of 10-Second Resting Heart Rate for the Evaluation of Short-Term Heart Rate Variability Indices. Pacing Clin. Electrophysiol. 2011, 34, 1498–1502. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Mechtler, L.L.; Kudrow, D.B.; Calhoun, A.H.; McClure, C.; Saper, J.R.; Liebler, E.J.; Engel, E.R.; Tepper, S.J. Non–Invasive Vagus Nerve Stimulation for the ACute Treatment of Cluster Headache: Findings from the Randomized, Double-Blind, Sham-Controlled ACT1 Study. Headache J. Head Face Pain 2016, 56, 1317–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silberstein, S.D.; Calhoun, A.H.; Lipton, R.B.; Grosberg, B.M.; Cady, R.K.; Dorlas, S.; Simmons, K.A.; Mullin, C.; Liebler, E.J.; Goadsby, P.J.; et al. Chronic migraine headache prevention with noninvasive vagus nerve stimulation: The EVENT study. Neurology 2016, 87, 529–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerman, I.; Hauger, R.; Sorkin, L.; Proudfoot, J.; Davis, B.; Huang, A.; Lam, K.; Simon, B.; Baker, D.G. Noninvasive Transcutaneous Vagus Nerve Stimulation Decreases Whole Blood Culture-Derived Cytokines and Chemokines: A Randomized, Blinded, Healthy Control Pilot Trial. Neuromodul. Technol. Neural Interface 2016, 19, 283–291. [Google Scholar] [CrossRef]
- Stavrakis, S.; Stoner, J.A.; Humphrey, M.B.; Morris, L.; Filiberti, A.; Reynolds, J.C.; Elkholey, K.; Javed, I.; Twidale, N.; Riha, P.; et al. TREAT AF (Transcutaneous Electrical Vagus Nerve Stimulation to Suppress Atrial Fibrillation) a randomized clinical trial. Clin. Electrophysiol. 2020, 6, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Wheat, A.L.; Larkin, K.T. Biofeedback of heart rate variability and related physiology: A critical review. Appl. Psychophysiol. Biofeedback 2010, 35, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P.; Vaschillo, B.; Zucker, T.; Graves, J.; Katsamanis, M.; Aviles, M.; Wamboldt, F. Protocol for Heart Rate Variability Biofeedback Training. Biofeedback 2013, 41, 98–109. [Google Scholar] [CrossRef] [Green Version]
- De Couck, M.; Caers, R.; Musch, L.; Fliegauf, J.; Giangreco, A.; Gidron, Y. How breathing can help you make better decisions: Two studies on the effects of breathing patterns on heart rate variability and decision-making in business cases. Int. J. Psychophysiol. 2019, 139, 1–9. [Google Scholar] [CrossRef]
- Hamasaki, H. Effects of Diaphragmatic Breathing on Health: A Narrative Review. Medicines 2020, 7, 65. [Google Scholar] [CrossRef]
- Ley, R. Blood, breath, and fears: A hyperventilation theory of panic attacks and agoraphobia. Clin. Psychol. Rev. 1985, 5, 271–285. [Google Scholar] [CrossRef]
- Tavel, M.E. Hyperventilation Syndrome: Why Is It Regularly Overlooked? Am. J. Med. 2020, 134, 13–15. [Google Scholar] [CrossRef]
- Laborde, S.; Allen, M.; Borges, U.; Dosseville, F.; Hosang, T.; Iskra, M.; Mosley, E.; Salvotti, C.; Spolverato, L.; Zammit, N.; et al. Effects of voluntary slow breathing on heart rate and heart rate variability: A systematic review and a meta-analysis. Neurosci. Biobehav. Rev. 2022, 138, 104711. [Google Scholar] [CrossRef] [PubMed]
- Kiecolt-Glaser, J.K.; Glaser, R.; Williger, D.; Stout, J.; Messick, G.; Sheppard, S.; Ricker, D.; Romisher, S.C.; Briner, W.; Bonnell, G. Psychosocial enhancement of immunocompetence in a geriatric population. Health Psychol. 1985, 4, 25. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, J.; Sauerland, M.; Wieland, R. Relaxation-induced cortisol changes within lunch breaks—An experimental longitudinal worksite field study. J. Occup. Organ. Psychol. 2011, 84, 382–394. [Google Scholar] [CrossRef]
- Pawlow, L.A.; Jones, G.E. The impact of abbreviated progressive muscle relaxation on salivary cortisol. Biol. Psychol. 2002, 60, 1–16. [Google Scholar] [CrossRef]
- Pawlow, L.A.; Jones, G.E. The Impact of Abbreviated Progressive Muscle Relaxation on Salivary Cortisol and Salivary Immunoglobulin A (sIgA). Appl. Psychophysiol. Biofeedback 2005, 30, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Vaschillo, E.G.; Vaschillo, B.; Lehrer, P.M. Characteristics of Resonance in Heart Rate Variability Stimulated by Biofeedback. Appl. Psychophysiol. Biofeedback 2006, 31, 129–142. [Google Scholar] [CrossRef]
- Karavaev, A.S.; Kiselev, A.; Gridnev, V.; Borovkova, E.I.; Prokhorov, M.D.; Posnenkova, O.M.; Ponomarenko, V.; Bezruchko, B.P.; Shvartz, V. Phase and frequency locking of 0.1-Hz oscillations in heart rate and baroreflex control of blood pressure by breathing of linearly varying frequency as determined in healthy subjects. Hum. Physiol. 2013, 39, 416–425. [Google Scholar] [CrossRef]
- Vaschillo, E.; Lehrer, P.; Rishe, N.; Konstantinov, M. Heart Rate Variability Biofeedback as a Method for Assessing Baroreflex Function: A Preliminary Study of Resonance in the Cardiovascular System. Appl. Psychophysiol. Biofeedback 2002, 27, 1–27. [Google Scholar] [CrossRef]
- Vaschillo, E.; Vaschillo, B.; Lehrer, P. Heartbeat Synchronizes with Respiratory Rhythm Only Under Specific Circumstances. Chest 2004, 126, 1385–1386. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Gevirtz, R. Heart rate variability biofeedback: How and why does it work? Front. Psychol. 2014, 5, 756. [Google Scholar] [CrossRef] [Green Version]
- Lehrer, P.M.; Vaschillo, E.; Vaschillo, B.; Lu, S.-E.; Scardella, A.; Siddique, M.; Habib, R.H. Biofeedback Treatment for Asthma. Chest 2004, 126, 352–361. [Google Scholar] [CrossRef] [Green Version]
- de Boer, R.W.; Karemaker, J.M.; Strackee, J. Hemodynamic fluctuations and baroreflex sensitivity in humans: A beat-to-beat model. Am. J. Physiol. Circ. Physiol. 1987, 253, H680–H689. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Gabutti, A.; Porta, C.; Spicuzza, L. Slow breathing reduces chemoreflex response to hypoxia and hypercapnia, and increases baroreflex sensitivity. J. Hypertens. 2001, 19, 2221–2229. [Google Scholar] [CrossRef] [PubMed]
- Yasuma, F.; Hayano, J.I. Respiratory sinus arrhythmia: Why does the heartbeat synchronize with respiratory rhythm? Chest 2004, 125, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Gevirtz, R. The nerve of that disease: The vagus nerve and cardiac rehabilitation. Biofeedback 2013, 41, 32. [Google Scholar] [CrossRef]
- Tracey, K.J. Physiology and immunology of the cholinergic anti-inflammatory pathway. J. Clin. Investig. 2007, 117, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Purcell, E.; Shaffer, F.; Urlakis, M. Brief resonance frequency training can reduce C-reactive protein. History of HRV Research 96 Fall 2013. Biofeedback levels in normals [Abstract]. Presented at the Meeting of the Association for Applied Psychophysiology and Biofeedback, New Orleans, LA, USA, 9–12 March 2011. [Google Scholar]
- Goessl, V.C.; Curtiss, J.E.; Hofmann, S.G. The effect of heart rate variability biofeedback training on stress and anxiety: A meta-analysis. Psychol. Med. 2017, 47, 2578–2586. [Google Scholar] [CrossRef]
- Lehrer, P.; Kaur, K.; Sharma, A.; Shah, K.; Huseby, R.; Bhavsar, J.; Sgobba, P.; Zhang, Y. Heart Rate Variability Biofeedback Improves Emotional and Physical Health and Performance: A Systematic Review and Meta Analysis. Appl. Psychophysiol. Biofeedback 2020, 45, 109–129. [Google Scholar] [CrossRef]
- Pizzoli, S.F.M.; Marzorati, C.; Gatti, D.; Monzani, D.; Mazzocco, K.; Pravettoni, G. A meta-analysis on heart rate variability biofeedback and depressive symptoms. Sci. Rep. 2021, 11, 6650. [Google Scholar] [CrossRef]
- Fournié, C.; Chouchou, F.; Dalleau, G.; Caderby, T.; Cabrera, Q.; Verkindt, C. Heart rate variability biofeedback in chronic disease management: A systematic review. Complement. Ther. Med. 2021, 60, 102750. [Google Scholar] [CrossRef]
- Imperiale, T.; McCullough, A.J. Do Corticosteroids Reduce Mortality from Alcoholic Hepatitis? Ann. Intern. Med. 1990, 113, 299–307. [Google Scholar] [CrossRef]
- Brinza, C.; Floria, M.; Covic, A.; Covic, A.; Scripcariu, D.-V.; Burlacu, A. The Usefulness of Assessing Heart Rate Variability in Patients with Acute Myocardial Infarction (HeaRt-V-AMI). Sensors 2022, 22, 3571. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. Atherosclerosis is an inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Farahi, L.; Sinha, S.K.; Lusis, A.J. Roles of Macrophages in Atherogenesis. Front. Pharmacol. 2021, 12, 785220. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, S.; Gotoh, T.; Tomisato, W.; Mima, S.; Hoshino, T.; Hwang, H.-J.; Takenaka, H.; Tsuchiya, T.; Mori, M.; Mizushima, T. Endoplasmic reticulum stress response is involved in nonsteroidal anti-inflammatory drug-induced apoptosis. Cell Death Differ. 2004, 11, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Lin, I.-M.; Fan, S.-Y.; Lu, H.-C.; Lin, T.-H.; Chu, C.-S.; Kuo, H.-F.; Lee, C.-S.; Lu, Y.-H. Randomized controlled trial of heart rate variability biofeedback in cardiac autonomic and hostility among patients with coronary artery disease. Behav. Res. Ther. 2015, 70, 38–46. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. The Association of Anger and Hostility with Future Coronary Heart Disease: A Meta-Analytic Review of Prospective Evidence. J. Am. Coll. Cardiol. 2009, 53, 936–946. [Google Scholar] [CrossRef]
- Climov, D.; Lysy, C.; Berteau, S.; Dutrannois, J.; Dereppe, H.; Brohet, C.; Melin, J. Biofeedback on heart rate variability in cardiac rehabilitation: Practical feasibility and psycho-physiological effects. Acta Cardiol. 2014, 69, 299–307. [Google Scholar] [CrossRef]
- Limmer, A.; Laser, M.; Schütz, A. Mobile Heart Rate Variability Biofeedback as a Complementary Intervention After Myocardial Infarction: A Randomized Controlled Study. Int. J. Behav. Med. 2021, 29, 230–239. [Google Scholar] [CrossRef]
- Yu, L.-C.; Lin, I.-M.; Fan, S.-Y.; Chien, C.-L.; Lin, T.-H. One-Year Cardiovascular Prognosis of the Randomized, Controlled, Short-Term Heart Rate Variability Biofeedback Among Patients with Coronary Artery Disease. Int. J. Behav. Med. 2018, 25, 271–282. [Google Scholar] [CrossRef]
- Nolan, R.P.; Floras, J.S.; Harvey, P.J.; Kamath, M.V.; Picton, P.E.; Chessex, C.; Hiscock, N.; Powell, J.; Catt, M.; Hendrickx, H.; et al. Behavioral neurocardiac training in hypertension: A randomized, controlled trial. Hypertension 2010, 55, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, E.B. Determinants of the Longitudinal Change in Heart Rate Variability: The Atherosclerosis Risk in Communities Study; The University of North Carolina at Chapel Hill: Chapel Hill, NC, USA, 2013. [Google Scholar]
- Lin, G.; Xiang, Q.; Fu, X.; Wang, S.; Wang, S.; Chen, S.; Shao, L.; Zhao, Y.; Wang, T. Heart Rate Variability Biofeedback Decreases Blood Pressure in Prehypertensive Subjects by Improving Autonomic Function and Baroreflex. J. Altern. Complement. Med. 2012, 18, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Rau, H.; Bührer, M.; Weitkunat, R. Biofeedback of R-Wave-to-Pulse Interval Normalizes Blood Pressure. Appl. Psychophysiol. Biofeedback 2003, 28, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.; Fink, B.; Dao, T.K.; Hebert, R.; Farmer, L.S.; Sanders, A.; Pastorek, N.; Gevirtz, R. Associations among Pain, PTSD, mTBI, and Heart Rate Variability in Veterans of Operation Enduring and Iraqi Freedom: A Pilot Study. Pain Med. 2009, 10, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caton, L.; Bolzon, M.; Boschiero, D.; Thayer, J.F.; Gidron, Y. Pre-surgical heart-rate variability strongly predicts less post-operative pain in patients with epilepsy. J. Psychosom. Res. 2021, 145, 110421. [Google Scholar] [CrossRef]
- Hendrix, J.; Nijs, J.; Ickmans, K.; Godderis, L.; Ghosh, M.; Polli, A. The Interplay between Oxidative Stress, Exercise, and Pain in Health and Disease: Potential Role of Autonomic Regulation and Epigenetic Mechanisms. Antioxidants 2020, 9, 1166. [Google Scholar] [CrossRef] [PubMed]
- Watkins, L.R.; Maier, S.F. Beyond Neurons: Evidence That Immune and Glial Cells Contribute to Pathological Pain States. Physiol. Rev. 2002, 82, 981–1011. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Neumann, L.; Alhosshle, A.; Kotler, M.; Abu-Shakra, M.; Buskila, D. Abnormal sympathovagal balance in men with fibromyalgia. J. Rheumatol. 2001, 28, 581–589. [Google Scholar]
- De Couck, M.; Nijs, J.; Gidron, Y. You may need a nerve to treat pain: The neurobiological rationale for vagal nerve activation in pain management. Clin. J. Pain 2014, 30, 1099–1105. [Google Scholar] [CrossRef]
- Berry, M.E.; Chapple, I.T.; Ginsberg, J.P.; Gleichauf, K.J.; Meyer, J.A.; Nagpal, M.L. Non-pharmacological Intervention for Chronic Pain in Veterans: A Pilot Study of Heart Rate Variability Biofeedback. Glob. Adv. Health Med. 2014, 3, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Hallman, D.M.; Olsson, E.M.; Von Schéele, B.; Melin, L.; Lyskov, E. Effects of heart rate variability biofeedback in subjects with stress-related chronic neck pain: A pilot study. Appl. Psychophysiol. Biofeedback 2011, 36, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Yetwin, A.K.; Mahrer, N.E.; Bell, T.S.; Gold, J.I. Heart Rate Variability biofeedback therapy for children and adolescents with chronic pain: A pilot study. J. Pediatr. Nurs. 2022, 66, 151–159. [Google Scholar] [CrossRef] [PubMed]
- De Couck, M.; Caers, R. Why we Should Stimulate the Vagus Nerve in Cancer. Clin. Oncol. 2018, 3, 1515. [Google Scholar]
- Kloter, E.; Barrueto, K.; Klein, S.D.; Scholkmann, F.; Wolf, U. Heart Rate Variability as a Prognostic Factor for Cancer Survival—A Systematic Review. Front. Physiol. 2018, 9, 623. [Google Scholar] [CrossRef] [Green Version]
- Øvrevik, J.; Refsnes, M.; Låg, M.; Brinchmann, B.C.; Schwarze, P.E.; Holme, J.A. Triggering Mechanisms and Inflammatory Effects of Combustion Exhaust Particles with Implication for Carcinogenesis. Basic Clin. Pharmacol. Toxicol. 2016, 121, 55–62. [Google Scholar] [CrossRef]
- Entschladen, F.; Drell, T.L.T.; Lang, K.; Joseph, J.; Zaenker, K.S. Tumour-cell migration, invasion, and metastasis: Navigation by neurotransmitters. Lancet Oncol. 2004, 5, 254–258. [Google Scholar] [CrossRef]
- Muz, B.; de la Puente, P.; Azab, F.; Azab, A.K. The role of hypoxia in cancer progression, angiogenesis, metastasis, and resistance to therapy. Hypoxia 2015, 3, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Bruni, D.; Angell, H.K.; Galon, J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat. Cancer 2020, 20, 662–680. [Google Scholar] [CrossRef]
- Tsutsumi, T.; Ide, T.; Yamato, M.; Kudou, W.; Andou, M.; Hirooka, Y.; Utsumi, H.; Tsutsui, H.; Sunagawa, K. Modulation of the myocardial redox state by vagal nerve stimulation after experimental myocardial infarction. Cardiovasc. Res. 2007, 77, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Saku, K.; Kishi, T.; Sakamoto, K.; Hosokawa, K.; Sakamoto, T.; Murayama, Y.; Kakino, T.; Ikeda, M.; Ide, T.; Sunagawa, K. Afferent vagal nerve stimulation resets baroreflex neural arc and inhibits sympathetic nerve activity. Physiol. Rep. 2014, 2, e12136. [Google Scholar] [CrossRef]
- A Nandiwada, P.; Hyman, A.L.; Kadowitz, P.J. Pulmonary vasodilator responses to vagal stimulation and acetylcholine in the cat. Circ. Res. 1983, 53, 86–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihaylova, S.; Schweighöfer, H.; Hackstein, H.; Rosengarten, B. Effects of anti-inflammatory vagus nerve stimulation in endotoxemic rats on blood and spleen lymphocyte subsets. Agents Actions 2014, 63, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Gidron, Y.; Perry, H.; Glennie, M. Does the vagus nerve inform the brain about preclinical tumours and modulate them? Lancet Oncol. 2005, 6, 245–248. [Google Scholar] [CrossRef]
- De Couck, M.; Mravec, B.; Gidron, Y. You may need the vagus nerve to understand pathophysiology and to treat diseases. Clin. Sci. 2011, 122, 323–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Rourke, M.A.; Franco, R.A.; Sofge, J.; Ginsberg, J.; Susko, K.; Crowley, E.; Anderson, A.; Christ, A.; Hanna, J.; Hendry, W.; et al. Use of heart rate variability (HRV) biofeedback for symptom management among cancer survivors. J. Clin. Oncol. 2017, 35, 10099. [Google Scholar] [CrossRef]
- Burch, J.B.; Ginsberg, J.P.; McLain, A.C.; Franco, R.; Stokes, S.; Susko, K.; Hendry, W.; Crowley, E.; Christ, A.; Hanna, J.; et al. Symptom Management Among Cancer Survivors: Randomized Pilot Intervention Trial of Heart Rate Variability Biofeedback. Appl. Psychophysiol. Biofeedback 2020, 45, 99–108. [Google Scholar] [CrossRef]
- Hasuo, H.; Kanbara, K.; Shizuma, H.; Morita, Y.; Fukunaga, M. Short-term efficacy of home-based heart rate variability biofeedback on sleep disturbance in patients with incurable cancer: A randomised open-label study. BMJ Support. Palliat. Care 2020, 21. [Google Scholar] [CrossRef]
- Fournié, C.; Verkindt, C.; Dalleau, G.; Bouscaren, N.; Mohr, C.; Zunic, P.; Cabrera, Q. Rehabilitation program combining physical exercise and heart rate variability biofeedback in hematologic patients: A feasibility study. Support. Care Cancer 2021, 30, 2009–2016. [Google Scholar] [CrossRef]
- Ozier, D.; Linden, W. Heart Variability Biofeedback as Supplementary Care for Brain Cancer: A Feasibility Study. J. Altern. Complement. Med. 2018, 24, 852–853. [Google Scholar] [CrossRef]
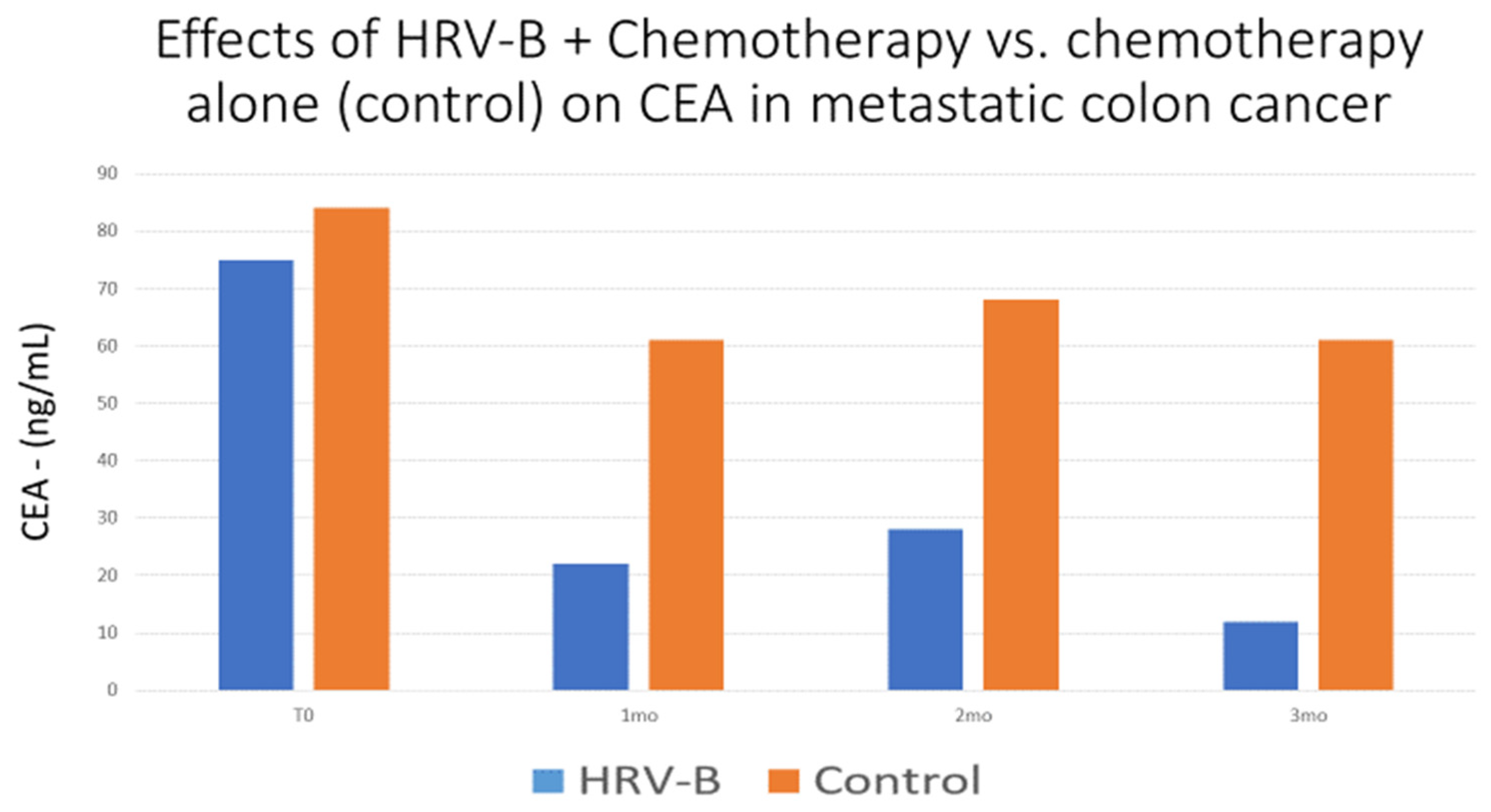
- Gidron, Y.; De Couck, M.; De Leeuw, I.; Blase, K.; Vanacker, L. The effects of heart-rate variability biofeedback on levels of the tumor marker CEA in metastatic colon cancer: A pilot controlled study. Psychosom. Med. 2017, 79, A18. [Google Scholar]
- Boer-Martins, L.; Figueiredo, V.N.; Demacq, C.; Martins, L.C.; Consolin-Colombo, F.; Figueiredo, M.J.; Cannavan, F.P.; Moreno, H. Relationship of autonomic imbalance and circadian disruption with obesity and type 2 diabetes in resistant hypertensive patients. Cardiovasc. Diabetol. 2011, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehman, K.; Akash, M.S.H. Mechanisms of inflammatory responses and development of insulin resistance: How are they interlinked? J. Biomed. Sci. 2016, 23, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Druschky, K.; Druschky, A. Mobile biofeedback of heart rate variability in patients with diabetic polyneuropathy: A preliminary study. Clin. Physiol. Funct. Imaging 2014, 35, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Munster-Segev, M.; Fuerst, O.; Kaplan, S.A.; Cahn, A. Incorporation of a Stress Reducing Mobile App in the Care of Patients with Type 2 Diabetes: A Prospective Study. JMIR mHealth uHealth 2017, 5, e75. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, V.P.; Ramalho Oliveira, B.R.; Tavares Mello, R.G.; Moraes, H.; Deslandes, A.C.; Laks, J. Heart Rate Variability Indexes in Dementia: A Systematic Review with a Quantitative Analysis. Curr. Alzheimer Res. 2018, 15, 80–88. [Google Scholar] [CrossRef]
- Rubio-Perez, J.M.; Morillas-Ruiz, J.M. A review: Inflammatory process in Alzheimer’s disease, role of cytokines. Sci. World J. 2012, 2012, 756357. [Google Scholar] [CrossRef]
- Hotta, H.; Uchida, S. Aging of the autonomic nervous system and possible improvements in autonomic activity using somatic afferent stimulation. Geriatr. Gerontol. Int. 2010, 10, S127–S136. [Google Scholar] [CrossRef]
- Dalise, A.M.; Prestano, R.; Fasano, R.; Gambardella, A.; Barbieri, M.; Rizzo, M.R. Autonomic Nervous System and Cognitive Impairment in Older Patients: Evidence from Long-Term Heart Rate Variability in Real-Life Setting. Front. Aging Neurosci. 2020, 12, 40. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarino, A.; Forte, G.; Giovannoli, J.; Casagrande, M. Executive functions in the elderly with mild cognitive impairment: A systematic review on motor and cognitive inhibition, conflict control and cognitive flexibility. Aging Ment. Health 2019, 24, 1028–1045. [Google Scholar] [CrossRef] [PubMed]
- de Vilhena Toledo, M.A.; Junqueira, L.F., Jr. Cardiac sympathovagal modulation evaluated by short-term heart interval variability is subtly impaired in Alzheimer’s disease. Geriatr. Gerontol. Int. 2008, 8, 109–118. [Google Scholar] [CrossRef]
- Algotsson, A.; Viitanen, M.; Winblad, B.; Solders, G. Autonomic dysfunction in Alzheimer’s disease. Acta Neurol. Scand. 1995, 91, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Struhal, W.; Mahringer, C.; Lahrmann, H.; Mörtl, C.; Buhl, P.; Huemer, M.; Ransmayr, G. Heart Rate Spectra Confirm the Presence of Autonomic Dysfunction in Dementia Patients. J. Alzheimer’s Dis. 2016, 54, 657–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zulli, R.; Nicosia, F.; Borroni, B.; Agosti, C.; Prometti, P.; Donati, P.; de Vecchi, M.; Romanelli, G.; Grassi, V.; Padovani, A. QT dispersion and heart rate variability abnormalities in Alzheimer’s disease and in mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 2135–2139. [Google Scholar] [CrossRef] [PubMed]
- Tinello, D.; Kliegel, M.; Zuber, S. Does Heart Rate Variability Biofeedback Enhance Executive Functions Across the Lifespan? A Systematic Review. J. Cogn. Enhanc. 2021, 6, 126–142. [Google Scholar] [CrossRef] [PubMed]
- Jester, D.J.; Rozek, E.K.; McKelley, R.A. Heart rate variability biofeedback: Implications for cognitive and psychiatric effects in older adults. Aging Ment. Health 2018, 23, 574–580. [Google Scholar] [CrossRef]
- Barbul, A. Immune Aspects of Wound Repair. Clin. Plast. Surg. 1990, 17, 433–442. [Google Scholar] [CrossRef]
- Pavlov, V.A.; Wang, H.; Czura, C.J.; Friedman, S.G.; Tracey, K.J. The Cholinergic Anti-inflammatory Pathway: A Missing Link in Neuroimmunomodulation. Mol. Med. 2003, 9, 125–134. [Google Scholar] [CrossRef]
- Gitler, A. Does Pre-Operative Vagal Activity Predict Clinical Outcomes after Total Knee Replacement? Master’s Thesis, University of Haifa, Haifa, Israel, 2021. Available online: https://haifa.alma.exlibrisgroup.com/discovery/delivery/972HAI_MAIN:AlmaGeneralView/12258677330002791 (accessed on 1 January 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gitler, A.; Vanacker, L.; De Couck, M.; De Leeuw, I.; Gidron, Y. Neuromodulation Applied to Diseases: The Case of HRV Biofeedback. J. Clin. Med. 2022, 11, 5927. https://doi.org/10.3390/jcm11195927
Gitler A, Vanacker L, De Couck M, De Leeuw I, Gidron Y. Neuromodulation Applied to Diseases: The Case of HRV Biofeedback. Journal of Clinical Medicine. 2022; 11(19):5927. https://doi.org/10.3390/jcm11195927
Chicago/Turabian StyleGitler, Asaf, Leen Vanacker, Marijke De Couck, Inge De Leeuw, and Yoram Gidron. 2022. "Neuromodulation Applied to Diseases: The Case of HRV Biofeedback" Journal of Clinical Medicine 11, no. 19: 5927. https://doi.org/10.3390/jcm11195927
APA StyleGitler, A., Vanacker, L., De Couck, M., De Leeuw, I., & Gidron, Y. (2022). Neuromodulation Applied to Diseases: The Case of HRV Biofeedback. Journal of Clinical Medicine, 11(19), 5927. https://doi.org/10.3390/jcm11195927