
Association of Visual Impairment with Psychological Distress in Older Adults: A Survey of 105,092 Older People in Taiwan


Abstract
:1. Introduction
2. Participants and Methods
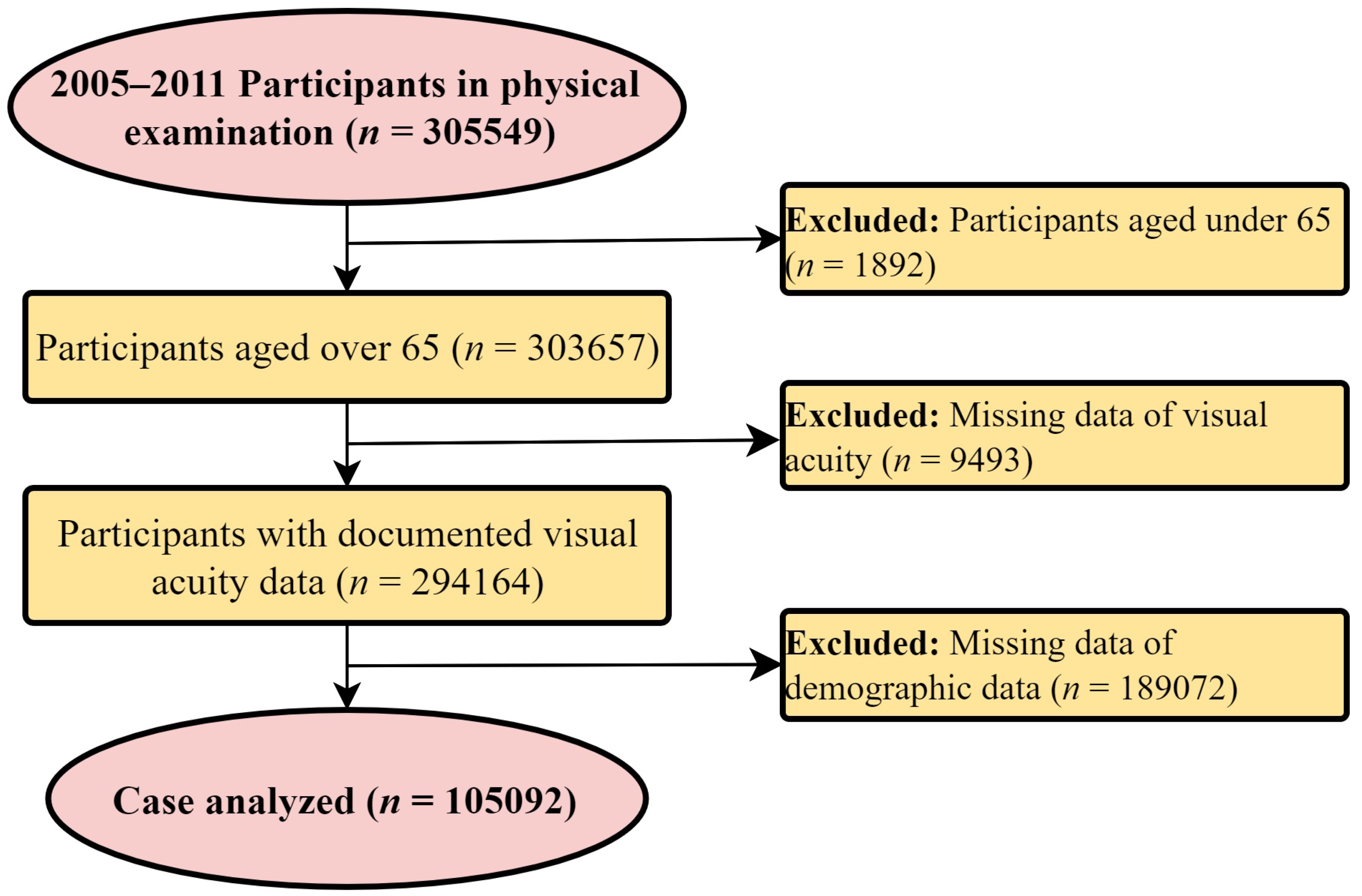
2.1. Study Population
2.2. Materials and Variable Definitions
2.3. Statistical Analysis
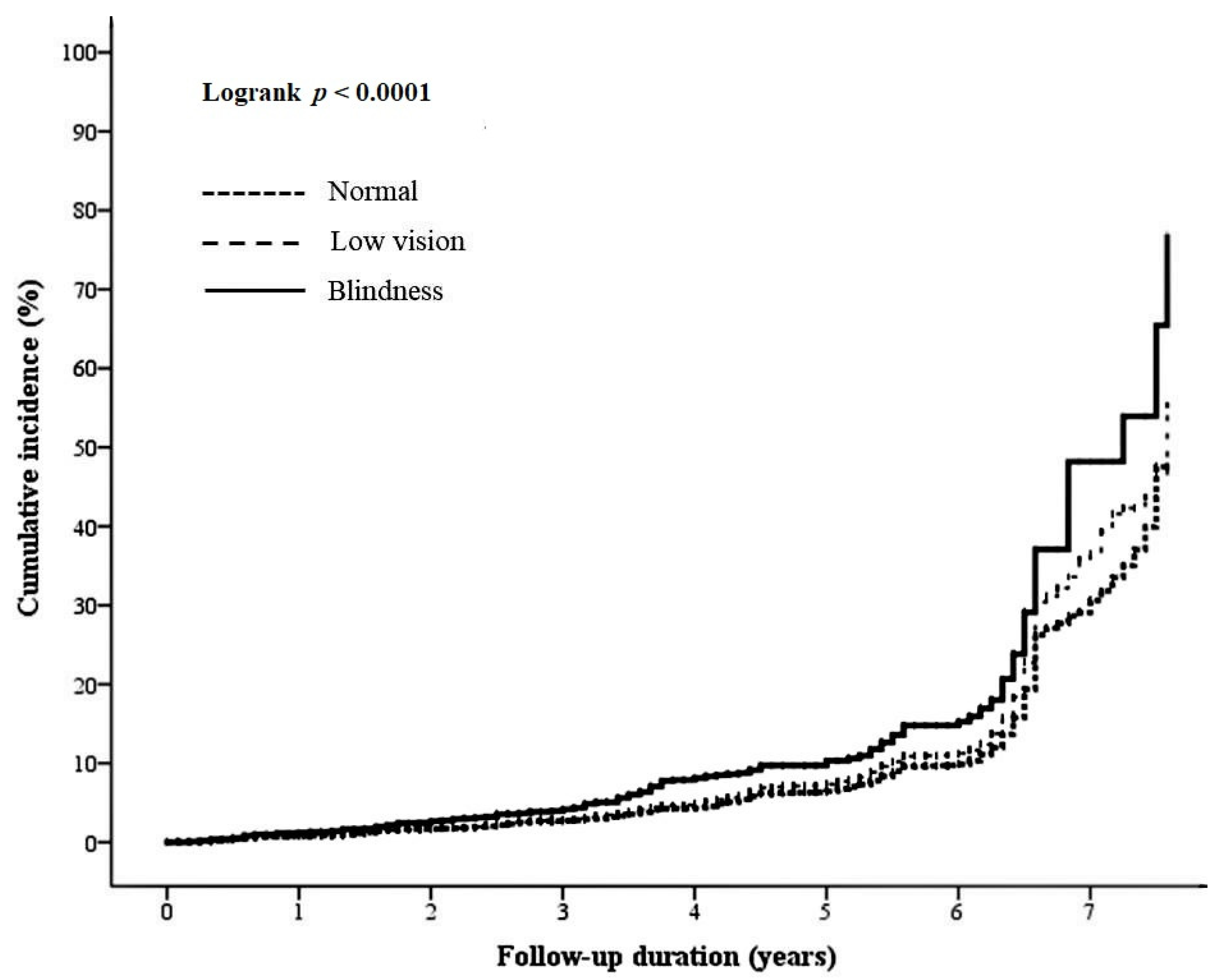
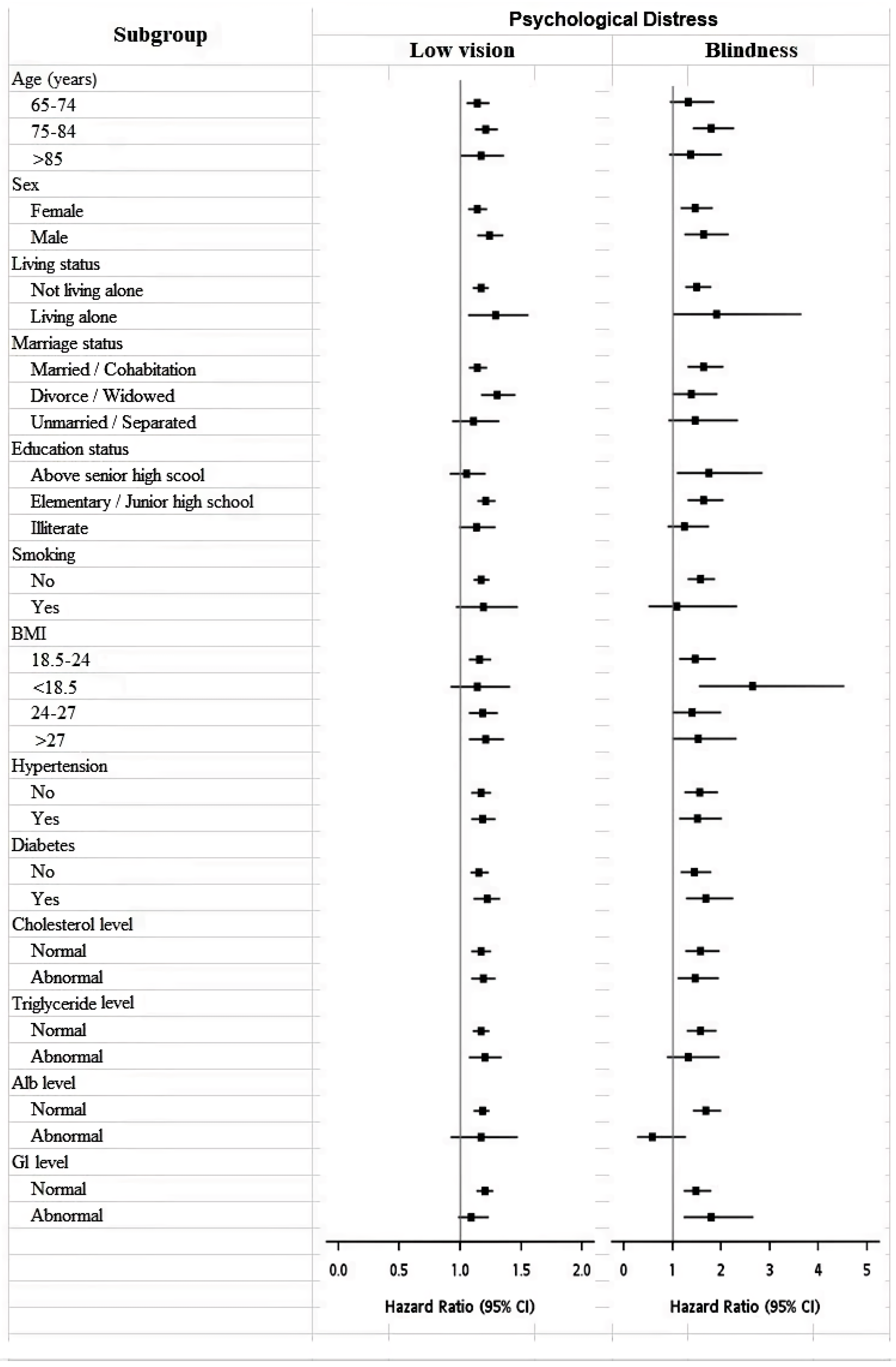
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017.
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Russ, T.C.; Stamatakis, E.; Hamer, M.; Starr, J.M.; Kivimäki, M.; Batty, G.D. Association between psychological distress and mortality: Individual participant pooled analysis of 10 prospective cohort studies. BMJ 2012, 345, e4933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picco, L.; Subramaniam, M.; Abdin, E.; Vaingankar, J.A.; Chong, S.A. Prevalence and correlates of heart disease among adults in Singapore. Asian J. Psychiatry 2016, 19, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.; Friedman, D.S.; Bradley, C.; Massof, R. Estimates of Incidence and Prevalence of Visual Impairment, Low Vision, and Blindness in the United States. JAMA Ophthalmol. 2018, 136, 12–19. [Google Scholar] [CrossRef]
- Wang, W.L.; Chen, N.; Sheu, M.M.; Wang, J.H.; Hsu, W.L.; Hu, Y.J. The prevalence and risk factors of visual impairment among the elderly in Eastern Taiwan. Kaohsiung J. Med. Sci. 2016, 32, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Kuang, T.M.; Tsai, S.Y.; Hsu, W.M.; Cheng, C.Y.; Liu, J.H.; Chou, P. Correctable visual impairment in an elderly Chinese population in Taiwan: The Shihpai Eye Study. Investig. Ophthalmol. Vis. Sci. 2007, 48, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Evans, B.J.; Rowlands, G. Correctable visual impairment in older people: A major unmet need. Ophthalmic Physiol. Opt. 2004, 24, 161–180. [Google Scholar] [CrossRef]
- Reidy, A.; Minassian, D.C.; Vafidis, G.; Joseph, J.; Farrow, S.; Wu, J.; Desai, P.; Connolly, A. Prevalence of serious eye disease and visual impairment in a north London population: Population based, cross sectional study. BMJ 1998, 316, 1643–1646. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, J.R.; Ramke, J.; Macleod, D.; Burn, H.; Lee, C.N.; Zhang, J.H.; Waldock, W.; Swenor, B.K.; Gordon, I.; Congdon, N.; et al. Association between vision impairment and mortality: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e418–e430. [Google Scholar] [CrossRef]
- Zhang, T.; Jiang, W.; Song, X.; Zhang, D. The association between visual impairment and the risk of mortality: A meta-analysis of prospective studies. J. Epidemiol. Community Health 2016, 70, 836–842. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice. Making Eye Health a Population Health Imperative: Vision for Tomorrow; Welp, A., Woodbury, R.B., McCoy, M.A., Teutsch, S.M., Eds.; National Academies Press (US): Washington, DC, USA, 2016. [Google Scholar]
- Lundeen, E.A.; Saydah, S.; Ehrlich, J.R.; Saaddine, J. Self-Reported Vision Impairment and Psychological Distress in U.S. Adults. Ophthalmic Epidemiol. 2021, 1–11, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, H.P.; Comijs, H.C.; Penninx, B.W.; van Rens, G.H.; van Nispen, R.M. Major depressive and anxiety disorders in visually impaired older adults. Investig. Ophthalmol. Vis. Sci. 2015, 56, 849–854. [Google Scholar] [CrossRef] [Green Version]
- Jones, G.C.; Crews, J.E.; Danielson, M.L. Health risk profile for older adults with blindness: An application of the International Classification of Functioning, Disability, and Health framework. Ophthalmic Epidemiol. 2010, 17, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Cimarolli, V.R.; Casten, R.J.; Rovner, B.W.; Heyl, V.; Sörensen, S.; Horowitz, A. Anxiety and depression in patients with advanced macular degeneration: Current perspectives. Clin. Ophthalmol. 2015, 10, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, J.R.; Fletcher, A.E.; Wormald, R.P. Depression and anxiety in visually impaired older people. Ophthalmology 2007, 114, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.L.; Barrett, A.E. Visual impairment and quality of life among older adults: An examination of explanations for the relationship. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 364–373. [Google Scholar] [CrossRef] [Green Version]
- Cosh, S.; Carriere, I.; Nael, V.; Tzourio, C.; Delcourt, C.; Helmer, C.; Sense-Cog Consortium. The association of vision loss and dimensions of depression over 12 years in older adults: Findings from the Three City study. J. Affect. Disord. 2019, 243, 477–484. [Google Scholar] [CrossRef]
- Blindness and Vision Impairment; World Health Organization: Geneva, Switzerland, 2018.
- Chen, H.C.; Wu, C.H.; Lee, Y.J.; Liao, S.C.; Lee, M.B. Validity of the five-item Brief Symptom Rating Scale among subjects admitted for general health screening. J. Formos. Med. Assoc. 2005, 104, 824–829. [Google Scholar]
- Lee, M.B.; Liao, S.C.; Lee, Y.J.; Wu, C.H.; Tseng, M.C.; Gau, S.F.; Rau, C.L. Development and verification of validity and reliability of a short screening instrument to identify psychiatric morbidity. J. Formos. Med. Assoc. 2003, 102, 687–694. [Google Scholar]
- Ong, S.R.; Crowston, J.G.; Loprinzi, P.D.; Ramulu, P.Y. Physical activity, visual impairment, and eye disease. Eye 2018, 32, 1296–1303. [Google Scholar] [CrossRef] [Green Version]
- Atkins, J.; Naismith, S.L.; Luscombe, G.M.; Hickie, I.B. Psychological distress and quality of life in older persons: Relative contributions of fixed and modifiable risk factors. BMC Psychiatry 2013, 13, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whillans, J.; Nazroo, J. Social Inequality and Visual Impairment in Older People. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, 532–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa, A.; Rudenstine, S. The contribution of financial well-being, social support, and trait emotional intelligence on psychological distress. Br. J. Clin. Psychol. 2020, 59, 224–240. [Google Scholar] [CrossRef]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K.L. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, D.D.; Swenor, B.K.; Christ, S.L.; West, S.K.; Lam, B.L.; Lee, D.J. Longitudinal Associations Between Visual Impairment and Cognitive Functioning: The Salisbury Eye Evaluation Study. JAMA Ophthalmol. 2018, 136, 989–995. [Google Scholar] [CrossRef] [Green Version]
- Ismail, Z.; Elbayoumi, H.; Fischer, C.E.; Hogan, D.B.; Millikin, C.P.; Schweizer, T.; Mortby, M.E.; Smith, E.E.; Patten, S.B.; Fiest, K.M. Prevalence of Depression in Patients With Mild Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA Psychiatry 2017, 74, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Bland, R.C.; Newman, S.C.; Orn, H. Prevalence of psychiatric disorders in the elderly in Edmonton. Acta Psychiatr. Scand Suppl. 1988, 338, 57–63. [Google Scholar] [CrossRef]
- Kramer, M.; German, P.S.; Anthony, J.C.; Von Korff, M.; Skinner, E.A. Patterns of mental disorders among the elderly residents of eastern Baltimore. J. Am. Geriatr. Soc. 1985, 33, 236–245. [Google Scholar] [CrossRef]
- Regier, D.A.; Boyd, J.H.; Burke, J.D.; Rae, D.S.; Myers, J.K.; Kramer, M.; Robins, L.N.; George, L.K.; Karno, M.; Locke, B.Z. One-month prevalence of mental disorders in the United States: Based on five Epidemiologic Catchment Area sites. Arch. Gen. Psychiatry 1988, 45, 977–986. [Google Scholar] [CrossRef]
- Kay, D.W.; Henderson, A.S.; Scott, R.; Wilson, J.; Rickwood, D.; Grayson, D.A. Dementia and depression among the elderly living in the Hobart community: The effect of the diagnostic criteria on the prevalence rates. Psychol. Med. 1985, 15, 771–788. [Google Scholar] [CrossRef]
- Blazer, D.; Burchett, B.; Service, C.; George, L.K. The association of age and depression among the elderly: An epidemiologic exploration. J. Gerontol. 1991, 46, M210–M215. [Google Scholar] [CrossRef] [PubMed]
- Paĺsson, S.P.; Ostling, S.; Skoog, I. The incidence of first-onset depression in a population followed from the age of 70 to 85. Psychol. Med. 2001, 31, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Bulloch, A.G.M.; Williams, J.V.A.; Lavorato, D.H.; Patten, S.B. The depression and marital status relationship is modified by both age and gender. J. Affect. Disord. 2017, 223, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.N.; Kawachi, I.; Chang, J.; Boo, K.; Shin, H.G.; Lee, H.; Cho, S.I. Marital status, gender, and depression: Analysis of the baseline survey of the Korean Longitudinal Study of Ageing (KLoSA). Soc. Sci. Med. 2009, 69, 1608–1615. [Google Scholar] [CrossRef] [PubMed]
- Buckman, J.E.; Saunders, R.; Stott, J.; Arundell, L.L.; O’Driscoll, C.; Davies, M.R.; Eley, T.C.; Hollon, S.D.; Kendrick, T.; Ambler, G.; et al. Role of age, gender and marital status in prognosis for adults with depression: An individual patient data meta-analysis. Epidemiol. Psychiatr. Sci. 2021, 30, e42. [Google Scholar] [CrossRef]
- Feder, K.A.; Heatherington, L.; Mojtabai, R.; Eaton, W.W. Perceived Marital Support and Incident Mental Illness: Evidence from the National Comorbidity Survey. J. Marital Fam. Ther. 2019, 45, 668–683. [Google Scholar] [CrossRef]
- Hewitt, B.; Turrell, G.; Giskes, K. Marital loss, mental health and the role of perceived social support: Findings from six waves of an Australian population based panel study. J. Epidemiol. Community Health 2012, 66, 308–314. [Google Scholar] [CrossRef] [Green Version]
- Schlax, J.; Jünger, C.; Beutel, M.E.; Münzel, T.; Pfeiffer, N.; Wild, P.; Blettner, M.; Kerahrodi, J.G.; Wiltink, J.; Michal, M. Income and education predict elevated depressive symptoms in the general population: Results from the Gutenberg health study. BMC Public Health 2019, 19, 430. [Google Scholar] [CrossRef] [Green Version]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafò, M.R. The Association of Cigarette Smoking With Depression and Anxiety: A Systematic Review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, S.K.; Ryoo, J.H.; Oh, C.M.; Choi, J.M.; McIntyre, R.S.; Mansur, R.B.; Kim, H.; Hales, S.; Jung, J.Y. U-shaped relationship between depression and body mass index in the Korean adults. Eur. Psychiatry 2017, 45, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Bădescu, S.V.; Tătaru, C.; Kobylinska, L.; Georgescu, E.L.; Zahiu, D.M.; Zăgrean, A.M.; Zăgrean, L. The association between Diabetes mellitus and Depression. J. Med. Life 2016, 9, 120–125. [Google Scholar] [PubMed]
- Chan, K.L.; Cathomas, F.; Russo, S.J. Central and Peripheral Inflammation Link Metabolic Syndrome and Major Depressive Disorder. Physiology 2019, 34, 123–133. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factors | Normal (n = 94,384) | Abnormal (n = 10,708) | p-Value |
|---|---|---|---|
| Sight | <0.0001 | ||
| Normal sight | 74,818 (79.27) | 8067 (75.34) | |
| Low vision | 18,421 (19.52) | 2454 (22.92) | |
| Blindness | 1145 (1.21) | 187 (1.75) | |
| Age (years) | <0.0001 | ||
| 65–74 | 46,611 (49.43) | 5367 (50.16) | |
| 75–84 | 37,713 (39.99) | 4360 (40.75) | |
| >85 | 9973 (10.58) | 973 (9.09) | |
| Sex | <0.0001 | ||
| Male | 45,230 (47.92) | 6586 (61.51) | |
| Female | 49,154 (52.08) | 4122 (38.49) | |
| Living status | <0.0001 | ||
| Not living alone | 89,312 (94.63) | 10,028 (93.65) | |
| Living alone | 5066 (5.37) | 680 (6.35) | |
| Marriage status | <0.0001 | ||
| Married/Cohabitation | 69,124 (74.34) | 7397 (69.94) | |
| Divorce/Widowed | 15,502 (16.67) | 2185 (20.66) | |
| Unmarried/Separated | 8359 (8.99) | 994 (9.40) | |
| Education status | <0.0001 | ||
| Illiterate | 23,421 (28.44) | 1953 (21.17) | |
| Elementary/Junior high school | 51,975 (63.11) | 6154 (66.70) | |
| Above senior high school | 6962 (8.45) | 1120 (12.14) | |
| Smoking | 0.026 | ||
| No | 88,169 (93.62) | 10,065 (94.17) | |
| Yes | 6012 (6.38) | 623 (5.83) | |
| Drinking | 0.013 | ||
| No | 92,115 (97.83) | 10,492 (98.19) | |
| Yes | 2047 (2.17) | 193 (1.81) | |
| Betel nut consumption | 0.293 | ||
| No | 93,612 (99.56) | 10,623 (99.63) | |
| Yes | 410 (0.44) | 39 (0.37) | |
| BMI | <0.0001 | ||
| <18.5 | 3801 (4.05) | 609 (5.73) | |
| 18.5–24 | 42,191 (44.93) | 4999 (47.07) | |
| 24–27 | 29,607 (31.53) | 2995 (28.20) | |
| >27 | 18,302 (19.49) | 2018 (19.00) | |
| Hypertension | <0.0001 | ||
| No | 58,034 (61.58) | 6973 (65.27) | |
| Yes | 36,202 (38.42) | 3710 (34.73) | |
| Diabetes | <0.0001 | ||
| No | 57,929 (61.53) | 6953 (65.07) | |
| Yes | 36,221 (38.47) | 3733 (34.93) | |
| Cholesterol level | 0.451 | ||
| Normal | 55,297 (58.78) | 6234 (58.40) | |
| Abnormal | 38,782 (41.22) | 4441 (41.60) | |
| Triglyceride level | <0.0001 | ||
| Normal | 76,262 (81.06) | 8474 (79.34) | |
| Abnormal | 17,823 (18.94) | 2206 (20.66) | |
| Alb level | <0.0001 | ||
| Normal | 84,826 (95.38) | 9476 (94.50) | |
| Abnormal | 4112 (4.62) | 552 (5.50) | |
| Gl level | <0.0001 | ||
| Normal | 67,739 (76.04) | 7915 (78.67) | |
| Abnormal | 21,340 (23.96) | 2146 (21.33) |
| Factors | Univariate | |
|---|---|---|
| Hazard Ratio (95% CI) | p-Value | |
| Sight | ||
| Normal | 1 | |
| Low vision | 1.16 (1.11–1.22) | <0.0001 |
| Blindness | 1.59 (1.37–1.83) | <0.0001 |
| Age (years) | ||
| 65–74 | 1 | |
| 75–84 | 0.58 (0.55–0.6) | <0.0001 |
| >85 | 0.49 (0.46–0.53) | <0.0001 |
| Sex | ||
| Female | 1 | |
| Male | 0.56 (0.54–0.58) | <0.0001 |
| Living status | ||
| Not living alone | 1 | |
| Living alone | 1.01 (0.94–1.09) | 0.754 |
| Marriage status | ||
| Married/Cohabitation | 1 | |
| Divorce/Widowed | 1.29 (1.23–1.35) | <0.0001 |
| Unmarried/Separated | 1.31 (1.23–1.4) | <0.0001 |
| Education status | ||
| Above senior high scool | 1 | |
| Elementary/Junior high school | 1.44 (1.37–1.51) | <0.0001 |
| Illiterate | 1.93 (1.8–2.08) | <0.0001 |
| Smoking | ||
| No | 1 | |
| Yes | 1.08 (0.99–1.17) | 0.062 |
| Drinking | ||
| No | 1 | |
| Yes | 0.83 (0.72–0.95) | 0.008 |
| Betel nut consumption | ||
| No | 1 | |
| Yes | 1.16 (0.85–1.59) | 0.351 |
| BMI | ||
| 18.5–24 | 1 | |
| <18.5 | 1.32 (1.21–1.43) | <0.0001 |
| 24–27 | 0.87 (0.83–0.91) | <0.0001 |
| >27 | 0.95 (0.91–1.01) | 0.069 |
| Hypertension | ||
| No | 1 | |
| Yes | 0.82 (0.79–0.85) | <0.0001 |
| Diabetes | ||
| No | 1 | |
| Yes | 0.87 (0.83–0.9) | <0.0001 |
| Cholesterol level | ||
| Normal | 1 | |
| Abnormal | 1.08 (1.04–1.12) | <0.0001 |
| Triglyceride level | ||
| Normal | 1 | |
| Abnormal | 1.14 (1.08–1.19) | <0.0001 |
| Alb level | ||
| Normal | 1 | |
| Abnormal | 1.22 (1.12–1.33) | <0.0001 |
| Gl level | ||
| Normal | 1 | |
| Abnormal | 0.88 (0.84–0.93) | <0.0001 |
| Factors | Multivariate | |
|---|---|---|
| Hazard Ratio (95% CI) | p-Value | |
| Sight | ||
| Normal | 1 | |
| Low vision | 1.18 (1.12–1.24) | <0.0001 |
| Blindness | 1.52 (1.28–1.8) | <0.0001 |
| Age (years) | ||
| 65–74 | 1 | |
| 75–84 | 0.55 (0.53–0.58) | <0.0001 |
| >85 | 0.45 (0.41–0.49) | <0.0001 |
| Sex | ||
| Female | 1 | |
| Male | 0.66 (0.63–0.69) | <0.0001 |
| Living status | ||
| Not living alone | 1 | |
| Living alone | 0.95 (0.87–1.04) | 0.294 |
| Marriage status | ||
| Married/Cohabitation | 1 | |
| Divorce/Widowed | 1.18 (1.11–1.25) | <0.0001 |
| Unmarried/Separated | 1.39 (1.28–1.5) | <0.0001 |
| Education status | ||
| Above senior high school | 1 | |
| Elementary/Junior high school | 1.19 (1.13–1.26) | <0.0001 |
| Illiterate | 1.46 (1.34–1.58) | <0.0001 |
| Smoking | ||
| No | 1 | |
| Yes | 1.25 (1.14–1.38) | <0.0001 |
| Drinking | ||
| No | 1 | |
| Yes | 0.96 (0.81–1.14) | 0.636 |
| Betel nut consumption | ||
| No | 1 | |
| Yes | 0.78 (1.05–0.74) | 0.784 |
| BMI | ||
| 18.5–24 | 1 | |
| <18.5 | 1.31 (1.19–1.44) | <0.0001 |
| 24–27 | 0.85 (0.81–0.9) | <0.0001 |
| >27 | 0.9 (0.85–0.96) | 0.0007 |
| Hypertension | ||
| No | 1 | |
| Yes | 0.85 (0.81–0.89) | <0.0001 |
| Diabetes | ||
| No | 1 | |
| Yes | 0.9 (0.86–0.94) | <0.0001 |
| Cholesterol level | ||
| Normal | 1 | |
| Abnormal | 0.94 (0.9–0.98) | 0.005 |
| Triglyceride level | ||
| Normal | 1 | |
| Abnormal | 1.13 (1.07–1.2) | <0.0001 |
| Alb level | ||
| Normal | 1 | |
| Abnormal | 1.24 (1.11–1.37) | <0.0001 |
| Gl level | ||
| Normal | 1 | |
| Abnormal | 0.87 (0.83–0.91) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-Y.; Fang, I.-M.; Hu, H.-Y.; Weng, S.-H. Association of Visual Impairment with Psychological Distress in Older Adults: A Survey of 105,092 Older People in Taiwan. J. Clin. Med. 2022, 11, 1458. https://doi.org/10.3390/jcm11051458
Yen C-Y, Fang I-M, Hu H-Y, Weng S-H. Association of Visual Impairment with Psychological Distress in Older Adults: A Survey of 105,092 Older People in Taiwan. Journal of Clinical Medicine. 2022; 11(5):1458. https://doi.org/10.3390/jcm11051458
Chicago/Turabian StyleYen, Chu-Yu, I-Mo Fang, Hsiao-Yun Hu, and Shih-Han Weng. 2022. "Association of Visual Impairment with Psychological Distress in Older Adults: A Survey of 105,092 Older People in Taiwan" Journal of Clinical Medicine 11, no. 5: 1458. https://doi.org/10.3390/jcm11051458
APA StyleYen, C.-Y., Fang, I.-M., Hu, H.-Y., & Weng, S.-H. (2022). Association of Visual Impairment with Psychological Distress in Older Adults: A Survey of 105,092 Older People in Taiwan. Journal of Clinical Medicine, 11(5), 1458. https://doi.org/10.3390/jcm11051458