
Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery—A Single Center, Open-Label, Randomized Controlled Trial

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
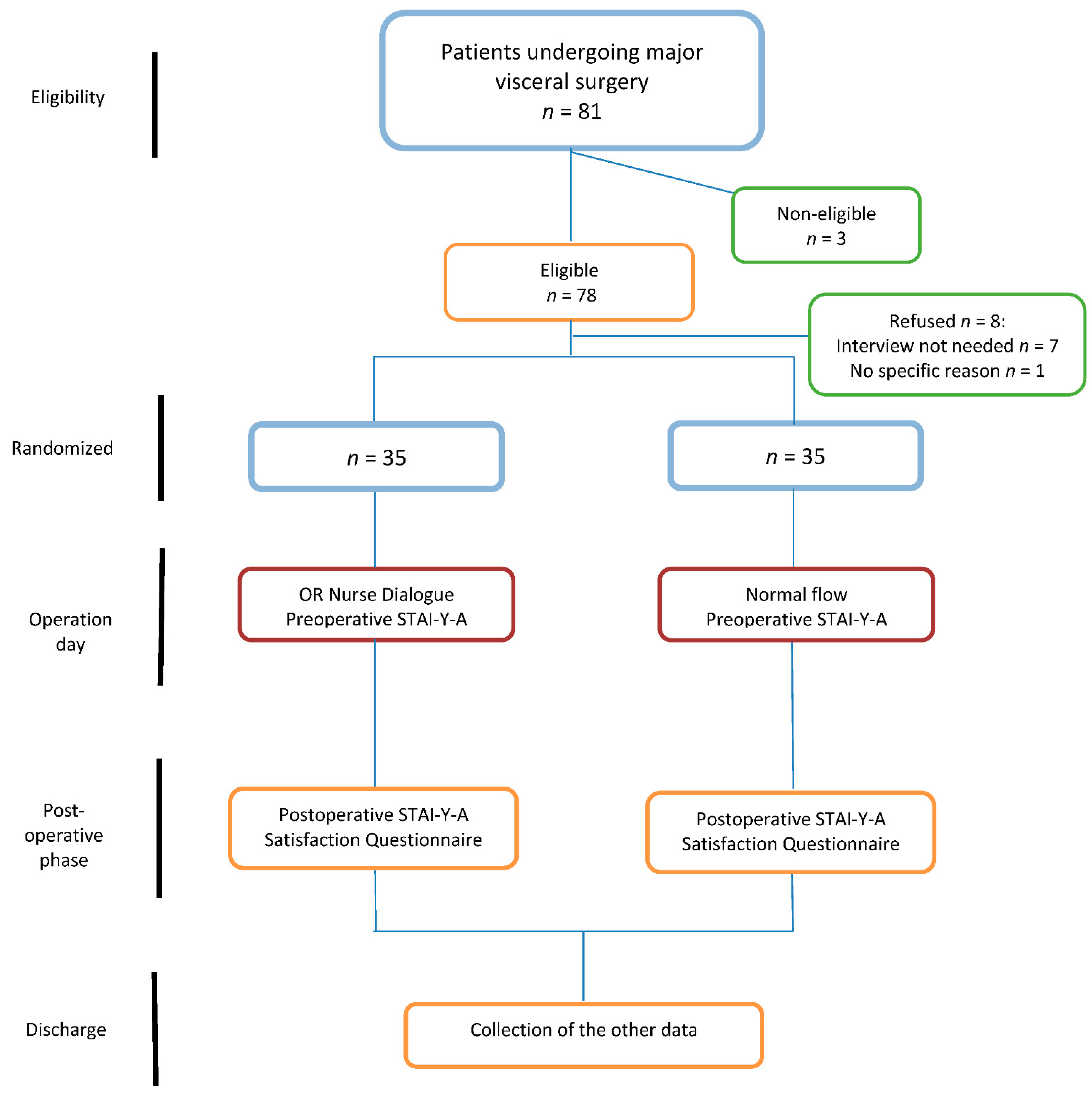
2.1. Study Design
2.2. Patients and Setting
2.3. Intervention
2.4. Outcomes
2.5. Statistical Analysis
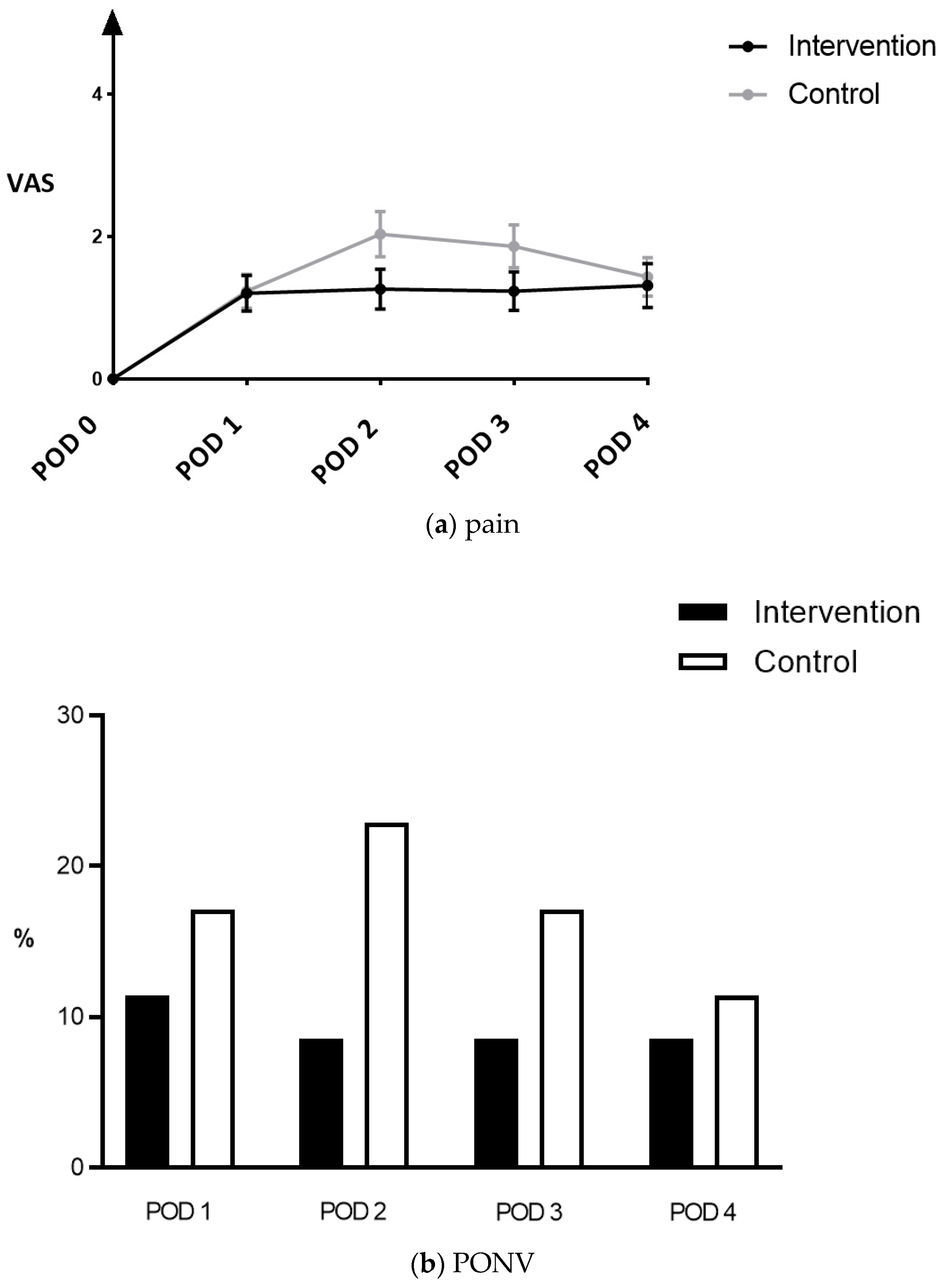
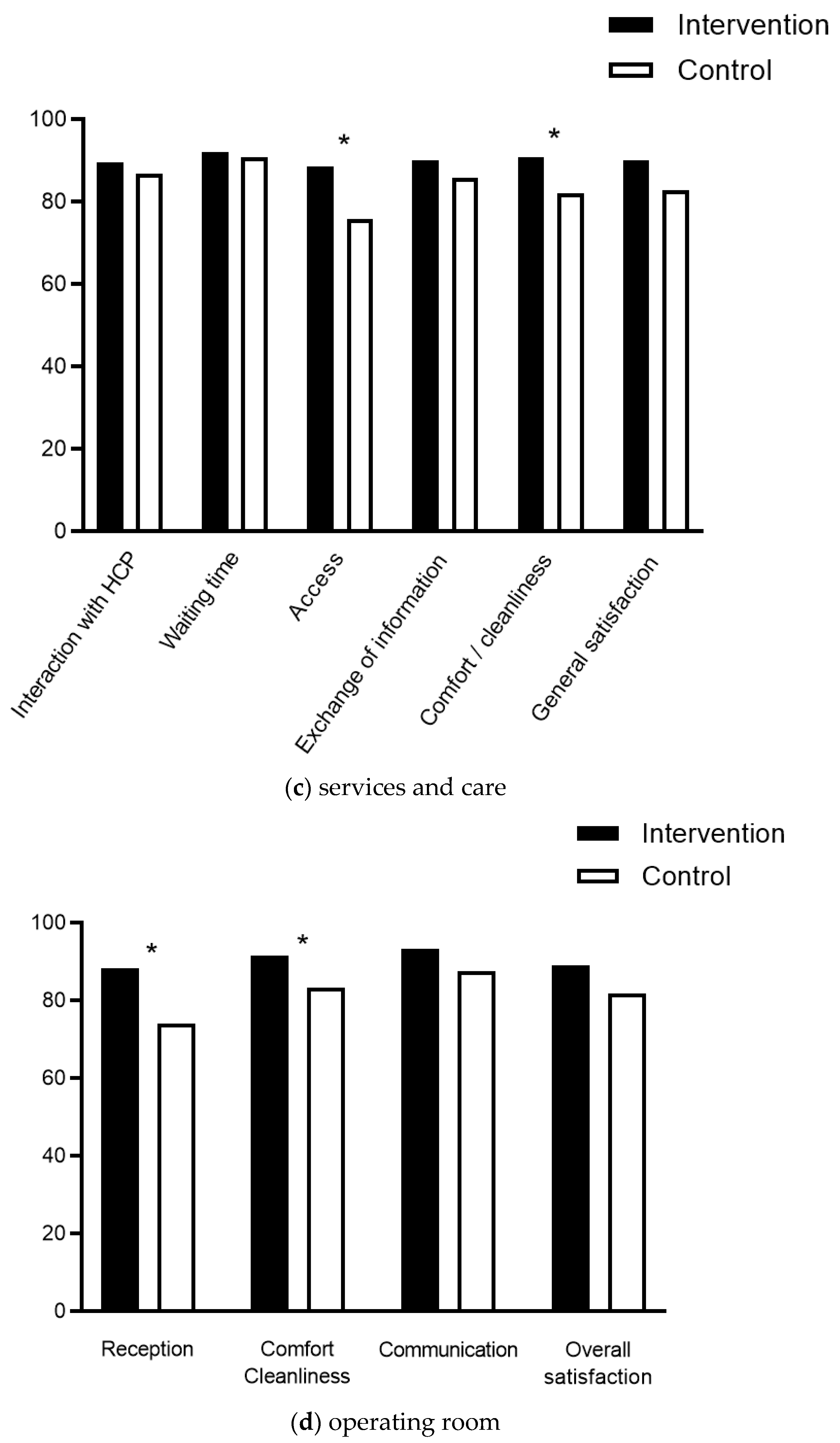
3. Results
Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villa, G.; Lanini, I.; Amass, T.; Bocciero, V.; Calabrisotto, C.S.; Chelazzi, C.; Romagnoli, S.; De Gaudio, A.R.; Grotto, R.L. Effects of psychological interventions on anxiety and pain in patients undergoing major elective abdominal surgery: A systematic review. Perioper. Med. 2020, 9, 38. [Google Scholar] [CrossRef]
- Tulloch, I.; Rubin, J.S. Assessment and Management of Preoperative Anxiety. J. Voice 2019, 33, 691–696. [Google Scholar] [CrossRef]
- Pereira, L.; Figueiredo-Braga, M.; Carvalho, I. Preoperative anxiety in ambulatory surgery: The impact of an empathic patient-centered approach on psychological and clinical outcomes. Patient Educ. Couns. 2015, 99, 733–738. [Google Scholar] [CrossRef]
- Gürsoy, A.; Candaş, B.; Güner, Ş.; Yılmaz, S. Preoperative Stress: An Operating Room Nurse Intervention Assessment. J. PeriAnesthesia Nurs. 2016, 31, 495–503. [Google Scholar] [CrossRef]
- Sadati, L.; Pazouki, A.; Mehdizadeh, A.; Shoar, S.; Tamannaie, Z.; Chaichian, S. Effect of preoperative nursing visit on preoperative anxiety and postoperative complications in candidates for laparoscopic cholecystectomy: A randomized clinical trial. Scand. J. Caring Sci. 2013, 27, 994–998. [Google Scholar] [CrossRef]
- Lindwall, L.; von Post, I. Continuity created by nurses in the perioperative dialogue—A literature review. Scand. J. Caring Sci. 2009, 23, 395–401. [Google Scholar] [CrossRef]
- Cachemaille, M.; Grass, F.; Fournier, N.; Suter, M.R.; Demartines, N.; Hübner, M.; Blanc, C. Pain Intensity in the First 96 Hours after Abdominal Surgery: A Prospective Cohort Study. Pain Med. 2019, 21, 803–813. [Google Scholar] [CrossRef]
- Grass, F.; Cachemaille, M.; Martin, D.; Fournier, N.; Hahnloser, D.; Blanc, C.; Demartines, N.; Hübner, M. Pain perception after colorectal surgery: A propensity score matched prospective cohort study. Biosci. Trends 2018, 12, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, B.L.; Schwab, J.J.; Morris, R.L.; Beldia, G. Assessment of state and trait anxiety in subjects with anxiety and depressive disorders. Psychiatr. Q. 2001, 72, 263–276. [Google Scholar] [CrossRef]
- Arraras, J.I.; Vera, R.; Martínez, M.; Hernández, B.; Laínez, N.; Rico, M.; Vila, M.; Chicata, V.; Asín, G. The EORTC cancer in-patient satisfaction with care questionnaire: EORTC IN-PATSAT32 Validation study for Spanish patients. Clin. Transl. Oncol. 2009, 11, 237–242. [Google Scholar] [CrossRef]
- Neijenhuijs, K.I.; Jansen, F.; Aaronson, N.K.; Brédart, A.; Groenvold, M.; Holzner, B.; Terwee, C.B.; Cuijpers, P.; Leeuw, I.M.V.-D. A systematic review of the measurement properties of the European Organisation for Research and Treatment of Cancer In-patient Satisfaction with Care Questionnaire, the EORTC IN-PATSAT32. Support. Care Cancer 2018, 26, 2551–2560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, T.J.; Belani, K.G.; Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; Meyer, T.A.; Urman, R.D.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2020, 131, 411–448. [Google Scholar] [CrossRef] [PubMed]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar]
- Hernández, C.R.; Gómez-Urquiza, J.L.; Pradas-Hernández, L.; Roman, K.V.; Suleiman-Martos, N.; Albendín-García, L.; Cañadas-De la Fuente, G.A. Effectiveness of nursing interventions for preoperative anxiety in adults: A systematic review with meta-analysis. J. Adv. Nurs. 2021, 77, 3274–3285. [Google Scholar] [CrossRef]
- Díez-Álvarez, E.; Arrospide, A.; Mar, J.; Alvarez, U.; Belaustegi, A.; Lizaur, B.; Arana, J.M. Effectiveness of pre-operative education in reducing anxiety in surgical patients. Enferm. Clin. 2012, 22, 18–26. [Google Scholar] [CrossRef]
- Zarei, B.; Valiee, S.; Nouri, B.; Khosravi, F.; Fathi, M. The effect of multimedia-based nursing visit on preoperative anxiety and vital signs in patients undergoing lumbar disc herniation surgery: A randomised clinical trial. J. Perioper. Pract. 2018, 28, 7–15. [Google Scholar] [CrossRef]
- Tou, S.; Tou, W.; Mah, D.; Karatassas, A.; Hewett, P. Effect of preoperative two-dimensional animation information on perioperative anxiety and knowledge retention in patients undergoing bowel surgery: A randomized pilot study. Color. Dis. 2013, 15, e256–e265. [Google Scholar] [CrossRef]
- Ljungqvist, O.; De Boer, H.D.; Balfour, A.; Fawcett, W.J.; Lobo, D.N.; Nelson, G.; Demartines, N. Opportunities and Challenges for the Next Phase of Enhanced Recovery after Surgery: A Review. JAMA Surg. 2021, 156, 775–784. [Google Scholar] [CrossRef]
- Pache, B.; Hubner, M.; Jurt, J.; Demartines, N.; Grass, F. Minimally invasive surgery and enhanced recovery after surgery: The ideal combination? J. Surg. Oncol. 2017, 116, 613–616. [Google Scholar] [CrossRef]
- Group, E.C. The Impact of Enhanced Recovery Protocol Compliance on Elective Colorectal Cancer Resection: Results from an International Registry. Ann. Surg. 2015, 261, 1153–1159. [Google Scholar]
- CHIR-Net SIGMA Study Group; Mihaljevic, A.L. Multicenter Prospective Cohort Study of the Patient-Reported Outcome Measures PRO-CTCAE and CAT EORTC QLQ-C30 in Major Abdominal Cancer Surgery (PATRONUS): A Student-Initiated German Medical Audit (SIGMA) Study. Ann. Surg. Oncol. 2021, 28, 3075–3089. [Google Scholar] [CrossRef] [PubMed]
- Dueck, A.C.; Mendoza, T.R.; Mitchell, S.A.; Reeve, B.B.; Castro, K.M.; Rogak, L.J.; Atkinson, T.M.; Bennett, A.V.; Denicoff, A.M.; O’Mara, A.M.; et al. Validity and Reliability of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 2015, 1, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- El-Hussuna, A.; Rubio-Perez, I.; Millan, M.; Pellino, G.; Negoi, I.; Gallo, G. Patient-Reported Outcome Measures in Colorectal Surgery: Construction of Core Measures Using Open-Source Research Method. Surg. Innov. 2021, 28, 560–566. [Google Scholar] [CrossRef]
- Black, N.; Varaganum, M.; Hutchings, A. Relationship between patient reported experience (PREMs) and patient reported outcomes (PROMs) in elective surgery. BMJ Qual. Saf. 2014, 23, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Koo, C.-H.; Park, J.-W.; Ryu, J.-H.; Han, S.-H. The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 3151. [Google Scholar] [CrossRef]
- Maurice-Szamburski, A.; Auquier, P.; Viarre-Oreal, V.; Cuvillon, P.; Carles, M.; Ripart, J. Effect of sedative premedication on patient experience after general anesthesia: A randomized clinical trial. JAMA 2015, 313, 916–925. [Google Scholar] [CrossRef] [Green Version]
- Wise, J. Routine use of sedatives before surgery has little benefit, study shows. BMJ 2015, 350, h1158. [Google Scholar] [CrossRef]
- Campbell, C.M.; Edwards, R.R. Ethnic differences in pain and pain management. Pain Manag. 2012, 2, 219–230. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Group n = 35 | Control Group n = 35 | Total n = 70 | p-Value | |
|---|---|---|---|---|
| Age (years, mean ± SD) | 56.6 ± 14.6 | 60.5 ± 16.1 | 58.6 ± 15.4 | 0.285 |
| ≥70 years (%) | 10 (28.6) | 14 (40) | 24 (34.3) | 0.450 |
| Gender (female, %) | 17 (48.6) | 25 (71.4) | 42 (60) | 0.087 |
| ASA score ≥ 3 | 6 (17.1) | 9 (25.7) | 15 (21.4) | 0.561 |
| Premedication (%) | 13 (37.1) | 17 (48.6) | 30 (42.9) | 0.469 |
| Peridural analgesia (%) | 15 (42.9) | 19 (54.3) | 34 (48.6) | 0.473 |
| COVID-19 phase (%) | 18 (51.4) | 19 (54.3) | 37 (52.9) | 1.000 |
| Type of major surgery (%) | 0.699 | |||
| Colorectal | 18 (51.4) | 15 (42.8) | 33 (47.1) | |
| HPB | 12 (34.3) | 15 (42.8) | 27 (38.6) | |
| Upper GI | 3 (8.6) | 5 (14.4) | 8 (11.4) | |
| Other (Endocrine) | 2 (5.7) | 0 | 2 (2.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias, P.; Clerc, D.; da Rocha Rodrigues, M.G.; Demartines, N.; Grass, F.; Hübner, M. Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery—A Single Center, Open-Label, Randomized Controlled Trial. J. Clin. Med. 2022, 11, 1895. https://doi.org/10.3390/jcm11071895
Dias P, Clerc D, da Rocha Rodrigues MG, Demartines N, Grass F, Hübner M. Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery—A Single Center, Open-Label, Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(7):1895. https://doi.org/10.3390/jcm11071895
Chicago/Turabian StyleDias, Patricia, Daniel Clerc, Maria Goreti da Rocha Rodrigues, Nicolas Demartines, Fabian Grass, and Martin Hübner. 2022. "Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery—A Single Center, Open-Label, Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 7: 1895. https://doi.org/10.3390/jcm11071895
APA StyleDias, P., Clerc, D., da Rocha Rodrigues, M. G., Demartines, N., Grass, F., & Hübner, M. (2022). Impact of an Operating Room Nurse Preoperative Dialogue on Anxiety, Satisfaction and Early Postoperative Outcomes in Patients Undergoing Major Visceral Surgery—A Single Center, Open-Label, Randomized Controlled Trial. Journal of Clinical Medicine, 11(7), 1895. https://doi.org/10.3390/jcm11071895