Abstract
Background: Foot deformities in children are common, and the majority can be treated conservatively. Nevertheless, there are deformities that require surgical treatment. These include rigid clubfeet, severe forms of pes planovalgus, pes cavus and several more. We retrospectively analysed the pseudarthrosis rate of surgical treatment of foot deformities with transcutaneous K-wire osteosynthesis in neurologically healthy children and adolescents. The aim of the study was to show that the results with K-wires are comparable to those with other osteosynthesis methods in the literature. Methods: A total of 46 paediatric patients aged 6 to 17 years treated between January 2010 and December 2015 met the inclusion criteria. Depending on the diagnosis, different surgical interventions were necessary. In clubfoot and pes planovalgus, representing n = 81, 70% of the whole collective triple arthrodesis with fusion of the talonavicular, calcaneocuboid and subtalar joints or Evans osteotomy was usually performed. Radiographs were taken at least 6 months post-surgery, and bony consolidation of the subtalar, talonavicular (TN), and calcaneocuboidal (CC) joints and the metatarsal I (MT I) osteotomy were assessed. If there was no evidence of fusion at this time, it was considered non-union. Results: In total, 117 arthrodesis procedures with K-wires were performed. Overall, 110 of the arthrodesis (94%) healed, and only 7 joints (6%) showed non-union (subtalar 0%, TN 7.7%, CC 6.5% and MT I 6.7%). All non-unions occurred in subjects with clubfoot deformities. No significant risk factors were observed. Conclusion: This study replicated the good consolidation rates reported in the literature with screws, plates, intramedullary nails or staples in arthrodesis of the adolescent foot in neurologically healthy subjects and confirmed the efficacy of K-wires. The main advantages of transcutaneous K-wire treatment are easy metal removal, lower osteosynthesis material costs and less concomitant damage. Further studies, especially randomised controlled trials, are needed to further investigate this topic.
1. Introduction
Many foot deformities affect children and adolescents, such as clubfoot, pes planovalgus, pes cavus, pes equinus, pes calcaneus and hallux valgus [1]. The incidence of clubfoot in Central Europe, for example, is 1–2/1000 [2]; symptomatic pes plano-valgus in juveniles is reported to have an incidence of 0.1/1000 [3], and juvenile hallux valgus has an incidence of 2–4% [4].
Generally, fusion surgery should be delayed to prevent changes in growth. Conservative therapy is therefore indicated for changes that are not time critical. If conservative therapy does not lead to improvement, joint-sparing interventions are indicated. If the deformity is so severe or rigid that joint sparing is not sufficient, arthrodesis surgery must be performed. Ideally, these operations are performed after the growth plates have closed.
Fortunately, most of these foot deformities are self-limiting or can be treated conservatively. After all conservative options have been exhausted and the deformity persists, a relapse occurs or if the deformity is rigid from onset, surgical correction is indicated at an age suitable for surgery. In cases of severe deformities, we performed operations for pes planovalgus from the age of 6 years. Bony correction of idiopathic clubfeet tended to be treated surgically at a later age. However, there are contraindications for surgery, such as an underlying disease that does not allow anaesthesia, legal guardians rejecting surgical therapy, acute (florid) or chronic infection, critical soft tissue conditions or general surgical risks. The standard treatment for clubfoot is Ponseti therapy, which has good clinical results [5], followed by soft tissue interventions. This consists of tenotomy of the Achilles tendon, with posterior release and occasional realignment between the talus and calcaneus followed by an orthopaedic brace. Only if this is not successful or a relapse occurs, bony correction is necessary. Surgical treatment depends on the extent of malposition. Multidimensional correction of bony structures and soft tissue is necessary for therapy-resistant clubfoot. Triple arthrodesis, consisting of Chopart (talonavicular and calcaneocuboid joints) and subtalar arthrodesis, has proven successful [6]. In this procedure, all components of the clubfoot (equinus, cavus, adductus, varus) are corrected. In less severe cases, Chopart arthrodesis can be sufficient.
The planovalgus foot is characterised by reduction or loss of the normal medial longitudinal arch (pes planus) by hindfoot valgus/forefoot abduction and often occurs with concomitant hindfoot equinus. All these components can be flexible or rigid. Bresnahan et al. and Blitz et al. demonstrated that early conservative therapy for paediatric pes plano-valgus leads to less long-term damage [7,8]. If there is no improvement, surgical therapy is indicated. The surgical treatment of pes planovalgus is triple arthrodesis or calcaneus lengthening osteotomies, and the most common lengthening therapy is Evans osteotomy.
A severe pes cavus should be treated with Chopart and subtalar arthrodesis and pes calcaneus with inverse Lambrinudi arthrodesis. Every surgery was performed using transcutaneous K-wires.
K-wires are inexpensive and can be easily removed during and after surgery [6]. Armstrong et al. showed that the surgical time was significantly longer for patients undergoing rigid internal fixation with a screw versus a K-wire for MT I osteotomies [9]. With the transcutaneous technique, the wires remain in the foot only for the first period of bone healing and are then removed in the postoperative outpatient treatment with pliers, sometimes under local anaesthesia, or, in rare cases, with sedation [6]. The use of K-wires is recommended for all ages.
Kim et al. demonstrated that proximal chevron metatarsal osteotomy with intramedullary screw fixation provides superior biomechanical stability to locking plate and K-wire fixations [10], raising the question of whether this approach leads to higher healing rates in bone consolidation.
Characteristics of the osteosynthesis materials in terms of costs, advantages/disadvantages and indications see Table 1.

Table 1.
Modified from Dreher et al. [6], characteristics of the osteosynthesis materials.
Seitz and Carpenter followed up a total of 66 patients in the years 1961–1970 and found a pseudarthrosis rate of 9.1% following triple arthrodesis. Five of the six pseudarthroses were in the talonavicular joint, and one was in the calcaneocuboid joint. K-wires were used in 22 cases, of which two did not heal; of 36 cases without osteosynthesis, four did not heal, and in the Staples group, a total of eight patients did not develop pseudarthrosis. The follow-up treatment consisted of wearing a full leg cast for 6 weeks followed by a short leg cast for 6–8 weeks [11]. Wilson et al. observed non-union in 10.3% of triple arthrodesis cases [12]. The highest incidence of non-union occurred in the talonavicular joint, followed by the calcaneocuboid and, rarely, the subtalar joint [13].
Nagy et al. showed a very good result for Evans osteotomy in pes planus, with 17 cases without non-union. They used screws for fixation [14]. Nejib et al used K-wires for lengthening calcaneal surgeries with good clinical and radiological results. One non-union occurred in a cuneiform osteotomy out of 20 flat feet surgeries [15].
Several factors leading to non-union have been described in the literature, for example, the absence of internal fixation, poor bony contact, and early weight-bearing [13]. In particular, early weight-bearing has a substantial impact. It is assumed that the resulting vertical shear forces prevent bony healing, especially in the talonavicular joint [16]. Other risk factors include age [12], the underlying diagnosis [11], the surgical technique used for fixation and deep wound infection [17].
We postulate that our treatment with K-wires and a rigid follow-up with 6 weeks of recumbent plaster and 6 weeks of walking plaster with slowly increasing weight-bearing achieves the same or even lower pseudarthrosis and non-union rates than reported in the literature for screws, plates, intramedullary nails or staples. In addition, K-wires have advantages, such as easy metal removal during an outpatient visit after 6 weeks and low material costs.
2. Materials and Methods
In this retrospective study, all medical records of subjects who presented to the orthopaedic clinic for arthrodesis surgery of the foot between January 2010 and December 2015 were reviewed. This study was conducted with the approval of the local ethics committee (University of Heidelberg).
Every patient under 18 years of age who underwent a foot arthrodesis operation with K-wires for a non-neurological cause was included. Different surgeons from the foot surgery department performed the standardised procedures. In approximately 70% of the subjects, the indication for the surgical procedure was clubfoot or pes planovalgus. Demographic characteristics and postoperative complications were assessed using the subjects’ medical records. The variables included age, sex, weight, comorbidities, affected side, complications, number of K-wires. The subjects were followed up regularly for a median of 25 (6; 127) months. An X-ray follow-up appointment after 6 and at least 26 weeks (median 79 weeks; 116 ± 104 weeks after) was needed. All joints that did not demonstrate bony consolidation on X-ray after 6 months were designated non-unions.
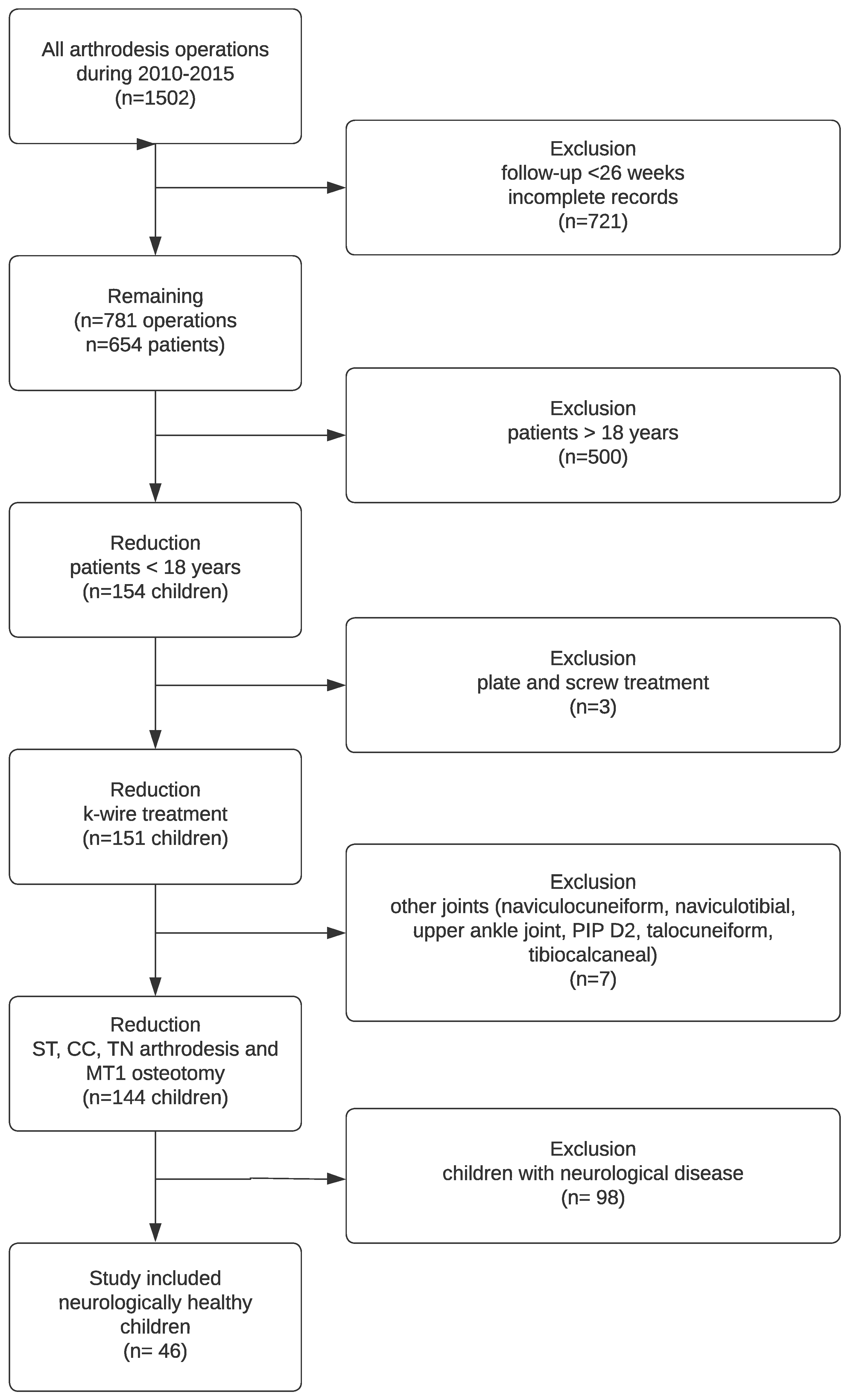
As shown in the following flowchart (Figure 1), the main reason for exclusion was missing X-rays after 6 months. In total, 154 children met the follow-up criteria; in three cases, other osteosynthesis material was used, seven subjects were excluded due to joints other than the TN, CC, subtalar and MT I, and 98 patients had a neurological disease causing the deformity. Therefore, at least 46 subjects were included (Table 2).
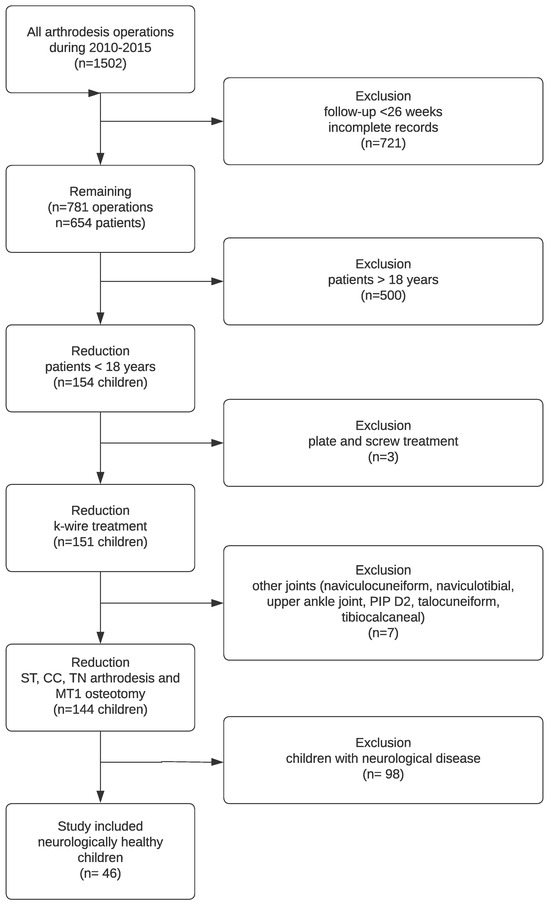
Figure 1.
Flowchart of the study population.
Table 2.
Sociodemographic variables.
After surgery, the young subjects continued to be treated as outpatients, and insufficient casts were changed as needed. After 6 weeks, radiographic control was performed, and the K-wires were removed. Another cast with weight bearing was applied for another 6 weeks. Thereafter, only one appointment was scheduled after 6 months for clinical and radiographic control and regular annual check-ups until the growth plates were closed.
2.1. Operative Procedure
It is common to combine different soft-tissue procedures (“balancing”) and bony procedures (“correction”) for the correction of multiplanar deformities. Here, we focus on bony procedures (Figure 2).

Figure 2.
Transcutaneous K-wires for Chopart arthrodesis and Metatarsale I osteotomy plus soft tissue procedure.
We used the surgical procedure as prescribed in Table 3 by Dreher et al. [6]:
Table 3.
Overview of surgical procedures and indications.
2.2. Clubfoot
The Chopart joint was prepared, and the cartilage from the joints to be fused was subsequently removed. The foot was then redressed into its corrected position, and first, the TN joint was fixed with two K-wires. Before the calcaneocuboid joint was transfixed with two K-wires, a spreader was inserted into the subtalar space. The correct size of the lateral-based wedge was measured and harvested from the iliac crest. The iliac crest wedge was inserted, and the spreader was removed. Two more transcutaneous K-wires in parallel or in crossing technique were used to fixate the calcaneus, wedge and talus (Figure 3a,b). In milder cases, only Chopart’s arthrodesis was occasionally necessary [6,13].

Figure 3.
(a) Relapse of clubfoot. (b) Foot position after Chopart’s arthrodesis.
2.3. Pes Cavovarus
The first step was to release the plantar fascia (Steindler procedure) [22]. This step should be performed in all cavovarus feet because the subsequent repositioning of the foot after corrective osteotomy (Cole [23] extension osteotomy of the first metatarsal) or fusion (Chopart’s arthrodesis) of the cavus is easier. Then, the posterior tibial tendon was split into two halves and transferred through the interosseous membrane (T-SPOTT). One was used to augment the dorsiflexor, and the other was used to laterally augment the short peroneal tendon. The following step was the bony correction of the cavus and hindfoot varus with Chopart’s fusion and dorsal-based wedge resection for hindfoot reconstruction. In more severe cases, triple fusion or Lambrinudi arthrodesis [19] was performed. Finally, soft tissue procedures, claw toe correction and an extension osteotomy of the first metatarsal were performed to correct the plantar flexion deformity (Figure 4a,b) [6].

Figure 4.
(a) Before correction of pes cavovarus. (b) Foot position after triple arthrodesis.
2.4. Pes Planovalgus
2.4.1. Modified Evans Procedure
First, a calcaneal neck osteotomy perpendicular to its longitudinal axis at least 1 cm proximal to the calcaneocuboid joint was performed. Then, a transcutaneous K-wire was drilled through the cuboid bone, the calcaneocuboid joint, and the distal part of the calcaneal neck. The osteotomy was opened with a spreader until the correct position was reached, and the iliac crest bone wedge was impacted. The osteotomy and the wedge were fixed with three to four crossing K-wires [6,24].
2.4.2. Calcaneocuboid Distraction-Fusion
The spreader was applied after removing cartilage from the calcaneocuboid joint. The joint was opened until the needed correction was achieved, and a prepared iliac crest bone wedge was impacted. This was followed by transfixation with three to four crossing K-wires [6,25].
2.4.3. Grice Procedure
The neck of the calcaneus was exposed, and cartilage was removed from the anterior aspect of the subtalar joint. An adequate iliac crest bone wedge was prepared and inserted between the calcaneus and talus. Finally, transfixation was performed with two to four crossing K-wires [6,26].
2.4.4. Triple Fusion
See the procedure for clubfoot above.
2.4.5. Skewfoot
We used the surgical procedure described by Hagmann et al.: Evans osteotomy [27]:
The saw blade was inserted approximately 1.5 cm proximal from the calcaneocuboid joint without affecting the medial, dorsal, or plantar cortical shell of the calcaneus. A transcutaneous K-wire was inserted to fixate the cuboid and the distal fragment of the calcaneus to prevent dorsal deviation during osteotomy. The calcaneal osteotomy of the medial cortex was completed with a chisel. A distractor helped to determine the degree of correction needed to reduce hindfoot valgus. A trapezoid-shaped graft of the needed size was taken from the iliac crest. The graft was fixed with two to four crossing K-wires, depending on primary stability [28].
2.4.6. Pes Equinus
Lambrinudi arthrodesis [19,29]: First, debridement of the sinus tarsi and removal of the bifurcate ligament were needed. Then, the subtalar, calcaneocuboidal, and talonavicular joints were exposed. For deformity correction, a bone wedge from the calcaneus and talus (25–30°) was removed. For better fitting, debridement of the talar head and navicular was performed. The cartilage of the calcaneocuboidal joint was removed. After reduction (neutral dorsiflexion and 10° foot abduction), fixation was performed with K-wires [30].
2.4.7. Pes Calcaneus
Inverse Lambrinudi arthrodesis [20]: The arthrodesis consists of triple arthrodesis between the talus, calcaneus, navicular, and cuboid, in combination with inserting a bone wedge and cancellous bone between the talus and calcaneus. After this correction, a further step was necessary, and an additional bone graft was implanted between the talus and navicular bone.
2.4.8. Hallux Valgus
There were different concepts for the treatment of hallux valgus depending on the severity of the deformity. Chevron and Scarf osteotomy for the correction of mild metatarsus primus varus deformities, lapidus arthrodesis (TMT I joint) for the correction of severe metatarsus primus varus deformities and Akin osteotomy for the supplementary correction of hallux valgus interphalangeus [31].
Occasionally, combinations of the operations mentioned above have been used to correct multidimensional foot deformities.
2.4.9. Postoperative Treatment
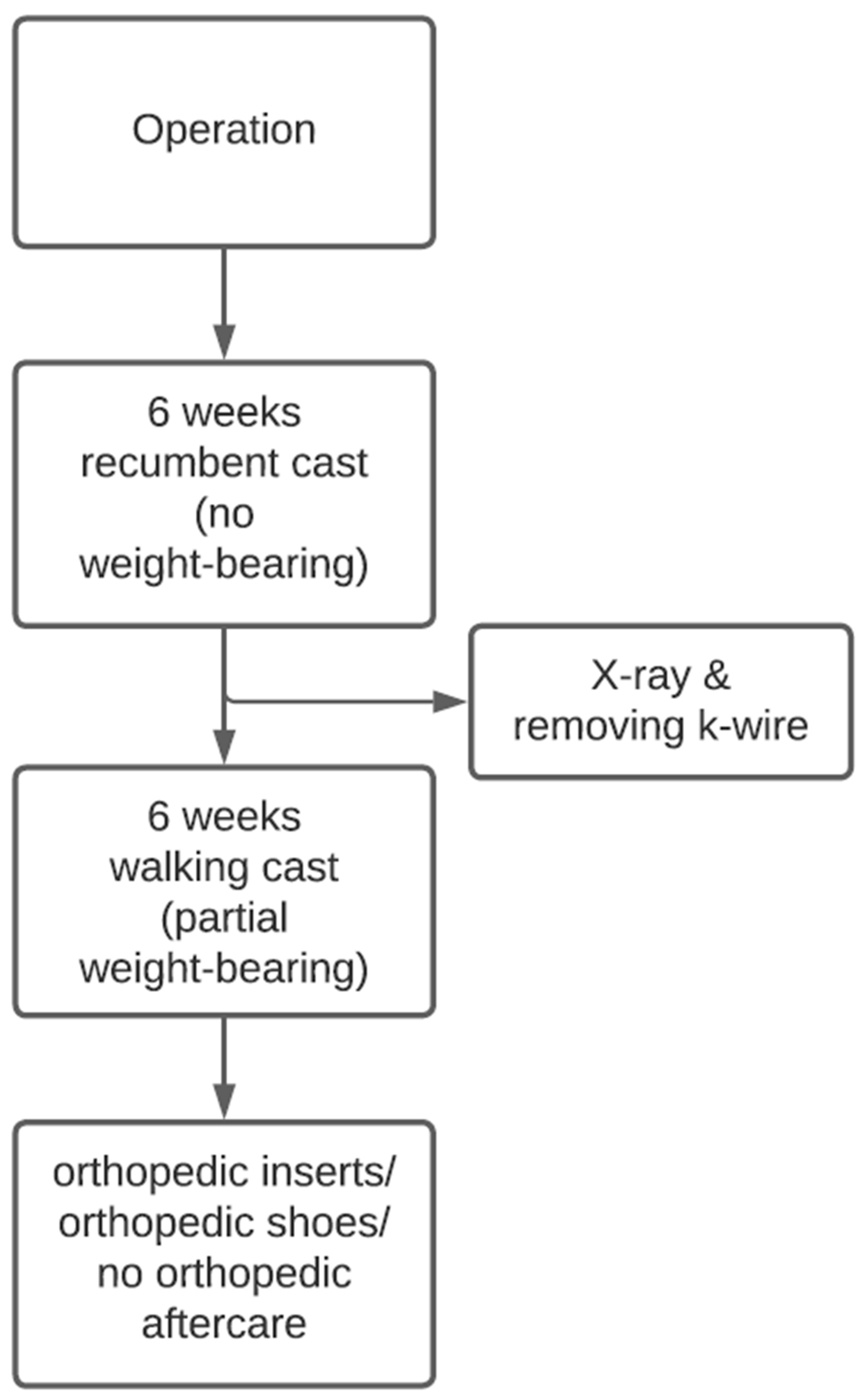
Standard wound checks were performed in our outpatient clinic. For this purpose, windows were cut into lower leg plaster to examine and dress the wounds. To prevent transcutaneous infections from the wires, regular wound checks should be made. Six weeks after surgery, the K-wires were removed. In some cases, local anaesthesia was necessary; wires were removed with pliers. During this appointment, the recumbent cast was changed to a walking cast, which the subjects wore for another 6 weeks. The walking cast allows partial weight-bearing, which should be increased over time with full weight-bearing occurring around the 12th postoperative week. Then, the cast was removed, and depending on the clinical findings, orthopaedic inserts or shoes were fitted in our technical orthopaedics department (Figure 5).
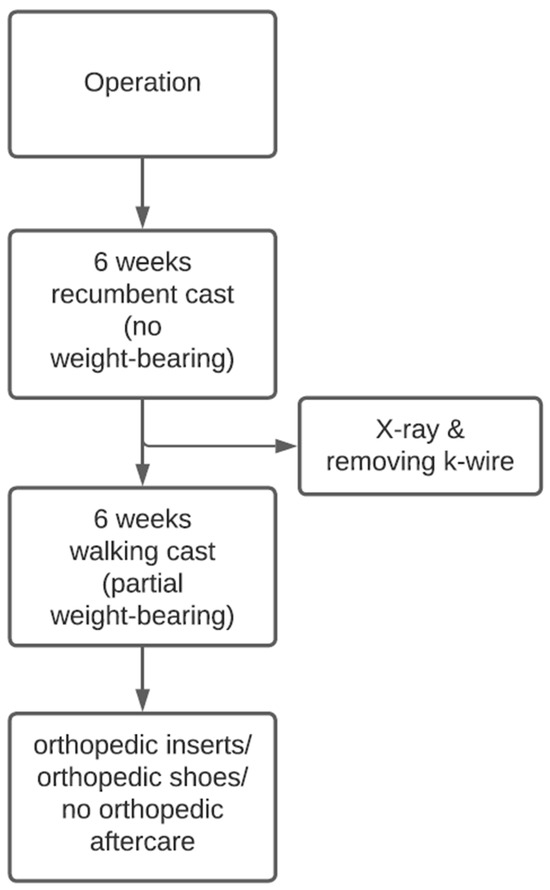
Figure 5.
Flowchart on standardised postoperative follow-up treatment.
X-ray controls were performed in a standardised manner in two planes. Depending on the region of the arthrodesis, additional planes were sometimes included. In this manner, it was possible to reliably determine the complications of non-union. For this study, only the subtalar, talonavicular (TN), calcaneocuboidal (CC) joints and metatarsal I (MT I) osteotomy treated with K-wire osteosynthesis were examined. As described above, depending on the indication, a combination arthrodesis of different joints was necessary to achieve a good clinical result.
2.4.10. Statistics
The statistical analyses were performed using IBM SPSS Statistics 28. P values were interpreted descriptively, and a p value < 0.05 was considered to indicate significance. The independence of the different factors (sex, joint, age, weight) was examined using chi-square and Mann–Whitney U tests. The statistical analysis was performed in collaboration with the Institute for Medical Biometry of the University Hospital Heidelberg.
3. Results
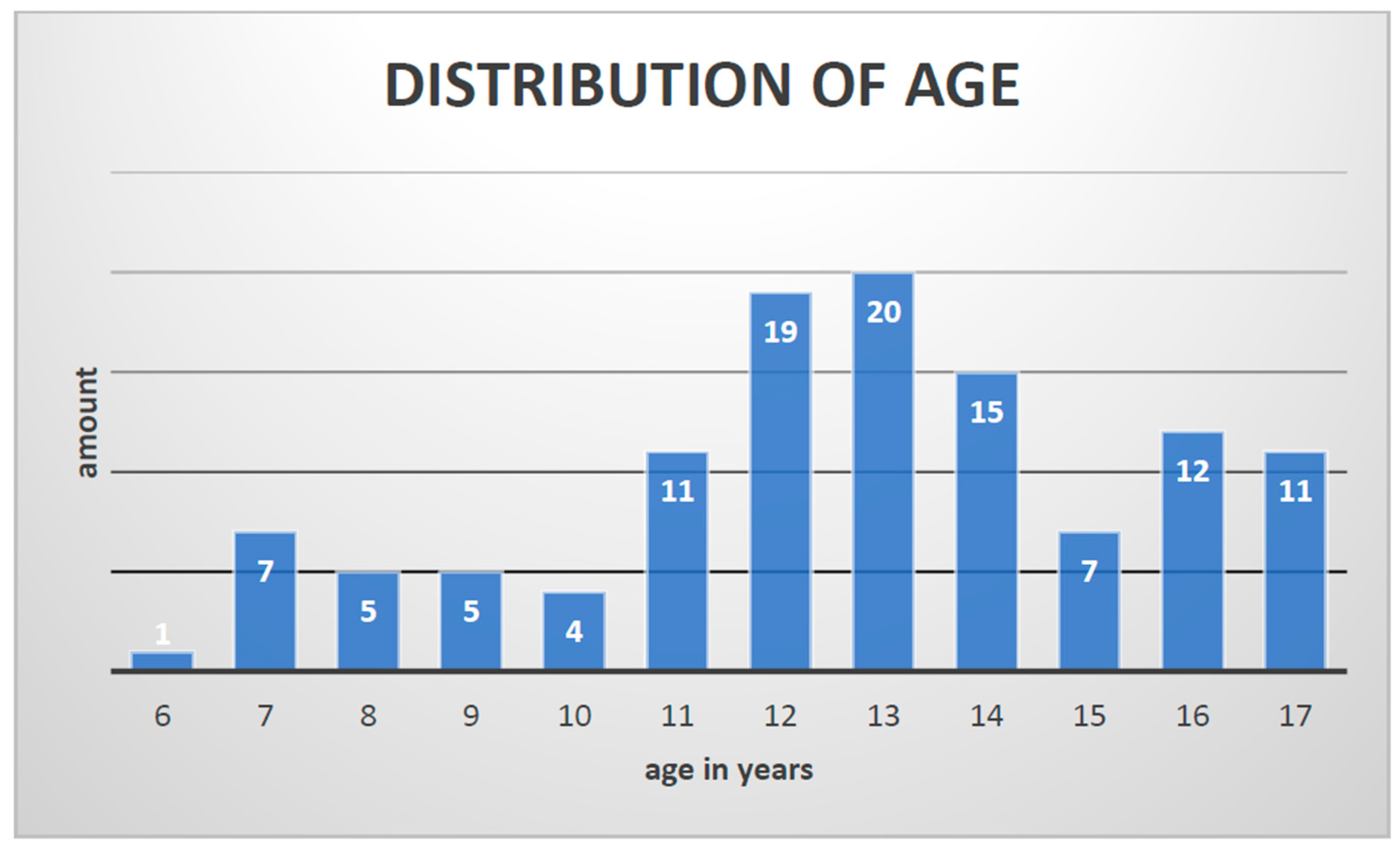
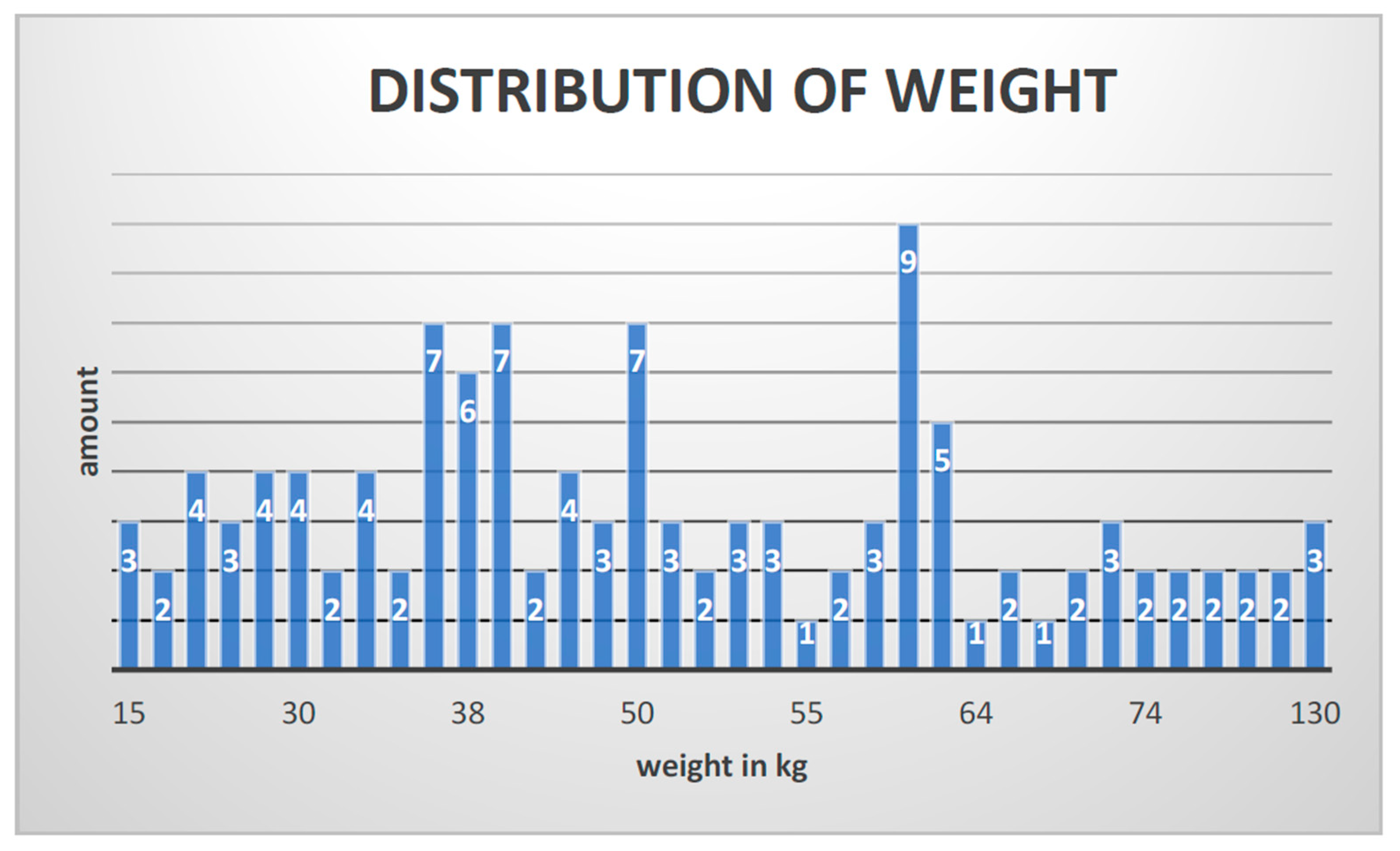
In total, 46 subjects matched the inclusion criteria, and 117 arthrodesis procedures with K-wires were performed. The entire patient cohort was distributed as follows: 70% (81) boys and 30% (36) girls with a median age of 13 years (6–17 y; 12.68 ± 2.815) and an average weight of 50 kg (15–130 kg; 51.01 ± 22.944) (Figure 6 and Figure 7).
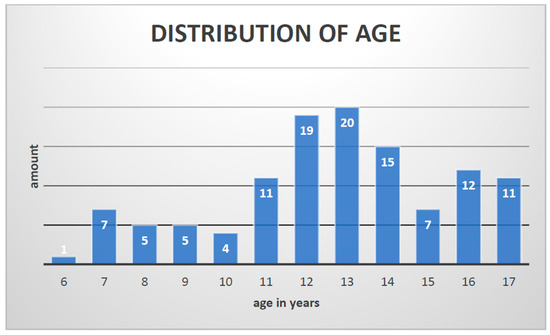
Figure 6.
Distribution of age.
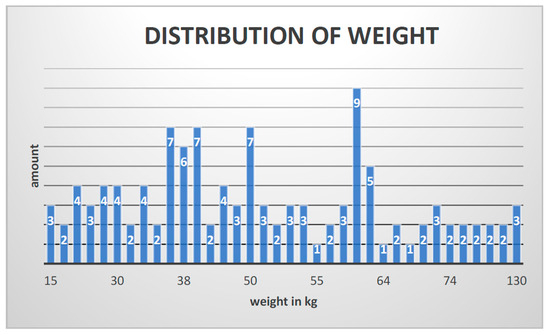
Figure 7.
Distribution of weight.
Neither age (p = 0.104) nor body weight (p = 0.501) was a significant risk factor for non-union.
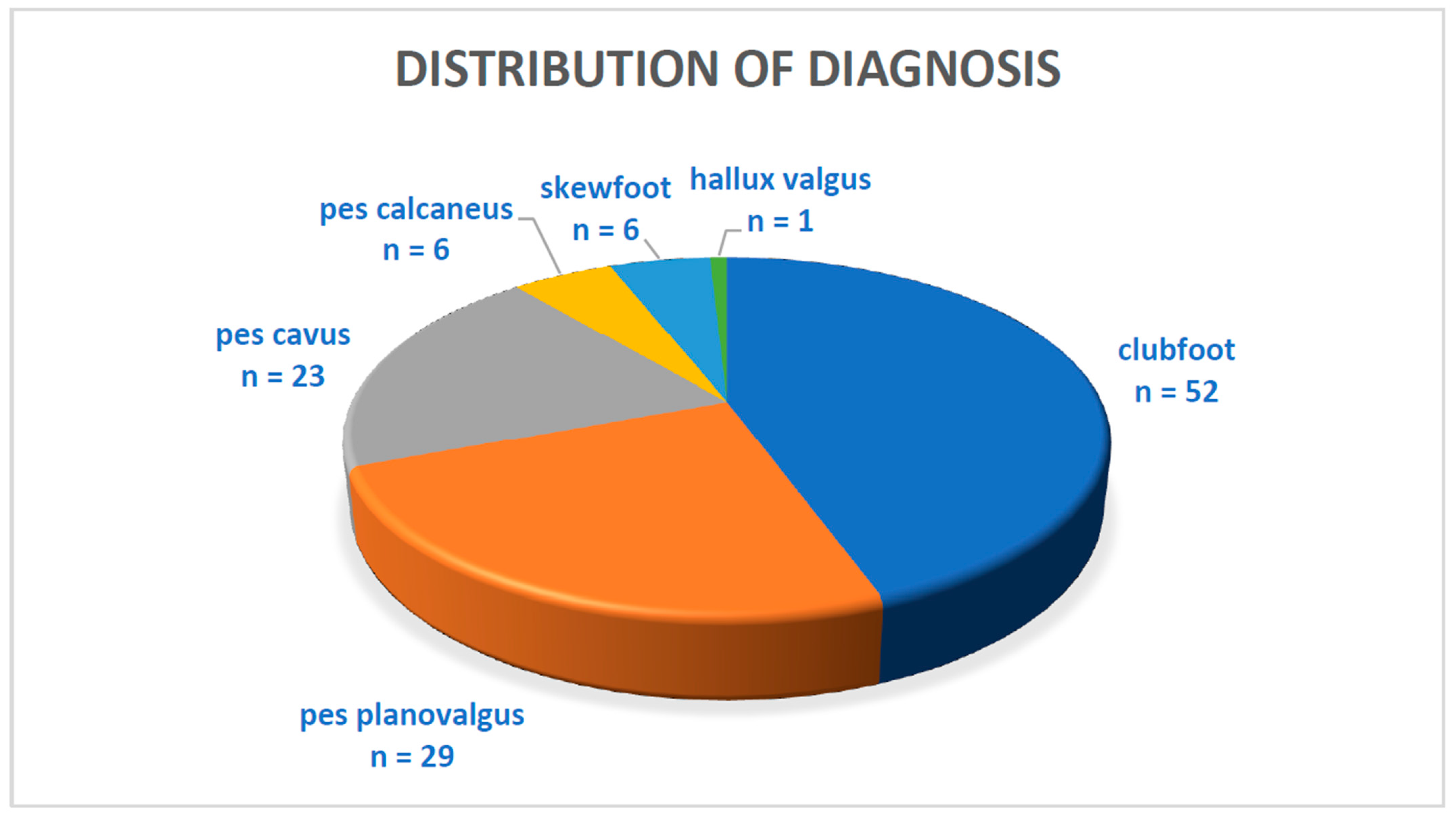
Regarding the distribution of the diagnoses (Figure 8) that led to the indication of arthrodesis, almost half of the subjects had clubfoot (52). The second most common diagnosis was pes planovalgus (29), followed by pes cavus (23), pes calcaneus (6), skewfoot (6) and hallux valgus (1).
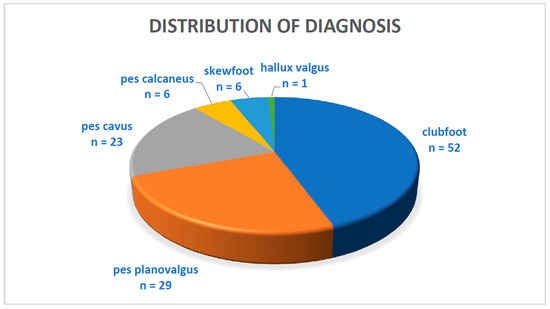
Figure 8.
Distribution of diagnosis.
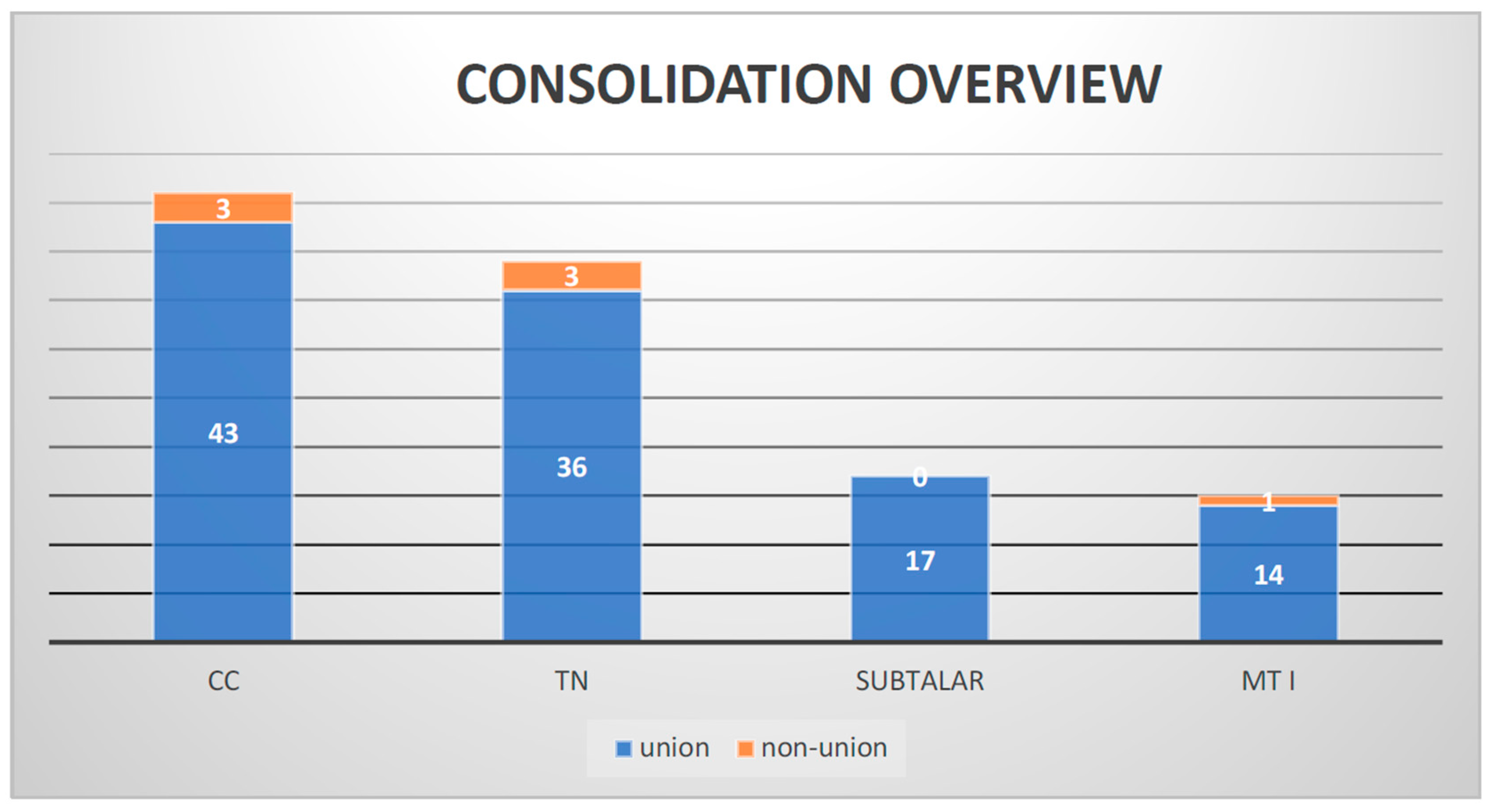
Our follow-up showed that over 94% of the arthrodesis cases healed. Of 117 joints, only 7 showed non-union, 3 TN joints, 3 CCs and 1 MT I (Figure 9).
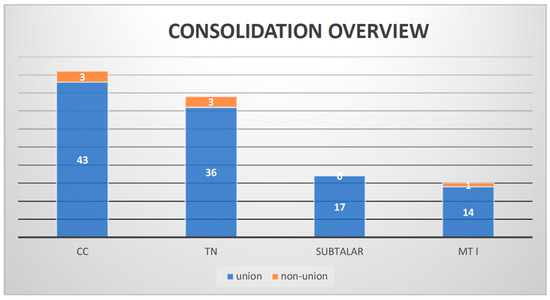
Figure 9.
Consolidation overview.
In total, 17 subtalar arthrodesis procedures were performed, and after 26 weeks, no non-union was found. Of 39 operated talonavicular joints, 3 showed non-union (7.7%). Regarding the calcaneocuboidal joints, 3 out of 46 showed non-union (6.5%), and the surgeries at MT I demonstrated one non-union out of 15 (6.7%). No significant association between joint and non-union was observed (p = 0.737) (Figure 10a,b and Figure 11a,b).
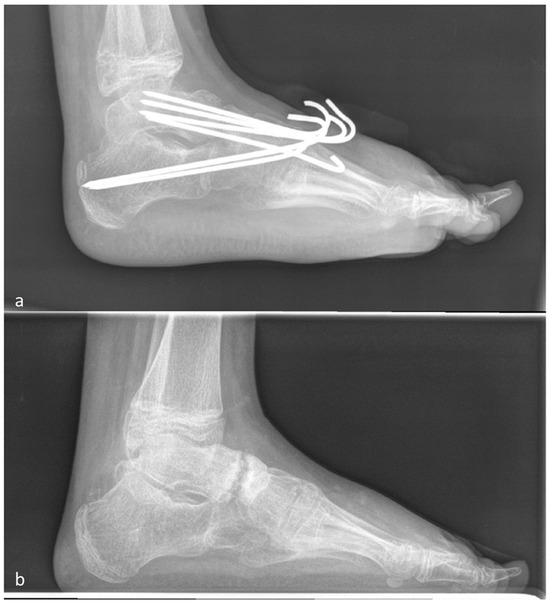
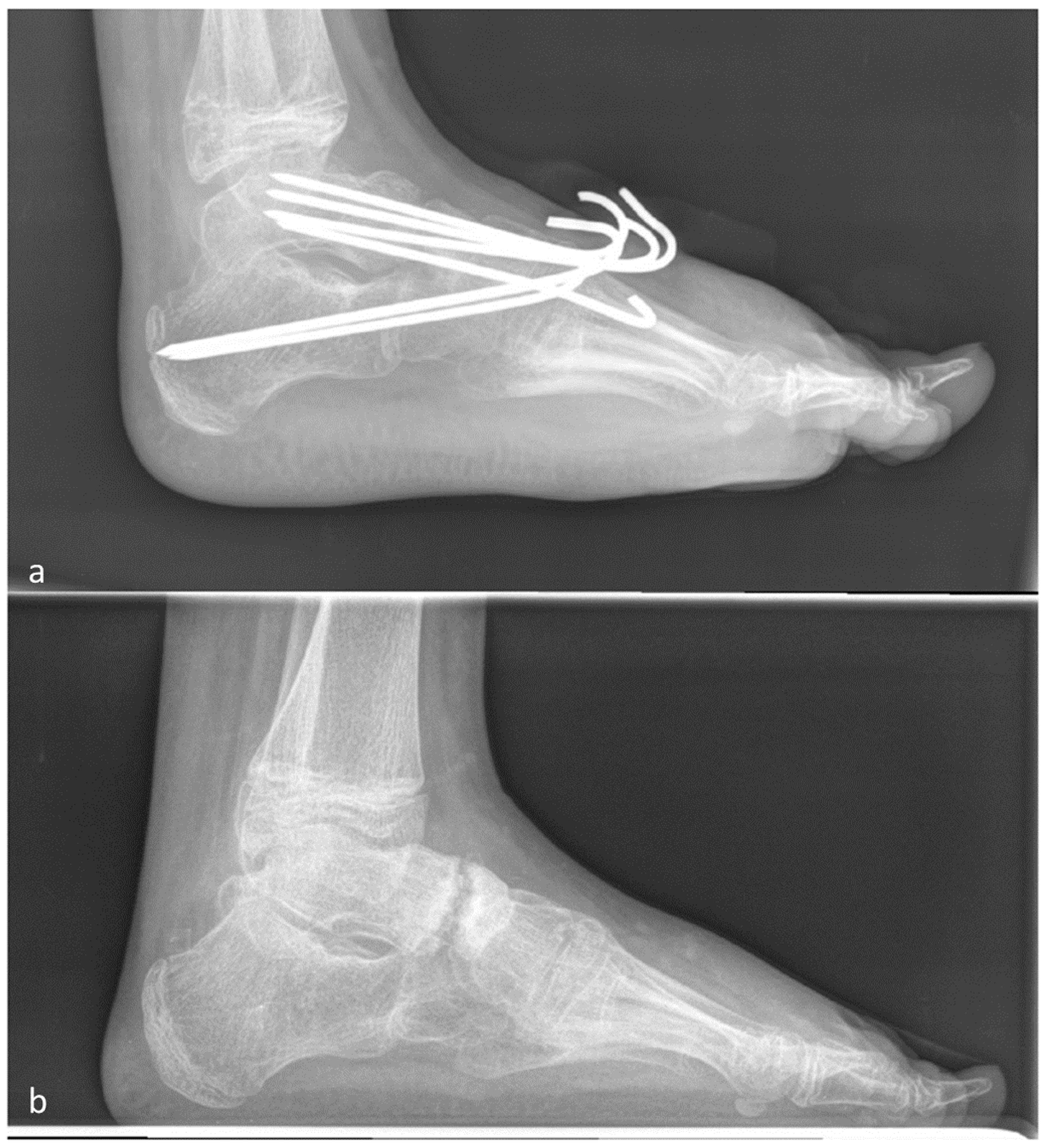
Figure 10.
(a) First post-surgery X-ray after talo-navicular and CC arthrodesis with K-wires. (b) Talo-navicular non-union 8 months after surgery.

Figure 11.
(a) First post-surgery X-ray after talo-navicular and CC arthrodesis with K-wires. (b) Talo-navicular bony consolidation 10 months after surgery.
Of the 46 subjects, 4 showed non-union (Table 4). The first had non-union in the TN and CC joints. The boy weighed 93 kg at age thirteen. Three revision surgeries were needed due to wound healing disorders. The second patient also had non-union in the TN and CC joints. The female patient was 10 years old, had a body weight of 37 kg and showed a wound-healing disorder that could be cured with antibiotics. The third patient, a male, 8 years old, 27 kg with a previous pantalar release and a respiratory disease, had a non-union in the TN joint. The fourth patient, a 12-year-old female weighing 35 kg, had a wound disorder that was healed by wound management and had non-union in the MT 1 and CC joints.
Table 4.
Overview of the non-unions in this study.
No significant association between poor fracture healing and a specific previous disease was observed, but all the non-union cases involved arthrodesis for clubfoot deformity. Five of the seven non-union subjects showed a wound-healing disorder in the postoperative period. Two of these needed surgery. In total, eight subjects (17%) had wound disorders. In four cases, revision was needed. The soft tissues healed properly during the procedure. Recurrence of the deformity was documented in two subjects despite correct bone healing. Further operations became necessary, one requiring Chopart arthrodesis for seven years and the other subject supramalleolar derotation approximately nine years after the initial surgery. There were no smokers or diabetes mellitus patients in our cohort.
4. Discussion
The purpose of this study was to investigate whether the non-union rate in arthrodesis of the foot with K-wires is comparable to screws and plates or other osteosynthesis materials. To our knowledge, this is the first study to focus on bony consolidation after K-wire osteosynthesis of various joints in the hind, mid and forefoot in children and adolescents aged 6–17 years without previous neurological disease. A total of 117 joints were re-examined in 46 children from January 2010 to December 2015. We defined non-union if no bone consolidation could be seen in the X-ray over 6 months after surgery. Due to the young patient population, standard CT diagnostics were not used.
Our results confirmed the union rates reported in the literature. Consistent with former studies, the talonavicular joint [32] had the worst outcome in our study, with a non-union rate of 7.7%. Wicks et al. demonstrated a non-union rate of 5%, which is comparable to our findings, and they also used pins and rigid postoperative treatment with 10–12 weeks of cast wearing [13]. They described 159 cases between 1971 and 2006. This retrospective study included patients younger than 16 who were operated on at the TN joint by a single surgeon with pins. Turriago et al. reported a non-union rate of 11.8% in children with cerebral palsy. They used Steinmann pins and cannulated cortical screws. Pseudarthrosis occurred in seven cases, six in the group with Steinmann pins and one in the screw group. However, no statistical significance between the occurrence of pseudarthrosis and the fixation method was found. The post-surgery treatment was a short leg cast for 6 weeks [33]. This retrospective study investigated TN arthrodesis after pes planus valgus correction between February 2002 and December 2005. A total of 59 feet were included, and the patient age ranged from 9–20 years.
Arumugam et al recently reviewed non-union rates in TN arthrodesis depending on the osteosynthesis material used: screw fixation (n = 75): 87.5% to 100%, staple fixation (n = 13): 100%, intraosseous fix system (n = 16): 100%, and K-wire fixation (n = 2): 100%. One study utilised a dorsal locking plate with two supplemented compression screws (n = 9, fusion rate = 100%), and two used a combination of screws with staples (n = 26, fusion rate = 96%) [34].
The CC joints did not heal in 6.5% of cases, consistent with the data from Moore et al., who reported a non-union rate of 7.1% for the CC joint in adults treated using screws [35]. Between 2007 and 2011, 70 patients with flat feet were retrospectively examined. The radiological follow-up was 52 weeks. The patients were transitioned to a weight-bearing Cam walker boot at 6 weeks postoperatively and allowed to gradually increase weight-bearing from 10% to 100% over the next 6 weeks with active and passive ankle movement permitted. Wicks et al. reported a slightly better outcome, with a non-union rate of 2% [13].
The 17 cases of subtalar arthrodesis all healed, consistent with previous findings; for example, Wicks et al. reported 1.3% non-union [13].
MT1 osteotomy showed a non-union rate of 6.7%, and the literature findings are inconsistent. Kim et al. demonstrated that proximal chevron metatarsal osteotomy with intramedullary screw fixation provides superior biomechanical stability to locking plate and K-wire fixations. The new technique using intramedullary screw fixation can offer robust fixation and may lead to better outcomes in the surgical treatment of hallux valgus [10]. Armstrong et al. found that those treated with rigid internal screw fixation for distal MT I osteotomies did not resume wearing shoes earlier, developed fewer postoperative infections, or had an increased long-term range of motion compared with the group receiving external fixation with a single K-wire. The surgical time was significantly longer for those patients undergoing rigid internal fixation with a screw (42.5 +/− 9.5 vs. 35.1 +/− 6.6 min, p < 0.001). Therefore, Armstrong concluded that there is no significant difference in postoperative infection, dehiscence, long-term structural correction attained, or range of motion achieved between rigid internal screws and external K-wires used to fixate distal metatarsal osteotomies [9].
In our cohort, only four cases (3.4%, two patients) needed revision due to a wound healing disorder. Superficial wound healing disorders occurred in 7.5% of patients and healed properly without surgical intervention. Wicks et al. reported a 7% wound infection rate, and Crevoisier documented a deep infection rate ranging from 0% to 2%, whereas superficial wound infection or scar dehiscence occurred in 0% to 10% of patients [13,32]. Overall, wound healing disorders seem to be a factor in bony consolidation in our study. We did not obtain a statistically significant result; however, wound-healing disorders were documented in three out of four patients with pseudarthrosis. This is consistent with the results of Galindo et al. and Martone et al. [17,36].
Regarding the gender distribution, there were twice as many boys included in the study than girls, and arthrodesis tended to heal worse in girls; however, we could not determine the reason for this, and the result was not significant. Only 3.6% of all arthrodesis in boys did not heal, while 11.1% of joints in girls showed non-union. Regarding age and weight, no significant risk factors were found.
Studies have shown that K-wires are not as stable as, for example, screws. We postulate that the posttreatment regimen of a total of 12 weeks of cast wearing, split into 6 weeks of recumbency followed by 6 weeks of walking plaster, can achieve comparable union rates. K-wire osteosynthesis coupled with rigid posttreatment leads to very good consolidation rates. K-wires also have the advantage of very uncomplicated metal removal, which can be conducted at a routine follow-up appointment after 6 weeks by pulling percutaneously inserted K-wires in an ambulant setting. This means that no foreign material remains that could irritate the musculoskeletal system, become infected or influence the surgical procedure in subsequent interventions. In addition, this procedure is much less expensive than other osteosynthesis and carries almost no periinterventional risks during removal, such as wound infection, anaesthesia-associated problems, or injury to the musculoskeletal system.
Plaster treatment ensures immobilisation, especially at a young age. When orthoses are prescribed, the patient’s compliance is not guaranteed; thus, bony consolidation is endangered by early weight-bearing.
Limitations
Limitations of the study are the retrospective design and the inclusion of inhomogeneous interventions based on different indications and different surgeons. Unfortunately, we did not have a comparison group, which is needed to compare our results with those reported in the current literature.
Ultimately, we could not identify a significant risk factor, only a tendency in which the female sex, postoperative wound infection and the underlying disease-causing clubfoot seem to play a role.
5. Conclusions
We demonstrated that K-wire osteosynthesis in combination with rigid postoperative cast treatment achieves very good results, with bone healing observed in 94% of patients, and is superior to the other procedures in terms of requiring fewer operations, easier metal removal, lower costs and shorter operating time. However, the follow-up treatment includes 12 weeks of plaster and thus a long immobilisation with higher effort in follow-up care with regular checks and at least one change in plaster. This potentially leads to more expensive follow-up care and necessitates closer patient follow-up. Further randomised controlled trials are needed to confirm the results.
Author Contributions
Conceptualization, C.P. and J.K.; methodology, A.H.; software, A.H. and S.F.; validation A.H., J.K. and S.F.; investigation, A.G., J.K. and S.F.; resources, A.H.; data curation, S.F.; writing—original draft preparation, J.K.; writing—review and editing, J.K. and S.M.; visualization, S.F.; supervision, A.G. and C.P.; project administration, C.P. and J.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional ethics committee of the University of Heidelberg (Nr. S-649/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to sensitive patient data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Biz, C.; Cerchiaro, M.; Mori, F.; Rossin, A.; Ponticiello, M.; Crimì, A.; Ruggieri, P. Flatfoot over the centuries: The background of current conservative and operative treatments. Int. Orthop. 2023, 47, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Krauspe, R.; Weimann-Stahlschmidt, K.; Westhoff, B. The Current State of Treatment for Clubfoot in Europe. In European Instructional Lectures; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Hefti, F.; Brunner, R. Das abgeflachte Fußlängsgewölbe. Der Orthopäde 1999, 28, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Myerson, M.S.; Badekas, A. Hypermobility of the first ray. Foot Ankle Clin. 2000, 5, 469–484. [Google Scholar]
- Ganesan, B.; Luximon, A.; Al-Jumaily, A.; Balasankar, S.K.; Naik, G.R. Ponseti method in the management of clubfoot under 2 years of age: A systematic review. PLoS ONE 2017, 12, e0178299. [Google Scholar] [CrossRef] [PubMed]
- Dreher, T.; Hagmann, S.; Wenz, W. Reconstruction of Multiplanar Deformity of the Hindfoot and Midfoot with Internal Fixation Techniques. Foot Ankle Clin. 2009, 14. [Google Scholar] [CrossRef] [PubMed]
- Bresnahan, P.J.; Juanto, M.A. Pediatric Flatfeet—A Disease Entity That Demands Greater Attention and Treatment. Front. Pediatr. 2020, 8. [Google Scholar] [CrossRef]
- Blitz, N.M.; Stabile, R.J.; Giorgini, R.J.; DiDomenico, L.A. Flexible Pediatric and Adolescent Pes Planovalgus: Conservative and Surgical Treatment Options. Clin. Podiatr. Med. Surg. 2010, 27, 59–77. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Pupp, G.R.; Harkless, L.B. Our fixation with fixation: Are screws clinically superior to external wires in distal first metatarsal osteotomies? J. Foot Ankle Surg. 1997, 36, 353–355. [Google Scholar] [CrossRef]
- Kim, J.S.; Cho, H.K.; Young, K.W.; Kim, J.S.; Lee, K.T. Biomechanical comparison study of three fixation methods for proximal chevron osteotomy of the first metatarsal in hallux valgus. CiOS Clin. Orthop. Surg. 2017, 9, 514–520. [Google Scholar] [CrossRef]
- Seitz, D.G.; Carpenter, E.B. Triple arthrodesis in children: A ten-year review. South. Med. J. 1974, 67, 1420–1424. [Google Scholar] [CrossRef]
- Wilson, F.C.; Fay, G.F.; Lamotte, P.; Williams, J.C. Triple arthrodesis. A study of the factors affecting fusion after three hubdred and one procedures. J. Bone Jt. Surgery. Am. Vol. 1965, 47, 340–348. [Google Scholar] [CrossRef]
- Wicks, E.D.; Morscher, M.A.; Newton, M.; Steiner, R.P.; Weiner, D.S. Partial or non-union after triple arthrodesis in children: Does it really matter? J. Child. Orthop. 2016, 10, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Nagy, M.; Kholeif, A.; Mansour, A.M.R.; Abdelhameed, S.; Radwan, Y.A.; Khedr, A.; Elhalawany, A.S.; Samir, A.; Sarhan, I.; Zein, A.B. Comparison between Malerba osteotomy and combined Evans/medial displacement calcaneal osteotomies for the management of flexible pes planus in young adults: A prospective randomised control trial, three years follow-up. Int. Orthop. 2021, 45, 2579–2588. [Google Scholar] [CrossRef] [PubMed]
- Nejib, K.; Delpont, M. Medium-term results of calcaneus lengthening in idiopathic symptomatic flat foot in children and adolescents. J. Child. Orthop. 2020, 14, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Adelaar, R.S.; Dannelly, E.A.; Meunier, P.A.; Stelling, F.H.; Goldner, J.L.; Colvard, D.F. A long term study of triple arthrodesis in children. Orthop. Clin. N. Am. 1976, 7, 895–908. [Google Scholar] [CrossRef]
- Galindo, M.J.; Siff, S.J.; Butler, J.E.; Cain, T.E. Triple Arthrodesis in Young Children: A Salvage Procedure After Failed Releases in Severely Affected Feet. Foot Ankle Int. 1987, 7, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Zwipp, H.; Rammelt, S. Modified evans osteotomy for the operative treatment of acquired pes planovalgus. Oper. Orthop. Und Traumatol. 2006, 18, 182–197. [Google Scholar] [CrossRef] [PubMed]
- Lambrinudi, C. New operation on drop-foot. Br. J. Surg. 1927, 15, 193–200. [Google Scholar] [CrossRef]
- Complete Tendon Transfer and Inverse Lambrinudi Arthrodesis: Preliminary Results of a New Technique for the Treatment of Paralytic Pes Calcaneus. Fuß Sprunggelenk 2009, 7, 683–689. [CrossRef]
- Grice, D.S. An extra-articular arthrodesis of the subastragalar joint for correction of paralytic flat feet in children. J. Bone Jt. Surg. Am. Vol. 1952, 34, 927–940. [Google Scholar] [CrossRef]
- Steindler, A. The treatment of pes cavus (Hollow claw foot). Arch. Surg. 1921, 2, 117–128. [Google Scholar] [CrossRef]
- Cole, W.H. The classic. The treatment of claw-foot. By Wallace, H. Cole. 1940. Clin. Orthop. Relat. Res. 1983, 181, 3–6. [Google Scholar]
- Lamm, B.M.; Knight, J.; Ernst, J.J. Evans Calcaneal Osteotomy: Assessment of Multiplanar Correction. J. Foot Ankle Surg. 2022, 61, 700–705. [Google Scholar] [CrossRef]
- Hyer, L.C.; Carpenter, A.M.; Swetenburg, J.R.; Westberry, D.E. Calcaneocuboid distraction arthrodesis for children with symptomatic pes planovalgus: Does fixation improve outcomes? J. Pediatr. Orthop. Part B 2021, 30, 273–281. [Google Scholar] [CrossRef]
- Osateerakun, P.; Cheewasukanon, S.; Limpaphayom, N. Grice extra-articular subtalar fusion for spastic pes planovalgus. Int. Orthop. 2022, 46, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Evans, D. Calcaneo valgus deformity. J. Bone Jt. Surg. Ser. B 1975, 57, 270–278. [Google Scholar] [CrossRef]
- Hagmann, S.; Dreher, T.; Wenz, W. Skewfoot. Foot Ankle Clin. 2009, 14. [Google Scholar] [CrossRef] [PubMed]
- So, L.W.N.; Kuong, E.E.; To, K.T.M.; Leong, J.C.Y.; Chow, W. Long-term outcome after Lambrinudi arthrodesis: How they’re doing after three decades. J. Orthop. Surg. 2019, 27, 2309499019826492. [Google Scholar] [CrossRef] [PubMed]
- Elsner, A.; Barg, A.; Stufkens, S.; Knupp, M.; Hintermann, B. Modified Lambrinudi arthrodesis with additional posterior tibial tendon transfer in adult drop foot. Oper. Orthop. Traumatol. 2011, 23, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Smyth, N.A.; Aiyer, A.A. Introduction: Why Are There so Many Different Surgeries for Hallux Valgus? Foot Ankle Clin. 2018, 23, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Crevoisier, X. The Isolated Talonavicular Arthrodesis. Foot Ankle Clin. 2011, 16, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Turriago, C.A.; Arbeláez, M.F.; Becerra, L.C. Talonavicular joint arthrodesis for the treatment of pes planus valgus in older children and adolescents with cerebral palsy. J. Child. Orthop. 2009, 3, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, V.; Ranjit, S.; Patel, S.; Welck, M. What is the best fixation technique for isolated talonavicular arthrodesis? —A systematic review. Foot 2023, 54, 101966. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.E.; Wingert, N.C.; Irgit, K.S.; Gaffney, C.J.; Cush, G.J. Single-Incision Lateral Approach for Triple Arthrodesis. Foot Ankle Int. 2014, 35, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Martone, J.; Poel, L.V.; Levy, N. Complications of Arthrodesis and Nonunion. Clin. Podiatr. Med. Surg. 2012, 29, 11–18. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).