
Clinical Impact of a Protocol Involving Cone-Beam CT (CBCT), Fusion Imaging and Ablation Volume Prediction in Percutaneous Image-Guided Microwave Ablation in Patients with Hepatocellular Carcinoma Unsuitable for Standard Ultrasound (US) Guidance


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
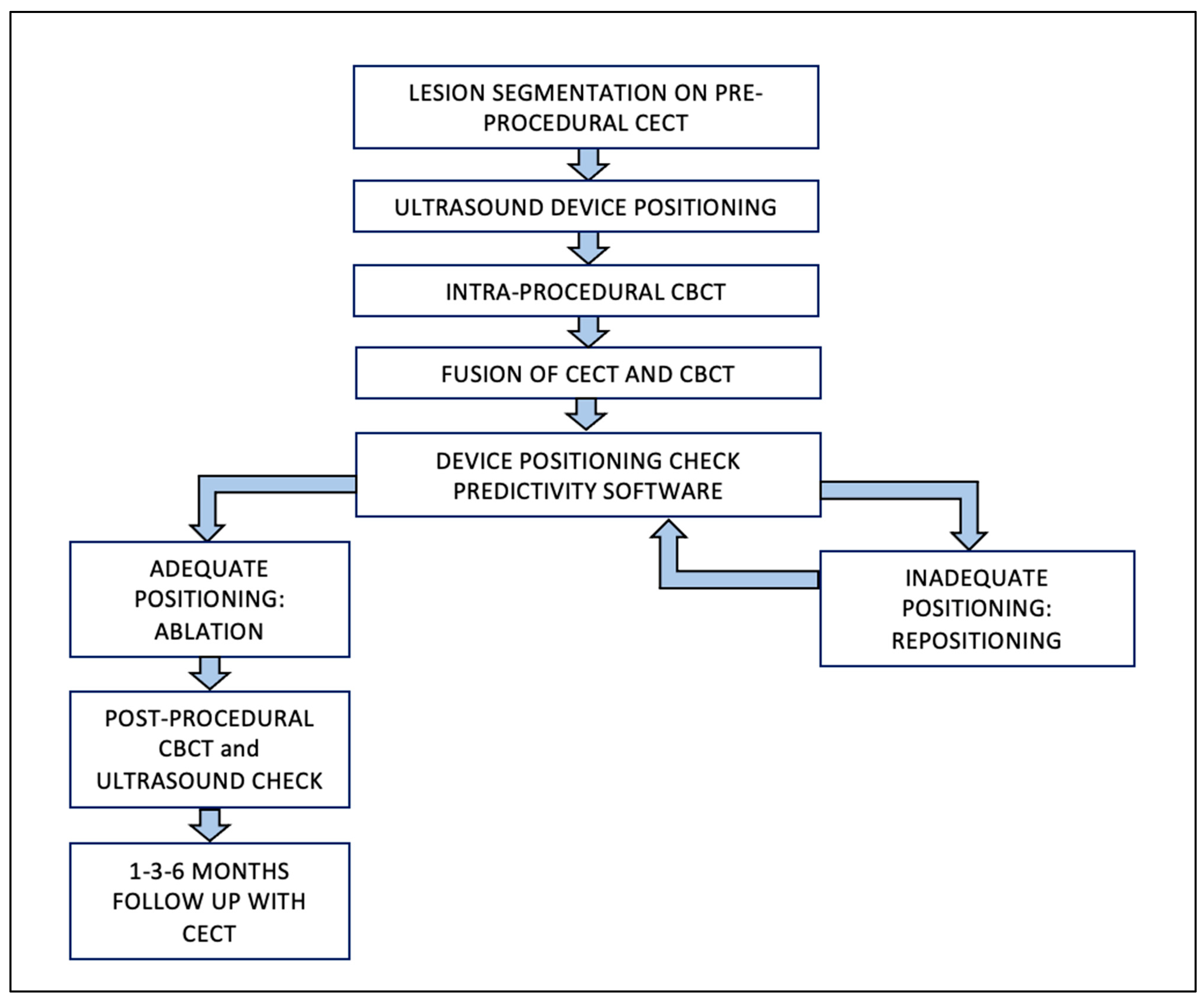
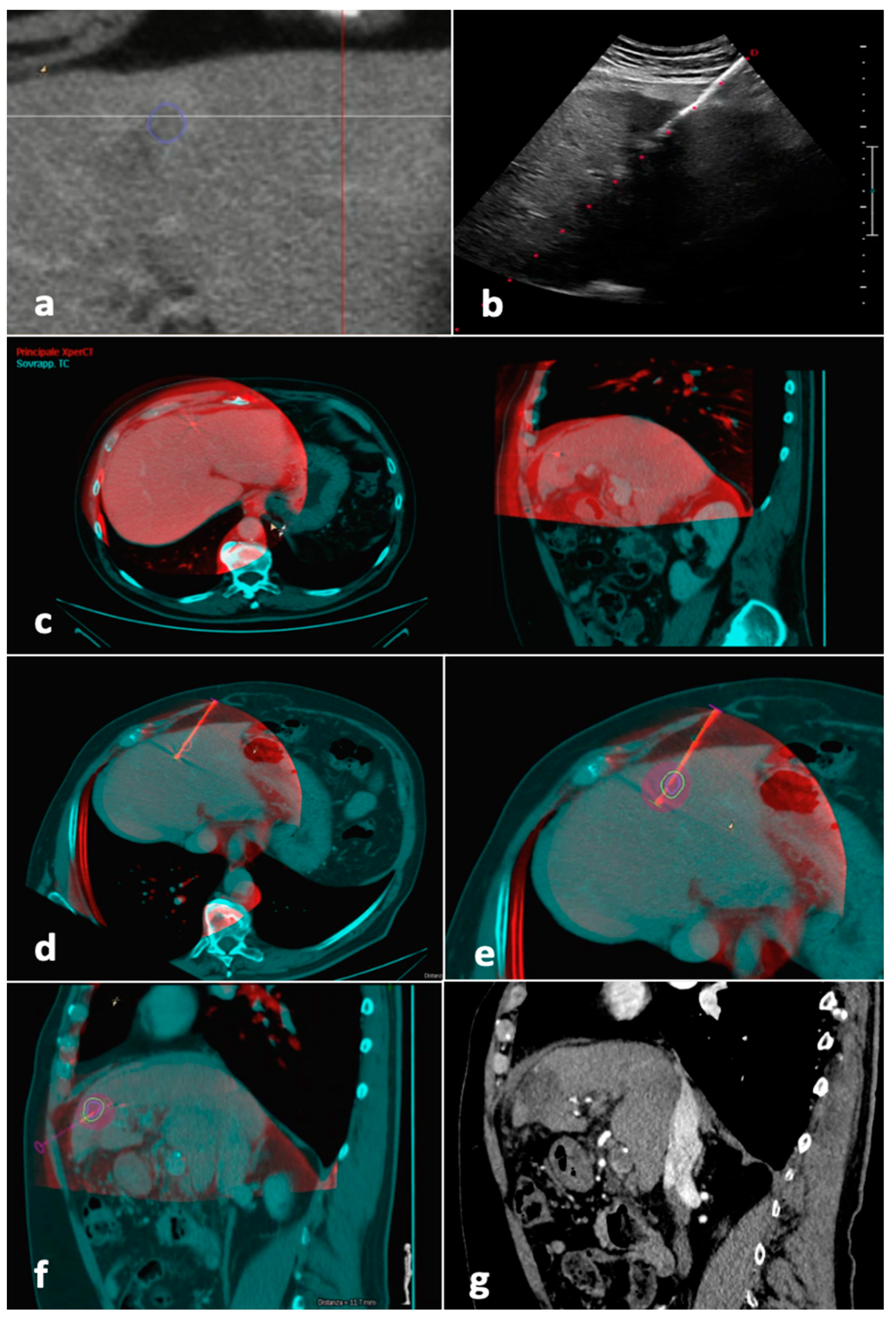
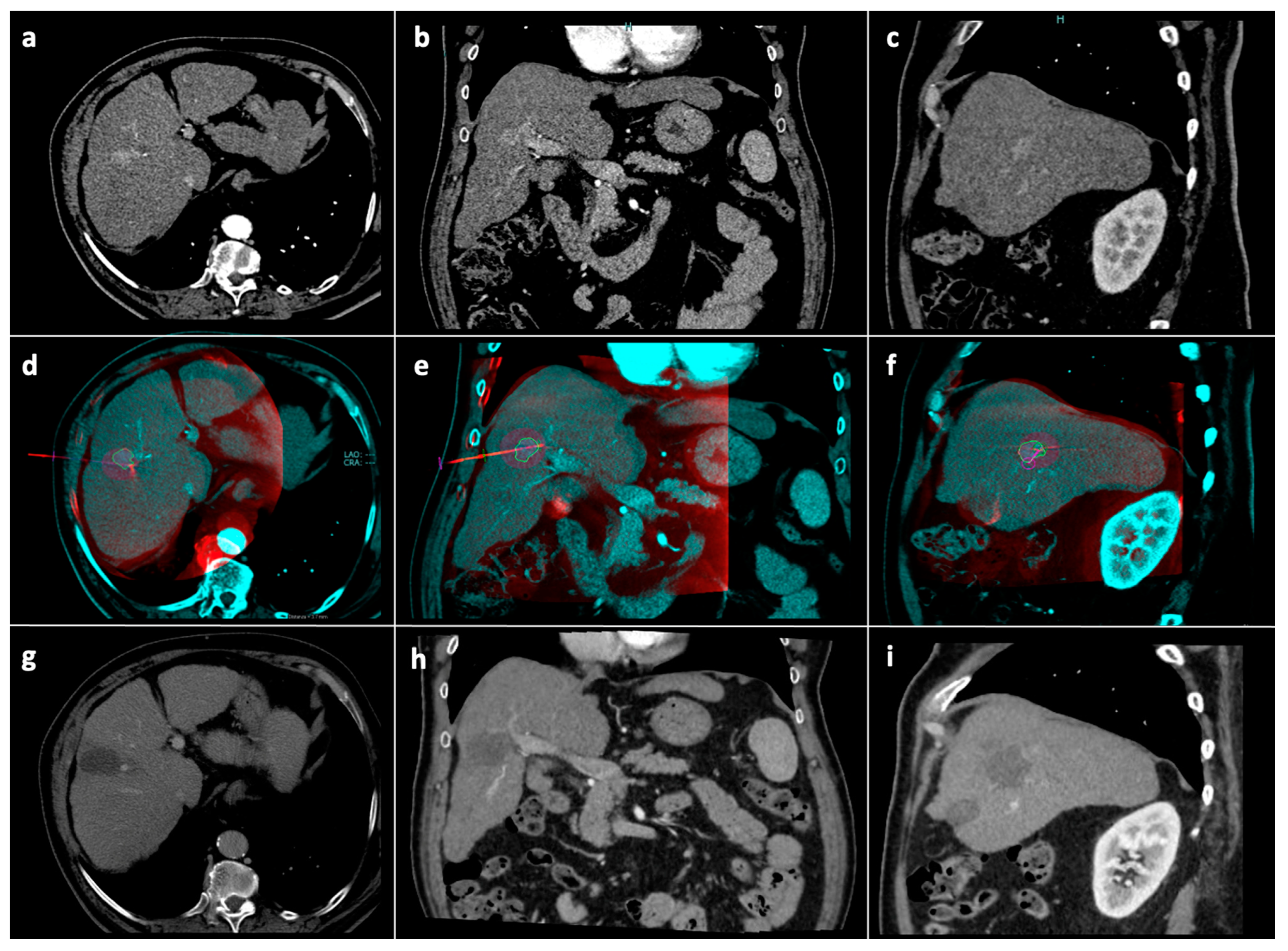
2.1. Procedure
2.2. Follow-Up
2.3. Outcomes
2.4. Statistical Analysis
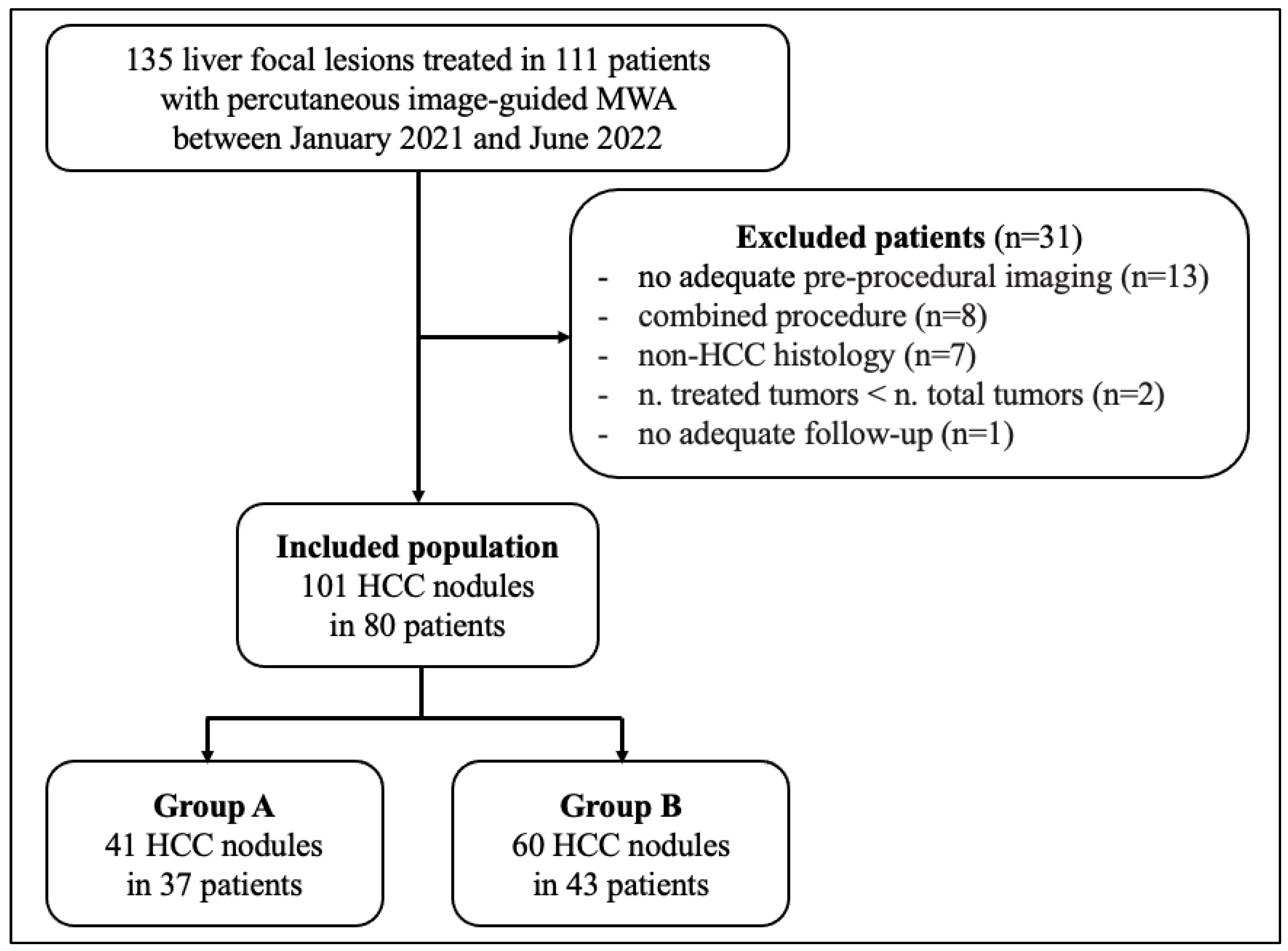
3. Results
3.1. Baseline Population Features
3.2. Protocol-Related Data
3.3. Complications
3.4. Outcome
3.4.1. Ablation Response at 1 Month According to mRECIST
3.4.2. Tumor Response
3.4.3. Patient Response
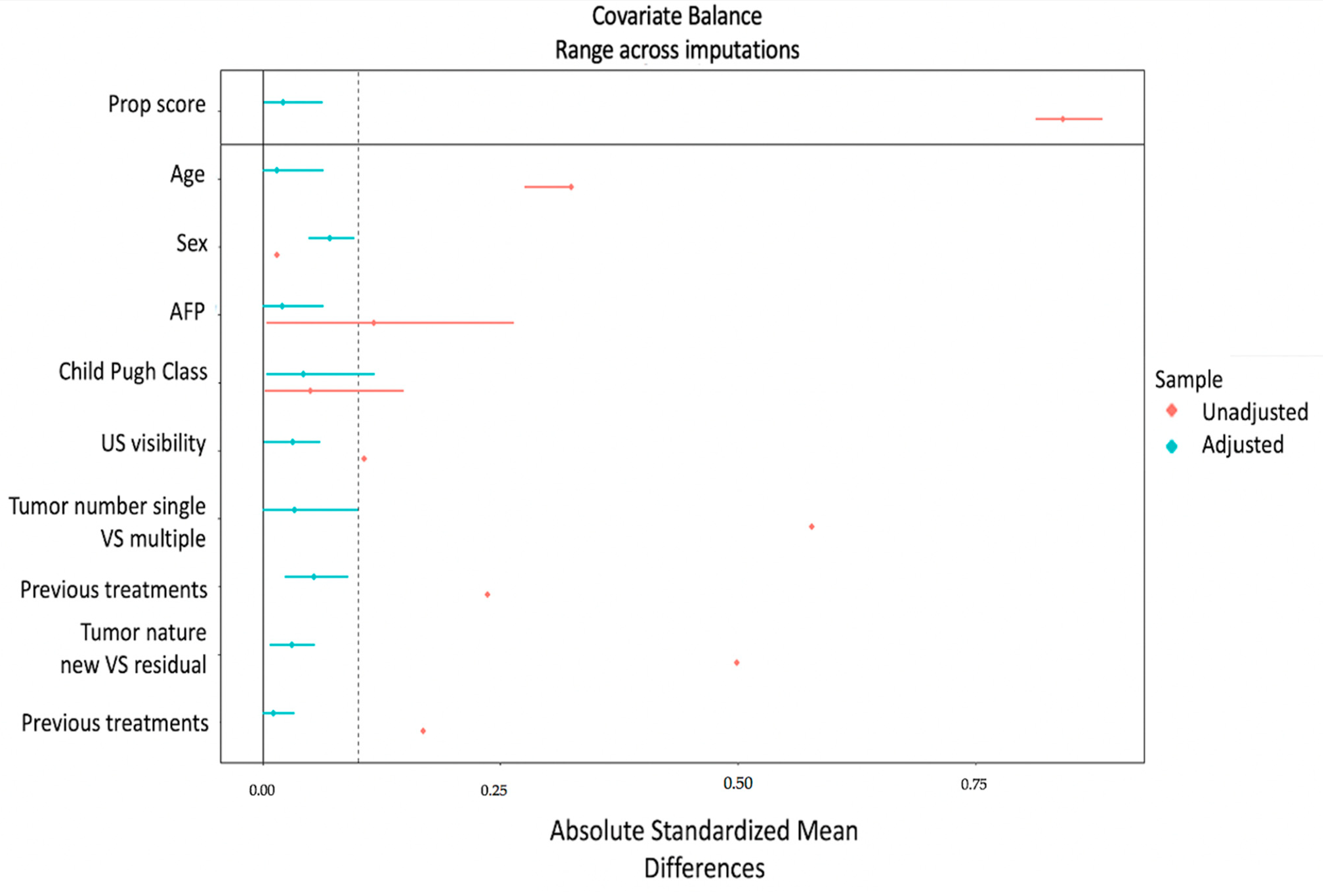
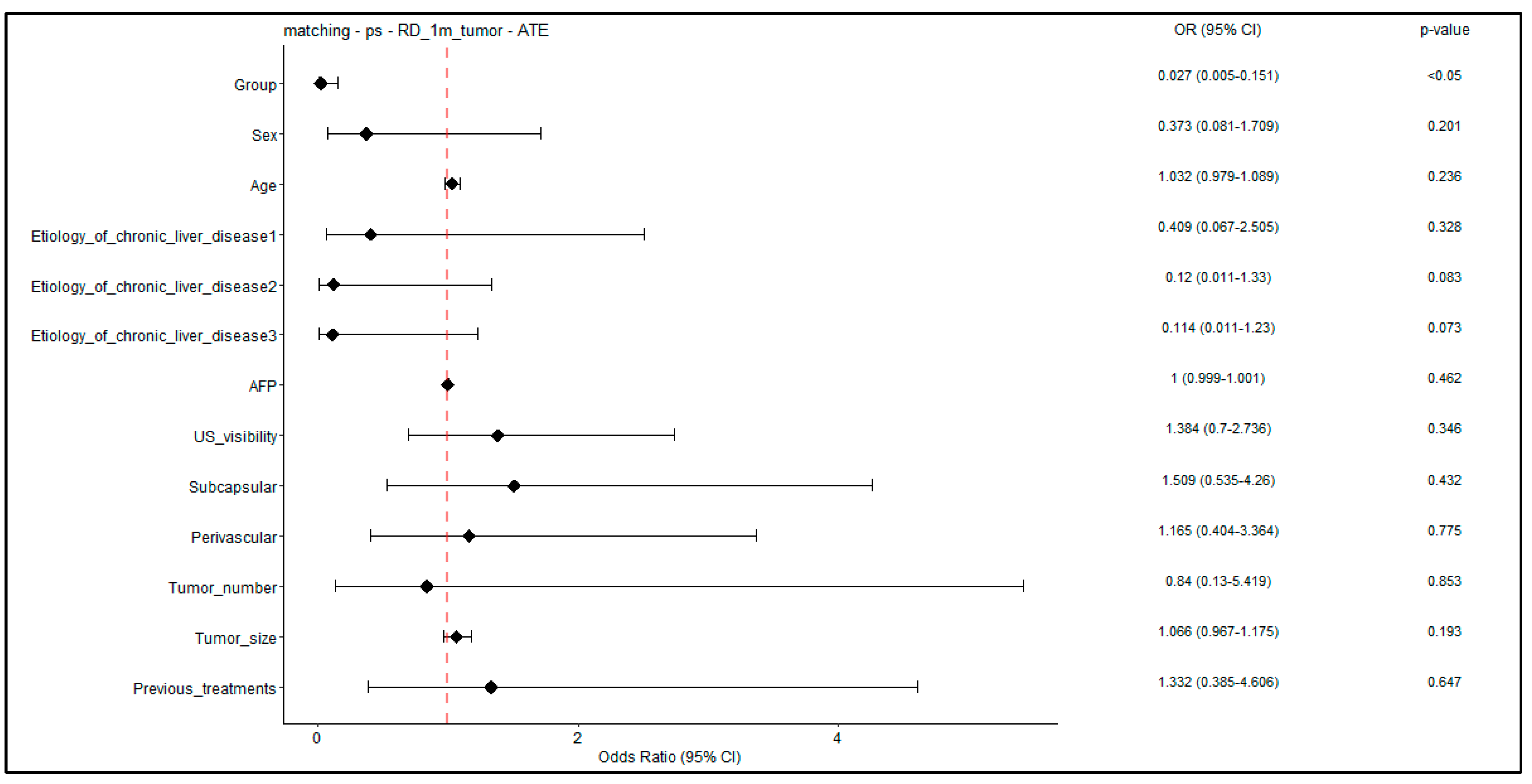
3.4.4. Tumor-Level Analysis: Propensity Score Weighting—1-Month RD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Ahmed, M.; Liu, Z.; Humphries, S.; Goldberg, S.N. Computer modeling of the combined effects of perfusion, electrical conductivity, and thermal conductivity on tissue heating patterns in radiofrequency tumor ablation. Int. J. Hyperth. 2008, 24, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Brace, C.L. Radiofrequency and Microwave Ablation of the Liver, Lung, Kidney, and Bone: What Are the Differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef]
- Lucatelli, P.; Argirò, R.; Crocetti, L.; Rocco, B.; Bozzi, E.; Gasparrini, F.; Tanzilli, A.; Catalano, C.; Iezzi, R. Percutaneous Thermal Segmentectomy: Proof of Concept. Cardiovasc. Interv. Radiol. 2022, 45, 665–676. [Google Scholar] [CrossRef]
- Aubé, C.; Schmidt, D.; Brieger, J.; Schenk, M.; Kroeber, S.; Vielle, B.; Claussen, C.D.; Goldberg, S.N.; Pereira, P.L. Influence of NaCl concentrations on coagulation, temperature, and electrical conductivity using a perfusion radiofrequency ablation system: An ex vivo experimental study. Cardiovasc. Interv. Radiol. 2007, 30, 92–97. [Google Scholar] [CrossRef]
- Lu, D.S.; Raman, S.S.; Vodopich, D.J.; Wang, M.; Sayre, J.; Lassman, C. Effect of vessel size on creation of hepatic radiofrequency lesions in pigs: Assessment of the “heat sink” effect. Am. J. Roentgenol. 2002, 178, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-S.; Rhim, H.; Cho, O.K.; Koh, B.H.; Kim, Y. Intrahepatic recurrence after percutaneous radiofrequency ablation of hepatocellular carcinoma: Analysis of the pattern and risk factors. Eur. J. Radiol. 2006, 59, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.B.; Silverman, S.G. Imaging in interventional oncology. Radiology 2010, 257, 624–640. [Google Scholar] [CrossRef]
- Orth, R.C.; Wallace, M.J.; Kuo, M.D. C-arm cone-beam CT: General principles and technical considerations for use in interventional radiology. J. Vasc. Interv. Radiol. 2008, 19, 814–820. [Google Scholar] [CrossRef]
- Iwazawa, J.; Hashimoto, N.; Mitani, T.; Ohue, S. Fusion of intravenous contrast-enhanced C-arm CT and pretreatment imaging for ablation margin assessment of liver tumors: A preliminary study. Indian J. Radiol. Imaging 2012, 22, 251–253. [Google Scholar] [CrossRef]
- Abdel-Rehim, M.; Ronot, M.; Sibert, A.; Vilgrain, V. Assessment of liver ablation using cone beam computed tomography. World J. Gastroenterol. 2015, 21, 517–524. [Google Scholar] [CrossRef]
- Sutter, O.; Fihri, A.; Ourabia-Belkacem, R.; Sellier, N.; Diallo, A.; Seror, O. Real-time 3D virtual target fluoroscopic display for challenging hepatocellular carcinoma ablations using cone beam CT. Technol. Cancer Res. Treat. 2018, 17, 1533033818789634. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Buy, X.; Alberti, N.; Fonck, M.; Grasso, R.F.; Palussière, J. Flat-Panel Cone-Beam Ct-Guided Radiofrequency Ablation of Very Small (≤1.5 cm) Liver Tumors: Technical Note on a Preliminary Experience. Cardiovasc. Interv. Radiol. 2015, 38, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Monfardini, L.; Orsi, F.; Caserta, R.; Sallemi, C.; Della Vigna, P.; Bonomo, G.; Varano, G.; Solbiati, L.; Mauri, G. Ultrasound and cone beam CT fusion for liver ablation: Technical note. Int. J. Hyperth. 2018, 35, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Floridi, C.; Radaelli, A.; Pesapane, F.; Fumarola, E.M.; Lecchi, M.; Agostini, A.; Giovagnoni, A.; Carrafiello, G.; Wood, B. Clinical impact of cone beam computed tomography on iterative treatment planning during ultrasound-guided percutaneous ablation of liver malignancies. Med. Oncol. 2017, 34, 113. [Google Scholar] [CrossRef] [PubMed]
- Kono, M.; Inoue, T.; Kudo, M.; Chishina, H.; Arizumi, T.; Takita, M.; Kitai, S.; Yada, N.; Hagiwara, S.; Minami, Y.; et al. Radiofrequency ablation for hepatocellular carcinoma measuring 2 cm or smaller: Results and risk factors for local recurrence. Dig. Dis. 2014, 32, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Song, I.; Rhim, H.; Lim, H.K.; Kim, Y.-S.; Choi, D. Percutaneous radiofrequency ablation of hepatocellular carcinoma abutting the diaphragm and gastrointestinal tracts with the use of artificial ascites: Safety and technical efficacy in 143 patients. Eur. Radiol. 2009, 19, 2630–2640. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Yoshida, H.; Shiina, S.; Tateishi, R.; Teratani, T.; Omata, M. Artificial ascites technique for percutaneous radiofrequency ablation of liver cancer adjacent to the gastrointestinal tract. Br. J. Surg. 2006, 93, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Shen, Q.; Liu, P.; Xu, Z.; Wu, P.; Lu, Z.; Chen, Y.; Huang, B.; Qian, G. Microwave ablation for the treatment of hepatocellular carcinoma that met up-to-seven criteria: Feasibility, local efficacy and long-term outcomes. Eur. Radiol. 2017, 27, 3877–3887. [Google Scholar] [CrossRef]
- Lee, S.; Kang, T.W.; Cha, D.I.; Song, K.D.; Lee, M.W.; Rhim, H.; Lim, H.K.; Sinn, D.H.; Kim, J.M.; Kim, K. Radiofrequency ablation vs. surgery for perivascular hepatocellular carcinoma: Propensity score analyses of long-term outcomes. J. Hepatol. 2018, 69, 70–78. [Google Scholar] [CrossRef]
- Patel, I.J.; Rahim, S.; Davidson, J.C.; Hanks, S.E.; Tam, A.L.; Walker, T.G.; Wilkins, L.R.; Sarode, R.; Weinberg, I. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions—Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2019, 30, 1168–1184.e1. [Google Scholar] [CrossRef] [PubMed]
- Filippiadis, D.K.; Binkert, C.; Pellerin, O.; Hoffmann, R.T.; Krajina, A.; Pereira, P.L. Cirse Quality Assurance Document and Standards for Classification of Complications: The Cirse Classification System. Cardiovasc. Interv. Radiol. 2017, 40, 1141–1146. [Google Scholar] [CrossRef]
- Ahmed, M. Image-guided tumor ablation: Standardization of terminology and reporting Criteria—A 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]
- Puijk, R.S.; Ahmed, M.; Adam, A.; Arai, Y.; Arellano, R.; de Baère, T.; Bale, R.; Bellera, C.; Binkert, C.A.; Brace, C.L.; et al. Consensus guidelines for the definition of time-to-event end points in image-guided tumor ablation: Results of the SIO and DATECAN initiative. Radiology 2021, 301, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified recist (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.; Monette, G. Generalized Collinearity Diagnostics. J. Am. Stat. Assoc. 1992, 87, 178–183. [Google Scholar] [CrossRef]
- Leyrat, C.; Seaman, S.R.; White, I.R.; Douglas, I.; Smeeth, L.; Kim, J.; Resche-Rigon, M.; Carpenter, J.R.; Williamson, E.J. Propensity score analysis with partially observed covariates: How should multiple imputation be used? Stat. Methods Med. Res. 2019, 28, 3–19. [Google Scholar] [CrossRef]
- Benedetto, U.; Head, S.J.; Angelini, G.D.; Blackstone, E.H. Statistical primer: Propensity score matching and its alternatives. Eur. J. Cardio-Thorac. Surg. 2018, 53, 1112–1117. [Google Scholar] [CrossRef]
- Koda, M.; Ueki, M.; Maeda, Y.; Mimura, K.I.; Okamoto, K.; Matsunaga, Y.; Kawakami, M.; Hosho, K.; Murawaki, Y. Percutaneous sonographically guided radiofrequency ablation with artificial pleural effusion for hepatocellular carcinoma located under the diaphragm. Am. J. Roentgenol. 2004, 183, 583–588. [Google Scholar] [CrossRef]
- Lee, M.W.; Kim, Y.J.; Park, H.S.; Yu, N.C.; Jung, S.I.; Ko, S.Y.; Jeon, H.J. Targeted sonography for small hepatocellular carcinoma discovered by CT or MRI: Factors affecting sonographic detection. Am. J. Roentgenol. 2010, 194, W396–W400. [Google Scholar] [CrossRef]
- Rhim, H.; Mi, H.L.; Kim, Y.S.; Choi, D.; Lee, W.J.; Lim, H.K. Planning sonography to assess the feasibility of percutaneous radiofrequency ablation of hepatocellular carcinomas. Am. J. Roentgenol. 2008, 190, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Cova, L.; de Beni, S.; Ierace, T.; Tondolo, T.; Cerri, A.; Goldberg, S.N.; Solbiati, L. Real-Time US-CT/MRI Image Fusion for Guidance of Thermal Ablation of Liver Tumors Undetectable with US: Results in 295 Cases. Cardiovasc. Interv. Radiol. 2015, 38, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Song, K.D.; Lee, M.W.; Rhim, H.; Cha, D.I.; Chong, Y.; Lim, H.K. Fusion imaging-guided radiofrequency ablation for hepatocellular carcinomas not visible on conventional ultrasound. Am. J. Roentgenol. 2013, 201, 1141–1147. [Google Scholar] [CrossRef]
- Lee, M.W.; Rhim, H.; Cha, D.I.; Kim, Y.J.; Choi, D.; Lim, H.K. Percutaneous radiofrequency ablation of hepatocellular carcinoma: Fusion imaging guidance for management of lesions with poor conspicuity at conventional sonography. Am. J. Roentgenol. 2012, 198, 1438–1444. [Google Scholar] [CrossRef]
- Lim, S.; Lee, M.W.; Rhim, H.; Cha, D.I.; Kang, T.W.; Min, J.H.; Song, K.D.; Choi, S.-Y.; Lim, H.K. Mistargeting after fusion imaging-guided percutaneous radiofrequency ablation of hepatocellular carcinomas. J. Vasc. Interv. Radiol. 2014, 25, 307–314. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Lesions | New Lesions | Overall Response |
|---|---|---|
| CR | No | CR |
| PR | No | PR |
| SD | No | SD |
| PD | Yes or No | PD |
| Any | Yes | PD |
| Variable | Overall (101 HCCs, 80 pts) | Group A (41 HCCs, 37 pts) | Group B (60 HCCs, 43 pts) | p-Value |
|---|---|---|---|---|
| Age at enrollment (y; mean, range) a | 68 (38–88) | 72 (46–88) | 64 (38–87) | 0.002 |
| Male sex (%) a | 61 (76.2) | 28 (75.7) | 33 (76.7) | 1 |
| Liver cirrhosis (%) a | 79 (98.8) | 36 (97.3) | 43 (100.0) | 0.94 |
| Etiology of chronic liver disease a | 0.247 | |||
| Alcohol | 9 (11.2) | 5 (13.9) | 4 (9.5) | |
| Cryptogenic | 1 (1.2) | 0 (0.0) | 1 (2.4) | |
| HBV | 13 (16.7) | 3 (8.3) | 10 (23.8) | |
| HCV | 45 (57.7) | 21 (58.3) | 24 (57.1) | |
| NASH | 9 (11.5) | 6 (16.7) | 3 (7.1) | |
| PBC | 1 (1.3) | 1 (2.8) | 0 (0.0) | |
| Child–Pugh class (%) a | 0.881 | |||
| A | 72 (90.0) | 34 (91.9) | 38 (88.4) | |
| B | 8 (10.0) | 3 (8.1) | 5 (11.6) | |
| AFP (ng/mL; mean [IQR]) a | 182.1 [2.6, 27.0] | 305.8 [2.9, 24.1] | 61.7 [2.2, 27.0] | 0.408 |
| Previous liver treatments a | 47 (58.8) | 20 (54.1) | 27 (62.8) | 0.573 |
| Tumor number a | 0.195 | |||
| 1 | 63 (78.8) | 32 (86.5) | 31 (72.1) | 0.195 |
| 2–3 | 17 (21.2) | 5 (13.5) | 12 (27.9) | |
| Tumor size (mm; mean, range) b | 17.9 (10–38) | 18.8 (11–35) | 17.3 (10–38) | 0.205 |
| Tumor location (Couinaud segment, %) b | 0.129 | |||
| Segments I–II–III–IV | 22 (21.8) | 8 (19.5) | 14 (23.3) | |
| Segments V–VI | 29 (28.7) | 18 (43.9) | 11 (18.3) | |
| Segments VII–VIII | 50 (49.5) | 15 (36.6) | 35 (58.3) | |
| US visibility (%) b | 0.227 | |||
| Visible | 63 (62.4) | 25 (61.0) | 38 (63.3) | |
| Non- or poorly visible | 38 (37.6) | 16 (39.0) | 22 (36.6) | |
| Subcapsular b | 47 (46.5) | 13 (31.7) | 34 (56.7) | 0.023 |
| Pericholecystic b | 4 (4.0) | 2 (4.9) | 2 (3.3) | 1 |
| Adjacent to GI b | 3 (3.0) | 1 (2.4) | 2 (3.3) | 1 |
| Perivascular b | 38 (37.6) | 7 (17.1) | 31 (51.7) | 0.001 |
| Tumor nature b | ||||
| New | 66 (65.3) | 21 (51.2) | 45 (75.0) | |
| Residual tumor | 35 (34.7) | 20 (48.8) | 15 (25.0) | 0.024 |
| Comorbidities a | ||||
| Hypertension | 34 (42.5) | 16 (43.2) | 18 (41.9) | 1 |
| Diabetes | 22 (27.5) | 8 (21.6) | 14 (32.6) | 0.4 |
| Obesity | 8 (10.0) | 5 (13.5) | 3 (7.0) | 0.55 |
| COPD | 3 (3.8) | 3 (8.1) | 0 (0.0) | 0.189 |
| Cardiopathy | 8 (10.0) | 4 (10.8) | 4 (9.3) | 1 |
| Hemophilia | 6 (7.5) | 3 (8.1) | 3 (7.0) | 1 |
| Outcome at 1 Month (%) * | Group A (n = 37) | Group B (n = 43) | p-Value | |
|---|---|---|---|---|
| Local AR | 0.001 | |||
| CR | 34 (91.9) | 23 (53.5) | ||
| PR | 2 (5.4) | 6 (14.0) | ||
| SD | 0 (0.0) | 12 (27.9) | ||
| PD | 1 (2.7) | 2 (4.7) | ||
| New distant lesions | Yes | 5 (13.5) | 5 (11.6) | 1 |
| Overall AR | 0.004 | |||
| CR | 30 (81.1) | 22 (51.2) | ||
| PR | 1 (2.7) | 5 (11.6) | ||
| SD | 0 (0.0) | 10 (23.3) | ||
| PD | 6 (16.2) | 6 (14.0) | ||
| SD | 0 (0.0) | 10 (23.3) |
| Group A (n = 41) | Group B (n = 60) | p-Value | ||
|---|---|---|---|---|
| Outcome * | 1-month RD | 3 (7.3) | 22 (36.7) | 0.002 |
| 3-month LTP | 1 (2.4) | 2 (3.3) | 1 | |
| 6-month LTP a | 2 (4.9) | 4 (6.6) | 0.9 |
| Group A (n = 37) | Group B (n = 43) | p-Value | |||
|---|---|---|---|---|---|
| Outcome * | 1 month | RD | 3 (8.1) | 20 (46.5) | <0.001 |
| IDR | 5 (13.5) | 7 (16.3) | 0.763 | ||
| 3 months | LTP | 1 (2.7) | 2 (4.6) | 0.965 | |
| IDR a | 8 (21.6) | 12 (27.9) | 0.609 | ||
| 6 months | LTP a | 2 (5.4) | 4 (9.3) | 0.681 | |
| IDR a | 9 (24.3) | 15 (34.8) | 0.334 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biondetti, P.; Ierardi, A.M.; Casiraghi, E.; Caruso, A.; Grillo, P.; Carriero, S.; Lanza, C.; Angileri, S.A.; Sangiovanni, A.; Iavarone, M.; et al. Clinical Impact of a Protocol Involving Cone-Beam CT (CBCT), Fusion Imaging and Ablation Volume Prediction in Percutaneous Image-Guided Microwave Ablation in Patients with Hepatocellular Carcinoma Unsuitable for Standard Ultrasound (US) Guidance. J. Clin. Med. 2023, 12, 7598. https://doi.org/10.3390/jcm12247598
Biondetti P, Ierardi AM, Casiraghi E, Caruso A, Grillo P, Carriero S, Lanza C, Angileri SA, Sangiovanni A, Iavarone M, et al. Clinical Impact of a Protocol Involving Cone-Beam CT (CBCT), Fusion Imaging and Ablation Volume Prediction in Percutaneous Image-Guided Microwave Ablation in Patients with Hepatocellular Carcinoma Unsuitable for Standard Ultrasound (US) Guidance. Journal of Clinical Medicine. 2023; 12(24):7598. https://doi.org/10.3390/jcm12247598
Chicago/Turabian StyleBiondetti, Pierpaolo, Anna Maria Ierardi, Elena Casiraghi, Alessandro Caruso, Pasquale Grillo, Serena Carriero, Carolina Lanza, Salvatore Alessio Angileri, Angelo Sangiovanni, Massimo Iavarone, and et al. 2023. "Clinical Impact of a Protocol Involving Cone-Beam CT (CBCT), Fusion Imaging and Ablation Volume Prediction in Percutaneous Image-Guided Microwave Ablation in Patients with Hepatocellular Carcinoma Unsuitable for Standard Ultrasound (US) Guidance" Journal of Clinical Medicine 12, no. 24: 7598. https://doi.org/10.3390/jcm12247598
APA StyleBiondetti, P., Ierardi, A. M., Casiraghi, E., Caruso, A., Grillo, P., Carriero, S., Lanza, C., Angileri, S. A., Sangiovanni, A., Iavarone, M., Guzzardi, G., & Carrafiello, G. (2023). Clinical Impact of a Protocol Involving Cone-Beam CT (CBCT), Fusion Imaging and Ablation Volume Prediction in Percutaneous Image-Guided Microwave Ablation in Patients with Hepatocellular Carcinoma Unsuitable for Standard Ultrasound (US) Guidance. Journal of Clinical Medicine, 12(24), 7598. https://doi.org/10.3390/jcm12247598