


Diagnosis and Treatment in Unilateral Condylar Hyperplasia
 , , and
, , and 
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olate, S.; Netto, H.D.; Rodriguez-Chessa, J.; Alister, J.P.; de Albergaria-Barbosa, J.; de Moraes, M. Mandible condylar hyperplasia: A review of diagnosis and treatment protocol. Int. J. Clin. Exp. Med. 2013, 6, 727–737. [Google Scholar] [PubMed]
- Nolte, J.W.; Schreurs, R.; Karssemakers, L.H.E.; Tuinzing, D.B.; Becking, A.G. Demographic features in Unilateral Condylar Hyperplasia: An overview of 309 asymmetric cases and presentation of an algorithm. J. Craniomaxillofac. Surg. 2018, 46, 1484–1492. [Google Scholar] [CrossRef]
- Villanueva-Alcojol, L.; Monje, F.; González-García, R. Hyperplasia of the mandibular condyle: Clinical, histopathologic, and treatment considerations in a series of 36 patients. J. Oral Maxillofac. Surg. 2011, 69, 447–455. [Google Scholar] [CrossRef]
- Martin-Granizo, R.; Garcia-Rielo, J.M.; De la Sen, O.; Maniegas, L.; Berguer, A.; De Pedro, M. Correlation between single photon emission computed tomography and histopathologic findings in condylar hyperplasia of the temporomandibular joint. J. Craniomaxillofac. Surg. 2017, 45, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.H.; Leung, Y.Y. SPECT bone scintigraphy for the assessment of condylar growth activity in mandibular asymmetry: Is it accurate? Int. J. Oral Maxillofac. Surg. 2018, 47, 470–479. [Google Scholar] [CrossRef]
- Obwegeser, H.L.; Makek, M.S. Hemimandibular hyperplasia—Hemimandibular elongation. J. Maxillofac. Surg. 1986, 14, 183–208. [Google Scholar] [CrossRef] [PubMed]
- Wolford, L.M.; Movahed, R.; Perez, D.E. A classification system for conditions causing condylar hyperplasia. J. Oral Maxillofac. Surg. 2014, 72, 567–595. [Google Scholar] [CrossRef]
- Maniskas, S.; Ly, C.L.; Parsaei, Y.; Bruckman, K.C.; Steinbacher, D.M. Facial asymmetry in unilateral condylar hyperplasia: Comparing treatment for active versus burnt-out disease. Plast. Reconstr. Surg. 2020, 146, 439e–445e. [Google Scholar] [CrossRef] [PubMed]
- Higginson, J.A.; Bartram, A.C.; Banks, R.J.; Keith, D.J.W. Condylar hyperplasia: Current thinking. Br. J. Oral Maxillofac. Surg. 2018, 56, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Olate, S.; Almeida, A.; Alister, J.P.; Navarro, P.; Netto, H.D.; de Moraes, M. Facial asymmetry and condylar hyperplasia: Considerations for diagnosis in 27 consecutives patients. Int. J. Clin. Exp. Med. 2013, 6, 937–941. [Google Scholar] [PubMed]
- Zapata, S.; Medina, H.; Saravia, D.; Navarro, P.; Olate, S. Morphometric analysis of the mandible in patients with facial asymmetry associated to condylar hyperplasia. A panoramic radiography study. Int. J. Morphol. 2014, 32, 161–165. [Google Scholar] [CrossRef]
- Goulart, D.R.; Muñoz, P.; Cantín López, M.G.; de Moraes, M.; Olate, S. Comparative evaluation of condylar volume between patients with unilateral condylar hyperplasia and class III dentofacial deformity. J. Oral Maxillofac. Surg. 2017, 75, 180–188. [Google Scholar] [CrossRef]
- Karssemakers, L.H.E.; Nolte, J.W.; Tuinzing, D.B.; Langenbach, G.E.J.; Becking, A.G.; Raijmakers, P.G. Impact of bone volume upon condylar activity in patients with unilateral condylar hyperplasia. J. Oral Maxillofac. Surg. 2018, 76, 2177–2182. [Google Scholar] [CrossRef] [PubMed]
- Goulart, D.R.; Muñoz, P.; Olate, S.; de Moraes, M.; Fariña, R. No differences in morphological characteristics between hyperplastic condyle and class III condyle. Int. J. Oral Maxillofac. Surg. 2015, 44, 1281–1286. [Google Scholar] [CrossRef]
- Matteson, S.R.; Proffit, W.R.; Terry, B.C.; Staab, E.V.; Burkes, E.J., Jr. Bone scanning with 99mtechnetium phosphate to assess condylar hyperplasia. Report of two cases. Oral Surg. Oral Med. Oral Pathol. 1985, 60, 356–367. [Google Scholar] [CrossRef]
- Lippold, C.; Kruse-Losler, B.; Danesh, G.; Joos, U.; Meyer, U. Treatment of hemimandibular hyperplasia: The biological basis of condylectomy. Br. J. Oral Maxillofac. Surg. 2007, 45, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Karssemakers, L.H.; Nolte, J.W.; Tuinzing, D.B.; Langenbach, G.E.; Raijmakers, P.G.; Becking, A.G. Microcomputed tomographic analysis of human condyles in unilateral condylar hyperplasia: Increased cortical porosity and trabecular bone volume fraction with reduced mineralisation. Br. J. Oral Maxillofac. Surg. 2014, 52, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Fariña, R.A.; Becar, M.; Plaza, C.; Espinoza, I.; Franco, M.E. Correlation between single photon emission computed tomography, AgNOR count, and histomorphologic features in patients with active mandibular condylar hyperplasia. J. Oral Maxillofac. Surg. 2011, 69, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Saridin, C.P.; Raijmakers, P.G.; Al Shamma, S.; Tuinzing, D.B.; Becking, A.G. Comparison of different analytical methods used for analyzing SPECT scans of patients with unilateral condylar hyperactivity. Int. J. Oral Maxillofac. Surg. 2009, 38, 942–946. [Google Scholar] [CrossRef]
- Shintaku, W.H.; Venturin, J.S.; Langlais, R.P.; Clark, G.T. Imaging modalities to access bony tumors and hyperplasic reactions of the temporomandibular joint. J. Oral Maxillofac. Surg 2010, 68, 1911–1921. [Google Scholar] [CrossRef]
- Liu, P.; Shi, J. Is single-photon emission computed tomography/computed tomography superior to single-photon emission computed tomography in assessing unilateral condylar hyperplasia? J. Oral Maxillofac. Surg. 2019, 77, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- López Buitrago, D.F.; Muñoz Acosta, J.M.; Cárdenas-Perilla, R.A. Comparison of four methods for quantitative assessment of 99mTc-MDP SPECT in patients with suspected condylar hyperplasia. Rev. Esp. Med. Nucl. Imagen. Mol. 2019, 38, 72–79. [Google Scholar] [CrossRef] [PubMed]
- López, D.F.; Ríos Borrás, V.; Muñoz, J.M.; Cardenas-Perilla, R.; Almeida, L.E. SPECT/CT Correlation in the diagnosis of unilateral condilar hyperplasia. Diagnostics 2021, 11, 477. [Google Scholar] [CrossRef]
- Saridin, C.P.; Raijmakers, P.G.; Slootweg, P.J.; Tuinzing, D.B.; Becking, A.G.; van der Waal, I. Unilateral condylar hyperactivity: A histopathologic analysis of 47 patients. J. Oral Maxillofac. Surg. 2010, 68, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Vásquez, B.; Olate, S.; Cantín, M.; Sandoval, C.; Del Sol, M.; de Moraes, M. Histomorphometric analysis of unilateral condylar hyperplasia in the temporomandibular joint: The value of the condylar layer and cartilage island. Int. J. Oral Maxillofac. Surg. 2017, 46, 861–866. [Google Scholar] [CrossRef]
- Vásquez, B.; Olate, S.; Cantín, M.; Sandoval, C.; Fariña, R.; Del Sol, M. Histopathological analysis of unilateral condylar hyperplasia: Difficulties in diagnosis and characterization of the disease. Int. J. Oral Maxillofac. Surg. 2016, 45, 601–609. [Google Scholar] [CrossRef]
- Nitzan, D.W.; Katsnelson, A.; Bermanis, I.; Brin, I.; Casap, N. The clinical characteristics of condylar hyperplasia: Experience with 61 patients. J. Oral Maxillofac. Surg. 2008, 66, 312–318. [Google Scholar] [CrossRef]
- Buschang, P.H.; Gandini Júnior, L.G. Mandibular skeletal growth and modelling between 10 and 15 years of age. Eur. J. Orthod. 2002, 24, 69–79. [Google Scholar] [CrossRef]
- Olate, S.; Cantín, M.; Alister, J.P.; Uribe, F.; Navarro, P.; Olate, G.; de Moraes, M. Relación entre el tamaño condilar y la asimetría facial transversal en individuos con hiperplasia condilar [Relationship between condylar size and transverse facial asymmetry in subject with condylar hyperplasia]. Int. J. Morphol. 2013, 31, 937–941. [Google Scholar] [CrossRef]
- Muñoz, G.; Olate, S.; Cantín, M.; Vásquez, B.; Del Sol, M. TMJ in facial class III deformity. Condylar morphology relations. Int. J. Clin. Exp. Med. 2014, 15, 3113–3117. [Google Scholar]
- Rabie, A.B.; Dai, J.; Xu, R. Recombinant AAV-mediated VEGF gene therapy induces mandibular condylar growth. Gene Ther. 2007, 14, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Guddadararangiah, S. Case report: Unilateral condylar hyperplasia. F1000Research 2021, 10, 46. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test | Characteristics and Definition |
|---|---|
| Family medical record | Family or patient describes a progressive facial asymmetry, occurring in the last time |
| With or without any family with facial deformity or facial asymmetry | |
| Pain or noise in the affected condyle could be reported | |
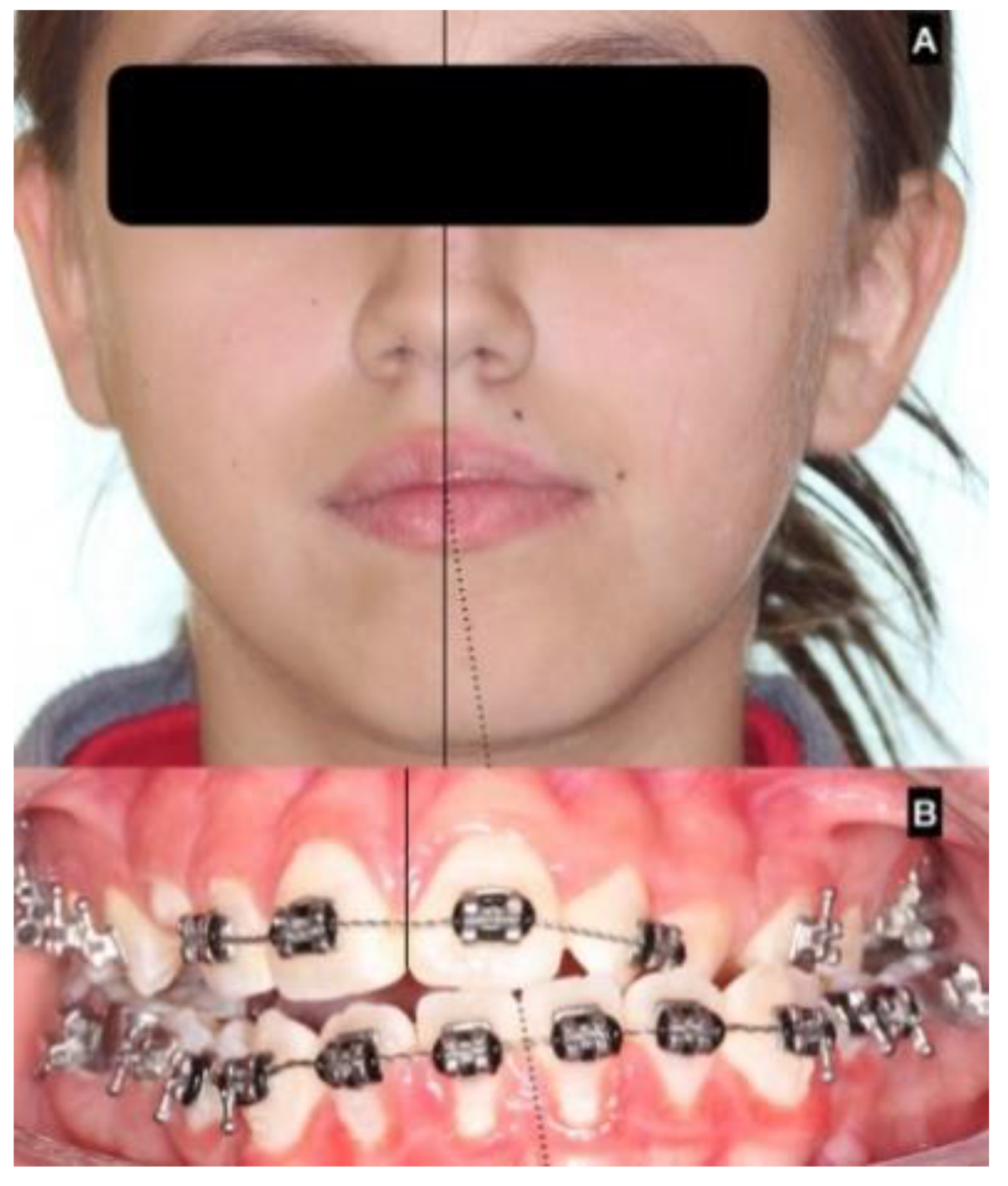
| Facial analysis | Chin midline deviation with the facial midline |
| Asymmetry in mandibular angles (vertical or horizontal differences) | |
| Dental conditions | Can be present with unilateral crossbite in the canine and/or molar area or unilateral open bite mainly in the posterior area |
| Progressive deviation of the dental midline with more than 4 mm. | |
| Trend to class III dental occlusion | |
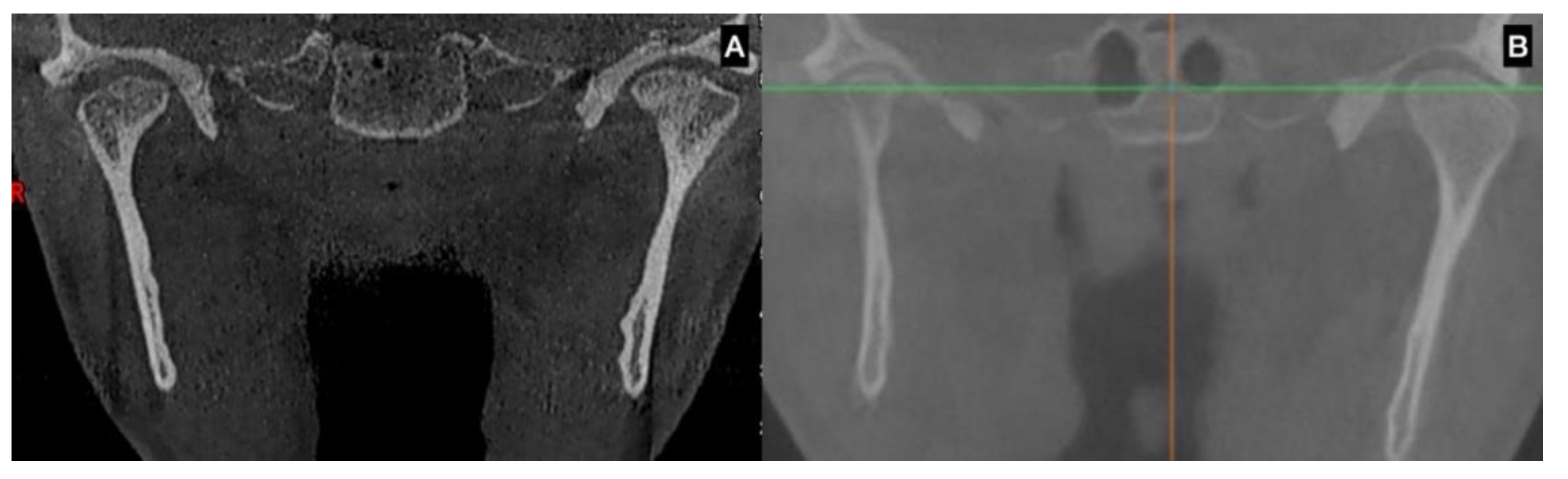
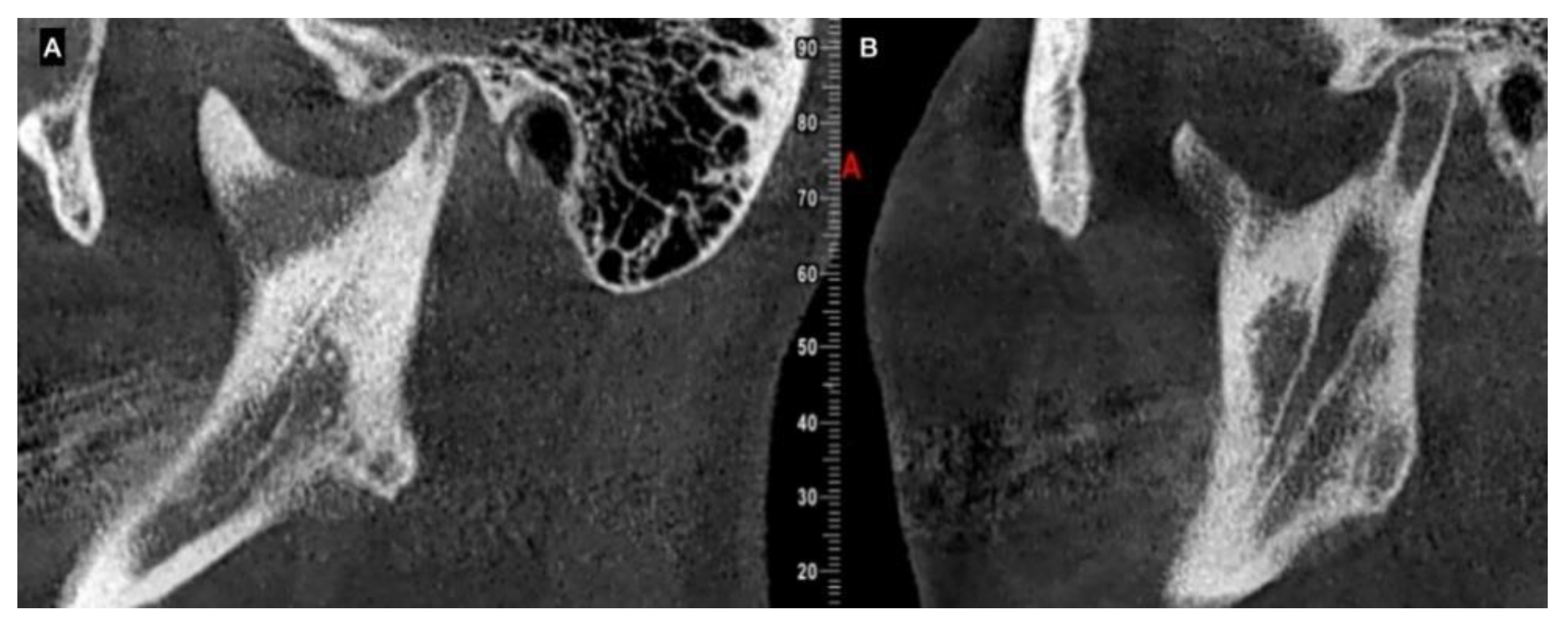
| CBCT | Augmentation in condylar size in comparison to the non-hyperplastic condyle |
| Lack in upper cortical line of the affected condyle in the upper area showing an active metabolism | |
| Augmentation in radiolucency in the affected condyle with an image related to poor density in some cases | |
| SPECT | Differences 10% in caption of the radioisotope between the hyperplastic and the non-hyperplastic condyle |
| Sex | Age | Affected Side | SPECT Differences | Secondary Surgery |
|---|---|---|---|---|
| F | 17 | R | 12 | NO |
| F | 19 | L | 6 | YES |
| F | 14 | L | 10 | NO |
| F | 22 | L | 16 | NO |
| F | 17 | L | 10 | NO |
| M | 22 | L | 14 | NO |
| F | 22 | R | 10 | NO |
| F | 14 | L | 18 | NO |
| F | 22 | L | 6 | NO |
| F | 12 | R | 48 | NO |
| F | 15 | R | 10 | NO |
| F | 14 | L | 14 | NO |
| F | 17 | L | 22 | NO |
| F | 14 | L | 10 | NO |
| F | 17 | L | 14 | NO |
| F | 22 | R | 18 | NO |
| M | 15 | R | 12 | NO |
| F | 10 | L | 12 | NO |
| M | 16 | L | 26 | NO |
| F | 18 | R | 24 | NO |
| F | 13 | R | 18 | NO |
| M | 18 | R | 16 | NO |
| Average | 16.81 | 15.72 | ||
| Standard Deviation | 3.55 | 8.92 |
| Sex | Age | Affected Side | SPECT Differences | Secondary Surgery |
|---|---|---|---|---|
| F | 15 | R | 16 | NO |
| F | 23 | R | 18 | YES |
| F | 21 | L | 16 | YES |
| F | 13 | L | 22 | NO |
| F | 45 | L | 28 | YES |
| F | 14 | L | 26 | NO |
| F | 41 | L | 10 | YES |
| F | 16 | L | 26 | YES |
| F | 20 | R | 24 | NO |
| M | 19 | L | 20 | NO |
| Average | 22.7 | 20.6 | ||
| Standard Deviation | 11.2 | 5.66 |
| Sex | Age | Affected Side | SPECT Differences | Secondary Surgery |
|---|---|---|---|---|
| F | 18 | L | 10 | YES |
| F | 14 | L | 16 | NO |
| F | 21 | L | 10 | NO |
| F | 16 | R | 20 | YES |
| F | 22 | L | 16 | YES |
| F | 14 | L | 22 | NO |
| F | 22 | R | 23 | YES |
| F | 18 | R | 24 | YES |
| F | 35 | R | 10 | YES |
| F | 14 | R | 26 | NO |
| F | 16 | R | 40 | NO |
| F | 17 | R | 14 | YES |
| F | 14 | R | 12 | NO |
| F | 16 | R | 12 | NO |
| F | 17 | R | 16 | NO |
| M | 22 | L | 28 | NO |
| M | 43 | L | 22 | YES |
| Average | 19.94 | 18.88 | ||
| Standard Deviation | 7.84 | 7.99 |
| Sex | Age | Affected Side | SPECT (R/L) | SPECT Differences | Clinical Type | Secondary Surgery |
|---|---|---|---|---|---|---|
| F | 10 | L | 44/56 | 12 | 1 | NO |
| F | 12 | R | 74/26 | 48 | 1 | NO |
| F | 13 | L | 39/61 | 22 | 2 | NO |
| F | 13 | R | 59/41 | 18 | 1 | NO |
| F | 14 | L | 42/58 | 16 | 3 | NO |
| F | 14 | L | 45/55 | 10 | 1 | NO |
| F | 14 | L | 41/59 | 18 | 1 | NO |
| M | 14 | L | 39/61 | 22 | 3 | NO |
| F | 14 | L | 43/57 | 14 | 1 | NO |
| F | 14 | L | 37/63 | 26 | 2 | NO |
| F | 14 | L | 45/55 | 10 | 1 | NO |
| F | 14 | R | 63/37 | 26 | 3 | NO |
| F | 14 | R | 56/44 | 12 | 3 | NO |
| F | 15 | R | 58/42 | 16 | 2 | NO |
| F | 15 | R | 55/45 | 10 | 1 | NO |
| M | 15 | R | 56/44 | 12 | 1 | NO |
| F | 16 | R | 60/40 | 20 | 3 | YES |
| F | 16 | R | 30/70 | 40 | 3 | NO |
| F | 16 | L | 37/63 | 26 | 2 | YES |
| M | 16 | L | 37/63 | 26 | 1 | NO |
| F | 16 | R | 56/44 | 12 | 3 | NO |
| Average | 14.23 | 19.8 | ||||
| Standard Deviation | 1.48 | 9.9 |
| Sex | Age | Affected Side | SPECT (R/L) | SPECT Differences | Clinical Type | Secondary Surgery |
|---|---|---|---|---|---|---|
| F | 17 | R | 56/44 | 12 | 1 | NO |
| F | 17 | L | 55/45 | 10 | 1 | NO |
| F | 17 | L | 39/61 | 22 | 1 | NO |
| F | 17 | R | 57/43 | 14 | 3 | YES |
| F | 17 | L | 43/57 | 14 | 1 | NO |
| F | 17 | R | 58/42 | 16 | 3 | NO |
| F | 18 | L | 45/55 | 10 | 3 | YES |
| F | 18 | R | 62/38 | 24 | 3 | YES |
| F | 18 | R | 62/38 | 24 | 1 | NO |
| M | 18 | R | 58/42 | 16 | 1 | NO |
| F | 19 | L | 47/53 | 6 | 1 | YES |
| M | 19 | L | 40/60 | 20 | 2 | NO |
| F | 20 | R | 62/38 | 24 | 2 | NO |
| F | 21 | L | 45/55 | 10 | 3 | NO |
| F | 21 | L | 58/42 | 16 | 2 | YES |
| F | 22 | L | 42/58 | 16 | 1 | NO |
| M | 22 | L | 43/57 | 14 | 1 | NO |
| F | 22 | R | 55/45 | 10 | 1 | NO |
| F | 22 | L | 42/58 | 16 | 3 | YES |
| F | 22 | L | 47/53 | 6 | 1 | NO |
| F | 22 | R | 61/39 | 23 | 3 | YES |
| F | 22 | R | 59/41 | 18 | 1 | NO |
| M | 22 | L | 36/64 | 28 | 3 | NO |
| F | 23 | R | 59/41 | 18 | 2 | YES |
| F | 35 | R | 55/45 | 10 | 3 | YES |
| F | 41 | L | 45/55 | 10 | 2 | YES |
| M | 43 | L | 39/61 | 22 | 3 | YES |
| F | 45 | L | 36/64 | 28 | 2 | YES |
| Average | 22.75 | 16.32 | ||||
| Standard Deviation | 7.98 | 6.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beltran, J.; Zaror, C.; Moya, M.P.; Netto, H.D.; Olate, S. Diagnosis and Treatment in Unilateral Condylar Hyperplasia. J. Clin. Med. 2023, 12, 1017. https://doi.org/10.3390/jcm12031017
Beltran J, Zaror C, Moya MP, Netto HD, Olate S. Diagnosis and Treatment in Unilateral Condylar Hyperplasia. Journal of Clinical Medicine. 2023; 12(3):1017. https://doi.org/10.3390/jcm12031017
Chicago/Turabian StyleBeltran, Jorge, Carlos Zaror, María Paz Moya, Henrique Duque Netto, and Sergio Olate. 2023. "Diagnosis and Treatment in Unilateral Condylar Hyperplasia" Journal of Clinical Medicine 12, no. 3: 1017. https://doi.org/10.3390/jcm12031017
APA StyleBeltran, J., Zaror, C., Moya, M. P., Netto, H. D., & Olate, S. (2023). Diagnosis and Treatment in Unilateral Condylar Hyperplasia. Journal of Clinical Medicine, 12(3), 1017. https://doi.org/10.3390/jcm12031017