
Validation of a Prediction Model for Acute Kidney Injury after Cardiac Surgery in a Retrospective Asian Cohort

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
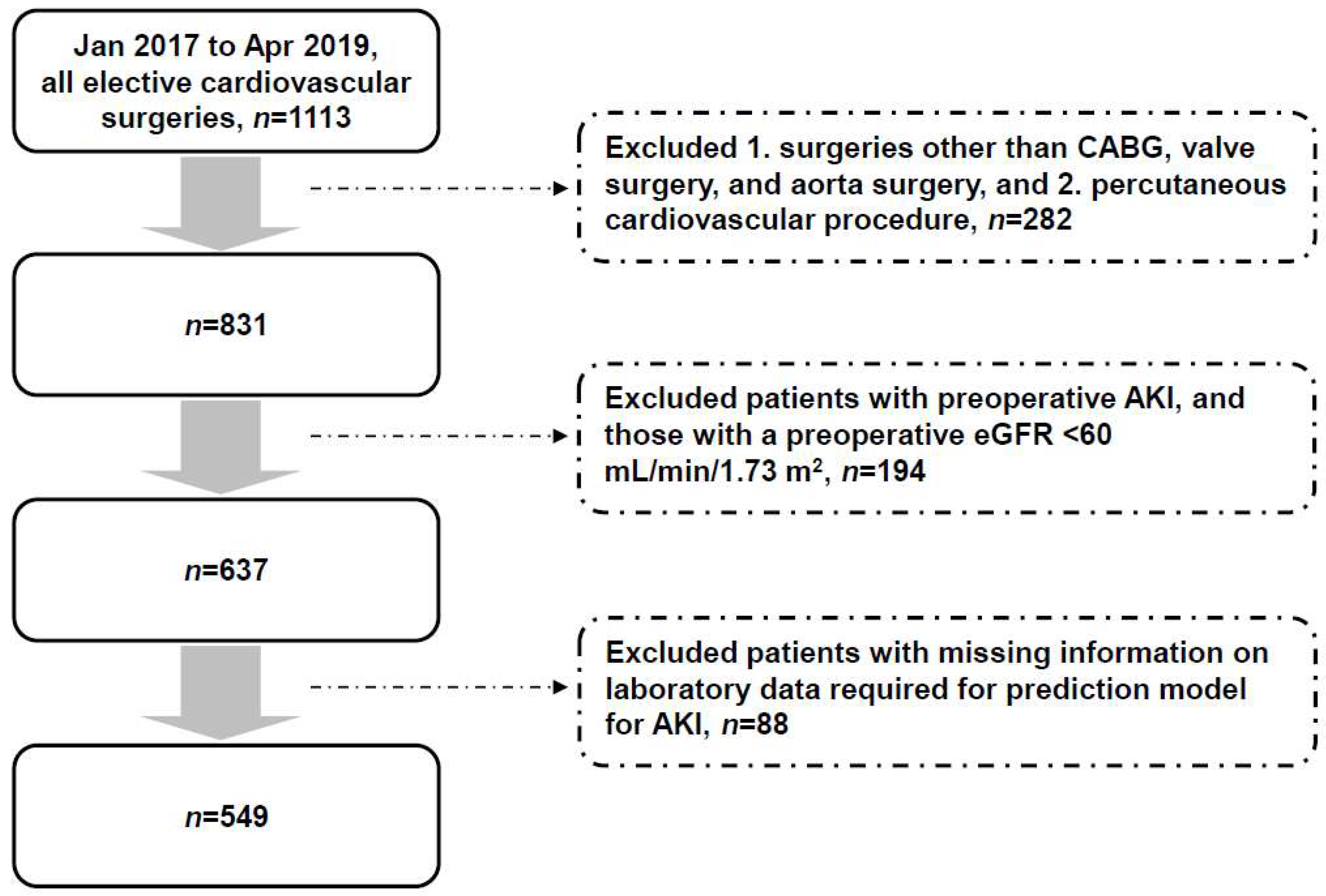
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Jaghbeer, M.; Dealmeida, D.; Bilderback, A.; Ambrosino, R.; Kellum, J.A. Clinical Decision Support for In-Hospital AKI. J. Am. Soc. Nephrol. 2018, 29, 654–660. [Google Scholar] [CrossRef]
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Wald, R.; Quinn, R.R.; Luo, J.; Li, P.; Scales, D.C.; Mamdani, M.M.; Ray, J.G.; University of Toronto Acute Kidney Injury Research Group. Chronic dialysis and death among survivors of acute kidney injury requiring dialysis. JAMA 2009, 302, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.J.; Go, A.S.; Chertow, G.M.; McCulloch, C.E.; Fan, D.; Ordoñez, J.D.; Hsu, C.Y. Dialysis-requiring acute renal failure increases the risk of progressive chronic kidney disease. Kidney Int. 2009, 76, 893–899. [Google Scholar] [CrossRef]
- See, E.J.; Jayasinghe, K.; Glassford, N.; Bailey, M.; Johnson, D.W.; Polkinghorne, K.R.; Toussaint, N.D.; Bellomo, R. Long-term risk of adverse outcomes after acute kidney injury: A systematic review and meta-analysis of cohort studies using consensus definitions of exposure. Kidney Int. 2019, 95, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Christianson, A.; Freyberg, R.; Almenoff, P.; Render, M.L. Incidence and outcomes of acute kidney injury in intensive care units: A Veterans Administration study. Crit. Care Med. 2009, 37, 2552–2558. [Google Scholar] [CrossRef] [PubMed]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Zarbock, A.; Weiss, R.; Albert, F.; Rutledge, K.; Kellum, J.A.; Bellomo, R.; Grigoryev, E.; Candela-Toha, A.M.; Demir, Z.A.; Legros, V.; et al. Epidemiology of surgery associated acute kidney injury (EPIS-AKI): A prospective international observational multi-center clinical study. Intensive Care Med. 2023, 49, 1441–1455. [Google Scholar] [CrossRef]
- Meersch, M.; Weiss, R.; Strauß, C.; Albert, F.; Booke, H.; Forni, L.; Pittet, J.F.; Kellum, J.A.; Rosner, M.; Mehta, R.; et al. Acute kidney disease beyond day 7 after major surgery: A secondary analysis of the EPIS-AKI trial. Intensive Care Med. 2024, 50, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Grams, M.E.; Sang, Y.; Coresh, J.; Ballew, S.; Matsushita, K.; Molnar, M.Z.; Szabo, Z.; Kalantar-Zadeh, K.; Kovesdy, C.P. Acute Kidney Injury After Major Surgery: A Retrospective Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. 2016, 67, 872–880. [Google Scholar] [CrossRef]
- Rydén, L.; Sartipy, U.; Evans, M.; Holzmann, M.J. Acute kidney injury after coronary artery bypass grafting and long-term risk of end-stage renal disease. Circulation 2014, 130, 2005–2011. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.R.; Zhu, J.M.; Jiang, J.; Ding, X.Q.; Fang, Y.; Shen, B.; Liu, Z.H.; Zou, J.Z.; Liu, L.; Wang, C.S.; et al. Risk Factors for Long-Term Mortality and Progressive Chronic Kidney Disease Associated with Acute Kidney Injury After Cardiac Surgery. Medicine 2015, 94, e2025. [Google Scholar] [CrossRef]
- Lange, H.W.; Aeppli, D.M.; Brown, D.C. Survival of patients with acute renal failure requiring dialysis after open heart surgery: Early prognostic indicators. Am. Heart J. 1987, 113, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Levy, E.M.; Hammermeister, K.E.; Grover, F.; Daley, J. Independent association between acute renal failure and mortality following cardiac surgery. Am. J. Med. 1998, 104, 343–348. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, J.B.; Shaw, A.D.; Billings, F.T., 4th. Acute kidney injury following cardiac surgery: Current understanding and future directions. Crit. Care 2016, 20, 187. [Google Scholar] [CrossRef]
- Wang, Y.; Bellomo, R. Cardiac surgery-associated acute kidney injury: Risk factors, pathophysiology and treatment. Nat. Rev. Nephrol. 2017, 13, 697–711. [Google Scholar] [CrossRef]
- Demirjian, S.; Bashour, C.A.; Shaw, A.; Schold, J.D.; Simon, J.; Anthony, D.; Soltesz, E.; Gadegbeku, C.A. Predictive Accuracy of a Perioperative Laboratory Test-Based Prediction Model for Moderate to Severe Acute Kidney Injury After Cardiac Surgery. JAMA 2022, 327, 956–964. [Google Scholar] [CrossRef]
- Hoste, E.A.J.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef]
- Grams, M.E.; Matsushita, K.; Sang, Y.; Estrella, M.M.; Foster, M.C.; Tin, A.; Kao, W.H.; Coresh, J. Explaining the racial difference in AKI incidence. J. Am. Soc. Nephrol. 2014, 25, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.O.; Balogun, R.A. The Effects of Race on Acute Kidney Injury. J. Clin. Med. 2022, 11, 5822. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Schurle, A.; Koyner, J.L. CSA-AKI: Incidence, Epidemiology, Clinical Outcomes, and Economic Impact. J. Clin. Med. 2021, 10, 5746. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Arrigain, S.; Worley, S.; Yared, J.P.; Paganini, E.P. A clinical score to predict acute renal failure after cardiac surgery. J. Am. Soc. Nephrol. 2005, 16, 162–168. [Google Scholar] [CrossRef]
- Mehta, R.H.; Grab, J.D.; O’Brien, S.M.; Bridges, C.R.; Gammie, J.S.; Haan, C.K.; Ferguson, T.B.; Peterson, E.D. Society of Thoracic Surgeons National Cardiac Surgery Database Investigators. Bedside tool for predicting the risk of postoperative dialysis in patients undergoing cardiac surgery. Circulation 2006, 114, 2208–2216. [Google Scholar] [CrossRef] [PubMed]
- Wijeysundera, D.N.; Karkouti, K.; Dupuis, J.Y.; Rao, V.; Chan, C.T.; Granton, J.T.; Beattie, W.S. Derivation and validation of a simplified predictive index for renal replacement therapy after cardiac surgery. JAMA 2007, 297, 1801–1809. [Google Scholar] [CrossRef]
- Shah, S.; Leonard, A.C.; Harrison, K.; Meganathan, K.; Christianson, A.L.; Thakar, C.V. Mortality and Recovery Associated with Kidney Failure due to Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2020, 15, 995–1006. [Google Scholar] [CrossRef] [PubMed]
- Saw, K.M.E.; Ng, R.G.R.; Chan, S.P.; Ang, Y.H.; Ti, L.K.; Chew, T.H.S. Association of genetic polymorphisms with acute kidney injury after cardiac surgery in a Southeast Asian population. PLoS ONE 2019, 14, e0213997. [Google Scholar] [CrossRef]
- Stafford-Smith, M.; Podgoreanu, M.; Swaminathan, M.; Phillips-Bute, B.; Mathew, J.P.; Hauser, E.H.; Winn, M.P.; Milano, C.; Nielsen, D.M.; Smith, M.; et al. Perioperative Genetics and Safety Outcomes Study (PEGASUS) Investigative Team. Association of genetic polymorphisms with risk of renal injury after coronary bypass graft surgery. Am. J. Kidney Dis. 2005, 45, 519–530. [Google Scholar] [CrossRef]
- Chandramohan, D.; Konda, R.; Pujari, A.; Avula, S.; Palleti, S.K.; Jena, N.; Naik, R.; Bali, A. Acute kidney injury after robot-assisted laparoscopic prostatectomy: A meta-analysis. Int. J. Med. Robot. 2024, 20, e2630. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.E.; Yavas, S.; Segal, M.S.; Schold, J.D.; Tribble, C.G.; Layon, A.J.; Bihorac, A. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation 2009, 119, 2444–2453. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Katz, N.; Ariyanon, W.; Blanca-Martos, L.; Adýbelli, Z.; Giuliani, A.; Danesi, T.H.; Kim, J.C.; Nayak, A.; Neri, M.; et al. Cardiac surgery-associated acute kidney injury. Cardiorenal Med. 2013, 3, 178–199. [Google Scholar] [CrossRef]
- Vazquez, M.A.; Oliver, G.; Amarasingham, R.; Sundaram, V.; Chan, K.; Ahn, C.; Zhang, S.; Bickel, P.; Parikh, S.M.; Wells, B.; et al. Pragmatic Trial of Hospitalization Rate in Chronic Kidney Disease. N. Engl. J. Med. 2024, 390, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGO guidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef] [PubMed]
- Zarbock, A.; Küllmar, M.; Ostermann, M.; Lucchese, G.; Baig, K.; Cennamo, A.; Rajani, R.; McCorkell, S.; Arndt, C.; Wulf, H.; et al. Prevention of Cardiac Surgery-Associated Acute Kidney Injury by Implementing the KDIGO Guidelines in High-Risk Patients Identified by Biomarkers: The PrevAKI-Multicenter Randomized Controlled Trial. Anesth. Analg. 2021, 133, 292–302. [Google Scholar] [CrossRef]
- Chew, S.T.; Ng, R.R.; Liu, W.; Chow, K.Y.; Ti, L.K. Acute kidney injury increases the risk of end-stage renal disease after cardiac surgery in an Asian population: A prospective cohort study. BMC Nephrol. 2017, 18, 60. [Google Scholar] [CrossRef] [PubMed]
- Lattenist, L.; Lechner, S.M.; Messaoudi, S.; Le Mercier, A.; El Moghrabi, S.; Prince, S.; Bobadilla, N.A.; Kolkhof, P.; Jaisser, F.; Barrera-Chimal, J. Nonsteroidal Mineralocorticoid Receptor Antagonist Finerenone Protects Against Acute Kidney Injury-Mediated Chronic Kidney Disease: Role of Oxidative Stress. Hypertension 2017, 69, 870–878. [Google Scholar] [CrossRef]
- Pan, H.C.; Chen, J.Y.; Chen, H.Y.; Yeh, F.Y.; Huang, T.T.; Sun, C.Y.; Wang, S.I.; Wei, J.C.; Wu, V.C. Sodium-Glucose Cotransport Protein 2 Inhibitors in Patients with Type 2 Diabetes and Acute Kidney Disease. JAMA Netw. Open 2024, 7, e2350050. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| 1. Mild: increase in sCr by ≥0.3 mg/dL within 48 h after surgery or increase in sCr to ≥1.5 times baseline within 7 days after surgery |
| 2. Moderate to severe: sCr increase by ≥2 times baseline or increase to ≥4 mg/dL |
| A. Within 72 h after surgery |
| B. Within 14 days after surgery |
| Preoperative serum creatinine |
| Perioperative change in serum creatinine |
| Postoperative serum albumin |
| Postoperative blood urea nitrogen |
| Postoperative serum potassium |
| Postoperative serum sodium |
| Postoperative serum bicarbonate |
| Duration in hours from end of surgery to postoperative metabolic panel |
| Number of patients | 549 |
| Age, years | 61.6 ± 12.6 |
| Male, n (%) | 386 (70.3) |
| Body mass index, kg/m2 | 24.9 ± 3.9 |
| Systolic blood pressure, mm Hg | 138 ± 24 |
| Diastolic blood pressure, mm Hg | 79 ± 14 |
| Smoking, n (%) | 93 (16.9) |
| Hypertension, n (%) | 244 (44.4) |
| Coronary artery disease, n (%) | 145 (26.4) |
| Diabetes, n (%) | 112 (20.4) |
| Surgical procedure, n (%) | |
| Coronary artery bypass graft | 192 (35.0) |
| Valve surgery | 197 (35.9) |
| Aorta surgery | 160 (29.1) |
| Preoperative serum creatinine, mg/dL | 0.89 ± 0.19 |
| Preoperative eGFR, mL/min/1.73 m2 | 84.9 ± 15.2 |
| Acute Kidney Injury | Patients with Event, n (%) | Area under the ROC Curve |
|---|---|---|
| a Mild | 53 (9.7) | 0.928 (95% CI 0.884 to 0.973) |
| b Moderate to severe: within 72 h after surgery | 13 (2.4) | 0.999 (95% CI 0.997 to 1.000) |
| b Moderate to severe: within 14 days after surgery | 19 (3.5) | 0.997 (95% CI 0.994 to 1.000) |
| a Mild Acute Kidney Injury | Area under the ROC Curve | p |
|---|---|---|
| Age < 65 years, n = 306 | 0.946 (95% CI 0.898 to 0.994) | <0.001 |
| Age ≥ 65 years, n = 243 | 0.910 (95% CI 0.832 to 0.987) | <0.001 |
| Male, n = 386 | 0.955 (95% CI 0.913 to 0.998) | <0.001 |
| Female, n = 163 | 0.852 (95% CI 0.735 to 0.968) | <0.001 |
| Hypertension (−), n = 305 | 0.941 (95% CI 0.894 to 0.987) | <0.001 |
| Hypertension (+), n = 244 | 0.911 (95% CI 0.824 to 0.999) | <0.001 |
| Diabetes (−), n = 437 | 0.920 (95% CI 0.867 to 0.972) | <0.001 |
| Diabetes (+), n = 112 | 0.954 (95% CI 0.871 to 1.000) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, P.-H.; Wang, J.-S.; Shen, C.-H. Validation of a Prediction Model for Acute Kidney Injury after Cardiac Surgery in a Retrospective Asian Cohort. J. Clin. Med. 2024, 13, 2740. https://doi.org/10.3390/jcm13102740
Tsai P-H, Wang J-S, Shen C-H. Validation of a Prediction Model for Acute Kidney Injury after Cardiac Surgery in a Retrospective Asian Cohort. Journal of Clinical Medicine. 2024; 13(10):2740. https://doi.org/10.3390/jcm13102740
Chicago/Turabian StyleTsai, Pei-Hsin, Jun-Sing Wang, and Ching-Hui Shen. 2024. "Validation of a Prediction Model for Acute Kidney Injury after Cardiac Surgery in a Retrospective Asian Cohort" Journal of Clinical Medicine 13, no. 10: 2740. https://doi.org/10.3390/jcm13102740
APA StyleTsai, P.-H., Wang, J.-S., & Shen, C.-H. (2024). Validation of a Prediction Model for Acute Kidney Injury after Cardiac Surgery in a Retrospective Asian Cohort. Journal of Clinical Medicine, 13(10), 2740. https://doi.org/10.3390/jcm13102740