
Recurrent Urinary Stone Formers: Imaging Assessment and Endoscopic Treatment Strategies: A Systematic Search and Review

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
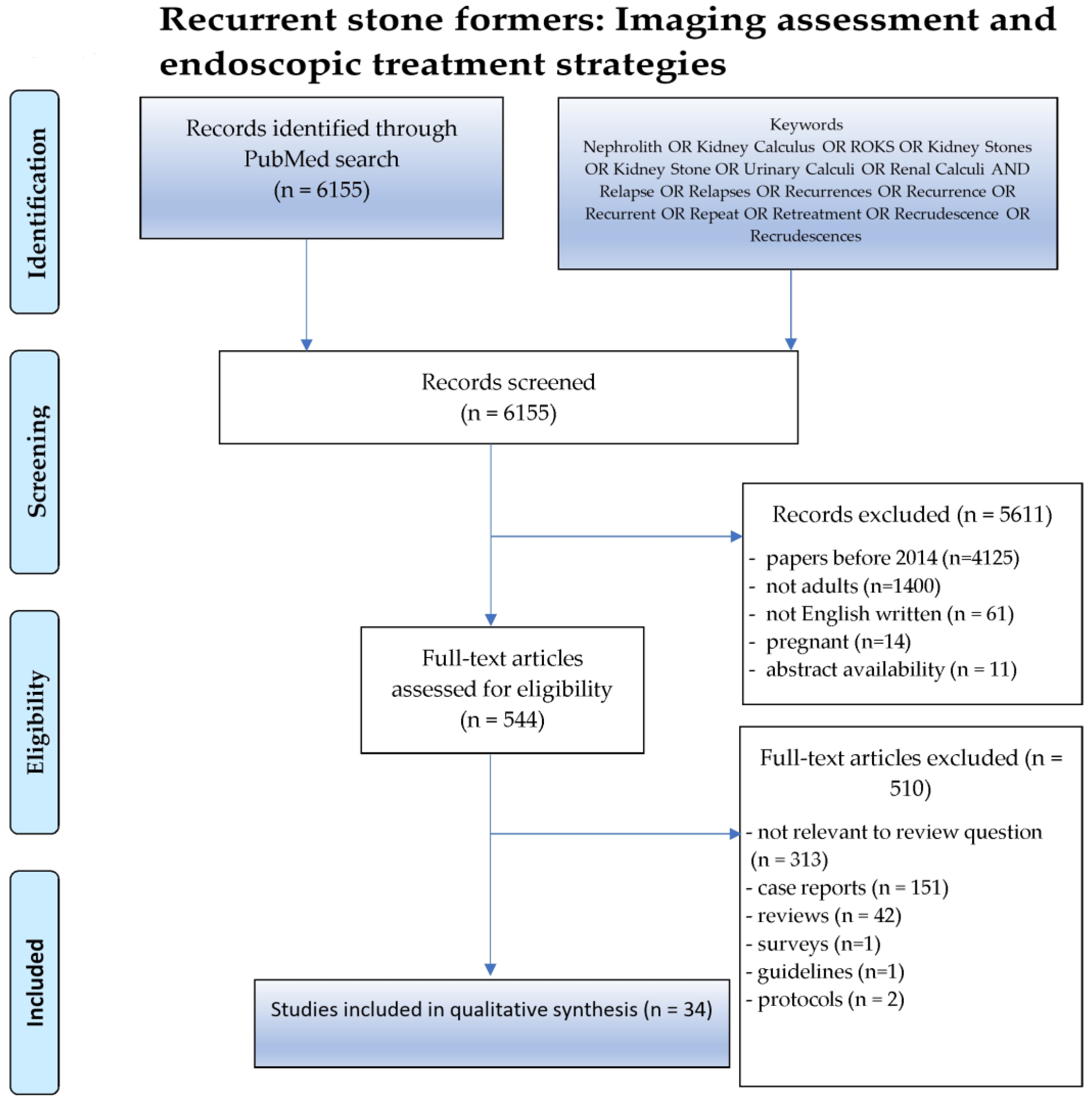
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
3. Results
3.1. Studies Selection
3.2. Imaging Modalities
3.2.1. CT
3.2.2. X-ray KUB
3.2.3. US
3.2.4. DT
3.3. Endoscopic Interventions
3.3.1. RIRS
3.3.2. URS
3.3.3. PCNL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stamatelou, K.; Goldfarb, D.S. Epidemiology of Kidney Stones. Healthcare 2023, 11, 424. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, I.; Mamoulakis, C.; Miyazawa, K.; Rodgers, A.; Talati, J.; Lotan, Y. Epidemiology of stone disease across the world. World J. Urol. 2017, 35, 1301–1320. [Google Scholar] [CrossRef] [PubMed]
- Tamborino, F.; Cicchetti, R.; Mascitti, M.; Litterio, G.; Orsini, A.; Ferretti, S.; Basconi, M.; De Palma, A.; Ferro, M.; Marchioni, M.; et al. Pathophysiology and Main Molecular Mechanisms of Urinary Stone Formation and Recurrence. Int. J. Mol. Sci. 2024, 25, 3075. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, V.; Ferraro, P.M.; Lombardi, G.; Friso, S.; Gambaro, G. Unravelling the Complex Relationship between Diet and Nephrolithiasis: The Role of Nutrigenomics and Nutrigenetics. Nutrients 2022, 14, 4961. [Google Scholar] [CrossRef] [PubMed]
- Ferrandino, M.N.; Bagrodia, A.; Pierre, S.A.; Scales, C.D., Jr.; Rampersaud, E.; Pearle, M.S.; Preminger, G.M. Radiation exposure in the acute and short-term management of urolithiasis at 2 academic centers. J. Urol. 2009, 181, 668–672; discussion 673. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.C.; Chang, H.C.; Holt, S.K.; Harper, J.D. National Trends in CT Utilization and Estimated CT-related Radiation Exposure in the Evaluation and Follow-up of Stone Patients. Urology 2019, 133, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Hyams, E.S.; Matlaga, B.R. Economic impact of urinary stones. Transl. Androl. Urol. 2014, 3, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and weaknesses. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2008, 22, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Abbassene, F.; Maizia, A.; Messaoudi, N.; Bendahmane, L.; Boukharouba, H.; Daudon, M.; Addou, A. Adult urolithiasis in Western Algeria: A study of 1104 cases. Tunis. Med. 2020, 98, 396–403. [Google Scholar]
- Arda, E.; Cakıroglu, B.; Akdeniz, E.; Yuksel, I.; Cetin, G.; Hilmi Aksoy, S. Comparison of Turkish Primary, Recurrent, and Non Stone-Forming Patients Using Hounsfield Unit Measurements: How Useful Is It? Curr. Urol. 2019, 12, 158–163. [Google Scholar] [CrossRef]
- Bhojani, N.; Paonessa, J.E.; El Tayeb, M.M.; Williams, J.C., Jr.; Hameed, T.A.; Lingeman, J.E. Sensitivity of Noncontrast Computed Tomography for Small Renal Calculi With Endoscopy as the Gold Standard. Urology 2018, 117, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, F.J.; Kaplan, A.G.; Youssef, R.F.; Tsivian, M.; Shin, R.H.; Scales, C.D.; Preminger, G.M.; Lipkin, M.E. Digital Tomosynthesis: A Viable Alternative to Noncontrast Computed Tomography for the Follow-Up of Nephrolithiasis? J. Endourol. 2016, 30, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Canales, B.K.; Sharma, N.; Yuzhakov, S.V.; Bozorgmehri, S.; Otto, B.J.; Bird, V.G. Long-term Recurrence Rates in Uric Acid Stone Formers With or Without Medical Management. Urology 2019, 131, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Chai, C.A.; Teoh, Y.C.; Tailly, T.; Emiliani, E.; Inoue, T.; Tanidir, Y.; Gadzhiev, N.; Bin Hamri, S.; Ong, W.L.; Shrestha, A.; et al. Influence of pre-stenting on RIRS outcomes. Inferences from patients of the Global Multicentre Flexible Ureteroscopy Outcome Registry (FLEXOR). Minerva Urol. Nephrol. 2023, 75, 493–500. [Google Scholar] [CrossRef]
- Cohen, A.J.; Borofsky, M.S.; Anderson, B.B.; Dauw, C.A.; Gillen, D.L.; Gerber, G.S.; Worcester, E.M.; Coe, F.L.; Lingeman, J.E. Endoscopic Evidence That Randall’s Plaque is Associated with Surface Erosion of the Renal Papilla. J. Endourol. 2017, 31, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Emiliani, E.; Piccirilli, A.; Cepeda-Delgado, M.; Kanashiro, A.K.; Mantilla, D.; Amaya, C.A.; Sanchez-Martin, F.M.; Millan-Rodriguez, F.; Territo, A.; Amón-Sesmero, J.H.; et al. Flexible ureteroscopy in extreme elderly patients (80 years of age and older) is feasible and safe. World J. Urol. 2021, 39, 2703–2708. [Google Scholar] [CrossRef] [PubMed]
- Evan, A.P.; Coe, F.L.; Worcester, E.M.; Williams, J.C.; Heiman, J.; Bledsoe, S.; Sommer, A.; Philips, C.L.; Lingeman, J.E. Discrepancy Between Stone and Tissue Mineral Type in Patients with Idiopathic Uric Acid Stones. J. Endourol. 2020, 34, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Evan, A.P.; Worcester, E.M.; Williams, J.C., Jr.; Sommer, A.J.; Lingeman, J.E.; Phillips, C.L.; Coe, F.L. Biopsy proven medullary sponge kidney: Clinical findings, histopathology, and role of osteogenesis in stone and plaque formation. Anat. Rec. 2015, 298, 865–877. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, V.; Chen, W.M.; Jain, R.; De, S.; Monga, M. Multiple sclerosis and nephrolithiasis: A matched-case comparative study. BJU Int. 2017, 119, 919–925. [Google Scholar] [CrossRef]
- Hadjipavlou, M.; Lam, V.; Seth, J.; Anjum, F.; Sriprasad, S. Radiation Exposure during Ureterorenoscopy and Laser Lithotripsy: An Analysis of Stone Characteristics. Urol. Int. 2018, 100, 198–202. [Google Scholar] [CrossRef]
- Hein, S.; Miernik, A.; Wilhelm, K.; Schlager, D.; Schoeb, D.S.; Adams, F.; Vach, W.; Schoenthaler, M. Endoscopically Determined Stone Clearance Predicts Disease Recurrence Within 5 Years After Retrograde Intrarenal Surgery. J. Endourol. 2016, 30, 644–649. [Google Scholar] [CrossRef]
- Iremashvili, V.; Li, S.; Penniston, K.L.; Best, S.L.; Hedican, S.P.; Nakada, S.Y. External Validation of the Recurrence of Kidney Stone Nomogram in a Surgical Cohort. J. Endourol. 2019, 33, 475–479. [Google Scholar] [CrossRef]
- Islam, A.K.; Holt, S.; Reisch, J.; Nwariaku, F.; Antonelli, J.; Maalouf, N.M. What Predicts Recurrent Kidney Stone after Parathyroidectomy in Patients with Primary Hyperparathyroidism? J. Am. Coll. Surg. 2020, 231, 74–82. [Google Scholar] [CrossRef]
- Ito, K.; Takahashi, T.; Somiya, S.; Kanno, T.; Higashi, Y.; Yamada, H. Predictors of Repeat Surgery and Stone-related Events After Flexible Ureteroscopy for Renal Stones. Urology 2021, 154, 96–102. [Google Scholar] [CrossRef]
- Kavoussi, N.L.; Da Silva, A.; Floyd, C.; McCoy, A.; Koyama, T.; Hsi, R.S. Feasibility of stone recurrence risk stratification using the recurrence of kidney stone (ROKS) nomogram. Urolithiasis 2023, 51, 73. [Google Scholar] [CrossRef]
- Li, S.; Iremashvili, V.; Vernez, S.L.; Penniston, K.L.; Jhagroo, R.A.; Best, S.L.; Hedican, S.P.; Nakada, S.Y. Effect of stone composition on surgical stone recurrence: Single center longitudinal analysis. Can. J. Urol. 2021, 28, 10744–10749. [Google Scholar]
- Lomas, D.J.; Jaeger, C.D.; Krambeck, A.E. Profile of the Ammonium Acid Urate Stone Former Based on a Large Contemporary Cohort. Urology 2017, 102, 43–47. [Google Scholar] [CrossRef]
- Mancuso, M.; Lavoie, C.; Assmus, M.; De, S. Characterizing patients with multiple same-sided ureteric stones. World J. Urol. 2022, 40, 1763–1767. [Google Scholar] [CrossRef]
- Ozgor, F.; Sahan, M.; Yanaral, F.; Savun, M.; Sarilar, O. Flexible ureterorenoscopy is associated with less stone recurrence rates over Shockwave lithotripsy in the management of 10–20 millimeter lower pole renal stone: Medium follow-up results. Int. Braz. J. Urol. 2018, 44, 314–322. [Google Scholar] [CrossRef]
- Ozgor, F.; Simsek, A.; Binbay, M.; Akman, T.; Kucuktopcu, O.; Sarilar, O.; Muslumanoglu, A.Y.; Berberoglu, Y. Clinically insignificant residual fragments after flexible ureterorenoscopy: Medium-term follow-up results. Urolithiasis 2014, 42, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Portis, A.J.; Laliberte, M.A.; Heinisch, A. Repeat Surgery After Ureteroscopic Laser Lithotripsy With Attempted Complete Extraction of Fragments: Long-term Follow-up. Urology 2015, 85, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.; Jaeger, C.; Yelfimov, D.; Krambeck, A.E. Risk of Chronic Kidney Disease in Brushite Stone Formers Compared With Idiopathic Calcium Oxalate Stone Formers. Urology 2017, 99, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Rule, A.D.; Lieske, J.C.; Li, X.; Melton, L.J., 3rd; Krambeck, A.E.; Bergstralh, E.J. The ROKS nomogram for predicting a second symptomatic stone episode. J. Am. Soc. Nephrol. 2014, 25, 2878–2886. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, M.S.; Gulati, A.; Saritha, J.; Nayak, B. Urolithiasis: Comparison of diagnostic performance of digital tomosynthesis and ultrasound. Which one to choose and when? Eur. J. Radiol. 2018, 105, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Shavit, L.; Girfoglio, D.; Kirkham, A.; Allen, D.; Ferraro, P.M.; Moochhala, S.; Unwin, R. Increased renal papillary density in kidney stone formers detectable by CT scan is a potential marker of stone risk, but is unrelated to underlying hypercalciuria. Urolithiasis 2016, 44, 471–475. [Google Scholar] [CrossRef]
- Shavit, L.; Girfoglio, D.; Vijay, V.; Goldsmith, D.; Ferraro, P.M.; Moochhala, S.H.; Unwin, R. Vascular calcification and bone mineral density in recurrent kidney stone formers. Clin. J. Am. Soc. Nephrol. 2015, 10, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Streeper, N.M.; Wertheim, M.L.; Nakada, S.Y.; Penniston, K.L. Cystine Stone Formers Have Impaired Health-Related Quality of Life Compared with Noncystine Stone Formers: A Case-Referent Study Piloting the Wisconsin Stone Quality of Life Questionnaire Among Patients with Cystine Stones. J. Endourol. 2017, 31, S48–S53. [Google Scholar] [CrossRef]
- Usawachintachit, M.; Sherer, B.; Hudnall, M.; Tzou, D.T.; Taguchi, K.; Hsi, R.S.; Stoller, M.; Chi, T. Clinical Outcomes for Cystinuria Patients with Unilateral Versus Bilateral Cystine Stone Disease. J. Endourol. 2018, 32, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, Y.; Yang, C.; Wang, J.; Zhang, X.C.; Zhang, L.; Zhao, M.H. Surgical procedure and recurrence of upper urinary tract stone: A national-wide study based on hospitalized patients. World J. Urol. 2024, 42, 132. [Google Scholar] [CrossRef]
- Yamashita, S.; Iguchi, T.; Nishizawa, S.; Iba, A.; Kohjimoto, Y.; Hara, I. Recurrent stone-forming patients have high visceral fat ratio based on computed tomography images compared to first-time stone-forming patients. Int. J. Urol. 2018, 25, 569–573. [Google Scholar] [CrossRef]
- Zeng, J.; Wang, S.; Zhong, L.; Huang, Z.; Zeng, Y.; Zheng, D.; Zou, W.; Lai, H. A Retrospective Study of Kidney Stone Recurrence in Adults. J. Clin. Med. Res. 2019, 11, 208–212. [Google Scholar] [CrossRef]
- Tzelves, L.; Geraghty, R.; Lombardo, R.; Davis, N.F.; Petřík, A.; Neisius, A.; Gambaro, G.; Türk, C.; Thomas, K.; Somani, B.; et al. Duration of Follow-up and Timing of Discharge from Imaging Follow-up, in Adult Patients with Urolithiasis After Surgical or Medical Intervention: A Systematic Review and Meta-analysis from the European Association of Urology Guideline Panel on Urolithiasis. Eur. Urol. Focus. 2023, 9, 188–198. [Google Scholar] [CrossRef]
- Lombardo, R.; Tzelves, L.; Geraghty, R.; Davis, N.F.; Neisius, A.; Petřík, A.; Gambaro, G.; Türk, C.; Somani, B.; Thomas, K.; et al. Follow-up of urolithiasis patients after treatment: An algorithm from the EAU Urolithiasis Panel. World J. Urol. 2024, 42, 202. [Google Scholar] [CrossRef]
- Ray, A.A.; Ghiculete, D.; Pace, K.T.; Honey, R.J. Limitations to ultrasound in the detection and measurement of urinary tract calculi. Urology 2010, 76, 295–300. [Google Scholar] [CrossRef]
- Smith-Bindman, R.; Aubin, C.; Bailitz, J.; Bengiamin, R.N.; Camargo, C.A., Jr.; Corbo, J.; Dean, A.J.; Goldstein, R.B.; Griffey, R.T.; Jay, G.D.; et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N. Engl. J. Med. 2014, 371, 1100–1110. [Google Scholar] [CrossRef]
- Khan, S.R.; Canales, B.K.; Dominguez-Gutierrez, P.R. Randall’s plaque and calcium oxalate stone formation: Role for immunity and inflammation. Nat. Rev. Nephrol. 2021, 17, 417–433. [Google Scholar] [CrossRef]
- Vaughan, L.E.; Enders, F.T.; Lieske, J.C.; Pais, V.M.; Rivera, M.E.; Mehta, R.A.; Vrtiska, T.J.; Rule, A.D. Predictors of Symptomatic Kidney Stone Recurrence After the First and Subsequent Episodes. Mayo Clin. Proc. 2019, 94, 202–210. [Google Scholar] [CrossRef]
- Forbes, C.M.; McCoy, A.B.; Hsi, R.S. Clinician Versus Nomogram Predicted Estimates of Kidney Stone Recurrence Risk. J. Endourol. 2021, 35, 847–852. [Google Scholar] [CrossRef]
- Flammia, S.; Salciccia, S.; Tufano, A.; Busetto, G.M.; Ricciuti, G.P.; Sciarra, A. How urinary stone emergencies changed in the time of COVID-19? Urolithiasis 2020, 48, 467–469. [Google Scholar] [CrossRef]

{kind=link}
| Reference | Year | Study | Population | Age | Gender | Imaging | Follow-Up | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Ozgor et al. [30] | 2014 | Retrospective | 44 patients (residual fragments < 5 mm) | Group 1, asymptomatic or stone-free (SFr) 44.1 + 13.4 Group 2, symptomatic 38 + 19.9 | Group 1 (18 males, 11 females) Group 2 (9 males, 6 females) | KUB and abdominal US (twice per year). Abdominal CT (annually) | 30.5 ± 8.809 months | Stone recurrence in 15 patients (34.1%). A total of 11 needed interventional therapy (5 RIRS, 2 SWL, 3 URS, and 1 PCNL). Size and number of residual stones were not associated with recurrence. |
| Rule et al. [33] | 2014 | Retrospective | 2239 first-time symptomatic SFs | 42 (32–54) 41 (31–51.0) in symptomatic recurrence patients | 1399 males, 840 females | CT imaging without clarifying further details about the follow-up or radiation protocol | 11.2 years | Surgery was weakly associated with a decreased risk of symptomatic recurrence but could not discriminate high- from low-risk patients. Prior incidental (asymptomatic) stone and ≥2 stones on imaging were risk factors for recurrence (unadjusted HRs = 1.53 (p = 0.004) and 1.72 (p < 0.001), respectively). Symptomatic recurrence rates at 2, 5, 10, and 15 years were 11%, 20%, 31%, and 39%, respectively. |
| Evan et al. [18] | 2015 | Retrospective | 12 recurrent SFs with medullary sponge kidney | 46.8 (36–66) | 4 males, 8 females | KUB and CT | NA | The osteogenic theory was not supported. Urinary stasis could explain the pathophysiology of stone recurrence. Biopsy is not of value in the clinical management of patients with MSK. |
| Portis et al. [31] | 2015 | Retrospective | 218 first-time SFs (burden < 1.5 cm) | 51.5 ± 15 | 124 consecutive procedures in males and 102 in females | CT (1 month after stent removal) | 4.1 years (interquartile range, 3.5–4.8) | A total of 19 patients (8.7%) needed repeat surgery (14 ureteroscopy and 5 PCNL). Total stone burden was associated with repeat surgery. Postoperative CT did not play a role in the need for reoperation. Cumulative repeat surgery rate was 5.8% and 8.6% at 1 and 5 years, respectively. A total of 26% of patients with fragments >2 to 4 mm and 46% of patients with fragments >4 mm needed reoperation. |
| Shavit et al. [36] | 2015 | Retrospective | 111 (57 recurrent calcium SFs and 54 age- and sex-matched controls) | 47 ± 14 (SFs), 47 ± 13 (controls) | 63 males, 48 females | NCCT KUB (assessed the abdominal aortic calcification and vertebral bone mineral density) | NA | The abdominal aortic calcification severity score was significantly higher in SFs compared with the control group. The average vertebral bone mineral density was significantly lower in SFs. |
| Cabrera et al. [12] | 2016 | Retrospective | 62 (the exact number of recurrent SFs was not clear) | 42 | NA | NCCT, DT | Mean time interval of 80.6 days between NCCT and DT. | DT could be used to follow-up patients with intrarenal lithiasis. Regarding the ureter, it is reported that NCCT identified 7 stones, while DT identified 1. |
| Hein et al. [21] | 2016 | Retrospective | 85 SFr patients (included those with small fragments < 1 mm) | 49.8 (17–80) | 68 males, 17 females | No routine imaging in asymptomatic patients. Low-dose CT at first stone-related event | 59 months (31–69) | Stone recurrence in 26 patients (30.1%). SWL in 6 patients, medical treatment in 5 patients, RIRS in 9, and multiple in 6. Residual fragments are an important predictor for ipsilateral stone recurrence both in high- and low-risk patients. |
| Shavit et al. [35] | 2016 | Prospective | 111 (57 recurrent nephrolithiasis and 54 age- and sex-matched controls) | 47 ± 14 (nephrolithiasis) 47 ± 13 (without lithiasis) | 63 males, 48 females | NCCT | NA | Increased HU papillary density in the recurrent SFs regardless of whether they are hypercalciuric or non-hypercalciuric. |
| Ganesan et al. [19] | 2017 | Retrospective | 181 recurrent SFs (61 patients with MS compared with 120 matched controls) | 53.7 (47.0–61.3, No MS) 53.2 (47.0–58.1, MS) | 57 males, 124 females | CT (when available) | 3.9 (1.5–7.7) years | MS patients more likely to have undergone a PCNL (25% vs. 12%, p = 0.005) with a higher proportion of struvite and calcium phosphate and stones (8% vs. 3%, p = 0.03 and 42% vs. 15%, p < 0.001, respectively). Less likely to have calcium oxalate monohydrate stones (39% vs. 64%, p < 0.001). |
| Bhojani et al. [11] | 2018 | Prospective | 11 known previous calcium oxalate SFs | 48 (21–74) | 7 males, 4 females | NCCT (helical) | NA | Non-contrast helical CT underestimates the total number of kidney stones compared to endoscopy (9.2 ± 6.1 vs. 5.9 ± 4.1, p < 0.004) but did not differ in total stone burden. |
| Hadjipavlou et al. [20] | 2018 | Retrospective | 302 SFs with single calculus until stone clearance | 56 (21–92) | 195 males, 107 females | NCCT KUB all patients, while 85 (29%) also had at least one X-ray | NA | Large stone burden, proximal stone location, and truncal obesity were associated with higher ionizing radiation during URS. Pre-stenting was associated with over 50% of the radiation delivered during URS (4.13 vs. 7.54 mGy, respectively). |
| Ozgor et al. [29] | 2018 | Retrospective | 113 and 128 patients with lower pole renal stone underwent SWL and RIRS, respectively | 45.9 ± 14.7 (RIRS) 48.6 ± 14.9 (SWL) | 128 males, 113 females | US and X-ray KUB twice per year. CT annually | 34.1 ± 13.2 months (RIRS) 32.4 ± 8.5 months (SWL) | Stone recurrence was more common in SWL (28 vs. 17 patients, p = 0.009). No differences for the recurrent stone size and recurrence period. |
| Sandhu et al. [34] | 2018 | Prospective | 66 (including recurrent SFs) | 44.2 (19–73) | 36 males, 30 females | US, DT, and NCCT | ΝA | DT is not superior to the US in the detection of kidney stones but still performs better in the identification of ureteral stones. |
| Yamashita et al. [40] | 2018 | Retrospective | 300 patients with upper urinary tract stones (148 recurrent, 152 first-time) | 59 (49–69) | 208 males, 98 females | Pretreatment NCCT | NA | The visceral fat ratio was greater in patients with recurrent lithiasis compared to first-time formers despite the fact that there were no statistically significant differences in BMI and waist circumference. |
| Arda et al. [10] | 2019 | Retrospective | 280 (98 recurrent SFs, 88 primary and 94 age-matched control participants) |
34 (21–60, primary) 37 (21–67, recurrent) | NA | NCCT (helical) | NA | Higher papillae HU could predict stone recurrence. |
| Canales et al. [13] | 2019 | Retrospective | 53 uric acid SFs | 61.4 ± 11.7 | 35 males, 18 females | Routinely followed at 6-month intervals with CT | 25 months (15.8–47.5) | A total of 32% of patients (17) had stone recurrence, and 13% (7) required surgical intervention. Mean time interval to stone recurrence was 16.8 ± 15.3 months. The 32% of patients had CT-documented stone recurrences over the 2-year interval regardless of therapy. |
| Dai et al. [6] | 2019 | Retrospective | 327,516 (active stone, 112,140 were ted operatively and 215,376 were managed nonoperatively) 175,228 inactive stone patients and 502,744 age- and gender-matched controls | 18–65 (divided into 4 groups, 18–39, 40–49, 50–59 and 60–65) | 552,052 males, 453,436 females | Standard dose CT | 3 years of continuous follow-up | The 3-year cumulative CT radiation (mean) was 28.3 ± 28.5 mSv for operative patients and 22.0 ± 24.4 mSv for nonoperative patients. For inactive stone patients and controls, exposure was 14.9 ± 19.3 mSv and 2.4 ± 10.0 mSv, respectively. Surgical-treated patients receive 9 to 12 times more CT scans than age- and sex-matched controls during the 3-year follow-up. Also, more than 10% of them exceeded occupational risk thresholds in the first year without accounting for exposure during surgical procedures. |
| Iremashvili et al. [22] | 2019 | Retrospective | 498 SFs | 53.6 (18.1–89.6) | 260 males, 238 females | CT (92%), US (1.6%), X-ray (6.4%) | 4.8 years (mean 4.6, IQR 3.1–6.1) | A total of 88 patients (17.7%) were symptomatic recurrent SFs at 5-year follow-up, requiring surgical treatment. This percentage increased to 25% by 8 years of follow-up. Symptomatic stone (renal pelvis or lower renal pole) and any concurrent non-obstructing, asymptomatic stone associated with the risk of repeat surgery (HR 1.66 (1.09–2.52), p = 0.018 and 2.11 (1.36–3.26) p = 0.001, respectively) |
| Zeng et al. [41] | 2019 | Retrospective | 146 recurrent SFs (of the 3985–3.7%) | Males’ mean 39.4 ± 15.8 Females’ mean age 41.5 ± 18.5 | 100 males, 48 females | Ultrasound assessment of severity of hydronephrosis | 4 years | Minimally invasive methods were mainly used to treat the first stone episode. The main symptom of recurrence was associated with infection (renal colic at first episode). Recurrences of lithiasis occur mainly with a lesser degree of hydronephrosis. |
| Abbassene et al. [9] | 2020 | Retrospective | 1104 SFs | 45.3 ± 13.9 | 727 males, 377 females | Imaging modalities are not clarified | Over 7 years | A total of 51.1% of patients had stone recurrence (prevalence of males). Cystine was the most recurrent stone (27.3% consanguinity). |
| Islam et al. [23] | 2020 | Retrospective | 69 SFs with primary hyperparathyroidism (Parathyroidectomy) | 57 ± 14 | 31 males, 38 females | X-ray KUB every 6 months after parathyroidectomy | 4.0 ± 2.9 years | A total of 23% of patients (16 of 69) had stone recurrence after parathyroidectomy, and 88% (14) needed surgical intervention. Younger patients are high-risk for stone recurrence. |
| Ito et al. [24] | 2021 | Retrospective | 664 SFs | 60.0 ± 12.7 | 418 males, 246 females | X-ray KUB and US at first month, followed by once every 6 months. | 31.1 months | A total of 15.5% of patients (103) experienced surgical intervention (40.8% URS, 56.3% SWL, and 2.9% PCNL). Stone burden ≥ 20 mm and RF ≥ 4 mm were predictive factors for stone recurrence. |
| Li et al. [26] | 2021 | Retrospective | 1051 SFs | 59.1 ± 15.1 | 555 males, 496 females | US, X-ray KUB and CT with no standardized plan | 4.7 ± 2.5 years | A total 26.7% of patients required repeat surgery. Cystine and brushite SFs had the highest and the second-highest risk for surgical recurrence, respectively. |
| Emiliani et al. [16] | 2021 | Retrospective | 173 SFs (78 for group 1, age < 80 and 95 for group 2, age ≥ 80 | group 1 → 44 (27–79) group 2 → 81 (80–94) | group 1 → 40 males, 38 females group 2 → 45 males, 50 females | US and NCCT (for non-radio-opaque stones) at 1 year | Not clarified | Recurrence rate did not differ between group 1 and group 2 (4.3% vs. 5.6%, p = 0.730, respectively). Elderly patients were controlled with longer operative time and hospitalization than younger patients. There was no difference regarding complications. |
| Mancuso et al. [28] | 2022 | Retrospective | 79 patients with multiple same-sided ureteric stones and 101 with single ureteric stone | 57 ± 13 (multiple) 49 ± 15 (single) | 122 males, 58 females | US, X-ray KUB, and NCCT | Not clarified | Patients with multiple stones were more likely to be recurrent SFs and formed a higher proportion of non-calcium oxalate stones. Also, they were more likely to have other procedures (except URS) such as PCNL. They underwent NCCT and KUB 11.5 times more frequently compared with single ureteric SFs. |
| Kavoussi et al. [25] | 2023 | Retrospective | 200 patients (100 without stone recurrence and 100 with recurrence) | 49 ± 15 (overall) 47 ± 15 (recurrence) 52 ± 6 (non-recurrence) | 101 males, 99 females | at least yearly imaging | 96 ± 38 months | Time to stone recurrence was 29 ± 32 months. Calcium oxalate monohydrate stone, family history of stone disease and a stone > 6 mm in diameter associated with risk of recurrent lithiasis. The surgical method was not associated with stone recurrence. |
| Chai et al. [14] | 2023 | Retrospective | 6579 SFs (3112 pre-stenting 3467 no stenting) | 49.34 ± 15.59 (overall) 51.44 ± 16.01 (pre-stenting) 47.47 ± 14.94 (no stenting) | 4346 males, 2233 females | CT, US, KUB X-rays with no standardized settings | NA | Recurrent SFs had higher overall complications and residual fragments. |
| Reference | Year | Study | Population | Age | Gender | Interventions | Follow-Up | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Ozgor et al. [30] | 2014 | Retrospective | 44 patients (residual fragments < 5 mm) | Group 1, asymptomatic or SFr 44.1 + 13.4 Group 2, symptomatic 38 + 19.9 | Group 1 (18 males, 11 females) Group 2 (9 males, 6 females) | RIRS | 30.5 ± 8.809 months | Stone recurrence in 15 patients (34.1%). A total of 11 needed interventional therapy (5 RIRS, 2 SWL, 3 URS, and 1 PCNL) Size and number of residual stones were not associated with recurrence. |
| Rule et al. [33] | 2014 | Retrospective | 2239 first-time symptomatic SFs | 42 (32–54) 41 (31, 51.0) in symptomatic recurrence patients | 1399 males, 840 females | Surgery documented in 33% of patients. No surgical intervention was included in the final nomogram. | 11.2 years | Surgery was weakly associated with a decreased risk of symptomatic recurrence but could not discriminate high- from low-risk patients. Prior incidental (asymptomatic) stone and ≥2 stones on imaging were risk factors for recurrence (unadjusted HRs = 1.53 (p = 0.004) and 1.72 (p < 0.001), respectively). Symptomatic recurrence rates at 2, 5, 10, and 15 years were 11%, 20%, 31%, and 39%, respectively. |
| Evan et al. [18] | 2015 | Retrospective | 12 recurrent SFs with medullary sponge kidney | 46.8 (36–66) | 4 males, 8 females | PCNL with papillary biopsy | NA | The osteogenic theory was not supported. Urinary stasis could explain the pathophysiology of stone recurrence. Biopsy is not of value in the clinical management of patients with MSK. |
| Portis et al. [31] | 2015 | Retrospective | 218 first time SFs (burden < 1.5 cm) | 51.5 ± 15 | 124 consecutive procedures in males and 102 in females | Rigid ureteroscopy (below the iliac vessels) flexible ureteroscopy (in the upper tract) | 4.1 years (interquartile range, 3.5–4.8) | A total of 19 patients (8.7%) needed repeat surgery (14 ureteroscopy and 5 PCNL). Total stone burden was associated with repeat surgery. Postoperative CT did not play a role in the need for reoperation. Cumulative repeat surgery rate was 5.8% and 8.6% at 1 and 5 years, respectively. A total of 26% of patients with fragments >2 to 4 mm and 46% of patients with fragments >4 mm needed reoperation. |
| Hein et al. [21] | 2016 | Retrospective | 85 SFr patients (included those with small fragments < 1 mm) | 49.8 (17–80) | 68 males, 17 females | RIRS | 59 months (31–69) | Stone recurrence in 26 patients (30.1%). SWL in 6 patients, medical treatment in 5 patients, RIRS in 9, and multiple in 6. Residual fragments are an important predictor for ipsilateral stone recurrence both in high- and low-risk patients. |
| Cohen et al. [15] | 2017 | Prospective | 13 patients (100% recurrent SFs, center 1) 63 patients (54.2% recurrent SFs, center 2) | 46 (42–52, center 1) 51 (41–63, center 2) | 42 males, 34 females | RIRS with complete papillary mapping | NA | Recurrent SFs had higher total scores (papillary mapping). The scoring system during endoscopy may have clinical usefulness for adapting specific treatment strategies. |
| Ganesan et al. [19] | 2017 | Retrospective | 181 recurrent s SFs (61 patients with MS compared with 120 matched controls) | 53.7 (47.0–61.3, No MS) 53.2 (47.0–58.1, MS) | 53.7 (47.0–61.3, No MS) 53.2 (47.0–58.1, MS) | URS, PCNL, SWL, Cystolithopaxy | 3.9 (1.5–7.7) years | MS patients more likely to have undergone a PCNL (25% vs. 12%, p = 0.005) with a higher proportion of struvite and calcium phosphate and stones (8% vs. 3%, p = 0.03 and 42% vs. 15%, p < 0.001, respectively). Less likely to have calcium oxalate monohydrate stones (39% vs. 64%, p < 0.001). |
| Lomas et al. [27] | 2017 | Retrospective | 89 patients with ammonium acid urate stones | 55 (39.5–70.5) at stone formation | 38 males, 17 females | 83% required surgical intervention (not clarified the method) | 4.9 years (IQR 1.8–8.5), | A total of 19 patients (21%) had stone recurrence with a median time to recurrence of 22 months (IQR 10.5–42). |
| Rivera et al. [32] | 2017 | Retrospective | 20 brushite SFs matched with 60 calcium oxalate SFs | 48 (38–58, brushite) 47 (40–56, calcium oxalate) | 57 males, 23 females | Prior stone surgery as SWL, PCNL or URS in 60% and 33% of brushite and calcium oxalate SFs, respectively | 12.2 years (10.0–17.4, brushite) 13.5 years (10.4–17.0, calcium oxalate) | Brushite SFs had a higher incidence of prior stones as well as prior surgical intervention. Also, they had a higher stone recurrence rate (80% vs. 42%, p = 0.003) without changing in the CKD stage. |
| Streeper et al. [37] | 2017 | Retrospective | 12 cystine matched with 12 non-cystine recurrent SFs | 50.6 ± 16.7 (cystine) 53.5 ± 16.8 (non cystine) | 6 males, 18 females | URS, PCNL, SWL | 5 years | Cystine SFs had a greater number of surgical interventions compared to non-cystine formers (8.5 ± 9.1 vs. 2.9 ± 3.1). 62% of cystine formers underwent PCNL, whereas the percentage of non-cystine patients was 15%. Similarly, for ureteroscopy, the percentages were 100% vs. 54%. |
| Bhojani et al. [11] | 2018 | Prospective | 11 known previous calcium oxalate SFs | 48 (21–74) | 7 males, 4 females | RIRS | NA | NCCT (helical) underestimated the total number of kidney stones compared to endoscopy (9.2 ± 6.1 vs. 5.9 ± 4.1, p < 0.004) but did not differ in total stone burden. |
| Hadjipavlou et al. [20] | 2018 | Retrospective | 302 SFs with single calculus until stone clearance | 56 (21–92) | 195 males, 107 females | URS | NA | Large stone burden, proximal stone location, and truncal obesity were associated with higher ionizing radiation during URS. Pre-stenting was associated with over 50% of the radiation delivered during URS (4.13 vs. 7.54 mGy, respectively). |
| Ozgor et al. [29] | 2018 | Retrospective | 113 and 128 patients with lower pole renal stone underwent SWL and RIRS, respectively | 45.9 ± 14.7 (RIRS) 48.6 ± 14.9 (SWL) | 128 males, 113 females | RIRS | 34.1 ± 13.2 months (RIRS) 32.4 ± 8.5 months (SWL) | Stone recurrence was more common in SWL (28 vs. 17 patients, p = 0.009). No differences for the recurrent stone size and recurrence period. |
| Usawachintachit et al. [38] | 2018 | Retrospective | 42 recurrent cystine stone patients | 45.5 (IQR: 28–63) | 20 males, 22 females | PCNL, URS, SWL, open surgery | 8.8 years (0.9–13.6) | A total of 2/3 of patients form bilateral stones which correlated with higher median number of lifetime URS compared with unilateral SFs (2 vs. 1 session, p < 0.05). There was no significant difference for PCNL (p = 0.55). |
| Yamashita et al. [40] | 2018 | Retrospective | 300 patients with upper urinary tract stones (148 recurrent, 152 first-time) | 59 (49–69) | 208 males, 98 females | PCNL, URS, SWL | NA | The visceral fat ratio was greater in patients with recurrent lithiasis compared to first-time formers despite the fact that there were no statistically significant differences in BMI and waist circumference. |
| Canales et al. [13] | 2019 | Retrospective | 53 uric acid SFs | 61.4 ± 11.7 | 35 males, 18 females | Not clarified | 25 months (15.8–47.5) | A total of 32% of patients (17) had stone recurrence, and 13% (7) required surgical intervention. Mean time interval to stone recurrence was 16.8 ± 15.3 months. The 32% of patients had CT-documented stone recurrences over the 2-year interval regardless of therapy. |
| Dai et al. [6] | 2019 | Retrospective | 327,516 (active stone, 112,140 were ted operatively and 215,376 were managed nonoperatively) 175,228 inactive stone patients and 502,744 age- and gender-matched controls | 18–65 (divided into 4 groups, 18–39, 40–49, 50–59 and 60–65) | 552,052 males, 453,436 females | PCNL, URS, SWL | 3 years of continuous follow-up | The 3-year cumulative CT radiation (mean) was 28.3 ± 28.5 mSv for operative patients and 22.0 ± 24.4 mSv for nonoperative patients. For inactive stone patients and controls, exposure was 14.9 ± 19.3 mSv and 2.4 ± 10.0 mSv, respectively. Surgical-treated patients receive 9 to 12 times more CT scans than age- and sex-matched controls during the 3-year follow-up. Also, more than 10% of them exceeded occupational risk thresholds in the first year without accounting for exposure during surgical procedures. |
| Iremashvili et al. [22] | 2019 | Retrospective | 498 SFs | 53.6 (18.1–89.6) | 260 males, 238 females | PCNL (12.2%), Ureteroscopy (83.5%), SWL (4.2%) | 4.8 years (mean 4.6, IQR 3.1–6.1) | A total of 88 patients (17.7%) were symptomatic recurrent SFs at 5-year follow-up, requiring surgical treatment. This percentage increased to 25% by 8 years of follow-up. Symptomatic stone (renal pelvis or lower renal pole) and any concurrent non-obstructing, asymptomatic stone associated with the risk of repeat surgery (HR 1.66 (1.09–2.52), p = 0.018 and 2.11 (1.36–3.26) p = 0.001, respectively). |
| Zeng et al. [41] | 2019 | Retrospective | 146 recurrent SFs (of the 3985–3.7%) | Males’ mean 39.4 ± 15.8 Females’ mean age 41.5 ± 18.5 | 100 males, 48 females | PCNL (65 cases) SWL (22 cases), super-mini PCNL (20 cases), open surgery (four cases) and ureteroscopy (one case). | 4 years | Minimally invasive methods were mainly used to treat the first stone episode. The main symptom of recurrence was associated with infection (renal colic at first episode). Recurrences of lithiasis occur mainly with a lesser degree of hydronephrosis. |
| Abbassene et al. [9] | 2020 | Retrospective | 1104 SFs | 45.3 ± 13.9 | 727 males, 377 females | Conventional surgery (19.7%) endourology or SWL (15.5%) | Over 7 years | A total of 51.1% of patients had stone recurrence (prevalence of males). Cystine was the most recurrent stone (27.3% consanguinity). |
| Evan et al. [17] | 2020 | Retrospective | 8 uric acid SFs (6 recurrent) | 45.5 (37–67) | 8 males | PCNL (Papillary mapping and biopsy) | NA | Renal papillae plaques and plugging did not correlate with patients’ prior episodes of symptomatic lithiasis (very small number of cases). |
| Islam et al. [23] | 2020 | Retrospective | 69 SFs with primary hyperparathyroidism (Parathyroidectomy) | 57 ± 14 | 31 males, 38 females | Not clarified | 4.0 ± 2.9 years | A total of 23% of patients (16 of 69) had stone recurrence after parathyroidectomy, and 88% (14) needed surgical intervention. Younger patients are high-risk for stone recurrence. |
| Ito et al. [24] | 2021 | Retrospective | 664 SFs | 60.0 ± 12.7 | 418 males, 246 females | RIRS | 31.1 months | A total of 15.5% of patients (103) experienced surgical intervention (40.8% URS, 56.3% SWL, and 2.9% PCNL). Stone burden ≥ 20 mm, and RF ≥ 4 mm were predictive factors for stone recurrence. |
| Li et al. [26] | 2021 | Retrospective | 1051 SFs | 59.1 ± 15.1 | 555 males, 496 females | URS, PCNL, SWL | 4.7 ± 2.5 | A total of 26.7% of patients required repeat surgery. Cystine and brushite SFs had the highest and the second-highest risk for surgical recurrence, respectively. |
| Emiliani et al. [16] | 2021 | Retrospective | 173 SFs (78 for group 1, age < 80 and 95 for group 2, age≥ 80 | group 1 → 44 (27–79) group 2 → 81 (80–94) | group 1 → 40 males, 38 females group 2 → 45 males, 50 females | RIRS | Not clarified | Recurrence rate did not differ between group 1 and group 2 (4.3% vs. 5.6%, p = 0.730, respectively). Elderly patients were controlled with longer operative time and hospitalization than younger patients. There was no difference regarding complications. |
| Mancuso et al. [28] | 2022 | Retrospective | 79 patients with multiple same-sided ureteric stones and 101 with single ureteric stone | 57 ± 13 (multiple) 49 ± 15 (single) | 122 males, 58 females | SWL, URS | Not clarified | Patients with multiple stones were more likely to be recurrent SFs and formed a higher proportion of non-calcium oxalate stones. Also, they were more likely to have other procedures (except URS) such as PCNL. They underwent NCCT and KUB 11.5 times more frequently compared with single ureteric SFs. |
| Kavoussi et al. [25] | 2023 | Retrospective | 200 patients (100 without stone recurrence and 100 with recurrence) | 49 ± 15 (overall) 47 ± 15 (recurrence) 52 ± 6 (non-recurrence) | 101 males, 99 females | URS, PCNL, SWL | 96 ± 38 months | Time to stone recurrence was 29 ± 32 months. Calcium oxalate monohydrate stone, family history of stone disease, and a stone > 6 mm in diameter were associated with the risk of recurrent lithiasis. The surgical method was not associated with stone recurrence. |
| Chai et al. [14] | 2023 | Retrospective | 6579 (3112 pre-stenting 3467 no stenting) | 49.34 ± 15.59 (overall) 51.44 ± 16.01 (pre-stenting) 47.47 ± 14.94 (no stenting) | 4346 males, 2233 females | RIRS | NA | Recurrent SFs had higher overall complications and residual fragments. |
| Wang et al. [39] | 2024 | Retrospective | 556,217 patients with upper urinary tract stone | 49.9 ± 13.1 | 356,532 males, 199,685 females | Open surgery (8.6%), SWL (8.4%), URS (53.4%), and PCNL (29.6%) | 2.7 years (IQR 1.5–4.0) | A total of 23,012 patients (4.1%) underwent a second surgical intervention (incidence rate of 14.9 per 1000 person-years). Hazard ratios for SWL, ureteroscopic lithotripsy, and PCNL were 1.59 (1.49–1.70), 1.38 (1.31–1.45), and 1.11 (1.06–1.18), respectively. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mavridis, C.; Bouchalakis, A.; Tsagkaraki, V.; Somani, B.K.; Mamoulakis, C.; Tokas, T. Recurrent Urinary Stone Formers: Imaging Assessment and Endoscopic Treatment Strategies: A Systematic Search and Review. J. Clin. Med. 2024, 13, 3461. https://doi.org/10.3390/jcm13123461
Mavridis C, Bouchalakis A, Tsagkaraki V, Somani BK, Mamoulakis C, Tokas T. Recurrent Urinary Stone Formers: Imaging Assessment and Endoscopic Treatment Strategies: A Systematic Search and Review. Journal of Clinical Medicine. 2024; 13(12):3461. https://doi.org/10.3390/jcm13123461
Chicago/Turabian StyleMavridis, Charalampos, Athanasios Bouchalakis, Vasiliki Tsagkaraki, Bhaskar Kumar Somani, Charalampos Mamoulakis, and Theodoros Tokas. 2024. "Recurrent Urinary Stone Formers: Imaging Assessment and Endoscopic Treatment Strategies: A Systematic Search and Review" Journal of Clinical Medicine 13, no. 12: 3461. https://doi.org/10.3390/jcm13123461
APA StyleMavridis, C., Bouchalakis, A., Tsagkaraki, V., Somani, B. K., Mamoulakis, C., & Tokas, T. (2024). Recurrent Urinary Stone Formers: Imaging Assessment and Endoscopic Treatment Strategies: A Systematic Search and Review. Journal of Clinical Medicine, 13(12), 3461. https://doi.org/10.3390/jcm13123461