


The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Study Selection and Review of the Literature
3. Case Report
3.1. Patient Information, Diagnosis and Treatment Plan
- Extraction of hopeless teeth and enucleation of periodontal lesions with immediate implantation in the positions of teeth 32, 34, 42, 44 and bone augmentation;
- After two months of evaluation of soft tissues and possible augmentation of them using free gingival graft/grafts;
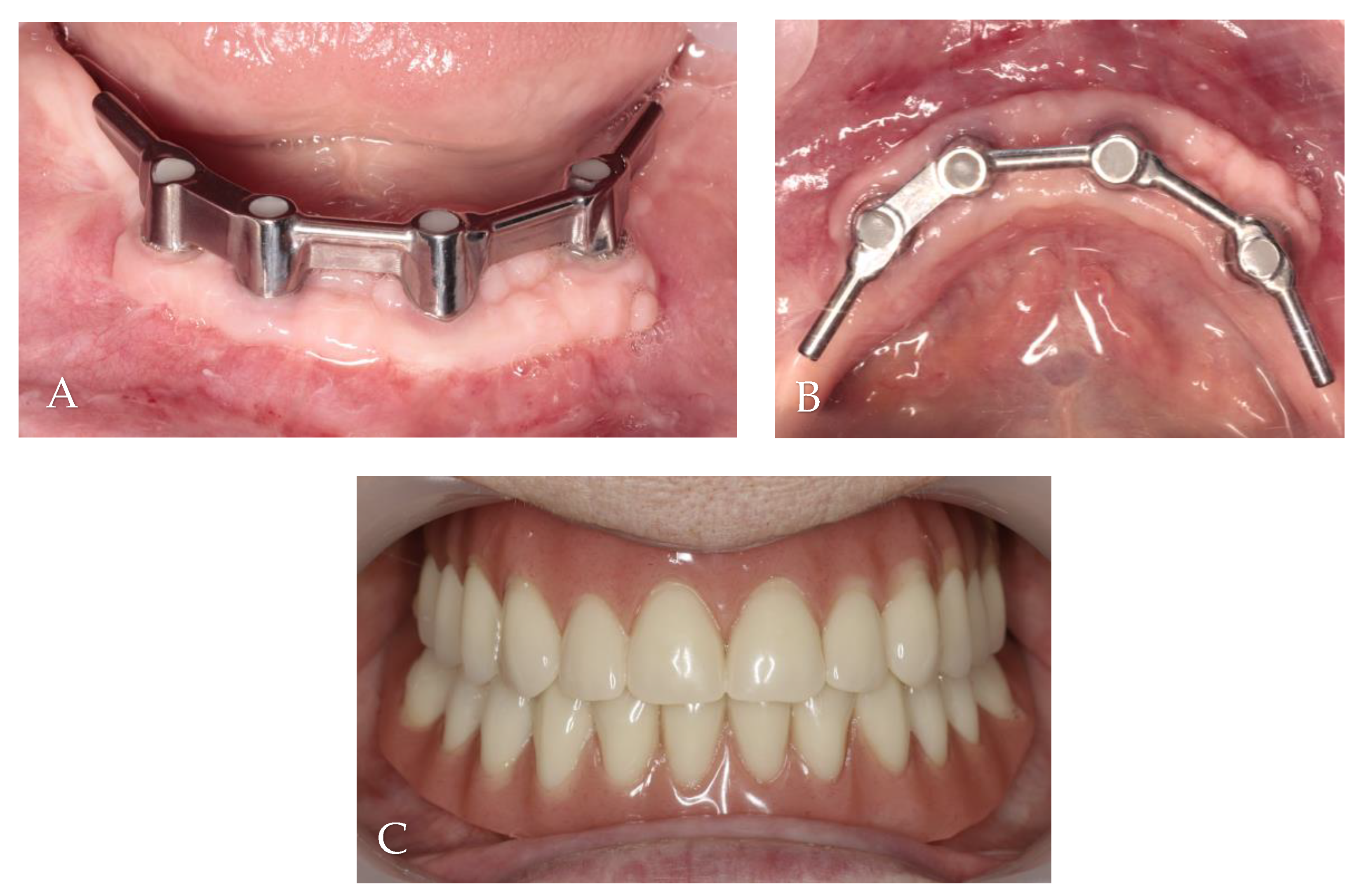
- Bar retained overdenture as the final restoration.
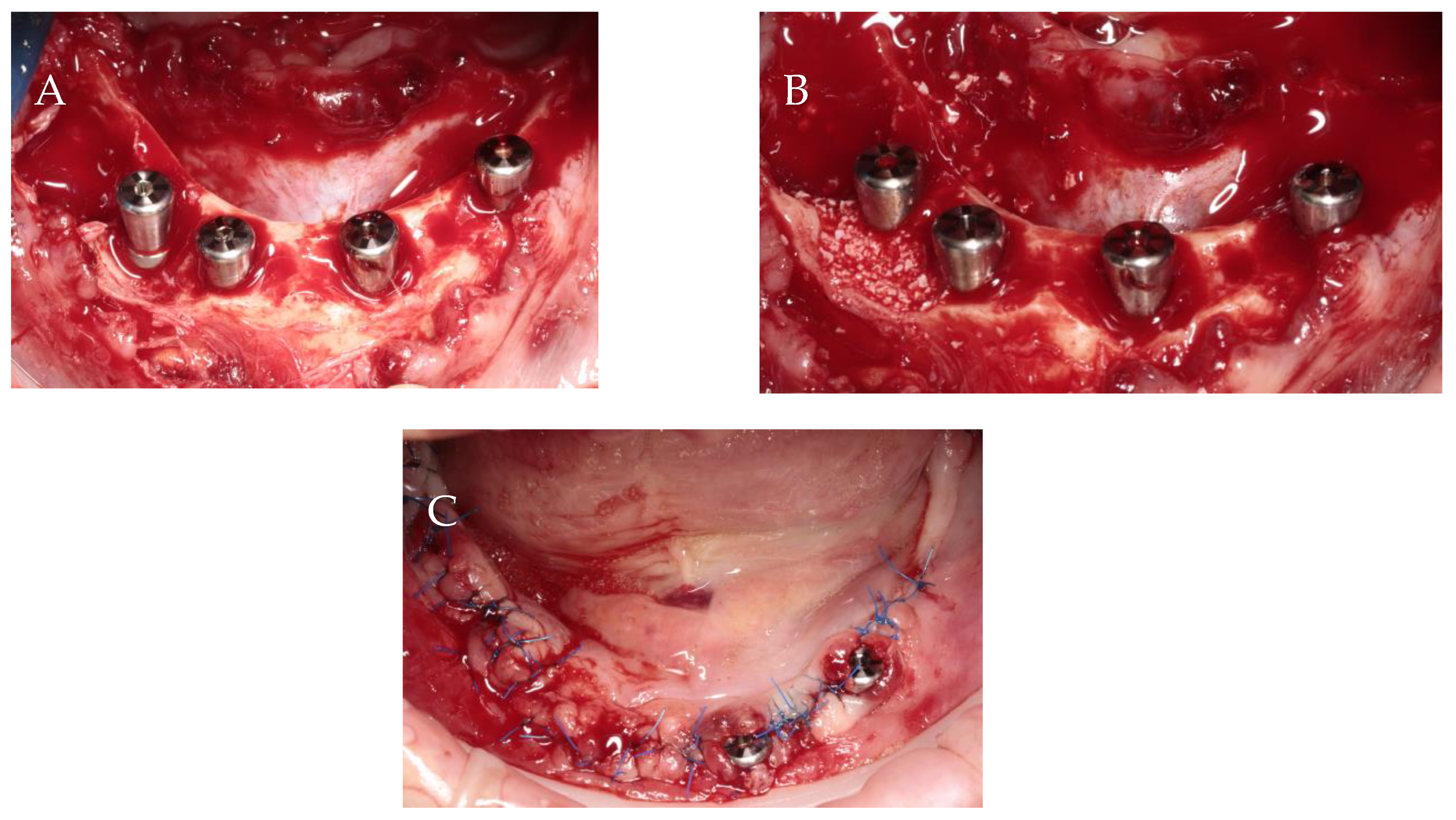
3.2. Surgery 1—Teeth Extraction and Periodontal Lesion Enucleation with Simultaneous Implantation
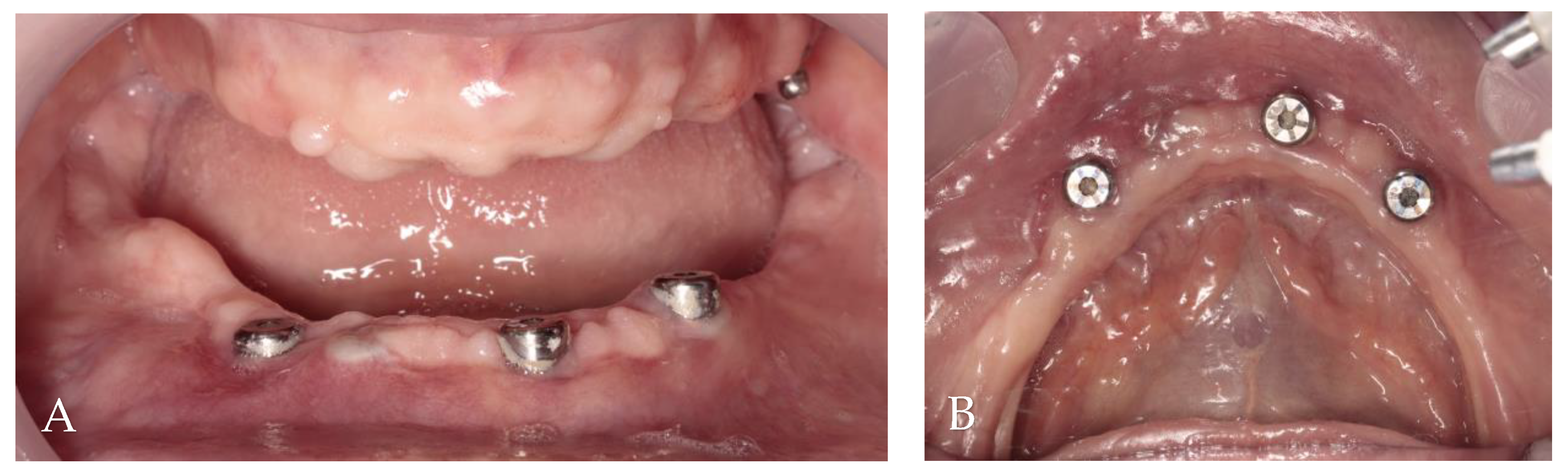
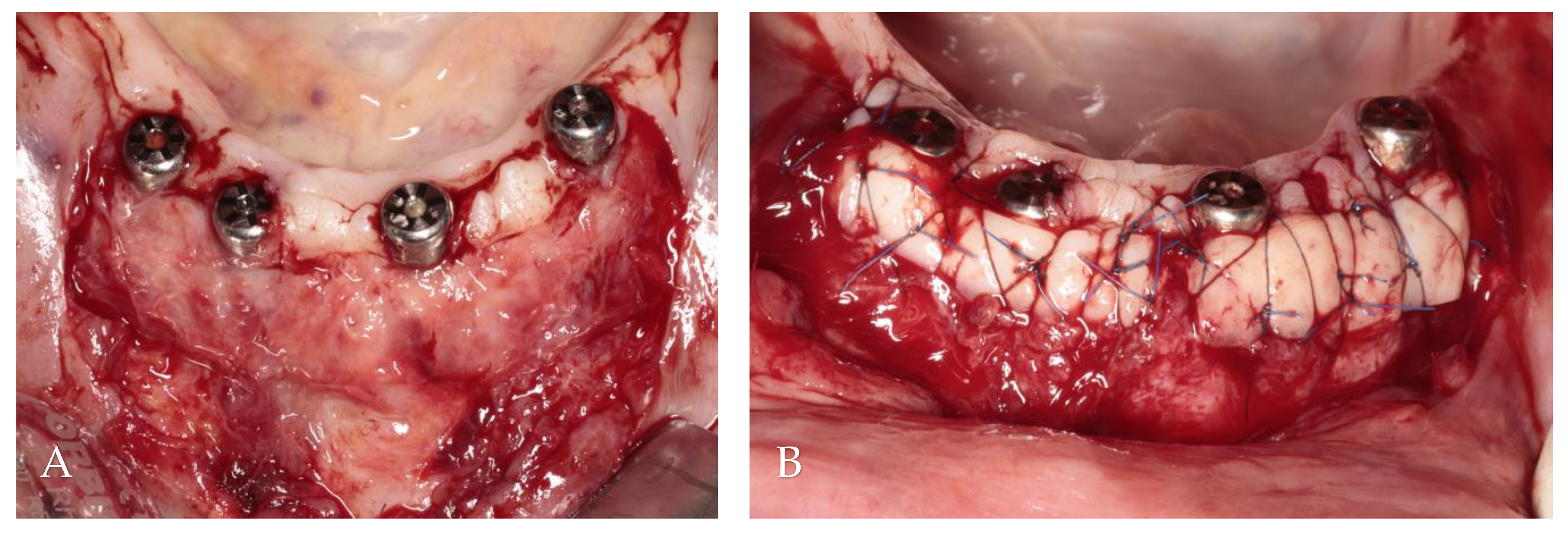
3.3. Surgery 2—Apically Positioned Partial-Thickness Flap (APPTF) in Combination with Free Gingival Grafts (FGGs)
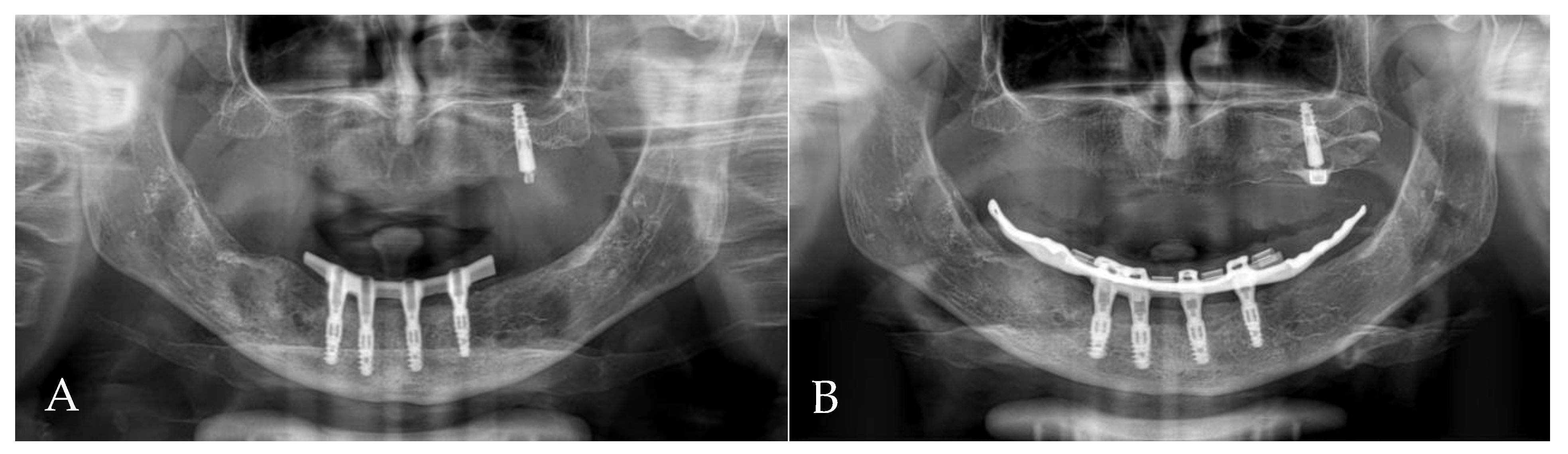
3.4. Results
4. Discussion
5. Conclusions
- (1)
- Many authors agree that keratinized mucosa is essential for maintaining peri-implant health. Nevertheless, there are different opinions about the specific impact of KM on various parameters describing the condition of the tissues in the vicinity of implants.
- (2)
- There is insufficient knowledge in the literature regarding the correlation between inadequate KM and the occurrence of peri-implantitis. Further research in this area is needed, especially case–control studies, cohort studies and randomized clinical trials.
- (3)
- A history of periodontitis is mentioned as one of the risk factors for peri-implantitis.
- (4)
- The present case report described the treatment process of a patient with periodontitis, including immediate implantation in the infected region, soft tissue augmentation using free gingival grafts and the ultimate placement of a bar-retained overdenture as the final restoration. After two years of observation, despite questionable hygiene, no symptoms of gingival inflammation were detected. The orthopantomogram did not show any bone resorption.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal Diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; Imber, J.C.; Marruganti, C.; Salvi, G.E.; Ramieri, G.; Roccuzzo, M. Clinical outcomes of dental implants in patients with and without history of periodontitis: A 20-year prospective study. J. Clin. Periodontol. 2022, 49, 1346–1356. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, Etiology, Prevention and Treatment of Peri-Implantitis—A Review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Naenni, N.; Figuero, E.; Hämmerle, C.H.F.; Schwarz, F.; Jung, R.E.; Sanz-Sánchez, I. Effects of soft tissue augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 32–49. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, R.G.; Stähli, A.; Bassetti, M.A.; Sculean, A. Soft tissue augmentation procedures at second-stage surgery: A systematic review. Clin. Oral Investig. 2016, 20, 1369–1387. [Google Scholar] [CrossRef] [PubMed]
- Mahardawi, B.; Jiaranuchart, S.; Damrongsirirat, N.; Arunjaroensuk, S.; Mattheos, N.; Somboonsavatdee, A.; Pimkhaokham, A. The lack of keratinized mucosa as a risk factor for peri-implantitis: A systematic review and meta-analysis. Sci. Rep. 2023, 13, 3778. [Google Scholar] [CrossRef] [PubMed]
- Ravidà, A.; Arena, C.; Tattan, M.; Caponio, V.C.A.; Saleh, M.H.A.; Wang, H.L.; Troiano, G. The role of keratinized mucosa width as a risk factor for peri-implant disease: A systematic review, meta-analysis, and trial sequential analysis. Clin. Implant Dent. Relat. Res. 2022, 24, 287–300. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Schwarz, F.; Sader, R. Influence of width of keratinized tissue on the prevalence of peri-implant diseases: A systematic review and meta-analysis. Clin. Oral Implants Res. 2022, 33, 8–31. [Google Scholar] [CrossRef]
- Brito, C.; Tenenbaum, H.C.; Wong, B.K.; Schmitt, C.; Nogueira-Filho, G. Is keratinized mucosa indispensable to maintain peri-implant health? A systematic review of the literature. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 643–650. [Google Scholar] [CrossRef]
- Carra, M.C.; Blanc-Sylvestre, N.; Courtet, A.; Bouchard, P. Primordial and primary prevention of peri-implant diseases: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50, 77–112. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, H.; Grischke, J.; Tiede, C.; Eberhard, J.; Schweitzer, A.; Toikkanen, S.E.; Glöckner, S.; Krause, G.; Stiesch, M. Epidemiology and risk factors of periimplantitis: A systematic review. J. Periodontal Res. 2018, 53, 657–681. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; Oh, K.C.; Jurado, C.A.; Lee, H. Lack of keratinized mucosa increases peri-implantitis risk. Evid. Based Dent. 2023, 24, 118–120. [Google Scholar] [CrossRef]
- Stefanini, M.; Barootchi, S.; Sangiorgi, M.; Pispero, A.; Grusovin, M.G.; Mancini, L.; Zucchelli, G.; Tavelli, L. Do Soft Tissue Augmentation Techniques Provide Stable and Favorable Peri-implant Conditions in the Medium and Long Term? A Systematic Review. Clin. Oral Implants Res. 2023, 34 (Suppl. 26), 28–42. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef]
- Lee, J.; Park, D.; Koo, K.T.; Seol, Y.J.; Lee, Y.M. Comparison of Immediate Implant Placement in Infected and Non-Infected Extraction Sockets: A Systematic Review and Meta-Analysis. Acta Odontol. Scand. 2018, 76, 338–345. [Google Scholar] [CrossRef]
- Li, S.; Di, P.; Zhang, Y.; Lin, Y. Immediate Implant and Rehabilitation Based on All-on-4 Concept in Patients with Generalized Aggressive Periodontitis: A Medium-Term Prospective Study. Clin. Implant Dent. Relat. Res. 2017, 19, 559–571. [Google Scholar] [CrossRef]
- Lee, J.; Kim, S.; Koo, K.T.; Seol, Y.J.; Cho, H.J.; Lee, Y.M. Histologic Analyses of Immediate Implant Placement in Infected and Noninfected Sockets: An Experimental Pilot Study in Beagle Dogs. Int. J. Oral Maxillofac. Implants 2019, 34, 575–584. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Fresh-Socket Implants in Periapical Infected Sites in Humans. J. Periodontol. 2010, 81, 378–383. [Google Scholar] [CrossRef]
- Bouri, A., Jr.; Bissada, N.; Al-Zahrani, M.S.; Faddoul, F.; Nouneh, I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int. J. Oral Maxillofac. Implants 2008, 23, 323–326. [Google Scholar]
- Schrott, A.R.; Jimenez, M.; Hwang, J.W.; Fiorellini, J.; Weber, H.P. Five-year evaluation of the influence of keratinized mucosa on peri-implant soft-tissue health and stability around implants supporting full-arch mandibular fixed prostheses. Clin. Oral Implants Res. 2009, 20, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Adibrad, M.; Shahabuei, M.; Sahabi, M. Significance of the width of keratinized mucosa on the health status of the supporting tissue around implants supporting overdentures. J. Oral Implantol. 2009, 35, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Zigdon, H.; Machtei, E.E. The dimensions of keratinized mucosa around implants affect clinical and immunological parameters. Clin. Oral Implants Res. 2008, 19, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.H.; Chan, H.L.; Wang, H.L. The significance of keratinized mucosa on implant health: A systematic review. J. Periodontol. 2013, 84, 1755–1767. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.M.; Oh, T.J.; Shotwell, J.L.; Misch, C.E.; Wang, H.L. Significance of keratinized mucosa in maintenance of dental implants with different surfaces. J. Periodontol. 2006, 77, 1410–1420. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.L.; Masri, R.M.; Williams, D.A.; Ji, C.; Romberg, E. Free gingival grafts for implants exhibiting lack of keratinized mucosa: A prospective controlled randomized clinical study. J. Clin. Periodontol. 2017, 44, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Kim, Y.K.; Yun, P.Y.; Yi, Y.J.; Lee, H.J.; Kim, S.G.; Son, J.S. Evaluation of peri-implant tissue response according to the presence of keratinized mucosa. Oral Surg. Oral. Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e24–e28. [Google Scholar] [CrossRef] [PubMed]
- Fons-Badal, C.; Agustín-Panadero, R.; Labaig-Rueda, C.; Solá-Ruiz, M.F.; García-Selva, M.; Fons Font, A. The Influence of Keratinized Mucosa on the Nonsurgical Therapeutic Treatment of Peri-Implantitis. J. Clin. Med. 2022, 11, 4118. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Effectiveness of Implant Therapy Analyzed in a Swedish Population: Prevalence of Peri-implantitis. J. Dent. Res. 2016, 95, 43–49. [Google Scholar] [CrossRef]
- Carra, M.C.; Rangé, H.; Swerts, P.J.; Tuand, K.; Vandamme, K.; Bouchard, P. Effectiveness of implant supported fixed partial denture in patients with history of periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2022, 49, 208–223. [Google Scholar] [CrossRef]
- Stimmelmayr, M.; Stangl, M.; Edelhoff, D.; Beuer, F. Clinical prospective study of a modified technique to extend the keratinized gingiva around implants in combination with ridge augmentation: One-year results. Int. J. Oral Maxillofac. Implants 2011, 26, 1094–1101. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication | Number of Included Studies | Results | Conclusions |
|---|---|---|---|
| 1. Thoma et al., 2018 [5] | 10 | Surgical interventions aimed at augmenting keratinized tissue demonstrated a notably superior enhancement in gingival index values when compared to both groups with or without keratinized tissue. | Soft tissue grafting techniques lead to improved peri-implant health outcomes. |
| 2. Mahardawi et al., 2023 [7] | 22 (16 were meta-analyzed) | The overall analysis revealed that the absence of keratinized mucosa correlated with an increased occurrence of peri-implantitis. | Insufficient keratinized mucosa is a risk factor, elevating the prevalence of peri-implantitis and highlighting the necessity of consideration during dental implant placement. |
| 3. Ravidà et al., 2022 [8] | 9 (4 in the meta-analysis) | There were no notable differences between groups, and limited evidence was found for probing depth, marginal bone loss and soft-tissue recession. However, a significant advantage was observed for a keratinized mucosa width (KMW) of at least 2 mm, with a lower mean plaque index, as indicated by three studies involving (430 implants, low-quality evidence). | The impact of keratinized mucosa width (KMW) as an underlying factor for peri-implantitis remains minimal. |
| 4. Ramanauskaite et al., 2022 [9] | 22 articles (21 studies) | Peri-implant mucositis and peri-implantitis were observed in 20.8% to 42% and at 10.5% to 44% of the implants with less than 2 mm or absent (0 mm). Conversely, at implant sites with a KT width of at least 2 mm or more than 0 mm, the corresponding values were 20.5% to 53% and 5.1% to 8%, respectively. | Inadequate KT width is correlated with heightened occurrences of peri-implantitis, plaque accumulation, soft-tissue inflammation, mucosal recession, marginal bone loss and greater patient discomfort. |
| 5. Brito et al., 2014 [10] | 7 | Bleeding indexes were noted in five studies overall, with three studies showing a clear association between higher bleeding indexes of implants with a perimeter of less than 2 mm. Additionally, five studies found significantly higher plaque scores in areas with insufficient KM width (<2 mm), while one study found no notable differences between sufficient and insufficient KM widths. | Having enough keratinized tissue around implants might be crucial as it has been demonstrated to correlate with better peri-implant tissue health. |
| 6. Carra et al., 2023 [11] | 48 | Dental implants inserted in sites with augmented peri-implant keratinized mucosa (PIKM) tend to exhibit reduced inflammation and lower marginal bone level (MBL) changes (compared to implants with inadequate PIKM). | Augmentation procedures for peri-implant keratinized mucosa (PIKM) in cases of deficiency may promote better management of peri-implant inflammation and help maintain stability in marginal bone levels. |
| 7. Dreyer et al., 2018 [12] | 57 | There is not sufficient convincing or strong evidence available to suggest that the absence of keratinized mucosa is a significant risk factor for peri-implantitis. | The overall level of evidence to answer the research question is considered weak. Future studies, ideally prospective, randomized and controlled with adequate sample sizes, are necessary to provide more information. |
| 8. Afrashtehfar et al., 2023 [13] | 22 (16 were meta-analyzed) | Research specifically targeting fixed prostheses showed correlation between the absence of keratinized mucosa and a higher incidence of peri-implantitis. This association remains significant even in patients receiving regular implant maintenance. Studies that accounted for other variables also reinforced the elevated risk of peri-implantitis in cases of insufficient keratinized mucosa. | The lack of KM was found to elevate the risk of peri-implantitis, underscoring the importance of taking it into account when placing dental implants. |
| 9. Stefanini et al., 2023 [14] | 15 | The majority of the enhanced implant sites sustained peri-implant health over the medium and long term, with the occurrence of peri-implant mucositis ranging from 0% to 50% and peri-implantitis from 0% to 7.14%. | Implants that received soft tissue augmentation procedures demonstrated a consistently high overall survival rate and a relatively low occurrence of peri-implantitis in the medium and long term. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jankowski, T.; Jankowska, A.; Kazimierczak, N.; Kazimierczak, W.; Janiszewska-Olszowska, J. The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation. J. Clin. Med. 2024, 13, 3501. https://doi.org/10.3390/jcm13123501
Jankowski T, Jankowska A, Kazimierczak N, Kazimierczak W, Janiszewska-Olszowska J. The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation. Journal of Clinical Medicine. 2024; 13(12):3501. https://doi.org/10.3390/jcm13123501
Chicago/Turabian StyleJankowski, Tomasz, Agnieszka Jankowska, Natalia Kazimierczak, Wojciech Kazimierczak, and Joanna Janiszewska-Olszowska. 2024. "The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation" Journal of Clinical Medicine 13, no. 12: 3501. https://doi.org/10.3390/jcm13123501
APA StyleJankowski, T., Jankowska, A., Kazimierczak, N., Kazimierczak, W., & Janiszewska-Olszowska, J. (2024). The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation. Journal of Clinical Medicine, 13(12), 3501. https://doi.org/10.3390/jcm13123501