

Associations between Peritonsillar Abscess and Deep Neck Infection in Chronic Periodontitis Patients: Two Nested Case—Control Studies Using a National Health Screening Cohort

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Ethical Consideration
2.2. Chronic Periodontitis (Outcome)
2.3. Peritonsillar Abscess (Exposure)
2.4. Deep neck Infection (Exposure)
2.5. Study Population
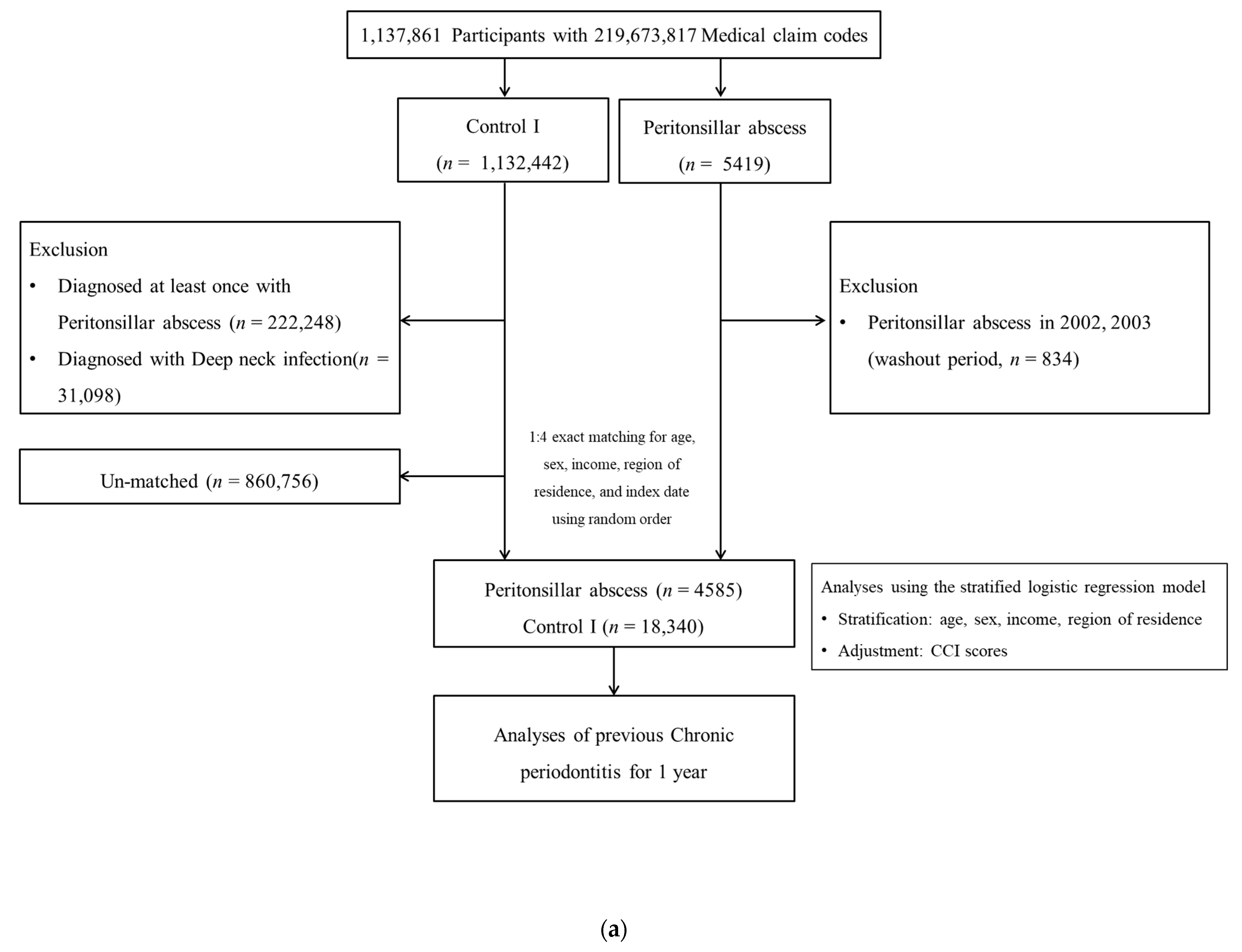
2.5.1. Study I
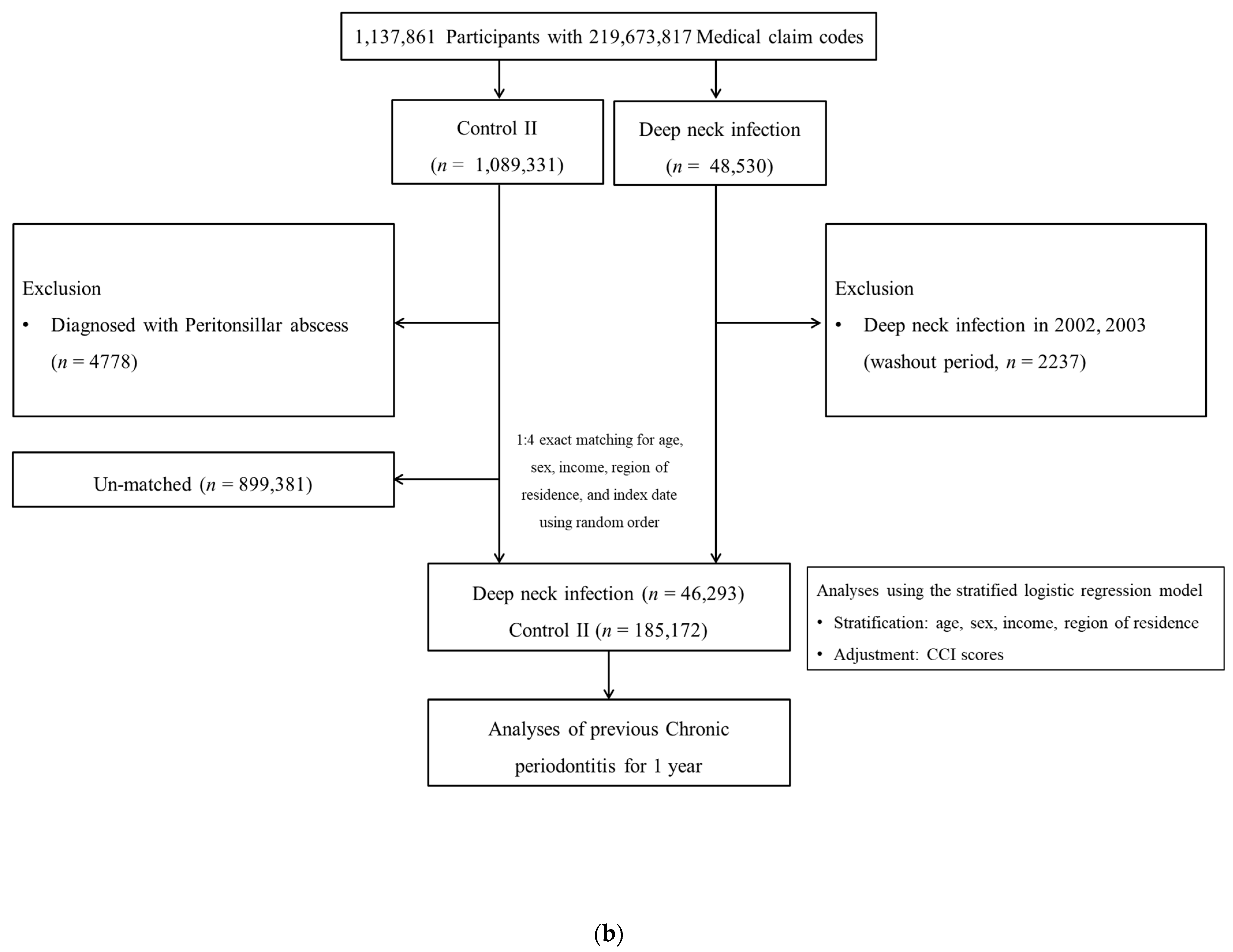
2.5.2. Study II
2.6. Variables
2.7. Statistical Methods
3. Results
3.1. Study I
3.2. Study II
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vieira, F.; Allen, S.M.; Stocks, R.M.; Thompson, J.W. Deep neck infection. Otolaryngol. Clin. North Am. 2008, 41, 459–483. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Nath, G.; Mishra, A. Clinico-Pathological Profile of Deep Neck Space Infection: A Prospective Study. Indian J. Otolaryngol. Head Neck Surg. 2017, 69, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Gargava, A.; Raghuwanshi, S.K.; Verma, P.; Jaiswal, S. Deep Neck Space Infection a Study of 150 Cases at Tertiary Care Hospital. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 5832–5835. [Google Scholar] [CrossRef]
- Alotaibi, N.; Cloutier, L.; Khaldoun, E.; Bois, E.; Chirat, M.; Salvan, D. Criteria for admission of odontogenic infections at high risk of deep neck space infection. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Klug, T.E.; Rusan, M.; Fuursted, K.; Ovesen, T. Peritonsillar Abscess: Complication of Acute Tonsillitis or Weber’s Glands Infection? Otolaryngol. Head Neck Surg. 2016, 155, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, K.; Takeuchi, M.; Kishimoto, Y.; Omori, K.; Kawakami, K. Risk Factors for Recurrence of Peritonsillar Abscess. Laryngoscope 2023, 133, 1846–1852. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lim, H.; Choi, H.G. Smoking and Alcohol Consumption Are Associated With the Increased Risk of Peritonsillar Abscess. Laryngoscope 2020, 130, 2833–2838. [Google Scholar] [CrossRef]
- Papalia, E.; Rena, O.; Oliaro, A.; Cavallo, A.; Giobbe, R.; Casadio, C.; Maggi, G.; Mancuso, M. Descending necrotizing mediastinitis: Surgical management. Eur. J. Cardiothorac. Surg. 2001, 20, 739–742. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Reis, C.; Manzanares-Cespedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. S1), S1–S8. [Google Scholar] [CrossRef]
- Cecoro, G.; Annunziata, M.; Iuorio, M.T.; Nastri, L.; Guida, L. Periodontitis, Low-Grade Inflammation and Systemic Health: A Scoping Review. Medicina 2020, 56, 272. [Google Scholar] [CrossRef] [PubMed]
- Deschamps-Lenhardt, S.; Martin-Cabezas, R.; Hannedouche, T.; Huck, O. Association between periodontitis and chronic kidney disease: Systematic review and meta-analysis. Oral. Dis. 2019, 25, 385–402. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Rinaldi, R.; Staffieri, C.; Marchese-Ragona, R.; Saia, G.; Stramare, R.; Bertolin, A.; Dal Borgo, R.; Ragno, F.; Staffieri, A. Deep neck infection with dental origin: Analysis of 85 consecutive cases (2000–2006). Acta Otolaryngol. 2008, 128, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Ismi, O.; Yesilova, M.; Ozcan, C.; Vayisoglu, Y.; Gorur, K. Difficult Cases of Odontogenic Deep Neck Infections: A Report of Three Patients. Balkan Med. J. 2017, 34, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, T.; Yamamoto, K.; Murakami, K.; Kirita, T. Odontogenic deep neck space infection in a patient with hyper-IgE syndrome: A case report. J. Clin. Exp. Dent. 2018, 10, e1049–e1053. [Google Scholar] [CrossRef] [PubMed]
- Byun, S.H.; Min, C.; Park, I.S.; Kim, H.; Kim, S.K.; Park, B.J.; Choi, H.G.; Hong, S.J. Increased Risk of Chronic Periodontitis in Chronic Rhinosinusitis Patients: A Longitudinal Follow-Up Study Using a National Health-Screening Cohort. J. Clin. Med. 2020, 9, 1170. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kong, I.G.; Min, C.; Choi, H.G. Association of Air Pollution With Increased Risk of Peritonsillar Abscess Formation. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Min, C.; Lee, W.H.; Choi, H.G. Tonsillectomy increases the risk of retropharyngeal and parapharyngeal abscesses in adults, but not in children: A national cohort study. PLoS ONE 2018, 13, e0193913. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Bidirectional Association Between GERD and Asthma: Two Longitudinal Follow-Up Studies Using a National Sample Cohort. J. Allergy Clin. Immunol. Pract. 2020, 8, 1005–1013.e1009. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Kinzer, S.; Pfeiffer, J.; Becker, S.; Ridder, G.J. Severe deep neck space infections and mediastinitis of odontogenic origin: Clinical relevance and implications for diagnosis and treatment. Acta Otolaryngol. 2009, 129, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, N.; Collyer, J.; Bowe, C.M. Neutrophil to lymphocyte ratio as a prognostic marker of deep neck space infections secondary to odontogenic infection. Br. J. Oral. Maxillofac. Surg. 2021, 59, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Alarcon-Sanchez, M.A.; Becerra-Ruiz, J.S.; Guerrero-Velazquez, C.; Mosaddad, S.A.; Heboyan, A. The role of the CX3CL1/CX3CR1 axis as potential inflammatory biomarkers in subjects with periodontitis and rheumatoid arthritis: A systematic review. Immun. Inflamm. Dis. 2024, 12, e1181. [Google Scholar] [CrossRef] [PubMed]
- Chi, T.H.; Tsao, Y.H.; Yuan, C.H. Influences of patient age on deep neck infection: Clinical etiology and treatment outcome. Otolaryngol. Head Neck Surg. 2014, 151, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.Y.; Chin, S.C.; Wang, Y.C.; Chen, S.L. Factors affecting patients with concurrent deep neck infection and aspiration pneumonia. Am. J. Otolaryngol. 2022, 43, 103463. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Mungul, S.; Ahmed, S. Deep Neck Space Infections: Changing Trends in Pediatric Versus Adult Patients. J. Oral. Maxillofac. Surg. 2020, 78, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Mungul, S.; Maharaj, S. Microbiology of paediatric deep neck space infection. Int. J. Pediatr. Otorhinolaryngol. 2019, 123, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Park, J.O.; Kim, J.H.; Joo, Y.H.; Kim, S.Y.; Kim, G.J.; Kim, H.B.; Lee, D.H.; Hong, H.J.; Park, Y.M.; Chung, E.J.; et al. Guideline for the Surgical Management of Locally Invasive Differentiated Thyroid Cancer From the Korean Society of Head and Neck Surgery. Clin. Exp. Otorhinolaryngol. 2023, 16, 1–19. [Google Scholar] [CrossRef]
- Ku, Y.; Kwon, S.B.; Yoon, J.H.; Mun, S.K.; Chang, M. Machine Learning Models for Predicting the Occurrence of Respiratory Diseases Using Climatic and Air-Pollution Factors. Clin. Exp. Otorhinolaryngol. 2022, 15, 168–176. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| PTA (n, %) | Control I (n, %) | Standardized Difference | |
| Total number | 4585 (100.0) | 18,340 (100.0) | |
| Age (n, %) | 0.00 | ||
| 0–4 | 12 (0.26) | 48 (0.26) | |
| 5–9 | 59 (1.29) | 236 (1.29) | |
| 10–14 | 175 (3.82) | 700 (3.82) | |
| 15–19 | 466 (10.16) | 1864 (10.16) | |
| 20–24 | 488 (10.64) | 1952 (10.64) | |
| 25–29 | 618 (13.48) | 2472 (13.48) | |
| 30–34 | 543 (11.84) | 2172 (11.84) | |
| 35–39 | 510 (11.12) | 2040 (11.12) | |
| 40–44 | 453 (9.88) | 1812 (9.88) | |
| 45–49 | 331 (7.22) | 1324 (7.22) | |
| 50–54 | 279 (6.09) | 1116 (6.09) | |
| 55–59 | 215 (4.69) | 860 (4.69) | |
| 60–64 | 166 (3.62) | 664 (3.62) | |
| 65–69 | 126 (2.75) | 504 (2.75) | |
| 70–74 | 71 (1.55) | 284 (1.55) | |
| 75–79 | 48 (1.05) | 192 (1.05) | |
| 80–84 | 18 (0.39) | 72 (0.39) | |
| 85+ | 7 (0.15) | 28 (0.15) | |
| Sex (n, %) | 0.00 | ||
| Male | 2750 (59.98) | 11,000 (59.98) | |
| Female | 1835 (40.02) | 7340 (40.02) | |
| Income (n, %) | 0.00 | ||
| 1 (lowest) | 844 (18.41) | 3376 (18.41) | |
| 2 | 770 (16.79) | 3080 (16.79) | |
| 3 | 886 (19.32) | 3544 (19.32) | |
| 4 | 994 (21.68) | 3976 (21.68) | |
| 5 (highest) | 1091 (23.79) | 4364 (23.79) | |
| Region of residence (n, %) | 0.00 | ||
| Urban | 2179 (47.52) | 8716 (47.52) | |
| Rural | 2406 (52.48) | 9624 (52.48) | |
| CCI score (Mean, SD) | 0.37 (1.03) | 0.31 (0.98) | 0.05 |
| Number of CP treatments (Mean, SD) | 0.26 (0.90) | 0.24 (0.92) | 0.02 |
| Characteristics | Odds Ratios for PTA (95% Confidence Interval) | |||
|---|---|---|---|---|
| Crude † | p-Value | Adjusted ‡ | p-Value | |
| Total participants (n = 22,925) | 1.27 (0.90–1.79) | 0.175 | 1.28 (0.91–1.81) | 0.154 |
| Age < 35 years old (n = 11,805) | 1.43 (0.61–3.35) | 0.415 | 1.45 (0.62–3.41) | 0.392 |
| Age ≥ 35 years old (n = 11,120) | 1.24 (0.85–1.81) | 0.261 | 1.25 (0.86–1.83) | 0.241 |
| Male (n = 13,750) | 1.28 (0.84–1.95) | 0.243 | 1.29 (0.85–1.95) | 0.238 |
| Female (n = 9175) | 1.24 (0.68–2.29) | 0.485 | 1.30 (0.70–2.39) | 0.404 |
| Low-income group (n = 12,500) | 1.30 (0.78–2.16) | 0.307 | 1.31 (0.79–2.18) | 0.297 |
| High-income group (n = 10,425) | 1.24 (0.78–1.99) | 0.366 | 1.27 (0.79–2.03) | 0.328 |
| Urban residents (n = 10,895) | 0.89 (0.54–1.47) | 0.651 | 0.91 (0.55–1.51) | 0.716 |
| Rural residents (n = 12,030) | 1.83 (1.13–2.96) | 0.014 * | 1.84 (1.13–2.97) | 0.013 * |
| CCI scores = 0 (n = 19,224) | 1.17 (0.79–1.73) | 0.444 | 1.20 (0.80–1.79) | 0.384 |
| CCI scores = 1 (n = 2071) | 1.01 (0.41–2.51) | 0.986 | 1.33 (0.53–3.32) | 0.547 |
| CCI scores ≥ 2 (n = 1630) | 2.02 (0.75–5.40) | 0.163 | 2.22 (0.82–6.01) | 0.117 |
| Characteristics | Total Participants | ||
|---|---|---|---|
| DNI (n, %) | Control II (n, %) | Standardized Difference | |
| Total number | 46,293 (100.0) | 185,172 (100.0) | |
| Age (n, %) | 0.00 | ||
| 0–4 | 3265 (7.05) | 13,060 (7.05) | |
| 5–9 | 2853 (6.16) | 11,412 (6.16) | |
| 10–14 | 2616 (5.65) | 10,464 (5.65) | |
| 15–19 | 3189 (6.89) | 12,756 (6.89) | |
| 20–24 | 3023 (6.53) | 12,092 (6.53) | |
| 25–29 | 3922 (8.47) | 15,688 (8.47) | |
| 30–34 | 4657 (10.06) | 18,628 (10.06) | |
| 35–39 | 4727 (10.21) | 18,908 (10.21) | |
| 40–44 | 3903 (8.43) | 15,612 (8.43) | |
| 45–49 | 3303 (7.13) | 13,212 (7.13) | |
| 50–54 | 2973 (6.42) | 11,892 (6.42) | |
| 55–59 | 2483 (5.36) | 9932 (5.36) | |
| 60–64 | 1931 (4.17) | 7724 (4.17) | |
| 65–69 | 1373 (2.97) | 5492 (2.97) | |
| 70–74 | 982 (2.12) | 3928 (2.12) | |
| 75–79 | 637 (1.38) | 2548 (1.38) | |
| 80–84 | 323 (0.70) | 1292 (0.70) | |
| 85+ | 133 (0.29) | 532 (0.29) | |
| Sex (n, %) | 0.00 | ||
| Male | 20,777 (44.88) | 83,108 (44.88) | |
| Female | 25,516 (55.12) | 102,064 (55.12) | |
| Income (n, %) | 0.00 | ||
| 1 (lowest) | 7331 (15.84) | 29,324 (15.84) | |
| 2 | 6621 (14.30) | 26,484 (14.30) | |
| 3 | 8808 (19.03) | 35,232 (19.03) | |
| 4 | 11,028 (23.82) | 44,112 (23.82) | |
| 5 (highest) | 12,505 (27.01) | 50,020 (27.01) | |
| Region of residence (n, %) | 0.00 | ||
| Urban | 21,228 (45.86) | 84,912 (45.86) | |
| Rural | 25,065 (54.14) | 100,260 (54.14) | |
| CCI score (Mean, SD) | 0.33 (0.96) | 0.31 (0.96) | 0.02 |
| Number of CP treatments (Mean, SD) | 0.33 (1.05) | 0.28 (0.98) | 0.04 |
| Characteristics | Odds Ratios for DNI (95% Confidence Interval) | |||
|---|---|---|---|---|
| Crude † | p-Value | Adjusted ‡ | p-Value | |
| Total participants (n = 231,465) | 1.54 (1.40–1.70) | <0.001 * | 1.55 (1.41–1.71) | <0.001 * |
| Age < 35 years old (n = 117,625) | 1.76 (1.36–2.29) | <0.001 * | 1.76 (1.36–2.29) | <0.001 * |
| Age ≥ 35 years old (n = 113,840) | 1.51 (1.36–1.68) | <0.001 * | 1.52 (1.36–1.69) | <0.001 * |
| Male (n = 103,885) | 1.62 (1.40–1.87) | <0.001 * | 1.63 (1.41–1.88) | <0.001 * |
| Female (n = 127,580) | 1.48 (1.29–1.69) | <0.001 * | 1.48 (1.30–1.70) | <0.001 * |
| Low-income group (n = 113,800) | 1.64 (1.41–1.89) | <0.001 * | 1.64 (1.42–1.90) | <0.001 * |
| High-income group (n = 117,665) | 1.47 (1.29–1.68) | <0.001 * | 1.48 (1.29–1.69) | <0.001 * |
| Urban residents (n = 106,140) | 1.44 (1.25–1.67) | <0.001 * | 1.45 (1.25–1.67) | <0.001 * |
| Rural residents (n = 125,325) | 1.64 (1.43–1.88) | <0.001 * | 1.65 (1.44–1.89) | <0.001 * |
| CCI scores = 0 (n = 194,230) | 1.52 (1.36–1.70) | <0.001 * | 1.56 (1.40–1.75) | <0.001 * |
| CCI scores = 1 (n = 21,585) | 1.19 (0.89–1.58) | 0.239 | 1.35 (1.01–1.81) | 0.043 * |
| CCI scores ≥ 2 (n = 15,650) | 1.57 (1.20–2.06) | 0.001 * | 1.61 (1.23–2.12) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Park, I.H.; Byun, C.S.; Choi, H.G.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Kim, C.W. Associations between Peritonsillar Abscess and Deep Neck Infection in Chronic Periodontitis Patients: Two Nested Case—Control Studies Using a National Health Screening Cohort. J. Clin. Med. 2024, 13, 2166. https://doi.org/10.3390/jcm13082166
Kim SY, Park IH, Byun CS, Choi HG, Kwon MJ, Kim JH, Kim J-H, Kim CW. Associations between Peritonsillar Abscess and Deep Neck Infection in Chronic Periodontitis Patients: Two Nested Case—Control Studies Using a National Health Screening Cohort. Journal of Clinical Medicine. 2024; 13(8):2166. https://doi.org/10.3390/jcm13082166
Chicago/Turabian StyleKim, So Young, Il Hwan Park, Chun Sung Byun, Hyo Geun Choi, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, and Chang Wan Kim. 2024. "Associations between Peritonsillar Abscess and Deep Neck Infection in Chronic Periodontitis Patients: Two Nested Case—Control Studies Using a National Health Screening Cohort" Journal of Clinical Medicine 13, no. 8: 2166. https://doi.org/10.3390/jcm13082166
APA StyleKim, S. Y., Park, I. H., Byun, C. S., Choi, H. G., Kwon, M. J., Kim, J. H., Kim, J.-H., & Kim, C. W. (2024). Associations between Peritonsillar Abscess and Deep Neck Infection in Chronic Periodontitis Patients: Two Nested Case—Control Studies Using a National Health Screening Cohort. Journal of Clinical Medicine, 13(8), 2166. https://doi.org/10.3390/jcm13082166