
Melanoma as Subsequent Primary Malignancy in Hematologic Cancer Survivors—A Literature Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Melanoma after Chronic Lymphocytic Leukemia/Small Cell Lymphoma
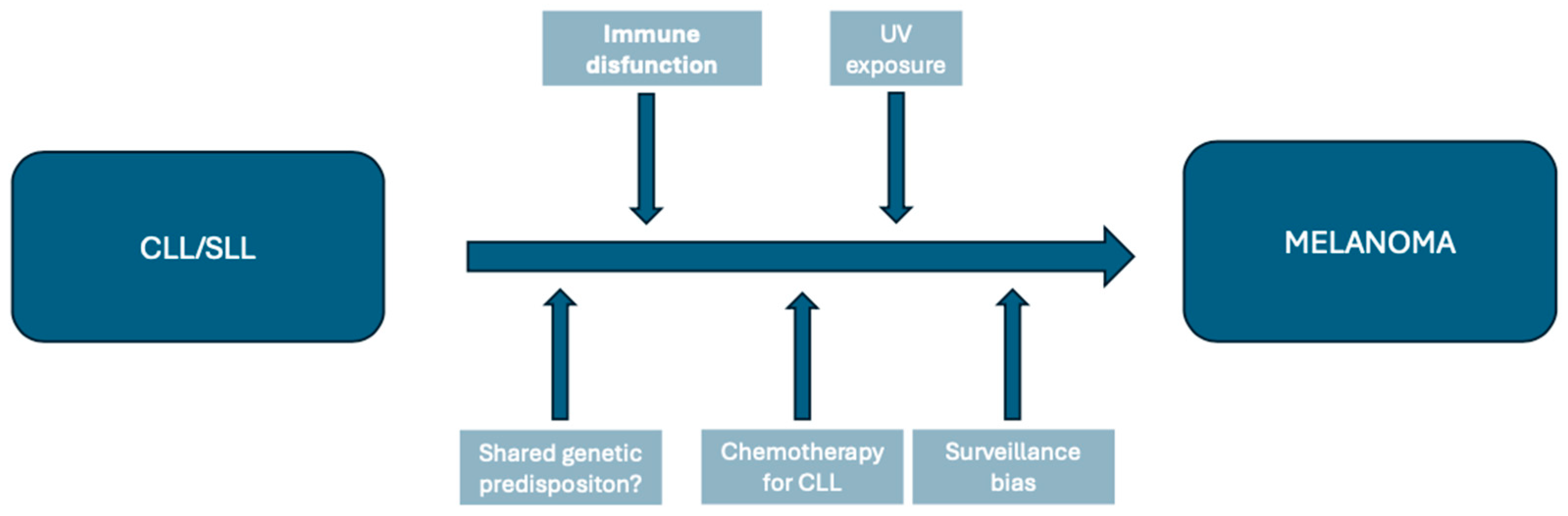
3.1.1. Factors Contributing to Melanoma Risk in CLL/SLL Patients
Immune Dysfunction
Ultraviolet Exposure
Genetic Predisposition
Therapeutic Factors
Surveillance Bias
3.1.2. Impact on Survival
3.1.3. Therapeutic Challenges
3.2. Melanoma as Second Primary Cancer after Non-Hodgkin Lymphoma
Factors Leading to Increased Melanoma Risk in NHL Survivors
3.3. Melanoma Following Hodgkin Lymphoma
3.4. Melanoma Following Primary Cutaneous Lymphoma
3.5. Melanoma Following Multiple Myeloma
3.6. Melanoma Following Philadelphia Chromosome-Negative Myeloproliferative Disorders
3.7. Melanoma Following Hematopoietic Stem Cell Transplantation
4. Implications for Melanoma Screening Recommendations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Devasia, T.; Mariotto, A.B.; Yabroff, K.R.; Jemal, A.; Kramer, J.; Siegel, R.L. Cancer treatment and survivorship statistics 2022. CA Cancer J Clin 2022, 72, 409–436. [Google Scholar] [CrossRef]
- SEER [Internet]. Cancer of Any Site—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/all.html (accessed on 15 April 2024).
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2022–2024; American Cancer Society: Atlanta, GA, USA, 2022. [Google Scholar]
- Zheng, X.; on behalf of Multidisciplinary Oncology Research Collaborative Group (MORCG); Li, X.; Wang, M.; Shen, J.; Sisti, G.; He, Z.; Huang, J.; Li, Y.M.; Wu, A. Second primary malignancies among cancer patients. Ann. Transl. Med. 2020, 8, 638. [Google Scholar] [CrossRef]
- Donin, N.; Filson, C.; Drakaki, A.; Tan, H.; Castillo, A.; Kwan, L.; Litwin, M.; Chamie, K. Risk of second primary malignancies among cancer survivors in the United States, 1992 through 2008. Cancer 2016, 122, 3075–3086. [Google Scholar] [CrossRef]
- Lopes, J.; Rodrigues, C.M.P.; Gaspar, M.M.; Reis, C.P. Melanoma Management: From Epidemiology to Treatment and Latest Advances. Cancers 2022, 14, 4652. [Google Scholar] [CrossRef]
- Arnold, M.; Singh, D.; Laversanne, M.; Vignat, J.; Vaccarella, S.; Meheus, F.; Cust, A.E.; de Vries, E.; Whiteman, D.C.; Bray, F. Global Burden of Cutaneous Melanoma in 2020 and Projections to 2040. JAMA Dermatol 2022, 158, 495–503. [Google Scholar] [CrossRef]
- SEER [Internet]. Melanoma of the Skin—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/melan.html (accessed on 16 April 2024).
- Conforti, C.; Zalaudek, I. Epidemiology and Risk Factors of Melanoma: A Review. Dermatol. Pract. Concept 2021, 11 (Suppl. S1), e2021161S. [Google Scholar] [CrossRef]
- Feller, A.; the NICER Working Group; Matthes, K.L.; Bordoni, A.; Bouchardy, C.; Bulliard, J.-L.; Herrmann, C.; Konzelmann, I.; Maspoli, M.; Mousavi, M.; et al. The relative risk of second primary cancers in Switzerland: A population-based retrospective cohort study. BMC Cancer 2020, 20, 51. [Google Scholar] [CrossRef]
- Caini, S.; Radice, D.; Tosti, G.; Spadola, G.; Cocorocchio, E.; Ferrucci, P.; Testori, A.; Pennacchioli, E.; Fargnoli, M.; Palli, D.; et al. Risk of second primary malignancies among 1537 melanoma patients and risk of second primary melanoma among 52 354 cancer patients in Northern Italy. J. Eur. Acad. Dermatol. Venereol. JEADV 2016, 30, 1491–1496. [Google Scholar] [CrossRef]
- Liu, L.; Soerjomataram, I.; Nijsten, T.; van der Aa, M.; van der Leest, R.; Coebergh, J.W.; de Vries, E. Trends in the risks of melanoma as a second primary cancer among cancer patients in the Netherlands, 1989–2008. Melanoma Res. 2013, 23, 206–212. [Google Scholar] [CrossRef]
- Balamurugan, A.; Rees, J.R.; Kosary, C.; Rim, S.H.; Li, J.; Stewart, S.L. Subsequent primary cancers among men and women with in situ and invasive melanoma of the skin. J. Am. Acad. Dermatol. 2011, 65, S69.e1–S69.e9. [Google Scholar] [CrossRef]
- Zhang, N.; Wu, J.; Wang, Q.; Liang, Y.; Li, X.; Chen, G.; Ma, L.; Liu, X.; Zhou, F. Global burden of hematologic malignancies and evolution patterns over the past 30 years. Blood Cancer J. 2023, 13, 82. [Google Scholar] [CrossRef]
- Allegra, A.; Tonacci, A.; Musolino, C.; Pioggia, G.; Gangemi, S. Secondary Immunodeficiency in Hematological Malignancies: Focus on Multiple Myeloma and Chronic Lymphocytic Leukemia. Front. Immunol. 2021, 12, 738915. [Google Scholar] [CrossRef]
- Travis, L.B. The Epidemiology of Second Primary Cancers. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2020–2026. [Google Scholar] [CrossRef]
- Turk, T.; Saad, A.; Al-Husseini, M.; Gad, M. The risk of melanoma in patients with chronic lymphocytic leukemia; A population-based study. Curr. Probl. Cancer 2019, 44, 100511. [Google Scholar] [CrossRef]
- Herr, M.M.; Schonfeld, S.J.; Dores, G.M.; Withrow, D.R.; A Tucker, M.; E Curtis, R.; Morton, L.M. Mutual Risks of Cutaneous Melanoma and Specific Lymphoid Neoplasms: Second Cancer Occurrence and Survival. J. Natl. Cancer Inst. 2018, 110, 1248–1258. [Google Scholar] [CrossRef]
- Famenini, S.; Martires, K.J.; Zhou, H.; Xavier, M.F.; Wu, J.J. Melanoma in patients with chronic lymphocytic leukemia and non-Hodgkin lymphoma. J. Am. Acad. Dermatol. 2015, 72, 78–84. [Google Scholar] [CrossRef]
- Brewer, J.D.; Shanafelt, T.D.; Call, T.G.; Cerhan, J.R.; Roenigk, R.K.; Weaver, A.L.; Otley, C.C. Increased incidence of malignant melanoma and other rare cutaneous cancers in the setting of chronic lymphocytic leukemia. Int. J. Dermatol. 2015, 54, e287–e293. [Google Scholar] [CrossRef]
- Goggins, W.B.; Finkelstein, D.M.; Tsao, H. Evidence for an association between cutaneous melanoma and non-Hodgkin lymphoma. Cancer 2001, 91, 874–880. [Google Scholar] [CrossRef]
- Ou, Y.; Long, Y.; Ji, L.; Zhan, Y.; Qiao, T.; Wang, X.; Chen, H.; Cheng, Y. Trends in Disease Burden of Chronic Lymphocytic Leukemia at the Global, Regional, and National Levels From 1990 to 2019, and Projections Until 2030: A Population-Based Epidemiologic Study. Front. Oncol. 2022, 12, 840616. [Google Scholar] [CrossRef]
- Yao, Y.; Lin, X.; Li, F.; Jin, J.; Wang, H. The global burden and attributable risk factors of chronic lymphocytic leukemia in 204 countries and territories from 1990 to 2019: Analysis based on the global burden of disease study 2019. Biomed. Eng. OnLine 2022, 21, 4. [Google Scholar] [CrossRef]
- Santos, F.P.S.; O’Brien, S. Small lymphocytic lymphoma and chronic lymphocytic leukemia: Are they the same disease? Cancer J. Sudbury Mass. 2012, 18, 396–403. [Google Scholar] [CrossRef]
- Hisada, M.; Biggar, R.J.; Greene, M.H.; Fraumeni, J.F.; Travis, L.B. Solid tumors after chronic lymphocytic leukemia. Blood 2001, 98, 1979–1981. [Google Scholar] [CrossRef]
- Royle, J.; Baade, P.; Joske, D.; Girschik, J.; Fritschi, L. Second cancer incidence and cancer mortality among chronic lymphocytic leukaemia patients: A population-based study. Br. J. Cancer 2011, 105, 1076–1081. [Google Scholar] [CrossRef]
- Morton, L.M.; Curtis, R.E.; Linet, M.S.; Bluhm, E.C.; Tucker, M.A.; Caporaso, N.; Ries, L.A.; Fraumeni, J.F. Second Malignancy Risks After Non-Hodgkin’s Lymphoma and Chronic Lymphocytic Leukemia: Differences by Lymphoma Subtype. J. Clin. Oncol. 2010, 28, 4935–4944. [Google Scholar] [CrossRef]
- Schöllkopf, C.; Rosendahl, D.; Rostgaard, K.; Pipper, C.; Hjalgrim, H. Risk of second cancer after chronic lymphocytic leukemia. Int. J. Cancer 2007, 121, 151–156. [Google Scholar] [CrossRef]
- McKenna, D.B.; Stockton, D.; Brewster, D.H.; Doherty, V.R. Evidence for an association between cutaneous malignant melanoma and lymphoid malignancy: A population-based retrospective cohort study in Scotland. Br. J. Cancer 2003, 88, 74–78. [Google Scholar] [CrossRef]
- van der Straten, L.; Levin, M.-D.; Dinnessen, M.A.W.; Visser, O.; Posthuma, E.F.M.; Doorduijn, J.K.; Langerak, A.W.; Kater, A.P.; Dinmohamed, A.G. Risk of second primary malignancies in patients with chronic lymphocytic leukemia: A population-based study in the Netherlands, 1989–2019. Blood Cancer J. 2023, 13, 1–10. [Google Scholar] [CrossRef]
- Tsimberidou, A.-M.; Wen, S.; McLaughlin, P.; O’Brien, S.; Wierda, W.G.; Lerner, S.; Strom, S.; Freireich, E.J.; Medeiros, L.J.; Kantarjian, H.M.; et al. Other malignancies in chronic lymphocytic leukemia/small lymphocytic lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 904–910. [Google Scholar] [CrossRef]
- Sayin, S.; Kiliacslan, E.; Yildirim, M.; Ozturk, H.B.A.; Yilmaz, E.S.; Albayrak, M.; Kaptan, M.K.; Ayli, M. Evaluation of Second Primary Cancer Risk Among Chronic Lymphocytic Leukemia Patients: Multicenter Study. Asian Pac. J. Cancer Prev. APJCP 2023, 24, 1971–1977. [Google Scholar] [CrossRef]
- Zheng, G.; Chattopadhyay, S.; Sud, A.; Sundquist, K.; Sundquist, J.; Försti, A.; Houlston, R.; Hemminki, A.; Hemminki, K. Second primary cancers in patients with acute lymphoblastic, chronic lymphocytic and hairy cell leukaemia. Br. J. Haematol. 2019, 185, 232–239. [Google Scholar] [CrossRef]
- Falchi, L.; Vitale, C.; Keating, M.J.; Lerner, S.; Wang, X.; Gbito, K.Y.E.; Strom, S.; Wierda, W.G.; Ferrajoli, A. Incidence and prognostic impact of other cancers in a population of long-term survivors of chronic lymphocytic leukemia. Ann. Oncol. 2016, 27, 1100–1106. [Google Scholar] [CrossRef]
- Shen, Y.; Coyle, L.; Kerridge, I.; Stevenson, W.; Arthur, C.; McKinlay, N.; Fay, K.; Ward, C.; Greenwood, M.; Best, O.G.; et al. Second primary malignancies in chronic lymphocytic leukaemia: Skin, solid organ, haematological and Richter’s syndrome. EJHaem 2021, 3, 129–138. [Google Scholar] [CrossRef]
- Attrill, G.H.; Ferguson, P.M.; Palendira, U.; Long, G.V.; Wilmott, J.S.; Scolyer, R.A. The tumour immune landscape and its implications in cutaneous melanoma. Pigment. Cell Melanoma Res. 2021, 34, 529–549. [Google Scholar] [CrossRef]
- Kubica, A.W.; Brewer, J.D. Melanoma in Immunosuppressed Patients. Mayo Clin. Proc. 2012, 87, 991–1003. [Google Scholar] [CrossRef] [PubMed]
- Slager, S.L.; Benavente, Y.; Blair, A.; Vermeulen, R.; Cerhan, J.R.; Costantini, A.S.; Monnereau, A.; Nieters, A.; Clavel, J.; Call, T.G.; et al. Medical History, Lifestyle, Family History, and Occupational Risk Factors for Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: The InterLymph Non-Hodgkin Lymphoma Subtypes Project. J. Natl. Cancer Inst. Monogr. 2014, 48, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Canchola, A.J.; Cockburn, M.; Lu, Y.; Wang, S.S.; Bernstein, L.; Clarke, C.A.; Horn-Ross, P.L. Adulthood residential ultraviolet radiation, sun sensitivity, dietary vitamin D, and risk of lymphoid malignancies in the California Teachers Study. Blood 2011, 118, 1591–1599. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Xu, F.; Hu, K.; Yin, L.; Duan, H.; Zhang, J.; Zhang, S. Occupational ultraviolet exposure and risk of non-Hodgkin’s lymphomas: A meta-analysis. Oncotarget 2017, 8, 62358–62370. [Google Scholar] [CrossRef]
- Buggins, A.G.S.; Pepper, C.J. The role of Bcl-2 family proteins in chronic lymphocytic leukaemia. Leuk. Res. 2010, 34, 837–842. [Google Scholar] [CrossRef]
- Trisciuoglio, D.; Del Bufalo, D. New insights into the roles of antiapoptotic members of the Bcl-2 family in melanoma progression and therapy. Drug Discov. Today 2021, 26, 1126–1135. [Google Scholar] [CrossRef]
- Crombie, J.; Davids, M.S. IGHV Mutational Status Testing in Chronic Lymphocytic Leukemia. Am. J. Hematol. 2017, 92, 1393–1397. [Google Scholar] [CrossRef] [PubMed]
- Chatzikonstantinou, T.; Scarfò, L.; Karakatsoulis, G.; Minga, E.; Chamou, D.; Iacoboni, G.; Kotaskova, J.; Demosthenous, C.; Smolej, L.; Mulligan, S.; et al. Other malignancies in the history of CLL: An international multicenter study conducted by ERIC, the European Research Initiative on CLL, in HARMONY. eClinicalMedicine 2023, 65, 102307. [Google Scholar] [CrossRef]
- Beiggi, S.; Pannu, M.; Banerji, V.; Dhaliwal, D.H.; Gibson, S.B.; Wiseman, M.; Johnston, J.B. Incidence and Implications of Skin Cancers in Cancercare Manitoba Chronic Lymphocytic Leukemia (CLL) Clinic Patients. Blood 2016, 128, 4359. [Google Scholar] [CrossRef]
- Speedy, H.E.; Kinnersley, B.; Chubb, D.; Broderick, P.; Law, P.J.; Litchfield, K.; Jayne, S.; Dyer, M.J.S.; Dearden, C.; Follows, G.A.; et al. Germ line mutations in shelterin complex genes are associated with familial chronic lymphocytic leukemia. Blood 2016, 128, 2319–2326. [Google Scholar] [CrossRef]
- Potrony, M.; Badenas, C.; Aguilera, P.; Puig-Butille, J.A.; Carrera, C.; Malvehy, J.; Puig, S. Update in genetic susceptibility in melanoma. Ann. Transl. Med. 2015, 3, 210. [Google Scholar] [CrossRef]
- Henry, M.L.; Osborne, J.; Else, T. POT1 Tumor Predisposition. In GeneReviews® [Internet]; Adam, M.P., Feldman, J., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.V., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. Available online: http://www.ncbi.nlm.nih.gov/books/NBK563529/ (accessed on 21 February 2024).
- Wu, Y.; Poulos, R.C.; Reddel, R.R. Role of POT1 in Human Cancer. Cancers 2020, 12, 2739. [Google Scholar] [CrossRef]
- Castellani, G.; Buccarelli, M.; Arasi, M.B.; Rossi, S.; Pisanu, M.E.; Bellenghi, M.; Lintas, C.; Tabolacci, C. BRAF Mutations in Melanoma: Biological Aspects, Therapeutic Implications, and Circulating Biomarkers. Cancers 2023, 15, 4026. [Google Scholar] [CrossRef]
- Sakata-Yanagimoto, M.; Enami, T.; Yokoyama, Y.; Chiba, S. Disease-specific mutations in mature lymphoid neoplasms: Recent advances. Cancer Sci. 2014, 105, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Jebaraj, B.M.C.; Kienle, D.; Bühler, A.; Winkler, D.; Döhner, H.; Stilgenbauer, S.; Zenz, T. BRAF mutations in chronic lymphocytic leukemia. Leuk. Lymphoma 2013, 54, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Giménez, N.; Martínez-Trillos, A.; Montraveta, A.; Lopez-Guerra, M.; Rosich, L.; Nadeu, F.; Valero, J.G.; Aymerich, M.; Magnano, L.; Rozman, M.; et al. Mutations in the RAS-BRAF-MAPK-ERK pathway define a specific subgroup of patients with adverse clinical features and provide new therapeutic options in chronic lymphocytic leukemia. Haematologica 2019, 104, 576–586. [Google Scholar] [CrossRef]
- Sellar, R.S.; Fend, F.; Akarca, A.U.; Agostinelli, C.; Shende, V.; Quintanilla-Martínez, L.; Stein, H.; Pileri, S.A.; Linch, D.; Marafioti, T. BRAF(V600E) mutations are found in Richter syndrome and may allow targeted therapy in a subset of patients. Br. J. Haematol. 2015, 170, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Fürstenau, M.; Giza, A.; Stumpf, T.; Robrecht, S.; Maurer, C.; Linde, H.; Jacobasch, L.; Dörfel, S.; Aldaoud, A.; Tresckow, J.; et al. Second primary malignancies in treated and untreated patients with chronic lymphocytic leukemia. Am. J. Hematol. 2021, 96, E457–E460. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.J.; Curtis, R.E.; Dores, G.M.; Engels, E.A.; Caporaso, N.E.; Polliack, A.; Warren, J.L.; Young, H.A.; Levine, P.H.; Elmi, A.F.; et al. Risk Factors for Melanoma Among Survivors of Non-Hodgkin Lymphoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 3096–3104. [Google Scholar] [CrossRef] [PubMed]
- Jobson, D.; McCormack, C.J.; Mar, V.; Tam, C.; Henderson, M.A. Impact of chronic lymphocytic leukaemia on melanoma outcomes: A retrospective case-control study. Br. J. Haematol. 2022, 197, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Brewer, J.D.; Shanafelt, T.D.; Otley, C.C.; Roenigk, R.K.; Cerhan, J.R.; Kay, N.E.; Weaver, A.L.; Call, T.G. Chronic lymphocytic leukemia is associated with decreased survival of patients with malignant melanoma and Merkel cell carcinoma in a SEER population-based study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Smithy, J.W.; Pianko, M.J.; Maher, C.; Postow, M.A.; Shoushtari, A.N.; Momtaz, P.; Chapman, P.B.; Wolchok, J.D.; Park, J.H.; Callahan, M.K. Checkpoint Blockade in Melanoma Patients with Underlying Chronic Lymphocytic Leukemia. J. Immunother. 2021, 44, 9. [Google Scholar] [CrossRef]
- Van Not, O.J.; Eertwegh, A.J.v.D.; Haanen, J.B.; van Rijn, R.S.; Aarts, M.J.; Berkmortel, F.W.v.D.; Blank, C.U.; Boers-Sonderen, M.J.; van Eijs, M.J.; de Groot, J.-W.B.; et al. Response to checkpoint inhibition and targeted therapy in melanoma patients with concurrent haematological malignancies. Eur. J. Cancer 2023, 186, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Archibald, W.J.; Meacham, P.J.; Williams, A.M.; Baran, A.M.; Victor, A.I.; Barr, P.M.; Sahasrahbudhe, D.M.; Zent, C.S. Management of melanoma in patients with chronic lymphocytic leukemia. Leuk. Res. 2018, 71, 43–46. [Google Scholar] [CrossRef]
- Chu, Y.; Liu, Y.; Fang, X.; Jiang, Y.; Ding, M.; Ge, X.; Yuan, D.; Lu, K.; Li, P.; Li, Y.; et al. The epidemiological patterns of non-Hodgkin lymphoma: Global estimates of disease burden, risk factors, and temporal trends. Front. Oncol. 2023, 13, 1059914. [Google Scholar] [CrossRef]
- Xie, S.; Yu, Z.; Feng, A.; Zheng, S.; Li, Y.; Zeng, Y.; Lyu, J. Analysis and prediction of relative survival trends in patients with non-Hodgkin lymphoma in the United States using a model-based period analysis method. Front. Oncol. 2022, 12, 942122. [Google Scholar] [CrossRef]
- Travis, L.B.; Curtis, R.E.; Glimelius, B.; Holowaty, E.; Leeuwen, F.E.V.; Lynch, C.F.; Adami, J.; Gospodarowicz, M.; Wacholder, S.; Inskip, P.; et al. Second cancers among long-term survivors of non-Hodgkin’s lymphoma. J. Natl. Cancer Inst. 1993, 85, 1932–1937. [Google Scholar] [CrossRef] [PubMed]
- Adami, J.; Frisch, M.; Yuen, J.; Glimelius, B.; Melbye, M. Evidence of an association between non-Hodgkin’s lymphoma and skin cancer. BMJ 1995, 310, 1491–1495. [Google Scholar] [CrossRef] [PubMed]
- Baras, N.; Dahm, S.; Haberland, J.; Janz, M.; Emrich, K.; Kraywinkel, K.; Salama, A. Subsequent malignancies among long-term survivors of Hodgkin lymphoma and non-Hodgkin lymphoma: A pooled analysis of German cancer registry data (1990–2012). Br. J. Haematol. 2017, 177, 226–242. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo Bermejo, J.; Pukkala, E.; Johannesen, T.B.; Sundquist, J.; Hemminki, K. Age-time risk patterns of solid cancers in 60 901 non-Hodgkin lymphoma survivors from Finland, Norway and Sweden. Br. J. Haematol. 2014, 164, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Brennan, P.; Coates, M.; Armstrong, B.; Colin, D.; Boffetta, P. Second primary neoplasms following non-Hodgkin’s lymphoma in New South Wales, Australia. Br. J. Cancer 2000, 82, 1344–1347. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Sud, A.; Zheng, G.; Yu, H.; Sundquist, K.; Sundquist, J.; Försti, A.; Houlston, R.; Hemminki, A.; Hemminki, K. Second primary cancers in non-Hodgkin lymphoma: Bidirectional analyses suggesting role for immune dysfunction. Int. J. Cancer 2018, 143, 2449–2457. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.; Hemminki, K. Second primary neoplasms among 53 159 haematolymphoproliferative malignancy patients in Sweden, 1958–1996: A search for common mechanisms. Br. J. Cancer 2001, 85, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.; Rosendahl, I.; Mattsson, A.; Einhorn, S. Non-Hodgkin’s lymphoma and skin malignancies-shared etiology? Int. J. Cancer 1995, 62, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Parsons, M.W.; Rock, C.; Chipman, J.J.; Shah, H.R.; Hu, B.; Stephens, D.M.; Tao, R.; Tward, J.D.; Gaffney, D.K. Secondary malignancies in non-Hodgkin lymphoma survivors: 40 years of follow-up assessed by treatment modality. Cancer Med. 2023, 12, 2624–2636. [Google Scholar] [CrossRef]
- Royle, J.S.; Baade, P.; Joske, D.; Fritschi, L. Risk of second cancer after lymphohematopoietic neoplasm. Int. J. Cancer 2011, 129, 910–919. [Google Scholar] [CrossRef]
- Giri, S.; Bhatt, V.R.; Verma, V.; Pathak, R.; Bociek, R.G.; Vose, J.M.; Armitage, J.O. Risk of Second Primary Malignancies in Patients with Follicular Lymphoma: A United States Population-based Study. Clin. Lymphoma Myeloma Leuk. 2017, 17, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Brewer, J.D. Skin cancer in patients with non-Hodgkin’s lymphoma. Expert Rev. Dermatol. 2010, 5, 525–533. [Google Scholar] [CrossRef]
- Kim, H.B.; Kim, J.H. Sunlight exposure in association with risk of lymphoid malignancy: A meta-analysis of observational studies. Cancer Causes Control CCC 2021, 32, 441–457. [Google Scholar] [CrossRef]
- A Bilmon, I.; Ashton, L.J.; E Le Marsney, R.; Dodds, A.J.; A O’Brien, T.; Wilcox, L.; Nivison-Smith, I.; Daniels, B.; Vajdic, C.M. Second cancer risk in adults receiving autologous haematopoietic SCT for cancer: A population-based cohort study. Bone Marrow Transplant 2014, 49, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, J.D.; Curtis, R.E.; Socié, G.; Sobocinski, K.A.; Gilbert, E.; Landgren, O.; Travis, L.B.; Travis, W.D.; Flowers, M.E.D.; Friedman, D.L.; et al. Solid cancers after allogeneic hematopoietic cell transplantation. Blood 2009, 113, 1175–1183. [Google Scholar] [CrossRef] [PubMed]
- Peuvrel, L.; Chiffoleau, A.; Quéreux, G.; Brocard, A.; Saint-Jean, M.; Batz, A.; Jolliet, P.; Dréno, B. Melanoma and Rituximab: An Incidental Association? Dermatology 2013, 226, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, V.; Vatve, M.; Longhi, P.; Iqbal, A.; Sripathy, T.K.; Barett, P. Progression of melanoma after treatment with rituximab for lymphoma—Cause or coincidence? J. Am. Acad. Dermatol. 2015, 72, AB174. [Google Scholar] [CrossRef]
- Velter, C.; Pagès, C.; Schneider, P.; Osio, A.; Brice, P.; Lebbé, C. Four cases of rituximab-associated melanoma. Melanoma Res. 2014, 24, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, F.P.; Cetin, G.; Emiroglu, N.; Onsun, N. Is rituximab therapy a risk factor for development of melanoma? Dermatol. Ther. 2020, 33, e13471. [Google Scholar] [CrossRef] [PubMed]
- Fleury, I.; Chevret, S.; Pfreundschuh, M.; Salles, G.; Coiffier, B.; van Oers, M.; Gisselbrecht, C.; Zucca, E.; Herold, M.; Ghielmini, M.; et al. Rituximab and risk of second primary malignancies in patients with non-Hodgkin lymphoma: A systematic review and meta-analysis. Ann. Oncol. 2016, 27, 390–397. [Google Scholar] [CrossRef]
- Huang, J.; Pang, W.S.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M.; Wong, M.C.S. Incidence, mortality, risk factors, and trends for Hodgkin lymphoma: A global data analysis. J. Hematol. Oncol. J. Hematol. Oncol. 2022, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Ansell, S.M. Hodgkin lymphoma: A 2020 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2020, 95, 978–989. [Google Scholar] [CrossRef] [PubMed]
- Townsend, W.; Linch, D. Hodgkin’s lymphoma in adults. Lancet 2012, 380, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Dores, G.M.; Metayer, C.; Curtis, R.E.; Lynch, C.F.; Clarke, E.A.; Glimelius, B.; Storm, H.; Pukkala, E.; van Leeuwen, F.E.; Holowaty, E.J.; et al. Second Malignant Neoplasms Among Long-Term Survivors of Hodgkin’s Disease: A Population-Based Evaluation over 25 Years. J. Clin. Oncol. 2002, 20, 3484–3494. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Garg, M.; Chandra, A.B.; Mayorga, V.S.; Ahmed, S.; Ailawadhi, S. Trends in the Risks of Secondary Cancers in Patients with Hodgkin Lymphoma. Clin. Lymphoma Myeloma Leuk. 2018, 18, 576–589.e1. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, A.F.; Andersen, A.; Nome, O.; Jacobsen, A.B.; Holte, H.; Abrahamsen, J.F.; Kvaløy, S. Long-term risk of second malignancy after treatment of Hodgkin’s disease: The influence of treatment, age and follow-up time. Ann. Oncol. 2002, 13, 1786–1791. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.K.; Bernardo, M.V.P.; Weller, E.; Backstrand, K.; Silver, B.; Marcus, K.C.; Tarbell, N.J.; Stevenson, M.A.; Friedberg, J.W.; Mauch, P.M. Second malignancy after Hodgkin disease treated with radiation therapy with or without chemotherapy: Long-term risks and risk factors. Blood 2002, 100, 1989–1996. [Google Scholar] [CrossRef] [PubMed]
- Daniëls, L.A.; Krol, A.D.; Schaapveld, M.; Putter, H.; Jansen, P.M.; Marijt, E.W.; van Leeuwen, F.E.; Creutzberg, C.L. Long-term risk of secondary skin cancers after radiation therapy for Hodgkin’s lymphoma. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2013, 109, 140–145. [Google Scholar] [CrossRef]
- Dietrich, P.Y.; Henry-Amar, M.; Cosset, J.M.; Bodis, S.; Bosq, J.; Hayat, M. Second Primary Cancers in Patients Continuously Disease-Free from Hodgkin’s Disease: A Protective Role for the Spleen? Blood 1994, 84, 1209–1215. [Google Scholar] [CrossRef]
- Henry-Amar, M. Second cancer after the treatment for Hodgkin’s disease: A report from the International Database on Hodgkin’s Disease. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 1992, 3 (Suppl. 4), 117–128. [Google Scholar] [CrossRef]
- Munker, R.; Grützner, S.; Hiller, E.; Aydemir, Ü.; Enne, W.; Dietzfelbinger, H.; Busch, M.; Haas, R.; Emmerich, B.; Schmidt, M.; et al. Second malignancies after Hodgkin’s disease: The Munich experience. Ann. Hematol. 1999, 78, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Thomsen, H.; Sundquist, K.; Houlston, R.S.; Hemminki, K. Risk of Second Cancer in Hodgkin Lymphoma Survivors and Influence of Family History. J. Clin. Oncol. 2017, 35, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, A.; Barber, J.; Hudson, G.V.; Cunningham, D.; Gupta, R.; Hancock, B.; Horwich, A.; Lister, T.; Linch, D. Risk of Second Malignancy After Hodgkin’s Disease in a Collaborative British Cohort: The Relation to Age at Treatment. J. Clin. Oncol. 2000, 18, 498. [Google Scholar] [CrossRef] [PubMed]
- Abrahão, R.; Brunson, A.M.; Kahn, J.M.; Li, Q.W.; Wun, T.; Keegan, T.H.M. Second primary malignancy risk after Hodgkin lymphoma treatment among HIV-uninfected and HIV-infected survivors. Leuk. Lymphoma 2022, 63, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, A.J.; Higgins, C.D.; Smith, P.; Cunningham, D.; Hancock, B.W.; Horwich, A.; Hoskin, P.J.; Lister, T.A.; Radford, J.A.; Rohatiner, A.Z.; et al. Second Cancer Risk After Chemotherapy for Hodgkin’s Lymphoma: A Collaborative British Cohort Study. J. Clin. Oncol. 2011, 29, 4096–4104. [Google Scholar] [CrossRef] [PubMed]
- Nassi, L.; De Sanctis, V.; Loseto, G.; Gerardi, C.; Allocati, E.; Ciavarella, S.; Minoia, C.; Guarini, A.; Bari, A. Second Cancers in Classical Hodgkin Lymphoma and Diffuse Large B-Cell Lymphoma: A Systematic Review by the Fondazione Italiana Linfomi. Cancers 2022, 14, 519. [Google Scholar] [CrossRef] [PubMed]
- Rosenbrock, J.; Kaul, H.; Oertel, M.; Celik, E.; Linde, P.; Fan, J.; Eichenauer, D.A.; Bröckelmann, P.J.; von Tresckow, B.; Kobe, C.; et al. Involved-site Radiation Therapy is Equally Effective and Less Toxic Than Involved-field Radiation Therapy in Patients Receiving Combined Modality Treatment for Early-stage Unfavorable Hodgkin Lymphoma—An Analysis of the Randomized Phase 3 HD17 Trial of the German Hodgkin Study Group. Int. J. Radiat. Oncol. Biol. Phys. 2024; Online ahead of print. [Google Scholar] [CrossRef]
- Eng, T.; Ha, C.S. Image-guided radiation therapy in lymphoma management. Radiat. Oncol. J. 2015, 33, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Massaccesi, M.; Cusumano, D.; Boldrini, L.; Dinapoli, N.; Fionda, B.; Teodoli, S.; Azario, L.; Mattiucci, G.C.; Balducci, M.; Cellini, F.; et al. A new frontier of image guidance: Organs at risk avoidance with MRI-guided respiratory-gated intensity modulated radiotherapy: Technical note and report of a case. J. Appl. Clin. Med. Phys. 2019, 20, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Hodak, E.; Zinzani, P.L.; Specht, L.; Ladetto, M. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv30–iv40. [Google Scholar] [CrossRef]
- Sokołowska-Wojdyło, M.; Olek-Hrab, K.; Ruckemann-Dziurdzińska, K. Primary cutaneous lymphomas: Diagnosis and treatment. Adv. Dermatol. Allergol. Dermatol. Alergol. 2015, 32, 368–383. [Google Scholar] [CrossRef]
- Miyashiro, D.; Sanches, J.A. Mycosis fungoides and Sézary syndrome: Clinical presentation, diagnosis, staging, and therapeutic management. Front. Oncol. 2023, 13, 1141108. [Google Scholar] [CrossRef]
- Goyal, A.; O’Leary, D.; Goyal, K.; Rubin, N.; Bohjanen, K.; Hordinsky, M.; Chen, S.T.; Pongas, G.; Duncan, L.M.; Lazaryan, A. Increased risk of second primary hematologic and solid malignancies in patients with mycosis fungoides: A Surveillance, Epidemiology, and End Results analysis. J. Am. Acad. Dermatol. 2020, 83, 404–411. [Google Scholar] [CrossRef]
- Huang, K.P.; Weinstock, M.A.; Clarke, C.A.; McMillan, A.; Hoppe, R.T.; Kim, Y.H. Second lymphomas and other malignant neoplasms in patients with mycosis fungoides and Sezary syndrome: Evidence from population-based and clinical cohorts. Arch. Dermatol. 2007, 143, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Brownell, I.; Etzel, C.J.; Yang, D.J.; Taylor, S.H.; Duvic, M. Increased malignancy risk in the cutaneous T-cell lymphoma patient population. Clin. Lymphoma Myeloma 2008, 8, 100–105. [Google Scholar] [CrossRef]
- Almukhtar, R.; Gill, F.; Soine, R.; McBurney, E. Gender differences in the risk of secondary malignancies in patients with mycosis fungoides and Sézary syndrome. J. Am. Acad. Dermatol. 2020, 83, 647–648. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, L.M.; Fenger-Grøn, M.; Iversen, L. Subsequent cancers, mortality, and causes of death in patients with mycosis fungoides and parapsoriasis: A Danish nationwide, population-based cohort study. J. Am. Acad. Dermatol. 2014, 71, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.; Kremer, N.; Dalal, A.; Solomon-Cohen, E.; Berkovich, E.; Noyman, Y.; Ben-Lassan, M.; Levi, A.; Pavlovsky, L.; Naveh, H.; et al. Melanoma Risk is Increased in Patients with Mycosis Fungoides Compared with Patients with Psoriasis and the General Population. Acta Derm. Venereol. 2020, 100, 5950. [Google Scholar] [CrossRef]
- Licata, A.G.; Wilson, L.D.; Braverman, I.M.; Feldman, A.M.; Kacinski, B.M. Malignant melanoma and other second cutaneous malignancies in cutaneous T-cell lymphoma. The influence of additional therapy after total skin electron beam radiation. Arch. Dermatol. 1995, 131, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Lutsyk, M.; Ben-Yosef, R.; Bergman, R.; Kuten, A.; Bar-Sela, G. Total Skin Electron Irradiation and Sequential Malignancies in Mycosis Fungoides Patients: Longitudinal Study. Clin. Oncol. 2018, 30, 618–624. [Google Scholar] [CrossRef]
- Lindahl, L.M.; Fenger-Grøn, M.; Iversen, L. Secondary cancers, comorbidities and mortality associated with nitrogen mustard therapy in patients with mycosis fungoides: A 30-year population-based cohort study. Br. J. Dermatol. 2014, 170, 699–704. [Google Scholar] [CrossRef]
- Evans, A.V.; Scarisbrick, J.J.; Child, F.J.; Acland, K.M.; Whittaker, S.J.; Russell-Jones, R. Cutaneous malignant melanoma in association with mycosis fungoides. J. Am. Acad. Dermatol. 2004, 50, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Błażewicz, I.; Olszewska, B.; Stawczyk-Macieja, M.; Jaœkiewicz, M.; Nowicki, R.; Sokołowska-Wojdyło, M. The incidences of other primary cancers in patients with mycosis fungoides and Sézary syndrome. Adv. Dermatol. Allergol. Dermatol. Alergol. 2021, 38, 289–294. [Google Scholar] [CrossRef]
- Martinez-Escala, M.E.; Amin, S.M.; Sable, K.A.; Gerami, P.; Guitart, J. Multiple melanocytic nevi restricted to mycosis fungoides patches in pediatric and young-adult patients. The potential role of local immunosuppression. Pediatr. Dermatol. 2019, 36, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Scarisbrick, J.J.; Woolford, A.J.; Calonje, E.; Photiou, A.; Ferreira, S.; Orchard, G.; Russell-Jones, R.; Whittaker, S.J. Frequent Abnormalities of the P15 and P16 Genes in Mycosis Fungoides and Sezary Syndrome. J. Investig. Dermatol. 2002, 118, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Gniadecki, R.; O’Keefe, S.; Hennessey, D.; Iyer, A. Is Cutaneous T-Cell Lymphoma Caused by Ultraviolet Radiation? A Comparison of UV Mutational Signatures in Malignant Melanoma and Mycosis Fungoides. Cells 2023, 12, 1616. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.A.; Barsouk, A.; Barsouk, A.; Rawla, P.; Vakiti, A.; Kolhe, R.; Kota, V.; Ajebo, G.H. Epidemiology, Staging, and Management of Multiple Myeloma. Med. Sci. 2021, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Maclachlan, K.; Diamond, B.; Maura, F.; Hillengass, J.; Turesson, I.; Landgren, C.O.; Kazandjian, D. Second malignancies in multiple myeloma; emerging patterns and future directions. Best Pract. Res. Clin. Haematol. 2020, 33, 101144. [Google Scholar] [CrossRef]
- Robinson, A.A.; Wang, J.; Vardanyan, S.; Madden, E.K.; Hebroni, F.; Udd, K.A.; Spektor, T.M.; Nosrati, J.D.; Kitto, A.Z.; Zahab, M.; et al. Risk of skin cancer in multiple myeloma patients: A retrospective cohort study. Eur. J. Haematol. 2016, 97, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.; Weaver, A.; Brewer, J.; Kyle, R.; Baum, C. Risk of malignant melanoma in patients with multiple myeloma. J. Am. Acad. Dermatol. 2015, 72 (Suppl. 1), AB175. [Google Scholar] [CrossRef]
- Langseth, Ø.O.; Myklebust, T.Å.; Johannesen, T.B.; Hjertner, Ø.; Waage, A. Patterns of previous and secondary malignancies in patients with multiple myeloma. Eur. J. Haematol. 2021, 106, 529–536. [Google Scholar] [CrossRef]
- Razavi, P.; Rand, K.A.; Cozen, W.; Chanan-Khan, A.; Usmani, S.; Ailawadhi, S. Patterns of second primary malignancy risk in multiple myeloma patients before and after the introduction of novel therapeutics. Blood Cancer J. 2013, 3, e121. [Google Scholar] [CrossRef] [PubMed]
- Mahindra, A.; Raval, G.; Mehta, P.; Brazauskas, R.; Zhang, M.-J.; Zhong, X.; Bird, J.M.; Freytes, C.O.; Hale, G.A.; Herzig, R.; et al. New Cancers after Autotransplants for Multiple Myeloma. Biol. Blood Marrow Transpl. J. Am. Soc. Blood Marrow Transpl. 2015, 21, 738–745. [Google Scholar] [CrossRef]
- Hoffman, R.; Prchal, J.T.; Samuelson, S.; Ciurea, S.O.; Rondelli, D. Philadelphia Chromosome–Negative Myeloproliferative Disorders: Biology and Treatment. Biol. Blood Marrow Transpl. 2007, 13, 64–72. [Google Scholar] [CrossRef]
- Frederiksen, H.; Farkas, D.K.; Christiansen, C.F.; Hasselbalch, H.C.; Sørensen, H.T. Chronic myeloproliferative neoplasms and subsequent cancer risk: A Danish population-based cohort study. Blood 2011, 118, 6515–6520. [Google Scholar] [CrossRef]
- Landtblom, A.R.; Bower, H.; Andersson, T.M.-L.; Dickman, P.W.; Samuelsson, J.; Björkholm, M.; Kristinsson, S.Y.; Hultcrantz, M. Second malignancies in patients with myeloproliferative neoplasms: A population-based cohort study of 9379 patients. Leukemia 2018, 32, 2203–2210. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Zheng, G.; Sud, A.; Yu, H.; Sundquist, K.; Sundquist, J.; Försti, A.; Hemminki, A.; Houlston, R.; Hemminki, K. Risk of second primary cancer following myeloid neoplasia and risk of myeloid neoplasia as second primary cancer: A nationwide, observational follow up study in Sweden. Lancet Haematol. 2018, 5, e368–e377. [Google Scholar] [CrossRef]
- Fallah, M.; Kharazmi, E.; Sundquist, J.; Hemminki, K. Higher risk of primary cancers after polycythaemia vera and vice versa. Br. J. Haematol. 2011, 153, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Joshi, U.; Bhattarai, A.; Gaire, S.; Gill, S.; Agrawal, V.; Yadav, S.K.; Low, S.K.; Dhakal, P.; Bhatt, V.R.; Kouides, P.A. Risk of second primary malignancy in patients with primary myelofibrosis: A SEER database study. Leuk. Lymphoma 2022, 63, 3456–3461. [Google Scholar] [CrossRef] [PubMed]
- Susini, M.C.; Masala, G.; Antonioli, E.; Pieri, L.; Guglielmelli, P.; Palli, D.; Bosi, A.; Vannucchi, A.M. Risk of second cancers in chronic myeloproliferative neoplasms. Blood 2012, 119, 3861–3862. [Google Scholar] [CrossRef]
- Curtis, R.E.; Rowlings, P.A.; Deeg, H.J.; Shriner, D.A.; Socié, G.; Travis, L.B.; Horowitz, M.M.; Witherspoon, R.P.; Hoover, R.N.; Sobocinski, K.A.; et al. Solid Cancers after Bone Marrow Transplantation. N. Engl. J. Med. 1997, 336, 897–904. [Google Scholar] [CrossRef]
- Martelin, E.; Volin, L.; Itälä-Remes, M.; Niittyvuopio, R.; Lindström, V.; Heiskanen, J.; Ruutu, T.; Nihtinen, A. Incidence and risk factors of secondary cancers after allogeneic stem cell transplantation: Analysis of a single centre cohort with a long follow-up. Bone Marrow Transplant. 2019, 54, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Tichelli, A.; Beohou, E.; Labopin, M.; Socié, G.; Rovó, A.; Badoglio, M.; van Biezen, A.; Bader, P.; Duarte, R.F.; Basak, G.; et al. Evaluation of Second Solid Cancers After Hematopoietic Stem Cell Transplantation in European Patients. JAMA Oncol. 2019, 5, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Omland, S.H.; Gniadecki, R.; Hædersdal, M.; Helweg-Larsen, J.; Omland, L.H. Skin Cancer Risk in Hematopoietic Stem-Cell Transplant Recipients Compared with Background Population and Renal Transplant Recipients: A Population-Based Cohort Study. JAMA Dermatol. 2016, 152, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Killeen, T.F.; Shanley, R.; Ramesh, V.; Giubellino, A. Malignant Melanoma in a Retrospective Cohort of Immunocompromised Patients: A Statistical and Pathologic Analysis. Cancers 2023, 15, 3600. [Google Scholar] [CrossRef] [PubMed]
- Arora, M.; Chen, Y.; Hageman, L.; Wu, J.; Landier, W.; Francisco, L.; Kung, M.; Ness, E.; Ba, A.B.; Pamukcuoglu, M.; et al. Morbidity Burden in Multiple Myeloma Survivors of Autologous Transplant—A Bone Marrow Transplant Survivor Study (BMTSS). Cancer 2020, 126, 3322–3329. [Google Scholar] [CrossRef] [PubMed]
- Herr, M.; Curtis, R.E.; Tucker, M.A.; Tecca, H.R.; Engels, E.A.; Cahoon, E.; Battiwalla, M.; Buchbinder, D.K.; Flowers, M.E.D.; Brazauskas, R.; et al. Risk factors for the development of cutaneous melanoma after allogeneic hematopoietic cell transplantation. J. Am. Acad. Dermatol. 2020, 83, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Shore, R. Radiation-induced skin cancer in human. Med. Pediatr. Oncol. 2001, 36, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.M.; Leachman, S.A.; Aspinwall, L.G.; Cranmer, L.D.; Curiel-Lewandrowski, C.; Sondak, V.K.; Stemwedel, C.E.; Swetter, S.M.; Vetto, J.; Bowles, T.; et al. Skin cancer screening: Recommendations for data-driven screening guidelines and a review of the US Preventive Services Task Force controversy. Melanoma Manag. 2017, 4, 13–37. [Google Scholar] [CrossRef] [PubMed]
- Hepner, A.; Gregorio, J.V.A.M.; Garicochea, B.; Munhoz, R.R. Risk of Melanoma among Survivors of Hematologic Malignancies. Adv. Cancer Prev. 2016, 1, e101. [Google Scholar]
- Baum, J.; Lax, H.; Lehmann, N.; Merkel-Jens, A.; Beelen, D.W.; Jöckel, H.; Dührsen, U. Preventive health care in blood cancer survivors: Results from the ABC study. J. Cancer Res. Clin. Oncol. 2023, 149, 11531–11540. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Year | Country/Registry | First Neoplasm | No Patients Followed | O | SIR (95% CI) | Follow-Up |
|---|---|---|---|---|---|---|---|
| Brewer et al. [21] | 2015 | USA/SEER 13 | CLL | 28,964 | 268 | 2.0 (1.8–2.2) | PYAR, mean ± SD 4.7 ± 3.8 |
| Herr et al. [19] | 2018 | USA/SEER 17 | CLL/SLL | 36,784 | 287 | 1.96 (1.74–2.21) | Mean FU 3.3–6 yrs |
| Hisada et al. [26] | 2001 | USA/SEER | CLL | 16,367 | 90 | 3.18 (NR) | 84,667 PYFU |
| McKenna et al. [30] | 2003 | Scotland/ SCR | CLL | 4016 | 6 | 2.3 (0.0–2.4) n.s | 14,450 PYFU |
| Morton et al. [28] | 2010 | USA/SEER 11 | CLL/SLL | 15,915 | 85 | 1.92 (1.53–2.37) | 4.3 Mean PYFU |
| Royle et al. [27] | 2011 | Australia/NCSCH | CLL | 13,580 | 272 | 7.74 (6.85–8.72) | 75,878 PYFU |
| Schöllkopf et al. [29] | 2007 | Denmark/DCR | CLL | 12,373 | 27 | 2.42 (1.66–3.53) | 47,636 PYFU |
| van der Straten et al. [31] | 2023 | Netherlands/NCR | CLL | 24,815 | 278 | 2.74 (2.43–3.08) | 162,698 PYFU |
| Turk et al. [18] | 2019 | USA/SEER 18 | CLL | 48,876 | 474 | 2.07 (1.89–2.27) | ns |
| Authors | Year of Publication | SIR in Men | SIR in Women |
|---|---|---|---|
| Brewer et al. [21] | 2015 | 2.0 | 1.9 |
| Herr et al. [19] | 2018 | 2.01 | 1.81 |
| Hisada et al. [26] | 2001 | 3.14 | 3.28 |
| McKenna et al. [30] | 2003 | 2.9 | 1.6 |
| Royle et al. [27] | 2011 | 7.40 | 6.40 |
| Van der Straten et al. [31] | 2023 | 2.80 | 2.63 |
| Authors | N | No Receiving Ch/R | No of MSC | No (%) of MSC with/without Ch/R | Melanoma Risk | ||
|---|---|---|---|---|---|---|---|
| Ch | R ± Ch | No Tx | |||||
| Herr et al. [19] | 36.784 | 7798/478 | 287 | 53 (18.4) | <5 | 234 (81.5) | ns |
| Morton et al. [28] | 15.915 | 4.680/490 | 85 | 26 (30.5) | <3 | 59 (69.5) | ns |
| Turk et al. [18] | 48.876 | 7827/0 | 474 | 70 (14.8%) | 0 | 404 (85.2) | O/E 2.28 (95% CI, 1.77–2.88) |
| Lam et al. [57] | 13.950 | 5.051/1.025 | 91 | 47 § (51.7) | <10 | 52 (57.1) | # HR 1.90, 95 CI 1.08–3.37) |
| Chatzikonstantinou et al. [45] | φ 19.705 | 7.128 */9 | 130 | nos | nos | nos | τ OR 2.08 (95% CI, 1.51–2.87) |
| Authors | Year | Country/Registry | No Patients | O | M Risk (95% CI) | FU Time |
|---|---|---|---|---|---|---|
| Adami et al. [66] | 1995 | Denmark + Sweden/Danish Cancer Registry | 34,641 | 52 | RR: 2.4 (1.8–3.2) | 114,423 PY |
| Baras et al. [67] | 2017 | Germany/ZfKD | 110,164 | 328 | SIR: 1.92 (1.71–2.14) | 462,890 PY |
| Bermejo et al. [68] | 2014 | Finland, Norway, Sweden | 60,901 | 217 | RR: 2.27 (1.98–2.59) | 324,798 PY |
| Brennan et al. [69] | 2020 | Australia/NSW Central Cancer Registry | 12,452 | 93 | SIR: 2.38 (1.92–2.91) | 54,308 PY |
| Chattopadhyay et al. [70] | 2018 | Sweden/Swedish FCD | 19,833 | 83 | RR: 1.98 (1.60–2.44) | 4 y median FU |
| Dong and Hemminki [71] | 2001 | Swedish Family Cancer Database | 18,960 | 33 | 1.14 (0.78–1.60) n.s | 94,088 PYAR |
| Goggins et al. [22] | 2021 | USA/SEER | 62,597 | 139 | SIR: 1.75 (1.48–2.07) | m: 123,288 f: 121,288 PY |
| Hall et al. [72] | 1995 | Sweden/SCR | 6176 | 10 | SIR: 1.7 (0.8–3.1) | ns |
| Parsons et al. [73] | 2023 | USA/SEER | 141,451 | 715 | SIR: 1.29 (1.20–1.39) | 923,475 PY |
| Royle et al. [74] | 2011 | NCSCH | 40.529 | 313 | SIR: 5.24 (4.67–5.85) | 198,717 PYAR |
| Travis et al. [65] | 1993 | ICR + OCR + SCR + affiliated tumor registry of the NCI | 6171 | 20 | O/E: 2.38 (1.45–3.67) | 7.4 y mean FU |
| Authors | Year | Registry/Hospital | No Patients | M Risk (95% CI) | FU Time |
|---|---|---|---|---|---|
| Abrahamsen et al. [90] | 2002 | Norwegian Cancer Registry | 1.024 | SIR: 2.8 (1.2–5.5) # | 14 y median FU |
| Andrea et al. [91] | 2002 | Four Harvard affiliated hospitals + | 1319 | RR 3.3 (1.3–6.7) | 15.910 PYFU |
| Daniëls et al. [92] | 2013 | LUMC cancer registry system + PALGA + NCR | 889 | SIR: 2.3 (0.9–5.6) | ns |
| Dietrich et al. [93] | 1994 | Institut Gustave Roussy | 892 | O/E: 11.76 (1.42–43) | 5.263 PYAR |
| Dong and Hemminki [71] | 2001 | Swedish Family Cancer Database | 5353 | 1.83 (1.04–2.98) | 46.206 PYAR |
| Henry-Amar et al. [94] | 1992 | IDHD | 12.411 | O/E m: 1.9 f: 1.2 n.s. | 82.850 PYFU |
| Herr et al. [19] | 2018 | 17 SEER Program registries | 17.556 | SIR: 1.75 (1.33–2.26) | 3.3–6 y mean FU |
| Munker et al. [95] | 1999 | Munich tumor registry | 1120 | SIR: 2.5 (0.4–8.2) | 9.1 y mean FU |
| Royle et al. [74] | 2011 | NCSCH | 8.396 | SIR: 8.00 (5.92–10.6) | 68.369 PYAR |
| Sud et al. [96] | 2017 | Swedish Family-Cancer Project Database | 9.522 | SIR: 2.08 (1.54–2.82) | 12.6 y median FU |
| Swerdlow et al. [97] | 2000 | BNLI database + Royal Marsden Hospital + St Bartholomew’s Hospital | 5.519 | SIR: 2.3 (0.9–4.6) n.s. SIR: 4.2 (1.3–9.9) # | 46.990 PYFU |
| Authors | Year | Country/Registry | First Neoplasia | No Patients Followed | M Risk (95% CI) | Follow-Up |
|---|---|---|---|---|---|---|
| Chattopadhyay et al. [131] | 2018 | Sweden/ SFCD | PV ET MF MPN-nos | 6.636 4081 1454 1634 | RR 2.27 (1.65–3.14) RR 2.26 (1.50–3.40) RR 1.66 (0.62–4.42) n.s. RR 1.60 (0.72–3.56) n.s. | 6 y median FU 4 y median FU 2 y median FU 3 y median FU |
| Fallah et al. [132] | 2011 | Sweden/ SCR | PV | 3530 | SIR 1.88 (1.13–2.93) | Not specified |
| Federiksen et al. [129] | 2011 | Denmark/DNRP | PV ET | 4.625 1578 | 1.7 (1.0–2.7) NR | 5 y median FU 4 y median FU |
| Joshi et al. [133] | 2022 | USA/ SEER 18 | PMF | 5.273 | SIR 1.76 (1.01–2.86) | 10 y |
| Landtblom et al. [130] | 2018 | Sweden/ SCR | PV, ET, PMF, MPN-U | c: 9.379 mc: 35.682 | HR 1.9 (1.4–2.7) | 7.7 y median FU |
| Susini et al. [134] | 2012 | Italy/UNIFI and RTT | PV, ET, MF | 733 | SIR 3.69 (1.39–9.64) | 6.45 y mean FU |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halmágyi, S.-R.; Ungureanu, L.; Trufin, I.-I.; Apostu, A.P.; Șenilă, S.C. Melanoma as Subsequent Primary Malignancy in Hematologic Cancer Survivors—A Literature Review. J. Clin. Med. 2024, 13, 4501. https://doi.org/10.3390/jcm13154501
Halmágyi S-R, Ungureanu L, Trufin I-I, Apostu AP, Șenilă SC. Melanoma as Subsequent Primary Malignancy in Hematologic Cancer Survivors—A Literature Review. Journal of Clinical Medicine. 2024; 13(15):4501. https://doi.org/10.3390/jcm13154501
Chicago/Turabian StyleHalmágyi, Salomea-Ruth, Loredana Ungureanu, Ioana-Irina Trufin, Adina Patricia Apostu, and Simona Corina Șenilă. 2024. "Melanoma as Subsequent Primary Malignancy in Hematologic Cancer Survivors—A Literature Review" Journal of Clinical Medicine 13, no. 15: 4501. https://doi.org/10.3390/jcm13154501