Evaluating the Efficacy of Gross-Motor-Based Interventions for Children with Developmental Coordination Disorder: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
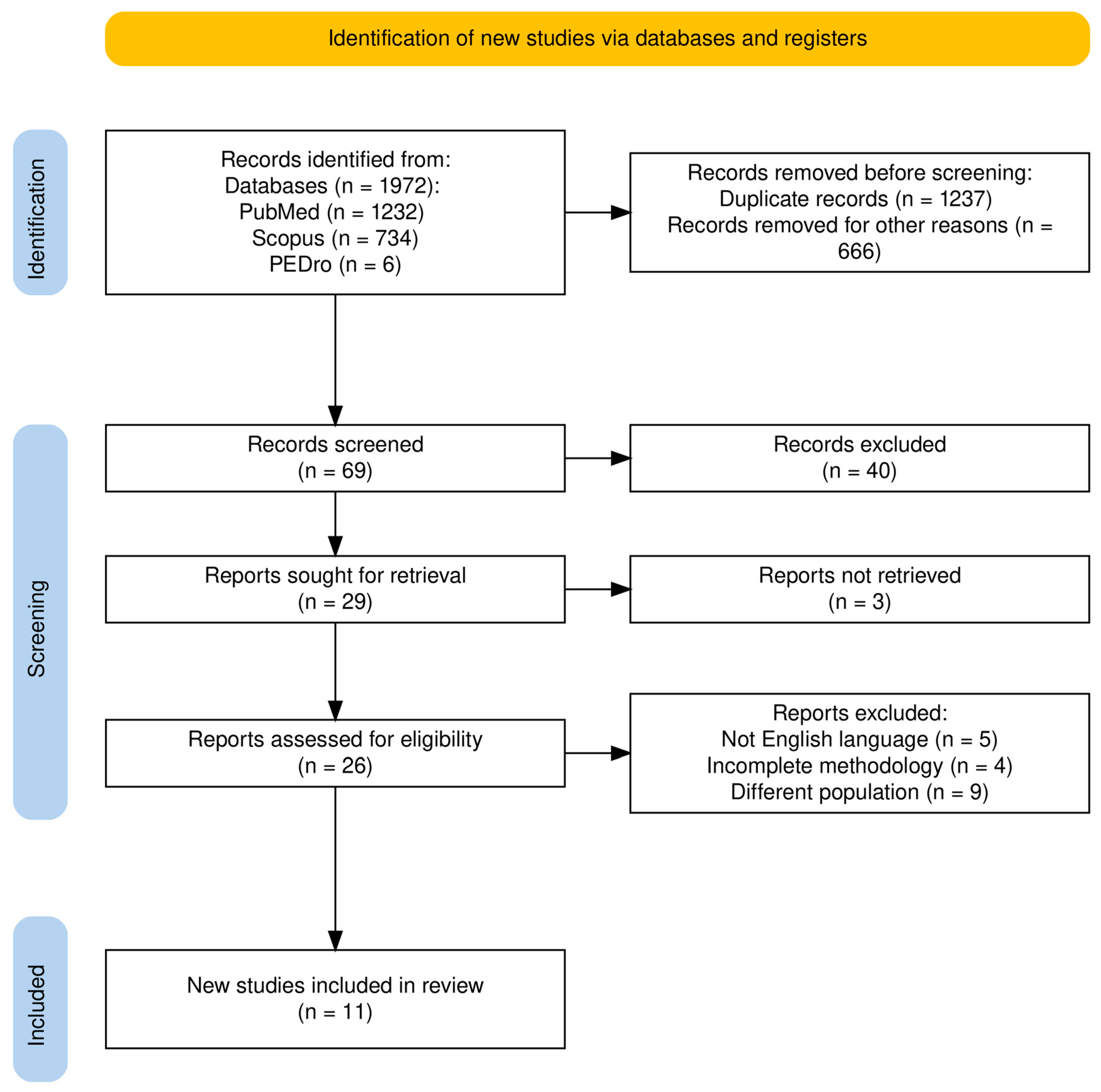
2.1. Search Strategy
2.2. Selection Criteria
2.3. Reviewing Procedure and Data Extraction
2.4. Methodological Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Studies’ Charactristics
3.2. Quality Studies
3.3. Summary of Included Studies
3.4. Task-Oriented Activities and Motor Performance
3.5. Fundamental Skills and Physical Exercise
3.6. Active Video Game and Motor Skills
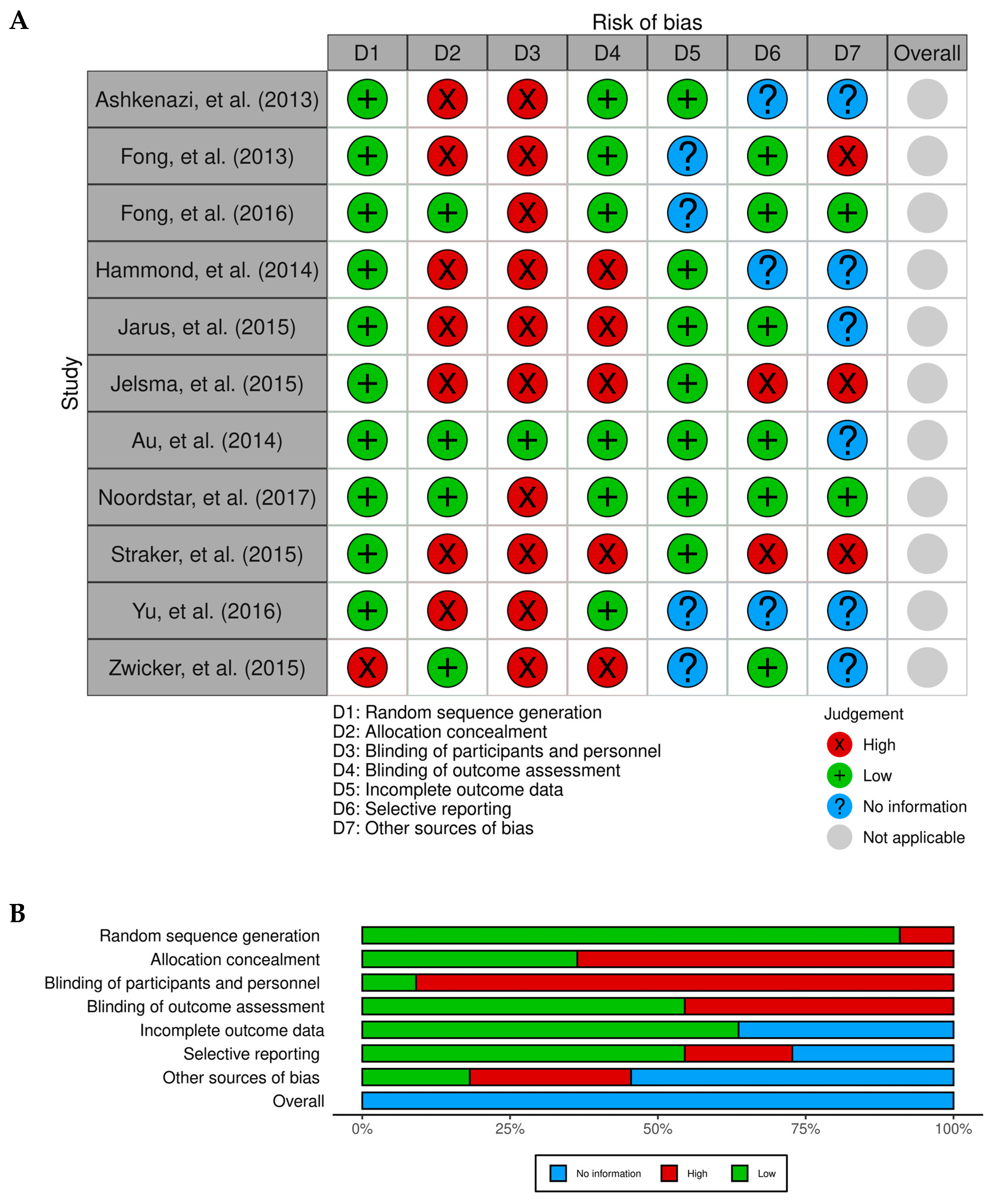
3.7. Analysis of Risk of Bias
4. Discussion
4.1. DCD and Motor Activities
4.2. Goal-Oriented Activities in DCD
4.3. Neuromotor Task Training (NTT)
4.4. Active Video Game Intervention
4.5. Limitations and Future Recommendations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kirby, A.; Sugden, D.A. Children with Developmental Coordination Disorders. J. R. Soc. Med. 2007, 100, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Smits-Engelsman, B.; Schoemaker, M.; Delabastita, T.; Hoskens, J.; Geuze, R. Diagnostic Criteria for DCD: Past and Future. Hum. Mov. Sci. 2015, 42, 293–306. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association, D.; American Psychiatric Association, D.S. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013; Volume 5. [Google Scholar]
- Subara-Zukic, E.; Cole, M.H.; McGuckian, T.B.; Steenbergen, B.; Green, D.; Smits-Engelsman, B.C.M.; Lust, J.M.; Abdollahipour, R.; Domellöf, E.; Deconinck, F.J.A. Behavioral and Neuroimaging Research on Developmental Coordination Disorder (DCD): A Combined Systematic Review and Meta-Analysis of Recent Findings. Front. Psychol. 2022, 13, 809455. [Google Scholar] [CrossRef] [PubMed]
- Girish, S.; Raja, K.; Kamath, A. Prevalence of Developmental Coordination Disorder among Mainstream School Children in India. J. Pediatr. Rehabil. Med. 2016, 9, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, G.D.; Aertssen, W.F.M.; Rameckers, E.A.A.; Jelsma, J.; Smits-Engelsman, B.C.M. Physical Fitness in Children with Developmental Coordination Disorder: Measurement Matters. Res. Dev. Disabil. 2014, 35, 1087–1097. [Google Scholar] [CrossRef] [PubMed]
- Farmer, M.; Echenne, B.; Drouin, R. Insights in Developmental Coordination Disorder. Curr. Pediatr. Rev. 2017, 13, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Lino, F.; Chieffo, D.P.R. Developmental Coordination Disorder and Most Prevalent Comorbidities: A Narrative Review. Children 2022, 9, 1095. [Google Scholar] [CrossRef]
- Karabak, M.; Akıncı, M.A.; Yıldırım Demirdöğen, E.; Bozkurt, A. Prevalence and Associated Factors of Developmental Coordination Disorder in Primary School Children. Eur. Child. Adolesc. Psychiatry 2024, 1–12. [Google Scholar] [CrossRef]
- Edwards, J.; Berube, M.; Erlandson, K.; Haug, S.; Johnstone, H.; Meagher, M.; Sarkodee-Adoo, S.; Zwicker, J.G. Developmental Coordination Disorder in School-Aged Children Born Very Preterm and/or at Very Low Birth Weight: A Systematic Review. J. Dev. Behav. Pediatr. 2011, 32, 678–687. [Google Scholar] [CrossRef]
- Zoia, S.; Biancotto, M.; Caravale, B.; Valletti, A.; Montelisciani, L.; Croci, I.; Voller, F.; Rusconi, F.; Carrozzi, M.; Chiandotto, V. Early Factors Associated with Risk of Developmental Coordination Disorder in Very Preterm Children: A Prospective Area-based Cohort Study in Italy. Paediatr. Perinat. Epidemiol. 2022, 36, 683–695. [Google Scholar] [CrossRef]
- Panceri, C.; Sbruzzi, G.; Zanella, L.W.; Wiltgen, A.; Procianoy, R.S.; Silveira, R.C.; Valentini, N.C. Developmental Coordination Disorder in Preterm Children: A Systematic Review and Meta-analysis. Eur. J. Neurosci. 2024, 60, 4128–4147. [Google Scholar] [CrossRef] [PubMed]
- Faebo Larsen, R.; Hvas Mortensen, L.; Martinussen, T.; Nybo Andersen, A. Determinants of Developmental Coordination Disorder in 7-year-old Children: A Study of Children in the D Anish N Ational B Irth C Ohort. Dev. Med. Child. Neurol. 2013, 55, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Lingam, R.; Golding, J.; Jongmans, M.J.; Hunt, L.P.; Ellis, M.; Emond, A. The Association between Developmental Coordination Disorder and Other Developmental Traits. Pediatrics 2010, 126, e1109–e1118. [Google Scholar] [CrossRef] [PubMed]
- Draghi, T.T.G.; Cavalcante, J.L.; Rohr, L.A.; Jelsma, L.D.; Tudella, E. Symptoms of Anxiety and Depression in Children with Developmental Coordination Disorder: A Systematic Review. J. Pediatr. 2020, 96, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Valentini, N.C.; de Souza, P.S.; de Souza, M.S.; Nobre, G.C. Individual and Environmental Parameters in Children with and without Developmental Coordination Disorder: Associations with Physical Activity and Body Mass Index. Front. Pediatr. 2023, 11, 1202488. [Google Scholar] [CrossRef]
- Gambra, L.; Cortese, S.; Lizoain, P.; Romero, D.R.; Paiva, U.; Gándara, C.; Arrondo, G.; Magallón, S. Excessive Body Weight in Developmental Coordination Disorder: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2024, 164, 105806. [Google Scholar] [CrossRef]
- Cavalcante Neto, J.L.; Draghi, T.T.G.; dos Santos, I.W.P.; Brito, R.D.S.; Silva, L.S.D.O.; Lima, U.D.S. Physical Fitness in Children With Developmental Coordination Disorder: A Systematic Review. Phys. Occup. Ther. Pediatr. 2024, 44, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Venezia, I.; De Biase, M.; Ascione, F.; Lala, M.R.; Arcangeli, V.; Mercuri, E.; Brogna, C. Developmental Coordination Disorder and Joint Hypermobility in Childhood: A Narrative Review. Children 2022, 9, 1011. [Google Scholar] [CrossRef]
- Reynolds, J.E.; Thornton, A.L.; Elliott, C.; Williams, J.; Lay, B.S.; Licari, M.K. A Systematic Review of Mirror Neuron System Function in Developmental Coordination Disorder: Imitation, Motor Imagery, and Neuroimaging Evidence. Res. Dev. Disabil. 2015, 47, 234–283. [Google Scholar] [CrossRef]
- Wilson, P.H.; Smits-Engelsman, B.; Caeyenberghs, K.; Steenbergen, B.; Sugden, D.; Clark, J.; Mumford, N.; Blank, R. Cognitive and Neuroimaging Findings in Developmental Coordination Disorder: New Insights from a Systematic Review of Recent Research. Dev. Med. Child. Neurol. 2017, 59, 1117–1129. [Google Scholar] [CrossRef]
- Balayi, E.; Sedaghati, P.; Ahmadabadi, S. Effects of Neuromuscular Training on Postural Control of Children with Intellectual Disability and Developmental Coordination Disorders: Neuromuscular Training and Postural Control. BMC Musculoskelet. Disord. 2022, 23, 631. [Google Scholar] [CrossRef] [PubMed]
- Schott, N.; El-Rajab, I.; Klotzbier, T. Cognitive-Motor Interference during Fine and Gross Motor Tasks in Children with Developmental Coordination Disorder (DCD). Res. Dev. Disabil. 2016, 57, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Shahbaz, R.; Saemi, E.; Doustan, M.; Hogg, J.A.; Diekfuss, J.A. The Effect of a Visual Illusion and Self-Controlled Practice on Motor Learning in Children at Risk for Developmental Coordination Disorder. Sci. Rep. 2024, 14, 12414. [Google Scholar] [CrossRef]
- Parr, J.V.V.; Foster, R.J.; Wood, G.; Thomas, N.M.; Hollands, M.A. Children with Developmental Coordination Disorder Show Altered Visuomotor Control during Stair Negotiation Associated with Heightened State Anxiety. Front. Hum. Neurosci. 2020, 14, 589502. [Google Scholar] [CrossRef]
- Speedtsberg, M.B.; Christensen, S.B.; Stenum, J.; Kallemose, T.; Bencke, J.; Curtis, D.J.; Jensen, B.R. Local Dynamic Stability during Treadmill Walking Can Detect Children with Developmental Coordination Disorder. Gait Posture 2018, 59, 99–103. [Google Scholar] [CrossRef]
- Biotteau, M.; Danna, J.; Baudou, É.; Puyjarinet, F.; Velay, J.-L.; Albaret, J.-M.; Chaix, Y. Developmental Coordination Disorder and Dysgraphia: Signs and Symptoms, Diagnosis, and Rehabilitation. Neuropsychiatr. Dis. Treat. 2019, 2019, 1873–1885. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Ayyub, M.; Sun, H.; Wen, X.; Xiang, P.; Gao, Z. Effects of Physical Activity on Motor Skills and Cognitive Development in Early Childhood: A Systematic Review. Biomed. Res. Int. 2017, 2017, 2760716. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sherrington, C.; Herbert, R.D.; Maher, C.G.; Moseley, A.M. PEDro. A Database of Randomized Trials and Systematic Reviews in Physiotherapy. Man. Ther. 2000, 5, 223–226. [Google Scholar] [CrossRef]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for Physiotherapy Practice: A Survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the Thematic Synthesis of Qualitative Research in Systematic Reviews. BMC Med. Res. Methodol. 2008, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 0203771583. [Google Scholar]
- Ashkenazi, T.; Weiss, P.L.; Orian, D.; Laufer, Y. Low-Cost Virtual Reality Intervention Program for Children with Developmental Coordination Disorder: A Pilot Feasibility Study. Pediatr. Phys. Ther. 2013, 25, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Au, M.K.; Chan, W.M.; Lee, L.; Chen, T.M.K.; Chau, R.M.W.; Pang, M.Y.C. Core Stability Exercise Is as Effective as Task-Oriented Motor Training in Improving Motor Proficiency in Children with Developmental Coordination Disorder: A Randomized Controlled Pilot Study. Clin. Rehabil. 2014, 28, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.G.; Rehal, H.; Sodhi, S.; Karkling, M.; Paul, A.; Hilliard, M.; Jarus, T. Effectiveness of a Summer Camp Intervention for Children with Developmental Coordination Disorder. Phys. Occup. Ther. Pediatr. 2015, 35, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.S.M.; Guo, X.; Liu, K.P.Y.; Ki, W.Y.; Louie, L.H.T.; Chung, R.C.K.; Macfarlane, D.J. Task-Specific Balance Training Improves the Sensory Organisation of Balance Control in Children with Developmental Coordination Disorder: A Randomised Controlled Trial. Sci. Rep. 2016, 6, 20945. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.S.M.; Chung, J.W.Y.; Chow, L.P.Y.; Ma, A.W.W.; Tsang, W.W.N. Differential Effect of Taekwondo Training on Knee Muscle Strength and Reactive and Static Balance Control in Children with Developmental Coordination Disorder: A Randomized Controlled Trial. Res. Dev. Disabil. 2013, 34, 1446–1455. [Google Scholar] [CrossRef] [PubMed]
- Jarus, T.; Ghanouni, P.; Abel, R.L.; Fomenoff, S.L.; Lundberg, J.; Davidson, S.; Caswell, S.; Bickerton, L.; Zwicker, J.G. Effect of Internal versus External Focus of Attention on Implicit Motor Learning in Children with Developmental Coordination Disorder. Res. Dev. Disabil. 2015, 37, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Sit, C.H.P.; Burnett, A.; Capio, C.M.; Ha, A.S.C.; Huang, W.Y.J. Effects of Fundamental Movement Skills Training on Children with Developmental Coordination Disorder. Adapt. Phys. Act. Q. 2016, 33, 134–155. [Google Scholar] [CrossRef] [PubMed]
- Straker, L.; Howie, E.; Smith, A.; Jensen, L.; Piek, J.; Campbell, A. A Crossover Randomised and Controlled Trial of the Impact of Active Video Games on Motor Coordination and Perceptions of Physical Ability in Children at Risk of Developmental Coordination Disorder. Hum. Mov. Sci. 2015, 42, 146–160. [Google Scholar] [CrossRef]
- Noordstar, J.J.; van der Net, J.; Voerman, L.; Helders, P.J.M.; Jongmans, M.J. The Effect of an Integrated Perceived Competence and Motor Intervention in Children with Developmental Coordination Disorder. Res. Dev. Disabil. 2017, 60, 162–175. [Google Scholar] [CrossRef]
- Hammond, J.; Jones, V.; Hill, E.L.; Green, D.; Male, I. An Investigation of the Impact of Regular Use of the Wii Fit It to Improve Motor and Psychosocial Outcomes in Children with Movement Difficulties: A Pilot Study. Child. Care Health Dev. 2014, 40, 165–175. [Google Scholar] [CrossRef]
- Jelsma, D.; Ferguson, G.D.; Smits-Engelsman, B.C.M.; Geuze, R.H. Short-Term Motor Learning of Dynamic Balance Control in Children with Probable Developmental Coordination Disorder. Res. Dev. Disabil. 2015, 38, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Blank, R.; Smits-Engelsman, B.; Polatajko, H.; Wilson, P. European Academy for Childhood Disability (EACD): Recommendations on the Definition, Diagnosis and Intervention of Developmental Coordination Disorder (Long Version). Dev. Med. Child. Neurol. 2012, 54, 54. [Google Scholar] [CrossRef] [PubMed]
- Cantell, M.H.; Smyth, M.M.; Ahonen, T.P. Two Distinct Pathways for Developmental Coordination Disorder: Persistence and Resolution. Hum. Mov. Sci. 2003, 22, 413–431. [Google Scholar] [CrossRef]
- Kagerer, F.A.; Contreras-Vidal, J.L.; Bo, J.; Clark, J.E. Abrupt, but Not Gradual Visuomotor Distortion Facilitates Adaptation in Children with Developmental Coordination Disorder. Hum. Mov. Sci. 2006, 25, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Wolpert, D.M. Computational Approaches to Motor Control. Trends Cogn. Sci. 1997, 1, 209–216. [Google Scholar] [CrossRef]
- Debrabant, J.; Gheysen, F.; Caeyenberghs, K.; Van Waelvelde, H.; Vingerhoets, G. Neural Underpinnings of Impaired Predictive Motor Timing in Children with Developmental Coordination Disorder. Res. Dev. Disabil. 2013, 34, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.A.; Keating, J.G.; Goodkin, H.P.; Bastian, A.J.; Thach, W.T. Throwing While Looking through Prisms: II. Specificity and Storage of Multiple Gaze—Throw Calibrations. Brain 1996, 119, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- van Swieten, L.M.; van Bergen, E.; Williams, J.H.G.; Wilson, A.D.; Plumb, M.S.; Kent, S.W.; Mon-Williams, M.A. A Test of Motor (Not Executive) Planning in Developmental Coordination Disorder and Autism. J. Exp. Psychol. Hum. Percept. Perform. 2010, 36, 493. [Google Scholar] [CrossRef]
- Ferguson, G.D.; Jelsma, D.; Jelsma, J.; Smits-Engelsman, B.C.M. The Efficacy of Two Task-Orientated Interventions for Children with Developmental Coordination Disorder: Neuromotor Task Training and Nintendo Wii Fit Training. Res. Dev. Disabil. 2013, 34, 2449–2461. [Google Scholar] [CrossRef]
- Lucas, B.R.; Elliott, E.J.; Coggan, S.; Pinto, R.Z.; Jirikowic, T.; McCoy, S.W.; Latimer, J. Interventions to Improve Gross Motor Performance in Children with Neurodevelopmental Disorders: A Meta-Analysis. BMC Pediatr. 2016, 16, 193. [Google Scholar] [CrossRef] [PubMed]
- Crosson, B.; Hampstead, B.M.; Krishnamurthy, L.C.; Krishnamurthy, V.; McGregor, K.M.; Nocera, J.R.; Roberts, S.; Rodriguez, A.D.; Tran, S.M. Advances in Neurocognitive Rehabilitation Research from 1992 to 2017: The Ascension of Neural Plasticity. Neuropsychology 2017, 31, 900. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Criteria | Inclusion | Exclusion |
|---|---|---|
| Publication type | Peer-reviewed articles | Non-peer-reviewed articles |
| Publication year | 2010 to 2022 | Earlier than 2010 |
| Study design | Randomized controlled trials; single-case experimental design studies | Opinion pieces, case reports, and editorials |
| Language | English | Other languages |
| Accessibility | Full-text articles | Studies with abstract only |
| Relevance | Studies discussing gross-motor-based interventions, children, and DCD | Other studies |
| Author | Country | Study Design | Total Participants | Age (Years) | Time of Assessment |
|---|---|---|---|---|---|
| Ashkenazi, et al. (2013) [34] | Israel | Pilot feasibility study | 9 Patients | 5.6 ± 0.5 | Baseline and post-treatment |
| Au, et al. (2014) [35] | China | Randomized controlled pilot study | 22 Patients | IG: 7.9 ± 1.2 CG: 7.6 ± 1.08 | Baseline and post-treatment |
| Zwicker, et al. (2015) [36] | Switzerland | Mixed method study | 11 Patients | 9.7 ± 1.8 | Baseline and post-treatment |
| Fong, et al. (2016) [37] | Hong Kong | Randomized control trial | 161 Patients | IG: 7.9 ± 1.4 CG: 7.5 ± 1.6 | Pre, post, and 3 months after treatment |
| Fong, et al. (2013) [38] | Hong Kong | Randomized, single-blinded, stratified, controlled trial | 44 Patients | DCD TKD: 7.7 ± 1.3 DCD CG: 7.4 ± 1.2 TD: 7.2 ± 1.0 | Baseline and post-treatment |
| Jarus, et al. (2015) [39] | Canada | Randomized controlled trial | 25 Patients | 10 ± 2.1 | Baseline and post-treatment |
| Yu, et al. (2016) [40] | China | Quasi-randomized, controlled, and single-blinded trial | 84 Patients | IG: 8.2 ± 0.7 CG: 8.9 ± 0.9 | Baseline and post-treatment |
| Straker, et al. (2015) [41] | Australia | Crossover randomized controlled trial | 21 Patients | 11 ± 1.0 | Baseline, 2nd week (first task), and after 2 weeks of 2nd task |
| Noordstar, et al. (2017) [42] | Netherlands | Randomized controlled trial | 31 Patients | IG: 8.1 ± 0.9 CG: 8.09 ± 1.1 | Pre- and post-treatment |
| Hammond, et al. (2014) [43] | United Kingdom | Randomized crossover-controlled trial | 18 Patients | IG: 8.5 ± 1.1 CG: 9.5 ± 1.4 | Pre- and post-treatment |
| Jelsma, et al. (2015) [44] | Netherlands | Single-blind, parallel-arm, randomized clinical trial | 66 Patients | DCD-NL: 8 ± 1.0 DCD-SA: 7 ± 1.0 TD-NL: 8 ± 1.0 | Baseline and post-treatment |
| Criterion * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
| Ashkenazi, et al. (2013) [34] | 1 | - | - | 1 | - | 1 | - | 1 | 1 | - | 1 | 6 |
| Au, et al. (2014) [35] | 1 | 1 | - | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Zwicker, et al. (2015) [36] | 1 | - | 1 | - | - | 1 | - | 1 | - | - | 1 | 5 |
| Fong, et al. (2016) [37] | 1 | 1 | 1 | 1 | - | - | 1 | 1 | 1 | 1 | 1 | 9 |
| Fong, et al. (2013) [38] | 1 | 1 | - | 1 | - | - | 1 | 1 | 1 | 1 | 1 | 8 |
| Jarus, et al. (2015) [39] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 7 |
| Yu, et al. (2016) [40] | 1 | 1 | 1 | 1 | - | - | 1 | 1 | 1 | 1 | 1 | 8 |
| Straker, et al. (2015) [41] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Noordstar, et al. (2017) [42] | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Hammond, et al. (2014) [43] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Jelsma, et al. (2015) [44] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 7 |
| Author | Objective | Intervention | Outcome Measures | Results | Conclusion |
|---|---|---|---|---|---|
| Ashkenazi, et al. (2013) [34] | To investigate the viability of treating young children with DCD using a low-cost, commercial VR game and to ascertain the impact of this intervention on motor function. | Ten game-based intervention sessions were conducted with nine children (4–6 years old) who were sent to physical therapy for suspected DCD. The intervention was divided into VR-based intervention and goal-directed tasks. |
| Statistically significant changes were seen in the total standard score (p = 0.02) and the sub-score of balance (p = 0.01) of the MABC-2 and in the DCD-Q (p < 0.05). | A low-cost, off-the-shelf VR game system is an efficient, fun, and motivating intervention tool. It is an effective way to improve motor function in children with DCD. |
| Au, et al. (2014) [35] | To compare the effectiveness of a core stability program and a task-oriented motor training program in improving motor proficiency in children with DCD. | Core stability group: The children underwent Physioball treatment, focusing on co-contracting their back and abdominal muscles to maintain a neutral spine position. Task-oriented group: The emphasis was on teaching functional tasks, such as standing, walking, running, jumping, hopping, skipping, and galloping. |
| The core stability and task-oriented training groups substantially increased motor skills. | The viability of the training approaches employed is practical, and the results are highly encouraging in improving motor function in children with DCD. |
| Zwicker, et al. (2015) [36] | To evaluate the efficacy of the summer camp in achieving the functional motor goal chosen by the child and in boosting self-efficacy and participation. | During camp, children participated in a range of group activities, such as baking, dragon boat racing, trekking, crafts, rock climbing, and games to boost their self-esteem. |
| Statistical improvement in performance and happiness with child-selected goals, but no significant gains in self-efficacy and engagement. Parents and children reported camp as a source of courage, interaction, and knowledge. | Task-specific cognitive intervention improves self-reported measures of functional motor goals for children with DCD. |
| Fong, et al. (2016) [37] | To assess the effectiveness of an FMT program for correcting balance impairments in a cohort of DCD patients. | FMT Group: Underwent specialized balance training combined with electromyographic biofeedback (an extrinsic kind of feedback) Control group: No physical training. |
| The FMT group showed more significant improvements than the controls in somatosensory ratio at 3 and 6 months (all p < 0.001). | The suggested task-specific balance training slightly improved the somatosensory function and functional balance performance of children with DCD. |
| Fong, et al. (2013) [38] | To explore how children with DCD’s isokinetic knee muscle strength and reactive and static balance control are affected by short-term, rigorous TKD training. | Intervention group: TKD training sessions, TKD home exercises Control group: No training. |
| After TKD training, DCD-TKD children’s isokinetic knee muscular strength, specifically at 180 degree/s, was equal to that of the typical control group children (p > 0.0083). | Children with DCD who participated in a 3-month TKD program showed increased static and isokinetic knee muscle strength and one-leg balance while standing. |
| Jarus, et al. (2015) [39] | How does the focus of attention affect motor learning in children with DCD compared to typically developing children, as well as the trends of implicit motor learning in such children. | Intervention group: Concentrate on their hand, wrist, and arm movements while executing the tracking assignment Control group: Concentrate on the computer monitor and the joystick’s movements while tracking the target. |
| Children with DCD did not perform well on the motor test, indicating less implicit learning. | Children with DCD exhibit lower accuracy in learning motor activities than children who are developing usually and differ in the impact of attention focus on motor performance during the three periods of motor learning. |
| Yu, et al. (2016) [40] | Basic movement skills training on children with DCD compared to children with typical development in terms of FMS competency, self-perceived physical competence, physical activity, and sleep disturbance. | Intervention group: Group-based multi-skill FMS training Control group: Regular physical exercises. |
| In the post-test, with fewer sleep disturbances, the experimental group had significantly higher FMS and SPC scores than the control group. | For children with DCD, FMS training enhances FMS and SPC and minimizes sleep disturbance. |
| Straker, et al. (2015) [41] | To compare 16 weeks of active video game use to regular activity to examine motor coordination changes. Additionally, it explores the perceptions of physical performance in both settings by children and parents. | Intervention group: Active video game Control group: Traditional/sedentary games. |
| Children’s perceptions of whether the active video game had improved their motor abilities in comparison to no intervention period. | There is no improvement in motor skills after a 16-week home-based active video game intervention, although children’s physical abilities were significantly improved. |
| Noordstar, et al. (2017) [42] | To examine the effects of a motor intervention alone versus a combined perceived competence and motor intervention on children with DCD motor performance, self-perceptions, and physical activity. | Intervention group: Care-as-usual group with therapist progressive feedback Control group: Deficient motor activities were being practiced. |
| After 12 therapy sessions, children improved their motor skills and perceived athletic ability, self-esteem, and competence. | In children with DCD, perceived competence and motor intervention are just as successful as standard treatment. |
| Hammond, et al. (2014) [43] | To determine if providing DCD kids short, frequent movement lessons on a commercially available home video game console would help them with their social and motor skills. | Intervention group: Supervised play for 10 min thrice weekly for one month using Wii Fit during the lunch break Control group: Regular Jump Ahead program. |
| For many children, there were significant improvements in motor skills, the impression of motor abilities, and reported mental well-being. | Wii Fit is a popular intervention and a valid strategy to aid children’s motor and social development. |
| Jelsma, et al. (2015) [44] | Children with and without DCD from various cultural backgrounds were given the same dynamic balance task to learn about the differences in their learning methods. | Wii Fit protocol: Children using the balancing board can play the video game by adjusting their weight. |
| Children with p-DCD-NL and p-DCD-SA showed no significant difference in motor-learning rates, but those with the disorder learned more slowly. | p-DCD kids learn at a different pace and maintain performance levels over 6 weeks, with experience and cultural background having minimal impact on learning rate. |
| Author (Year)— Outcome Measure | Pre-Test Mean ± SD | Post-Test Mean ± SD | Effect Size (Cohen’s d) | Lower CI for ES | Upper CI for ES |
|---|---|---|---|---|---|
| Ashkenazi, et al. (2013) [34]—MABC-2 | 4.7 ± 1.4 | 7.4 ± 3.5 | 1.02 | 0.15 | 1.78 |
| Au, et al. (2014) [35]— BOT-SF | 39.7 ± 3.9 | 44.8 ± 5.5 | 1.07 | 0.28 | 1.77 |
| Fong, et al. (2016) [37]—MABC | 3.0 ± 2.1 | 1.9 ± 1.5 | 0.60 | 0.25 | 0.94 |
| Yu, et al. (2016) [40]— TGMD | 16.8 ± 5.1 | 19.0 ± 7.9 | 0.33 | −0.19 | 0.80 |
| Straker, et al. (2015) [41]— MABC-2 | 8.1 ± 8.2 | 17.7 ± 14.0 | 0.80 | 0.26 | 31 |
| Noordstar, et al. (2017) [42]—MABC-2 | 3.8 ± 2.4 | 5.6 ± 4.1 | 0.54 | 0.00 | 1.05 |
| Hammond, et al. (2014) [43]—BOT-SF | 4.0 ± 11.9 | 11.7 ± 32.5 | 0.32 | −0.43 | 1.04 |
| Jelsma, et al. (2015) [44]— MABC and BOT | 2.6 ± 1.6 | 4.2 ± 3.0 | 0.67 | 0.20 | 1.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghadier, M.; Alhusayni, A.I. Evaluating the Efficacy of Gross-Motor-Based Interventions for Children with Developmental Coordination Disorder: A Systematic Review. J. Clin. Med. 2024, 13, 4609. https://doi.org/10.3390/jcm13164609
Alghadier M, Alhusayni AI. Evaluating the Efficacy of Gross-Motor-Based Interventions for Children with Developmental Coordination Disorder: A Systematic Review. Journal of Clinical Medicine. 2024; 13(16):4609. https://doi.org/10.3390/jcm13164609
Chicago/Turabian StyleAlghadier, Mshari, and Abdullah I. Alhusayni. 2024. "Evaluating the Efficacy of Gross-Motor-Based Interventions for Children with Developmental Coordination Disorder: A Systematic Review" Journal of Clinical Medicine 13, no. 16: 4609. https://doi.org/10.3390/jcm13164609
APA StyleAlghadier, M., & Alhusayni, A. I. (2024). Evaluating the Efficacy of Gross-Motor-Based Interventions for Children with Developmental Coordination Disorder: A Systematic Review. Journal of Clinical Medicine, 13(16), 4609. https://doi.org/10.3390/jcm13164609