
The Usefulness of the CHA2DS2-VASc Score to Predict Outcomes in Patients with Infective Endocarditis
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.1.1. The “Endocarditis Team”
2.1.2. The CHA2DS2-VASC Score
2.2. Clinical Data and Study Endpoint
2.3. Statistical Analysis
3. Results
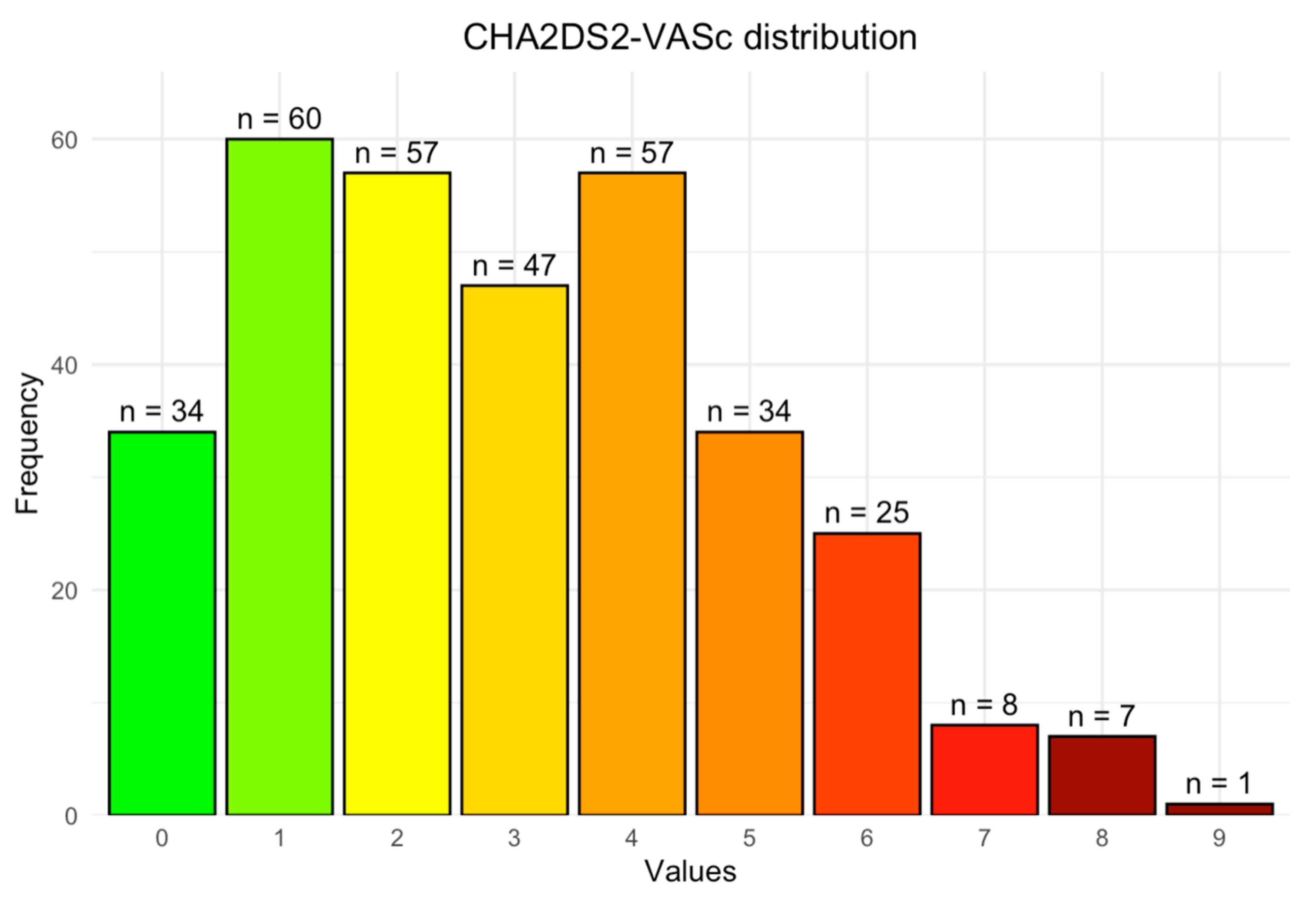
3.1. CHA2DS2-VASC Score
3.2. Multivariate Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pant, S.; Patel, N.J.; Deshmukh, A.; Golwala, H.; Patel, N.; Badheka, A.; Hirsch, G.A.; Mehta, J.L. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J. Am. Coll. Cardiol. 2015, 65, 2070–2076. [Google Scholar] [CrossRef] [PubMed]
- El Kadi, S.; van den Buijs, D.M.F.; Meijers, T.; Gilbers, M.D.; Bekkers, S.C.A.M.; van Melle, J.P.; Riezebos, R.K.; Blok, W.L.; Tanis, W.; Wahadat, A.R.; et al. Infective endocarditis in the Netherlands: Current epidemiological profile and mortality. Neth. Heart J. 2020, 28, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Arockiam, A.D.; Jamil, Y.; El Dahdah, J.; Honnekeri, B.; Chedid El Helou, M.; Kassab, J.; Wang, T.K.M. Contemporary risk models for infective endocarditis surgery: A narrative review. Ther. Adv. Cardiovasc. Dis. 2023, 17, 17539447231193292. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.F.; Liu, C.J.; Wang, K.L.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Chen, T.J.; Lip, G.Y.; et al. Using the CHA2DS2-VASc score for refining stroke risk stratification in “low-risk” Asian patients with atrial fibrillation. J. Am. Coll. Cardiol. 2014, 64, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Botto, G.L.; Padeletti, L.; Santini, M.; Capucci, A.; Gulizia, M.; Ricci, R.; Biffi, M.; De Santo, T.; Corbucci, G.; et al. Improving stroke risk stratification using the CHADS2 and CHA2DS2-VASc risk scores in patients with paroxysmal atrial fibrillation by continuous arrhythmia burden monitoring. Stroke 2011, 42, 1768–1770. [Google Scholar] [CrossRef] [PubMed]
- Orvin, K.; Levi, A.; Landes, U.; Bental, T.; Sagie, A.; Shapira, Y.; Vaknin-Assa, H.; Assali, A.; Kornowski, R. Usefulness of the CHA2DS2-VASc Score to Predict Outcome in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2018, 121, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; De Allie, G.; Eyituoyo, H.O.; Abe, T.; Tobun, T.; Asotibe, J.C.; Hayes, D.; Mather, P. CHA2DS2-VASc Is Associated With In-Hospital Mortality in Patients With Infective Endocarditis: A Cross-Sectional Cohort Study. Cureus 2020, 12, e11620. [Google Scholar] [CrossRef] [PubMed]
- Marsan, N.A.; de Waha, S.; Bonaros, N.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; Foldager, D.; Fosbøl, E.L.; Kovac, J.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Orvin, K.; Bental, T.; Assali, A.; Lev, E.I.; Vaknin-Assa, H.; Kornowski, R. Usefulness of the CHA2DS2-VASC Score to Predict Adverse Outcomes in Patients Having Percutaneous Coronary Intervention. Am. J. Cardiol. 2016, 117, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Thuny, F.; Giorgi, R.; Habachi, R.; Ansaldi, S.; Le Dolley, Y.; Casalta, J.P.; Avierinos, J.F.; Riberi, A.; Renard, S.; Collart, F.; et al. Excess mortality and morbidity in patients surviving infective endocarditis. Am. Heart J. 2012, 164, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.J.; Chu, H.; Chao, P.W.; Lee, Y.J.; Kuo, S.C.; Li, S.Y.; Tarng, D.C.; Yang, C.Y.; Yang, W.C.; Ou, S.M.; et al. Long-term clinical outcome of major adverse cardiac events in survivors of infective endocarditis: A nationwide population-based study. Circulation 2014, 130, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, V.; Salmasi, M.Y.; Sabetai, M.; Primus, C.; Sandoe, J.; Lewis, M.; Woldman, S.; Athanasiou, T. Infective endocarditis: Do we have an effective risk score model? A systematic review. Front. Cardiovasc. Med. 2023, 10, 1093363. [Google Scholar] [CrossRef] [PubMed]
- Park, L.P.; Chu, V.H.; Peterson, G.; Skoutelis, A.; Lejko-Zupa, T.; Bouza, E.; Tattevin, P.; Habib, G.; Tan, R.; Gonzalez, J.; et al. Validated Risk Score for Predicting 6-Month Mortality in Infective Endocarditis. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2016, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Pizzino, F.; Paradossi, U.; Trimarchi, G.; Benedetti, G.; Marchi, F.; Chiappino, S.; Conti, M.; Di Bella, G.; Murzi, M.; Di Sibio, S.; et al. Clinical Features and Patient Outcomes in Infective Endocarditis with Surgical Indication: A Single-Centre Experience. J. Cardiovasc. Dev. Dis. 2024, 11, 138. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Wang, X.; Su, G. Infective endocarditis complicated by embolic events: Pathogenesis and predictors. Clin. Cardiol. 2021, 44, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Duval, X.; Alla, F.; Doco-Lecompte, T.; Le Moing, V.; Delahaye, F.; Mainardi, J.L.; Plesiat, P.; Célard, M.; Hoen, B.; Leport, C. Diabetes mellitus and infective endocarditis: The insulin factor in patient morbidity and mortality. Eur. Heart J. 2007, 28, 59–64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Overall | CHADS-VASC 0–2 | CHADS-VASC > 2 | p Value | |
|---|---|---|---|---|
| N | 330 | 151 | 179 | |
| Age (years) | 65.2 ± 14.7 | 56 ± 14.2 | 72.9 ± 10 | <0.001 |
| Gender—male | 232 (70) | 124 (82) | 108 (60) | <0.001 |
| Diabetes mellitus | 107 (32) | 13 (8.6) | 94 (52.5) | <0.001 |
| Hypertension | 150 (46) | 33 (21.9) | 117 (65) | <0.001 |
| Coronary artery disease | 111 (34) | 15 (9.9) | 96 (53.6) | <0.001 |
| Heart failure | 104 (32) | 28 (18.5) | 76 (42.5) | <0.001 |
| Prior stroke | 61 (21.3) | 4 (3.4) | 57 (33.5) | <0.001 |
| Atrial fibrillation | 55 (16.7) | 11 (7.3) | 44 (24.6) | <0.001 |
| Chronic kidney disease | 40 (26.8) | 10 (16.1) | 30 (34.5) | 0.021 |
| Malignancy (active or past) | 38 (11.5) | 10 (6.6) | 28 (15.6) | 0.017 |
| Prosthetic valve | 137 (42) | 50 (33.1) | 87 (48.6) | 0.006 |
| Mechanical | 55 (16.7) | 23 (15.2) | 32 (17.9) | 0.621 |
| Biological | 21 (6.4) | 14 (9.3) | 7 (3.9) | 0.078 |
| Percutaneous valve (TAVI, Melody) | 33 (10) | 2 (1.3) | 31 (17.3) | <0.001 |
| Prior endocarditis | 23 (7) | 7 (4.6) | 16 (8.9) | 0.189 |
| Cardiovascular implantable electronic device (Pacemaker/CRT/ICD) | 51 (15.5) | 13 (8.6) | 38 (21.2) | 0.003 |
| Vascular catheters (Piccline/portacath/permacath) | 27 (8.2) | 7 (4.6) | 20 (11.2) | 0.05 |
| Overall | CHADS-VASC 0–2 | CHADS-VASC > 2 | p Value | |
|---|---|---|---|---|
| N | 330 | 151 | 179 | |
| Fever (max, °C) | 37.9 ± 0.9 | 37.8 ± 0.9 | 38 ± 0.9 | 0.213 |
| CRP (highest) | 16.481 ± 0.75 | 16.62 ± 10.94 | 16.37 ± 10.62 | 0.836 |
| Hemoglobin (on presentation, g/dL) | 11.13 ± 2.12 | 11.44 ± 2.23 | 10.87 ± 1.99 | 0.016 |
| Creatinine (on presentation, mg/dL) | 1.62 ± 1.53 | 1.46 ± 1.52 | 1.75 ± 1.53 | 0.082 |
| Platelets (on presentation) | 210 ± 96 | 213 ± 102 | 207 ± 91 | 0.541 |
| Albumin (on presentation, g/dL) | 3.57 ± 0.62 | 3.64 ± 0.66 | 3.51 ± 0.58 | 0.058 |
| WBC (on presentation, k/µL) | 10.91 ± 5.8 | 10.68 ± 5.85 | 11.1 ± 5.76 | 0.513 |
| CRP (on presentation) | 10.79 ± 8.97 | 11.05 ± 9.41 | 10.56 ± 8.61 | 0.625 |
| Cardiac CT | 95 (28.8) | 54 (35.8) | 41 (22.9) | 0.014 |
| FDG—PET—CT | 96 (29.1) | 43 (28.5) | 53 (29.6) | 0.917 |
| Trans-esophageal echocardiography | 278 (84) | 113 (75) | 165 (92) | <0.001 |
| Ejection fraction—median (IQR) | 60 (45–60) | 60 (55–60) | 60 (40–60) | 0.009 |
| Echo abscess | 49 (14.8%) | 28 (18.5%) | 21 (11.7%) | 0.521 |
| Echo vegetation | 191 (57.9%) | 95 (62.9%) | 95 (53.1%) | 0.071 |
| Endocarditis on prosthetic valve | ||||
| Positive IE imaging on FDG PET CT | 35 (10.6) | 20 (13.2) | 15 (8.4) | 0.211 |
| Positive IE imaging cardiac CT | 151 (46) | 74 (49) | 77 (43) | 0.328 |
| Microbiology | 0.001 | |||
| Enterococcus | 40 (12.1) | 11 (7.3) | 29 (16.2) | |
| Fungi | 3 (0.9) | 1 (0.7) | 2 (1.1) | |
| Gram-negative bacteria | 16 (4.8) | 5 (3) | 11 (6.7) | |
| CoNS | 37 (11.2) | 15 (9.9) | 22 (12.3) | |
| HACEK group | 13 (3.9) | 8 (5.3) | 5 (2.8) | |
| MRSA | 14 (4.2) | 3 (1.8) | 11 (6.7) | |
| MSSA | 46 (13.9) | 19 (12.6) | 27 (15.1) | |
| Other strep species | 59 (17.9) | 26 (17.2) | 33 (18.4) | |
| Others | 64 (19.4) | 45 (29.8) | 19 (10.6) | |
| Q FEVER | 11 (3.3) | 5 (3.3) | 6 (3.6) | |
| Strep viridans | 27 (8.2) | 14 (9.3) | 13 (7.3) |
| Overall | CHADS-VASC ≤ 2 | CHADS-VASC > 2 | p Value | |
|---|---|---|---|---|
| N | 330 | 151 | 179 | |
| Surgical valve replacement/repair | 102 (31) | 63 (41.7) | 39 (21.8) | <0.001 |
| Conservative management | 228 (69) | 88 (58.3) | 140 (78) | <0.001 |
| In-hospital brain emboli and stroke | 46 (13.9) | 26 (17.2) | 20 (11.2) | 0.156 |
| In-hospital acute kidney injury | 93 (33.9) | 29 (25.7) | 64 (39.8) | 0.022 |
| In-hospital mortality | 48 (14.5) | 13 (8.6) | 35 (19.6) | 0.008 |
| 1-year mortality | 88 (26.7) | 24 (15.9) | 64 (35.8) | <0.001 |
| Hospital stay (days) | 19.57 (16.08) | 18.57 (15.66) | 20.62 (16.51) | 0.25 |
| Overall mortality (study period) | 121 (36.7) | 30 (19.9) | 91 (50.8) | <0.001 |
| HR (CI) | p Value | |
|---|---|---|
| CHA2DS-VASC 1 | 1.44 [0.51, 4.05] | 0.485 |
| CHA2DS-VASC 2 | 1.61 [0.57, 4.58] | 0.37 |
| CHA2DS-VASC 3 | 3.06 [1.13, 8.24] | 0.027 |
| CHA2DS-VASC 4 | 3.90 [1.51, 10.09] | 0.005 |
| CHA2DS-VASC 5 | 5.87 [2.21, 15.58] | <0.001 |
| CHA2DS-VASC 6 | 4.94 [1.78, 13.73] | 0.002 |
| CHA2DS-VASC 7–9 | 3.61 [1.18, 11.03] | 0.024 |
| HR (CI) | p Value | |
|---|---|---|
| CHA2DS-VASC > 2 | 2.21 [1.12, 4.39] | 0.023 |
| Acute kidney injury | 2.18 [1.44, 3.30] | <0.001 |
| Age | 1.02 [1.00, 1.04] | 0.088 |
| Male | 1.32 [0.85, 2.04] | 0.215 |
| Coronary artery disease | 1.08 [0.68, 1.74] | 0.737 |
| Atrial fibrillation | 0.83 [0.54, 1.28] | 0.392 |
| Diabetes mellitus | 1.33 [0.87, 2.02] | 0.189 |
| Hypertension | 1.22 [0.79, 1.88] | 0.368 |
| Embolic stroke | 1.16 [0.66, 2.04] | 0.613 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Itelman, E.; Sharony, R.; Hamdan, A.; Atamna, A.; Shaked, H.; Rubchevsky, V.; Barak, Y.D.; Bernstine, H.; Shapira, Y.; Vaturi, M.; et al. The Usefulness of the CHA2DS2-VASc Score to Predict Outcomes in Patients with Infective Endocarditis. J. Clin. Med. 2024, 13, 4917. https://doi.org/10.3390/jcm13164917
Itelman E, Sharony R, Hamdan A, Atamna A, Shaked H, Rubchevsky V, Barak YD, Bernstine H, Shapira Y, Vaturi M, et al. The Usefulness of the CHA2DS2-VASc Score to Predict Outcomes in Patients with Infective Endocarditis. Journal of Clinical Medicine. 2024; 13(16):4917. https://doi.org/10.3390/jcm13164917
Chicago/Turabian StyleItelman, Edward, Ram Sharony, Ashraf Hamdan, Alaa Atamna, Hila Shaked, Victor Rubchevsky, Yaron D. Barak, Hanna Bernstine, Yaron Shapira, Mordehay Vaturi, and et al. 2024. "The Usefulness of the CHA2DS2-VASc Score to Predict Outcomes in Patients with Infective Endocarditis" Journal of Clinical Medicine 13, no. 16: 4917. https://doi.org/10.3390/jcm13164917
APA StyleItelman, E., Sharony, R., Hamdan, A., Atamna, A., Shaked, H., Rubchevsky, V., Barak, Y. D., Bernstine, H., Shapira, Y., Vaturi, M., Epstein, H. O., Kornowski, R., & Orvin, K. (2024). The Usefulness of the CHA2DS2-VASc Score to Predict Outcomes in Patients with Infective Endocarditis. Journal of Clinical Medicine, 13(16), 4917. https://doi.org/10.3390/jcm13164917