
Transthoracic Cross Clamp versus Endoaortic Balloon Occlusion in Minimally Invasive Mitral Valve Surgery: A Pooled Study with Subgroup Analyses
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Articles Selection Strategy
2.2. Data Extraction and Endpoints
2.3. Sensitivity Analysis on Primary Endpoints
2.4. Quality and Publication Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Search Strategy and Patient Demographics
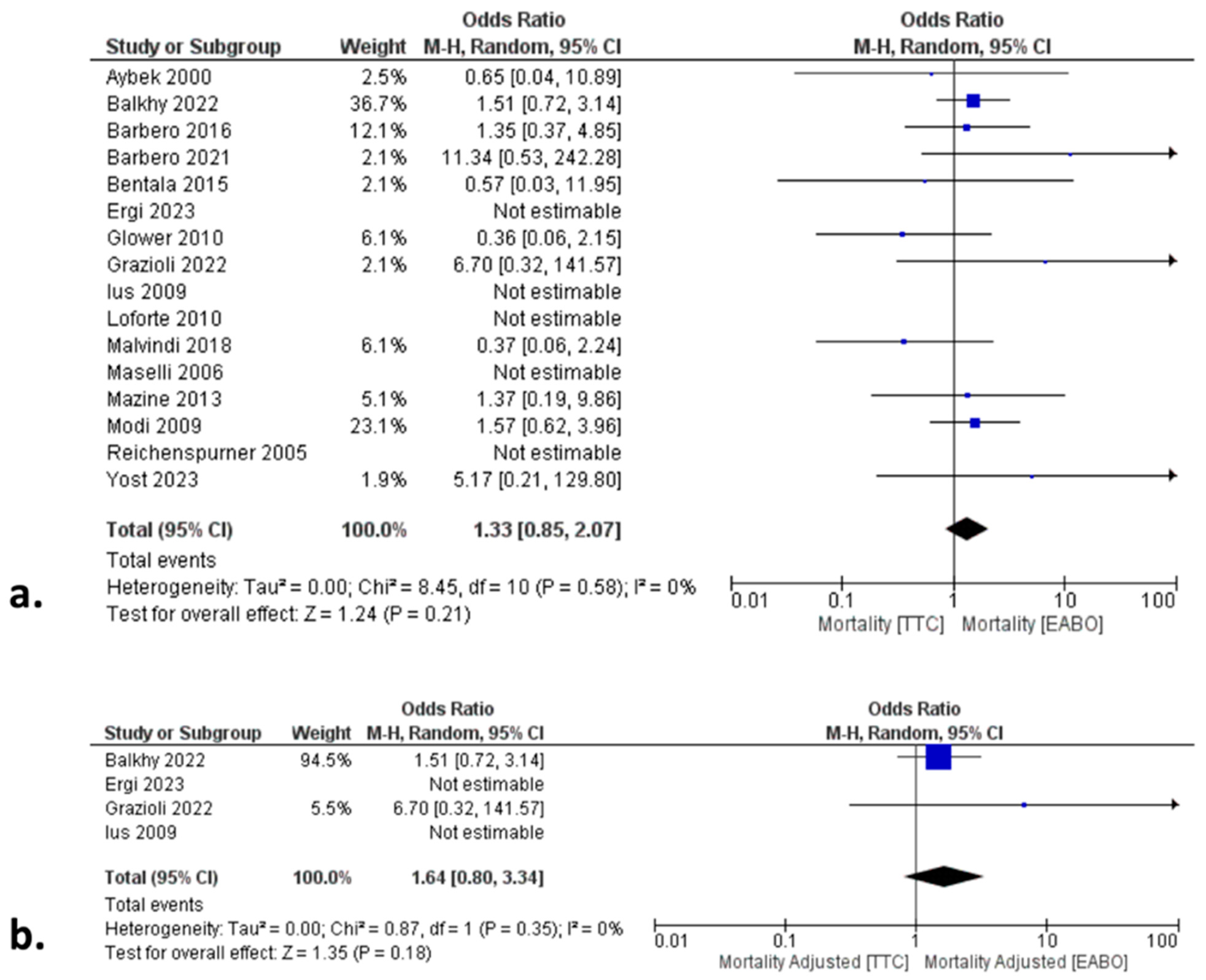
3.2. Primary Endpoints: All-Cause Mortality, CVA, and Aortic Dissection
3.3. Secondary Endpoints
3.4. Subgroup and Sensitivity Analyses
3.5. Quality and Publication Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watt, T.M.F.; Brescia, A.A.; Murray, S.L.; Burn, D.A.; Wisniewski, A.; Romano, M.A.; Bolling, S.F. Degenerative Mitral Valve Repair Restores Life Expectancy. Ann. Thorac. Surg. 2020, 109, 794–801. [Google Scholar] [CrossRef]
- Mihaljevic, T.; Jarrett, C.M.; Gillinov, A.M.; Williams, S.J.; DeVilliers, P.A.; Stewart, W.J.; Svensson, L.G.; Sabik, J.F.; Blackstone, E.H. Robotic repair of posterior mitral valve prolapse versus conventional approaches: Potential realized. J. Thorac. Cardiovasc. Surg. 2011, 141, 72–80.e4. [Google Scholar] [CrossRef] [PubMed]
- Bates, M.J.; Chitwood, W.R. Minimally invasive and robotic approaches to mitral valve surgery: Transthoracic aortic crossclamping is optimal. JTCVS Tech. 2021, 10, 84–88. [Google Scholar] [CrossRef]
- Mohr, F.W.; Falk, V.; Diegeler, A.; Walther, T.; Van Son JA, M.; Autschbach, R.; Borst, H.G. Minimally invasive port-access mitral valve surgery. J. Thorac. Cardiovasc. Surg. 1998, 115, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Rival, P.M.; Moore, T.H.M.; McAleenan, A.; Hamilton, H.; Du Toit, Z.; Akowuah, E.; Angelini, G.D.; A Vohra, H. Transthoracic clamp versus endoaortic balloon occlusion in minimally invasive mitral valve surgery: A systematic review and meta-analysis. Eur. J. Cardiothorac. Surg. 2019, 56, 643–653. [Google Scholar] [CrossRef]
- Kowalewski, M.; Malvindi, P.G.; Suwalski, P.; Raffa, G.M.; Pawliszak, W.; Perlinski, D.; Kowalkowska, M.E.; Kowalewski, J.; Carrel, T.; Anisimowicz, L. Clinical safety and effectiveness of endoaortic as compared to transthoracic clamp for small thoracotomy mitral valve surgery: Metaanalysis of observational studies. Ann. Thoracic. Surg. 2017, 103, 676–686. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration. 2011. Available online: www.cochrane-handbook.org (accessed on 1 July 2024).
- Aybek, T.; Dogan, S.; Wimmer-Greinecker, G.; Westphal, K.; Mortiz, A. The micro-mitral operation comparing the Port-Access technique and the transthoracic clamp technique. J. Card. Surg. 2000, 15, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Balkhy, H.H.; Grossi, E.A.; Kiaii, B.; Murphy, D.; Geirsson, A.; Guy, S.; Lewis, C. A Retrospective Evaluation of Endo-Aortic Balloon Occlusion Compared to External Clamping in Minimally Invasive Mitral Valve Surgery. Semin. Thorac. Cardiovasc. Surg. 2024, 36, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Barbero, C.; Marchetto, G.; Ricci, D.; El Qarra, S.; Attisani, M.; Filippini, C.; Boffini, M.; Rinaldi, M. Right Minithoracotomy for Mitral Valve Surgery: Impact of Tailored Strategies on Early Outcome. Ann. Thorac. Surg. 2016, 102, 1989–1994. [Google Scholar] [CrossRef]
- Barbero, C.; Rinaldi, M.; Pocar, M.; Cura Stura, E.; Calia, C.; Sebastiano, V.; Marchetto, G.; Filippini, C.; Boffini, M.; Ricci, D. Endo-Aortic vs. Trans-Thoracic Clamping in Right Mini-Thoracotomy Mitral Valve Surgery: Outcome on Myocardial Protection. Front. Cardiovasc. Med. 2021, 8, 719687. [Google Scholar] [CrossRef] [PubMed]
- Bentala, M.; Heuts, S.; Vos, R.; Maessen, J.; Scohy, T.V.; Gerritse, B.M.; Sardari Nia, P. Comparing the endo-aortic balloon and the external aortic clamp in minimally invasive mitral valve surgery. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 359–365. [Google Scholar] [CrossRef]
- Ergi, D.G.; Rowse, P.G.; Daly, R.C.; Crestanello, J.A.; Schaff, H.V.; Dearani, J.A.; Todd, A.; Arghami, A. Single Center Prospective Study of Cross-Clamp versus Balloon Occlusion in Robotic Mitral Surgery. Ann. Thorac. Surg. 2024, 118, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Glower, D.D.; Desai, B. Transaortic endoclamp for mitral valve operation through right minithoracotomy in 369 patients. Innovations 2010, 5, 394–399. [Google Scholar] [CrossRef]
- Grazioli, V.; Giroletti, L.; Graniero, A.; Albano, G.; Mazzoni, M.; Panisi, P.G.; Gerometta, P.; Anselmi, A.; Agnino, A. Comparative myocardial protection of endoaortic balloon versus external clamp in minimally invasive mitral valve surgery. J. Cardiovasc. Med. 2023, 24, 184–190. [Google Scholar] [CrossRef]
- Ius, F.; Mazzaro, E.; Tursi, V.; Guzzi, G.; Spagna, E.; Vetrugno, L.; Bassi, F.; Livi, U. Clinical results of minimally invasive mitral valve surgery: Endoaortic clamp versus external aortic clamp techniques. Innovations 2009, 4, 311–318. [Google Scholar] [CrossRef]
- Loforte, A.; Luzi, G.; Montalto, A.; Ranocchi, F.; Polizzi, V.; Sbaraglia, F.; Della Monica, P.L.; Menichetti, A.; Musumeci, F. Video-assisted minimally invasive mitral valve surgery: External aortic clamp versus endoclamp techniques. Innovations 2010, 5, 413–418. [Google Scholar] [CrossRef]
- Malvindi, P.G.; Margari, V.; Mastro, F.; Visicchio, G.; Kounakis, G.; Favale, A.; Dambruoso, P.; Labriola, C.; Carbone, C.; Paparella, D.; et al. External aortic cross-clamping and endoaortic balloon occlusion in minimally invasive mitral valve surgery. Ann. Cardiothorac. Surg. 2018, 7, 748–754. [Google Scholar] [CrossRef]
- Maselli, D.; Pizio, R.; Borelli, G.; Musumeci, F. Endovascular balloon versus transthoracic aortic clamping for minimally invasive mitral valve surgery: Impact on cerebral microemboli. Interact. Cardiovasc Thorac Surg. 2006, 5, 183–186. [Google Scholar] [CrossRef]
- Mazine, A.; Pellerin, M.; Lebon, J.S.; Dionne, P.O.; Jeanmart, H.; Bouchard, D. Minimally invasive mitral valve surgery: Influence of aortic clamping technique on early outcomes. Ann. Thorac. Surg. 2013, 96, 2116–2122. [Google Scholar] [CrossRef]
- Modi, P.; Rodriguez, E.; Hargrove, W.C., 3rd; Hassan, A.; Szeto, W.Y.; Chitwood, W.R., Jr. Minimally invasive video-assisted mitral valve surgery: A 12-year, 2-center experience in 1178 patients. J. Thorac. Cardiovasc. Surg. 2009, 137, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Reichenspurner, H.; Detter, C.; Deuse, T.; Boehm, D.H.; Treede, H.; Reichart, B. Video and robotic-assisted minimally invasive mitral valve surgery: A comparison of the Port-Access and transthoracic clamp techniques. Ann Thorac Surg. 2005, 79, 485–490; discussion 490–491. [Google Scholar] [CrossRef]
- Yost, C.C.; Rosen, J.L.; Mandel, J.L.; Prochno, K.W.; Wu, M.; Komlo, C.M.; Guy, T.S. Endoaortic balloon occlusion versus transthoracic cross-clamp for totally endoscopic robotic mitral valve surgery: A retrospective cohort study. J. Robot. Surg. 2023, 17, 2305–2313. [Google Scholar] [CrossRef] [PubMed]
- Marullo, A.; Irace, F.; Vitulli, P.; Peruzzi, M.; Rose, D.; D’Ascoli, R. Recent developments in minimally invasive cardiac surgery: Evolution or revolution? Biomed Res. Int. 2015, 2015, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Atluri, P.; Goldstone, A.B.; Fox, J.Y.; Szeto, W.; Hargrove, W.C. Port access cardiac operations can be safely performed with either endoaortic balloon or Chitwood clamp. Ann. Thorac. Surg. 2014, 98, 1579–1584. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study ID, Year | Study Design | Patients, n TTC/EABO | Age, Mean ± SD TTC/EABO | Female Sex, % TTC/EABO | LVEF, Mean ± SD, TTC/EABO | NYHA Class 3/4, % TTC/EABO | Previous CVA, % TTC/EABO | Previous CS, % TTC/EABO | Type of TTC | Type of EABO Cannulation Approach | MVR:MVRe, % TTC/EABO | NOS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aybek, 2000 [11] | R | 35/23 | 56 ± 13/58 ± 16 | 46/52 | 61 ± 11/66 ± 13 | 3 ± 1/3 ± 1 | 3/0 | N/A | Chitwood | Heartport Endoaortic Clamp | 37:63/26:74 | 5 |
| Balkhy, 2022 [12] | R-STS-A | 1163/1163 | 62 ± 12/62 ± 12 | 36/36 | EF < 30: 1/1 | 23/23 | 8/8 | 6/5 | N/A | Intraclude | 14:86/14:86 | 8 |
| Barbero, 2016 [13] | R | 150/301 | 67 ± 12/P:61 ± 14 C: 69 ± 9 | 43/P: 52 C: 24 | 61 ± 10/P: 59 ± 11 C: 57 ± 13 | N/A | 11/P: 6 C: 10 | 6/P: 32 C: 25 | Chitwood | Intraclude | 38:62/40:60 | 6 |
| Barbero, 2021 [14] | P | 37/80 | 62 ± 9/55 ± 12 | 30/35 | 63 ± 8/62 ± 7 | N/A | N/A | 3/10 | Chitwood | Intraclude | 10:90/21:79 | 6 |
| Bentala, 2015 [15] | R | 57/164 | 62 (57–73)/66 (60–74) | 44/44 | EF < 30: 9/4 | NYHA III: 54/52 | 7/2 | N/A | Chitwood | Intraclude | 16:84/9:91 | 6 |
| Ergi, 2023 [16] | P-A | 168/56 | 65 (56–70)/66 (55–72) | 32/27 | 63 (59–65)/61.5 (59–65) | 17/17 | 0/0 | N/A | Chitwood | IntraClude | N/A | 8 |
| Glower, 2010 [17] | R | 436/235 | 59 ± 13/58 ± 14 | 53/59 | 51 ± 12/53 ± 10 | 72/56 | N/A | 20/14 | Cosgrove | Intraclude | 22:78/33:67 | 6 |
| Grazioli, 2022 [18] | R-A | 78/102 | 60 ± 14/6 ± 12 | 35/49 | 58 ± 6/56 ± 8 | 31/48 | N/A | N/A | Chitwood, Cygnet | Intraclude | 14:86/23:77 | 7 |
| Ius, 2009 [19] | R-A | 95/32 | 62 ± 11/63 ± 9 | 49/59 | 65 ± 8/64 ± 8 | 26/22 | N/A | N/A | Cygnet, Portaclamp, Chitwood | Intraclude | 23:77/41:59 | 7 |
| Loforte, 2010 [20] | R * | 93/45 | 59 ± 8/58 ± 11 | 73/78 | 60 ± 10/58 ± 9 | 40/40 | N/A | 0/0 | Cygnet | Intraclude | 77:23/73:27 | 6 |
| Malvindi, 2018 [21] | R * | 165/93 | 63 ± 13/56 ± 15 | 47/51 | 55 ± 7/55 ± 9 | N/A | N/A | N/A | N/A | N/A | 30:70/42:58 | 6 |
| Maselli, 2006 [22] | P | 16/20 | 55 ± 5/57 ± 6 | 63/70 | N/A | N/A | N/A | N/A | Chitwood | Intraclude | 38:62/45:55 | 6 |
| Mazine, 2013 [23] | R * | 103/140 | 62 ± 11/55 ± 2 | 39/40 | 61 ± 9/61 ± 8 | 32/31 | 6/6 | 3/7 | Chitwood | N/A | 13:87/20:80 | 6 |
| Modi, 2009 [24] | P | 573/479 | 61 ± 14 | 51 | N/A | N/A | N/A | 7/15 | N/A | N/A | 20:80/15:85 | 6 |
| Reichenspurner, 2005 [25] | R | 60/60 | 62 ± 11 | 71 | 56 ± 16 | N/A | N/A | N/A | Chitwood | Intraclude | 33:67 | 5 |
| Yost, 2023 [26] | R | 42/71 | 62 (56–69)/65 (56–72) | 40/30 | N/A | N/A | 7/11 | N/A | Chitwood | IntraClude | 2:98/9:91 | 6 |
| Baseline Characteristics | Arms | OR * | 95% CI | p-Value | Heterogeneity | |
|---|---|---|---|---|---|---|
| I2 | p-Value | |||||
| Age | 14 | 0.21 | −1.5, 1.93 | 0.81 | 90% | <0.01 |
| Female ratio | 14 | 0.92 | 0.82, 0.73 | 0.15 | 0% | 0.82 |
| LVEF | 10 | 0.55 | −0.49, 1.59 | 0.30 | 63% | <0.01 |
| NYHA III/IV | 8 | 1.08 | 0.80, 1.47 | 0.06 | 66% | <0.01 |
| Previous CVA | 7 | 1.04 | 0.79, 1.36 | 0.80 | 0% | 0.57 |
| Previous CS | 8 | 0.45 | 0.22, 0.91 | 0.03 | 88% | <0.01 |
| MVR rate | 15 | 0.83 | 0.65, 1.05 | 0.12 | 55% | <0.01 |
| Endpoints | Arms | OR * | 95% CI | p-Value | Heterogeneity | |
|---|---|---|---|---|---|---|
| I2 | p-Value | |||||
| Total cohort | ||||||
| All-cause mortality | 16 | 1.33 | 0.85, 2.07 | 0.21 | 0% | 0.58 |
| CPB time | 17 | −1.68 | −8.21, 4.85 | 0.61 | 95% | <0.01 |
| Aortic cross-clamp time | 16 | −3.27 | −7.61, 1.07 | 0.14 | 92% | <0.01 |
| Conversion to sternotomy | 14 | 0.51 | 0.19, 1.39 | 0.19 | 65% | <0.01 |
| Aortic dissection | 15 | 0.51 | 0.20, 1.33 | 0.17 | 0% | 0.50 |
| CVA | 15 | 0.68 | 0.44, 1.04 | 0.07 | 0% | 0.59 |
| Re-exploration | 14 | 0.90 | 0.64, 1.28 | 0.57 | 0% | 0.61 |
| Ventilation | 8 | −0.03 | −0.58, 0.52 | 0.92 | 0% | 0.71 |
| New onset AF | 10 | 0.86 | 0.61, 1.21 | 0.37 | 54% | 0.03 |
| AKI | 11 | 1.22 | 0.91, 1.65 | 0.19 | 0% | 0.85 |
| ICU stay | 10 | −0.27 | −0.72, 0.19 | 0.25 | 97% | <0.01 |
| LOS | 15 | −0.20 | −0.99, 0.58 | 0.61 | 99% | <0.01 |
| Femoral cannulation EABO | ||||||
| All-cause mortality | 14 | 1.44 | 0.91, 2.28 | 0.12 | 0% | 0.71 |
| CPB time | 14 | −3.78 | −9.84, 2.28 | 0.22 | 94% | <0.01 |
| Aortic cross-clamp time | 13 | −5.60 | −10.47, −0.73 | 0.02 | 93% | <0.01 |
| Conversion to sternotomy | 14 | 0.52 | 0.19, 1.40 | 0.20 | 65% | <0.01 |
| Aortic dissection | 14 | 0.51 | 0.20, 1.33 | 0.17 | 0% | 0.50 |
| CVA | 15 | 0.66 | 0.43, 1.02 | 0.06 | 0% | 0.65 |
| Re-exploration | 13 | 0.87 | 0.61, 1.24 | 0.45 | 0% | 0.59 |
| Ventilation | 7 | −0.04 | −0.59, 0.51 | 0.89 | 0% | 0.64 |
| New onset AF | 9 | 1.12 | 0.93, 1.35 | 0.22 | 0% | 0.44 |
| AKI | 10 | 1.27 | 0.93, 1.72 | 0.13 | 0% | 0.88 |
| ICU stay | 9 | −0.30 | −0.78, 0.18 | 0.22 | 98% | <0.01 |
| LOS | 13 | −0.20 | −1.17, 0.77 | 0.69 | 99% | <0.01 |
| Aortic cannulation EABO | ||||||
| All-cause mortality | 2 | 1.51 | 0.72, 3.14 | 0.21 | N/A | − |
| CPB time | 3 | 10.07 | −35.55, 55.49 | 0.66 | 98% | <0.01 |
| Aortic cross-clamp time | 3 | 7.89 | 3.65, 12.12 | <0.01 | 0% | 0.42 |
| Conversion to sternotomy | 2 | 0.14 | 0.01, 3.44 | 0.23 | N/A | − |
| Aortic dissection | 2 | N/E | − | − | − | − |
| CVA | 2 | 3.01 | 0.15, 59.20 | 0.47 | N/A | − |
| Re-exploration | 2 | 1.60 | 0.51, 4.97 | 0.42 | 0% | 0.75 |
| Ventilation | 1 | 2.60 | −6.73, 11.93 | 0.58 | N/A | − |
| New onset AF | 1 | 0.45 | 0.27, 0.76 | <0.01 | N/A | − |
| AKI | 2 | 0.73 | 0.25, 2.08 | 0.13 | 0% | 0.88 |
| ICU stay | 1 | 0.10 | −0.70, 0.90 | 0.81 | N/A | − |
| LOS | 2 | 0.00 | −0.10, 0.10 | 0.99 | 0% | 0.40 |
| Video-assisted approach | ||||||
| All-cause mortality | 12 | 1.18 | 0.67, 2.08 | 0.57 | 0% | 0.48 |
| CPB time | 13 | −4.85 | −14.51, 4.80 | 0.32 | 94% | <0.01 |
| Aortic cross-clamp time | 12 | −5.41 | −11.54, 0.72 | 0.08 | 89% | <0.01 |
| Conversion to sternotomy | 10 | 0.31 | 0.16, 0.61 | <0.01 | 0% | 0.69 |
| Aortic dissection | 11 | 0.39 | 0.14, 1.13 | 0.08 | 0% | 0.45 |
| CVA | 11 | 0.55 | 0.31, 0.98 | 0.04 | 0% | 0.52 |
| Re-exploration | 12 | 0.87 | 0.61, 1.23 | 0.43 | 0% | 0.43 |
| Ventilation | 8 | −0.03 | −0.58, 0.52 | 0.92 | 0% | 0.71 |
| New onset AF | 8 | 0.77 | 0.52, 1.14 | 0.19 | 37% | 0.14 |
| AKI | 10 | 1.08 | 0.59, 1.97 | 0.81 | 0% | 0.79 |
| ICU stay | 8 | −0.07 | −0.09, −0.05 | <0.01 | 0% | 0.88 |
| LOS | 12 | −0.40 | −1.36, 0.57 | 0.42 | 99% | <0.01 |
| Robotic-assisted approach | ||||||
| All-cause mortality | 2 | 5.17 | 0.21, 129.80 | 0.32 | N/A | − |
| CPB time | 2 | 13.68 | 7.31, 20.05 | <0.01 | 94% | <0.01 |
| Aortic cross-clamp time | 2 | 4.46 | −4.36, 13.28 | 0.32 | 98% | <0.01 |
| Conversion to sternotomy | 2 | 1.71 | 0.10, 280.03 | 0.71 | N/A | − |
| Aortic dissection | 2 | 1.01 | 0.04, 25.20 | 0.99 | N/A | − |
| CVA | 2 | 0.55 | 0.02, 13.88 | 0.72 | N/A | − |
| Re-exploration | 2 | 5.38 | 0.54, 53.54 | 0.15 | N/A | − |
| Ventilation | 0 | − | − | − | − | − |
| New onset AF | 1 | 1.38 | 0.49, 3.86 | 0.54 | N/A | − |
| AKI | 0 | − | − | − | − | − |
| ICU stay | 0 | − | − | − | − | − |
| LOS | 1 | 0.00 | −0.14, 0.14 | 1.00 | N/A | − |
| Risk-Adjusted Total Cohort | ||||||
| All-cause mortality | 4 | 1.64 | 0.80, 3.34 | 0.18 | 0% | 0.35 |
| CPB time | 4 | 0.51 | −9.03, 10.06 | 0.92 | 89% | <0.01 |
| Aortic cross-clamp time | 4 | −3.84 | −9.16, 1.49 | 0.16 | 81% | <0.01 |
| Conversion to sternotomy | 4 | 0.51 | 0.05, 5.54 | 0.58 | 84% | <0.01 |
| Aortic dissection | 4 | 0.90 | 0.14, 5.93 | 0.91 | 29% | 0.24 |
| CVA | 4 | 0.71 | 0.35, 1.44 | 0.34 | 7% | 0.34 |
| Re-exploration | 3 | 1.03 | 0.04, 25.96 | 0.98 | N/A | − |
| Ventilation | 2 | −5.77 | −19.75, 8.21 | 0.42 | 58% | 0.12 |
| New onset AF | 4 | 1.18 | 0.97, 1.44 | 0.10 | 0% | 0.50 |
| AKI | 4 | 1.33 | 0.96, 1.84 | 0.09 | 0% | 0.39 |
| ICU stay | 4 | −0.50 | −1.28, 0.28 | 0.21 | 99% | <0.01 |
| LOS | 4 | 0.30 | −0.60, 1.21 | 0.51 | 95% | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magouliotis, D.E.; Sicouri, S.; Baudo, M.; Yamashita, Y.; Xanthopoulos, A.; Arjomandi Rad, A.; Athanasiou, T.; Ramlawi, B. Transthoracic Cross Clamp versus Endoaortic Balloon Occlusion in Minimally Invasive Mitral Valve Surgery: A Pooled Study with Subgroup Analyses. J. Clin. Med. 2024, 13, 4989. https://doi.org/10.3390/jcm13174989
Magouliotis DE, Sicouri S, Baudo M, Yamashita Y, Xanthopoulos A, Arjomandi Rad A, Athanasiou T, Ramlawi B. Transthoracic Cross Clamp versus Endoaortic Balloon Occlusion in Minimally Invasive Mitral Valve Surgery: A Pooled Study with Subgroup Analyses. Journal of Clinical Medicine. 2024; 13(17):4989. https://doi.org/10.3390/jcm13174989
Chicago/Turabian StyleMagouliotis, Dimitrios E., Serge Sicouri, Massimo Baudo, Yoshiyuki Yamashita, Andrew Xanthopoulos, Arian Arjomandi Rad, Thanos Athanasiou, and Basel Ramlawi. 2024. "Transthoracic Cross Clamp versus Endoaortic Balloon Occlusion in Minimally Invasive Mitral Valve Surgery: A Pooled Study with Subgroup Analyses" Journal of Clinical Medicine 13, no. 17: 4989. https://doi.org/10.3390/jcm13174989