

The Use of Proton Pump Inhibitors in Patients with Liver Cirrhosis: Real Life Experience

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definitions
2.3. Data Collection and Assessment
2.4. Statistical Analysis
3. Results
3.1. Selection of Patients
3.2. Baseline Characteristics of Liver Cirrhosis Cohort
3.3. Comorbidities in Liver Cirrhosis Cohort
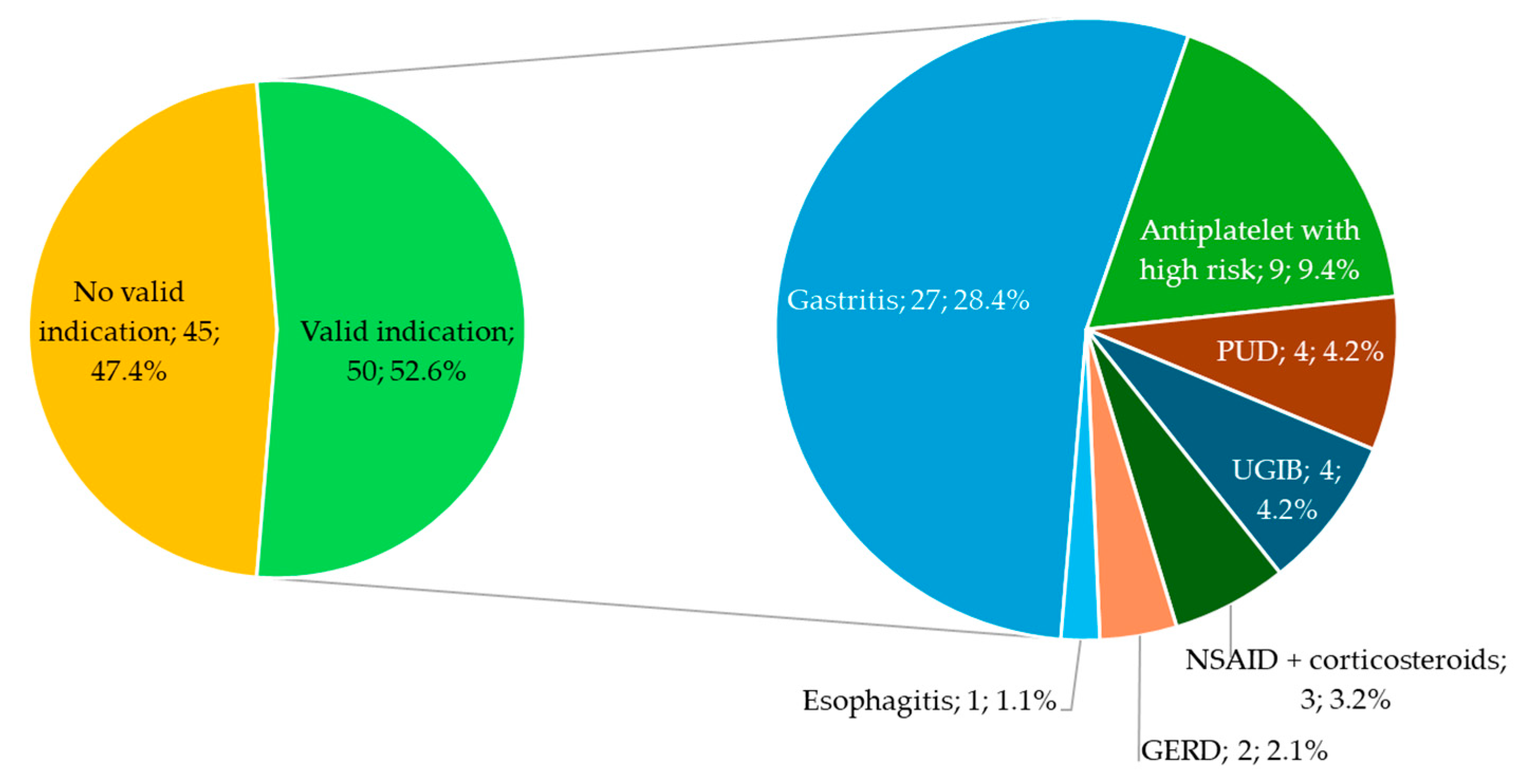
3.4. PPI Prescription during Hospital Stays and at Discharge and the Validity of Prescription
3.5. The Appropriate Indications for PPI Prescription in the Cohort of Patients with Liver Cirrhosis
3.6. Patients without PPI Treatment during Hospital Stays or at Discharge
3.7. Route of Administration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baumgartner, K.; Cooper, J.; Smith, A.; St Louis, J. Liver Disease: Cirrhosis. FP Essent. 2021, 511, 36–43. [Google Scholar] [PubMed]
- Ginès, P.; Krag, A.; Abraldes, J.G.; Solà, E.; Fabrellas, N.; Kamath, P.S. Liver cirrhosis. Lancet 2021, 398, 1359–1376. [Google Scholar] [CrossRef] [PubMed]
- Hsiang, J.C.; Gane, E.J.; Bai, W.W.; Gerred, S.J. Type 2 diabetes: A risk factor for liver mortality and complications in hepatitis B cirrhosis patients. J. Gastroenterol. Hepatol. 2015, 30, 591–599. [Google Scholar] [CrossRef]
- Wang, T.; Huang, S.; Wu, C.; Wang, N.; Zhang, R.; Wang, M.; Mao, D. Intestinal Microbiota and Liver Diseases: Insights into Therapeutic Use of Traditional Chinese Medicine. Evid. Based Complement. Altern. Med. 2021, 2021, 6682581. [Google Scholar] [CrossRef]
- Prescribing PPIs. Drug Ther. Bull. 2017, 55, 117–120. [CrossRef] [PubMed]
- Brandl, K.; Schnabl, B. Is intestinal inflammation linking dysbiosis to gut barrier dysfunction during liver disease? Expert. Rev. Gastroenterol. Hepatol. 2015, 9, 1069–1076. [Google Scholar] [CrossRef]
- Lambert, A.A.; Lam, J.O.; Paik, J.J.; Ugarte-Gil, C.; Drummond, M.B.; Crowell, T.A. Risk of Community-Acquired Pneumonia with Outpatient Proton-Pump Inhibitor Therapy: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0128004. [Google Scholar] [CrossRef]
- Goel, G.A.; Deshpande, A.; Lopez, R.; Hall, G.S.; van Duin, D.; Carey, W.D. Increased rate of spontaneous bacterial peritonitis among cirrhotic patients receiving pharmacologic acid suppression. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2012, 10, 422–427. [Google Scholar] [CrossRef]
- Hwang, S.J.; Lee, D.H.; Koh, S.J.; Kim, J.W.; Park, H.S.; Kim, B.G.; Lee, K.L. Correlation Between Proton Pump Inhibitors and the Complications of Liver Cirrhosis: A Systematic Review and Meta-Analysis. Turk. J. Gastroenterol. 2022, 33, 44–52. [Google Scholar] [CrossRef]
- De Roza, M.A.; Kai, L.; Kam, J.W.; Chan, Y.H.; Kwek, A.; Ang, T.L.; Hsiang, J.C. Proton pump inhibitor use increases mortality and hepatic decompensation in liver cirrhosis. World J. Gastroenterol. 2019, 25, 4933–4944. [Google Scholar] [CrossRef]
- Chinzon, D.; Domingues, G.; Tosetto, N.; Perrotti, M. Safety of Long-Term Proton Pump Inhibitors: Facts and Myths. Arq. Gastroenterol. 2022, 59, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Sakata, Y.; Tsuruoka, N.; Takedomi, H.; Akutagawa, T.; Shimoda, R.; Esaki, M.; Fujimoto, K. A Study on the Status of Proton Pump Inhibitor Prescriptions Using Diagnosis Procedure Combination Data in Japan. Digestion 2020, 101, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Cole, H.L.; Pennycook, S.; Hayes, P.C. The impact of proton pump inhibitor therapy on patients with liver disease. Aliment. Pharmacol. Ther. 2016, 44, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Scarpignato, C.; Gatta, L.; Zullo, A.; Blandizzi, C. Effective and safe proton pump inhibitor therapy in acid-related diseases—A position paper addressing benefits and potential harms of acid suppression. BMC Med. 2016, 14, 179. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Gastro-Oesophageal Reflux Disease and Dyspepsia in Adults: Investigation and Management; NICE Clinical Guidelines, No. 184; National Institute for Health and Care Excellence (NICE): London, UK, 2019. [Google Scholar]
- Lanza, F.L.; Chan, F.K.L.; Quigley, E.M.M.; Practice Parameters Committee of the American College of Gastroenterology. Guidelines for prevention of NSAID-related ulcer complications. Am. J. Gastroenterol. 2009, 104, 728–738. [Google Scholar]
- Freedberg, D.E.; Kim, L.S.; Yang, Y.-X. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 2017, 152, 706–715. [Google Scholar] [CrossRef]
- Chia, C.T.W.; Lim, W.P.; Vu, C.K.F. Inappropriate use of proton pump inhibitors in a local setting. Singap. Med. J. 2014, 55, 363–366. [Google Scholar] [CrossRef]
- Gamelas, V.; Salvado, V.; Dias, L. Prescription Pattern of Proton Pump Inhibitors at Hospital Admission and Discharge. GE Port. J. Gastroenterol. 2019, 26, 114–120. [Google Scholar] [CrossRef]
- Dultz, G.; Piiper, A.; Zeuzem, S.; Kronenberger, B.; Waidmann, O. Proton pump inhibitor treatment is associated with the severity of liver disease and increased mortality in patients with cirrhosis. Aliment. Pharmacol. Ther. 2015, 41, 459–466. [Google Scholar] [CrossRef]
- Dutta, A.K.; Sharma, V.; Jain, A.; Elhence, A.; Panigrahi, M.K.; Mohta, S.; Kirubakaran, R.; Philip, M.; Goenka, M.; Bhatia, S.; et al. Inappropriate use of proton pump inhibitors in clinical practice globally: A systematic review and meta-analysis. Gut 2024. [Google Scholar] [CrossRef]
- García Rodríguez, L.A.; Lanas, A.; Soriano-Gabarró, M.; Vora, P.; Cea Soriano, L. Effect of Proton Pump Inhibitors on Risks of Upper and Lower Gastrointestinal Bleeding among Users of Low-Dose Aspirin: A Population-Based Observational Study. J. Clin. Med. 2020, 9, 928. [Google Scholar] [CrossRef]
- Lodato, F.; Azzaroli, F.; Girolamo, M.D.; Feletti, V.; Cecinato, P.; Lisotti, A.; Festi, D.; Roda, E.; Mazzella, G. Proton pump inhibitors in cirrhosis: Tradition or evidence based practice? World J. Gastroenterol. 2008, 14, 2980–2985. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Mela, G.S.; Zentilin, P.; Mansi, C.; Mele, M.R.; Vigneri, S.; Cutela, P.; Vassallo, A.; Dallorto, E.; Celle, G. Evaluation of 24-hour gastric acidity in patients with hepatic cirrhosis. J. Hepatol. 1996, 25, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Saenz-de-Sicilia, M.; Sanchez-Avila, F.; Chavez-Tapia, N.-C.; Lopez-Arce, G.; Garcia-Osogobio, S.; Ruiz-Cordero, R.; Tellez-Avila, F.-I. PPIs are not associated with a lower incidence of portal-hypertension-related bleeding in cirrhosis. World J. Gastroenterol. 2010, 16, 5869–5873. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.G.; Pounder, R.E.; Burroughs, A.K. Gastric secretion and peptic ulceration in cirrhosis. J. Hepatol. 1993, 19, 171–182. [Google Scholar] [CrossRef]
- Ostrow, J.D.; Timmerman, R.J.; Gray, S.J. Gastric Secretion in Human Hepatic Cirrhosis. Gastroenterology 1960, 38, 303–316. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Cox, I.J.; Betrapally, N.S.; Heuman, D.M.; Schubert, M.L.; Ratneswaran, M.; Hylemon, P.B.; White, M.B.; Daita, K.; Noble, N.A.; et al. Systems biology analysis of omeprazole therapy in cirrhosis demonstrates significant shifts in gut microbiota composition and function. Am. J. Physiol. Gastrointest. Liver Physiol. 2014, 307, G951–G957. [Google Scholar] [CrossRef]
- Qi, X.; Su, C.; Ren, W.; Yang, M.; Jia, J.; Dai, J.; Xu, W.; Guo, X. Association between portal vein thrombosis and risk of bleeding in liver cirrhosis: A systematic review of the literature. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 683–691. [Google Scholar] [CrossRef]
- Flores, B.; Trivedi, H.D.; Robson, S.C.; Bonder, A. Hemostasis, bleeding and thrombosis in liver disease. J. Transl. Sci. 2017, 3. [Google Scholar] [CrossRef]
- Serper, M.; Weinberg, E.M.; Cohen, J.B.; Reese, P.P.; Taddei, T.H.; Kaplan, D.E. Mortality and Hepatic Decompensation in Patients With Cirrhosis and Atrial Fibrillation Treated With Anticoagulation. Hepatol. Baltim. Md. 2021, 73, 219–232. [Google Scholar] [CrossRef]
- Ma, J.; Chalasani, N.P.; Schwantes-An, L.; Björnsson, E.S. Review article: The safety of anticoagulants and antiplatelet agents in patients with cirrhosis. Aliment. Pharmacol. Ther. 2023, 57, 52–71. [Google Scholar] [CrossRef]
- Cui, S.-B.; Shu, R.-H.; Yan, S.-P.; Wu, H.; Chen, Y.; Wang, L.; Zhu, Q. Efficacy and safety of anticoagulation therapy with different doses of enoxaparin for portal vein thrombosis in cirrhotic patients with hepatitis B. Eur. J. Gastroenterol. Hepatol. 2015, 27, 914–919. [Google Scholar] [CrossRef]
- Lee, S.R.; Kwon, S.; Choi, E.-K.; Jung, J.-H.; Han, K.-D.; Oh, S.; Lip, G.Y.H. Proton Pump Inhibitor Co-Therapy in Patients with Atrial Fibrillation Treated with Oral Anticoagulants and a Prior History of Upper Gastrointestinal Tract Bleeding. Cardiovasc. Drugs Ther. 2022, 36, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Butler, E.; Møller, M.H.; Cook, O.; Granholm, A.; Penketh, J.; Rygård, S.L.; Aneman, A.; Perner, A. The effect of systemic corticosteroids on the incidence of gastrointestinal bleeding in critically ill adults: A systematic review with meta-analysis. Intensive Care Med. 2019, 45, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Narum, S.; Westergren, T.; Klemp, M. Corticosteroids and risk of gastrointestinal bleeding: A systematic review and meta-analysis. BMJ Open 2014, 4, e004587. [Google Scholar] [CrossRef] [PubMed]
- Conn, H.O.; Poynard, T. Corticosteroids and peptic ulcer: Meta-analysis of adverse events during steroid therapy. J. Intern. Med. 1994, 236, 619–632. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, N.; Jia, X.; Zhai, Y.; Xue, X.; Qiao, Y. Appropriateness and Associated Factors of Stress Ulcer Prophylaxis for Surgical Inpatients of Orthopedics Department in a Tertiary Hospital: A Cross-Sectional Study. Front. Pharmacol. 2022, 13, 881063. [Google Scholar] [CrossRef]
- Thurber, K.M.; O Otto, A.; Stricker, S.L. Proton pump inhibitors: Understanding the associated risks and benefits of long-term use. Am. J. Health-Syst. Pharm. AJHP Off. J. Am. Soc. Health-Syst. Pharm. 2023, 80, 487–494. [Google Scholar] [CrossRef]
- Mahmud, N.; Serper, M.; Taddei, T.H.; Kaplan, D.E. The Association Between Proton Pump Inhibitor Exposure and Key Liver-Related Outcomes in Patients With Cirrhosis: A Veterans Affairs Cohort Study. Gastroenterology 2022, 163, 257–269. [Google Scholar] [CrossRef]
- Cacciola, I. Effects of Proton Pump Inhibitors in Cirrhotic Patients: What Do We Really Know? Gastroenterology 2022, 163, 47–49. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Liver Cirrhosis Patients (N = 189) | |
|---|---|---|
| Age, Mean ± SD [Min–Max] | 63.1 ± 9.7 (41–89) | |
| Gender, No. (%) | ||
| Male | 127 (67.2) | |
| Female | 62 (32.8) | |
| Cirrhosis etiology, No. (%) | ||
| Alcohol | 99 (52.4) | |
| Hepatitis C | 32 (16.9) | |
| Combined causes | 16 (8.5) | |
| Cryptogenic | 14 (7.4) | |
| Autoimmune | 12 (6.4) | |
| Primary biliary cholangitis | 9 (4.8) | |
| Hepatitis B | 6 (3.2) | |
| Drug-induced | 1 (0.5) | |
| Child–Pugh Class, No. (%) | ||
| A | 79 (41.8) | |
| B | 71 (37.6) | |
| C | 31 (16.4) | |
| Unknown | 8 (4.2) | |
| Complications of Liver Cirrhosis | No. (%) | |||
|---|---|---|---|---|
| Ascites | ||||
| Absent/mild | 136 (72) | |||
| Moderate | 22 (11.6) | |||
| Severe | 31 (16.4) | |||
| Hepatic encephalopathy | ||||
| Absent | 158 (82.5) | |||
| Mild/moderate (Stage I–II) | 26 (14.8) | |||
| Severe (Stage III–IV) | 5 (2.7) | |||
| Esophageal varices | ||||
| Yes | 104 (55) | |||
| Grade I | 36 (19.1) | |||
| Grade II | 57 (30.1) | |||
| Grade III | 8 (4.2) | |||
| Unknown | 3 (1.6) | |||
| No | 27 (14.3) | |||
| Gastroscopy not performed | 58 (30.7) | |||
| Renal failure | 29 (15.3) | |||
| Hepatocellular carcinoma | ||||
| No | 177 (93.6) | |||
| Yes | 6 (3.2) | |||
| Possible (uncharacterized nodule) | 6 (3.2) | |||
| Upper gastrointestinal bleeding | 9 (4.8) | |||
| Spontaneous bacterial peritonitis | 1 (0.5) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eftimie Spitz, R.; Popa, S.L.; Grad, S.; Dumitrascu, D.L.; Ismaiel, A.; Surdea-Blaga, T. The Use of Proton Pump Inhibitors in Patients with Liver Cirrhosis: Real Life Experience. J. Clin. Med. 2024, 13, 5155. https://doi.org/10.3390/jcm13175155
Eftimie Spitz R, Popa SL, Grad S, Dumitrascu DL, Ismaiel A, Surdea-Blaga T. The Use of Proton Pump Inhibitors in Patients with Liver Cirrhosis: Real Life Experience. Journal of Clinical Medicine. 2024; 13(17):5155. https://doi.org/10.3390/jcm13175155
Chicago/Turabian StyleEftimie Spitz, Raphaël, Stefan Lucian Popa, Simona Grad, Dan Lucian Dumitrascu, Abdulrahman Ismaiel, and Teodora Surdea-Blaga. 2024. "The Use of Proton Pump Inhibitors in Patients with Liver Cirrhosis: Real Life Experience" Journal of Clinical Medicine 13, no. 17: 5155. https://doi.org/10.3390/jcm13175155
APA StyleEftimie Spitz, R., Popa, S. L., Grad, S., Dumitrascu, D. L., Ismaiel, A., & Surdea-Blaga, T. (2024). The Use of Proton Pump Inhibitors in Patients with Liver Cirrhosis: Real Life Experience. Journal of Clinical Medicine, 13(17), 5155. https://doi.org/10.3390/jcm13175155