
Implementing Oxygen Therapy in Medical Wards—A Scoping Review to Understand Health Services Protocols and Procedures


Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
- Documents included local guidance of policy, procedure, protocol or guideline (or a combination);
- The title contained the term ‘oxygen therapy’ or similar;
- The content concentrated on adult ARF ward-delivered COT implementation.
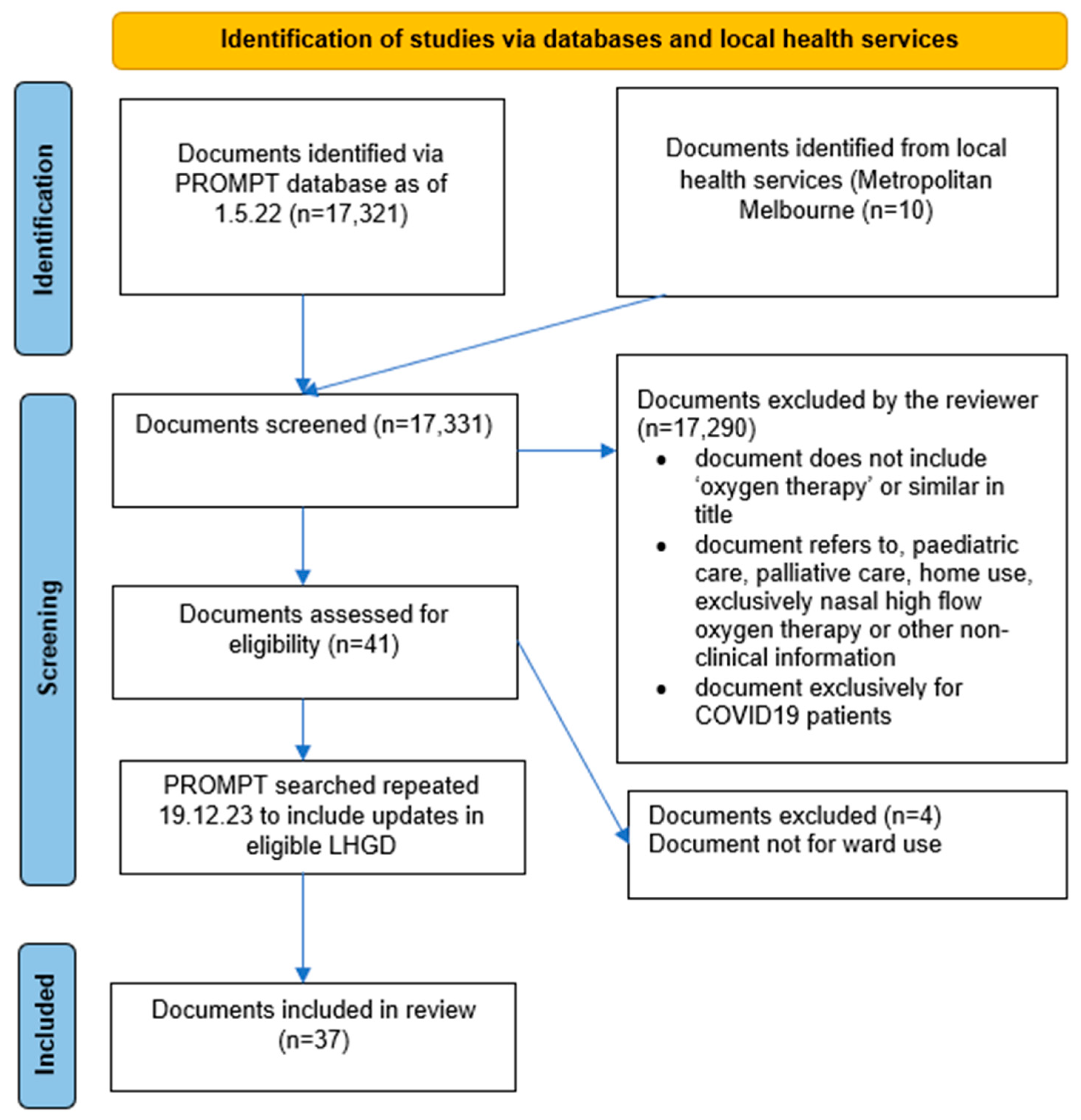
2.2. Screening, Data Extraction, and Analysis
3. Results
3.1. Characteristics of Included Documents
3.2. Indications for COT
3.3. COT Initiation and Maintenance
3.4. Escalation of Care
3.5. Weaning
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, L.; Rackley, C.R. Diagnosis and Epidemiology of Acute Respiratory Failure. Crit. Care Clin. 2024, 40, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.-K.I.; Kamaleswaran, R.; Tabaie, A.; Reyna, M.A.; Josef, C.; Robichaux, C.; de Hond, A.A.H.; Steyerberg, E.W.; Holder, A.L.; Nemati, S.; et al. Prediction of Acute Respiratory Failure Requiring Advanced Respiratory Support in Advance of Interventions and Treatment: A Multivariable Prediction Model From Electronic Medical Record Data. Crit. Care Explor. 2021, 3, e0402. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-C.; Peng, Y.; Dai, B.; Hou, H.-J.; Zhao, H.-W.; Wang, W.; Tan, W. Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: A systematic review and meta-analysis. Ther. Adv. Respir. Dis. 2024, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Riera, J.; Torres, F.; Masclans, J.R. High-flow oxygen therapy in acute respiratory failure. Respir. Care 2010, 55, 408–413. [Google Scholar]
- Batool, S.; Garg, R. Appropriate Use of Oxygen Delivery Devices. Open Anesthesiol. J. 2017, 11, 35–38. [Google Scholar] [CrossRef]
- Gottlieb, J.; Capetian, P.; Hamsen, U.; Janssens, U.; Karagiannidis, C.; Kluge, S.; Nothacker, M.; Roiter, S.; Volk, T.; Worth, H.; et al. German S3 Guideline: Oxygen Therapy in the Acute Care of Adult Patients. Respiration 2022, 101, 214–252. [Google Scholar] [CrossRef]
- Barnett, A.; Beasley, R.; Buchan, C.; Chien, J.; Farah, C.S.; King, G.; McDonald, C.F.; Miller, B.; Munsif, M.; Psirides, A.; et al. Thoracic Society of Australia and New Zealand Position Statement on Acute Oxygen Use in Adults: ‘Swimming between the flags’. Respirology 2022, 27, 262–276. [Google Scholar] [CrossRef]
- O’Driscoll, B.R.; Howard, L.S.; Davison, A.G. BTS guideline for emergency oxygen use in adult patients. Thorax 2008, 63, vi1–vi68. [Google Scholar] [CrossRef]
- O’Driscoll, B.R.; Howard, L.S.; Earis, J.; Mak, V. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax 2017, 72, ii1–ii90. [Google Scholar] [CrossRef]
- Kane, B.; Decalmer, S.; Ronan O’Driscoll, B. Emergency oxygen therapy: From guideline to implementation. Breathe 2013, 9, 246–253. [Google Scholar] [CrossRef]
- Guerra-Farfan, E.; Garcia-Sanchez, Y.; Jornet-Gibert, M.; Nuñez, J.H.; Balaguer-Castro, M.; Madden, K. Clinical practice guidelines: The good, the bad, and the ugly. Injury 2023, 54, S26–S29. [Google Scholar] [CrossRef]
- Pereira, V.C.; Silva, S.N.; Carvalho, V.K.S.; Zanghelini, F.; Barreto, J.O.M. Strategies for the implementation of clinical practice guidelines in public health: An overview of systematic reviews. Health Res. Policy Syst. 2022, 20, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, K.; Levesque, J.F. Unwarranted clinical variation in health care: Definitions and proposal of an analytic framework. J. Eval. Clin. Pract. 2020, 26, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care. The Fourth Australian Atlas of Healthcare Variation; Australian Commission on Safety and Quality in Health Care: Canberra, Australia, 2021.
- NHS Right Care. Reducing unwarranted variation to improve health outcomes and value. In The 2nd Atlas of Variation in Risk Factors and Healthcare for Respiratory Disease in England; Public Health England: London, UK, 2019. Available online: https://fingertips.phe.org.uk/static-reports/atlas-of-variation/2ndRespiratoryAtlas_v1.0_20190923.pdf (accessed on 3 September 2024).
- Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards Guideline for Hospitals. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/National-Safety-and-Quality-Health-Service-Standards-Guide-for-Hospitals.pdf (accessed on 29 June 2024).
- Australian Commission on Safety and Quality in Health Care. Action 1.07: Policies and Procedures. Available online: https://www.safetyandquality.gov.au/standards/nsqhs-standards/clinical-governance-standard/patient-safety-and-quality-systems/action-107#:~:text=Action%201.07%20states,-The%20health%20service&text=Set%20out%2C%20review%2C%20and%20maintain,legislation%2C%20regulation%20and%20jurisdictional%20requirements (accessed on 29 June 2024).
- Beasley, R.; Chien, J.; Douglas, J.; Eastlake, L.; Farah, C.; King, G.; Moore, R.; Pilcher, J.; Richards, M.; Smith, S.; et al. Thoracic Society of Australia and New Zealand oxygen guidelines for acute oxygen use in adults: ‘Swimming between the flags’. Respirology 2015, 20, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- Oczkowski, S.; Ergan, B.; Bos, L.; Chatwin, M.; Ferrer, M.; Gregoretti, C.; Heunks, L.; Frat, J.-P.; Longhini, F.; Nava, S.; et al. ERS clinical practice guidelines: High-flow nasal cannula in acute respiratory failure. Eur. Respir. J. 2022, 59, 2101574. [Google Scholar] [CrossRef]
- Bowton, D.L.; Scuderi, P.E.; Haponik, E.F. The incidence and effect on outcome of hypoxemia in hospitalized medical patients. Am. J. Med. 1994, 97, 38–46. [Google Scholar] [CrossRef]
- Buist, M.; Bernard, S.; Nguyen, T.V.; Moore, G.; Anderson, J. Association between clinically abnormal observations and subsequent in-hospital mortality: A prospective study. Resuscitation 2004, 62, 137–141. [Google Scholar] [CrossRef]
- Siemieniuk, R.A.C.; Chu, D.K.; Kim, L.H.-Y.; Güell-Rous, M.-R.; Alhazzani, W.; Soccal, P.M.; Karanicolas, P.J.; Farhoumand, P.D.; Siemieniuk, J.L.K.; Satia, I.; et al. Oxygen therapy for acutely ill medical patients: A clinical practice guideline. BMJ 2018, 363, k4169. [Google Scholar] [CrossRef]
- Harper, J.C.P.; Semprini, R.; Kearns, N.A.; Hatter, L.; Bird, G.E.; Braithwaite, I.; Eathorne, A.; Weatherall, M.; Beasley, R. Determination of oxygen saturation compared to a prescribed target range using continuous pulse oximetry in acutely unwell medical patients. BMC Pulm. Med. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Chu, D.K.; Kim, L.H.; Young, P.J.; Zamiri, N.; Almenawer, S.A.; Jaeschke, R.; Szczeklik, W.; Schünemann, H.J.; Neary, J.D.; Alhazzani, W. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): A systematic review and meta-analysis. Lancet 2018, 391, 1693–1705. [Google Scholar] [CrossRef]
- Sarkar, M.; Madabhavi, I.; Kadakol, N. Oxygen-induced hypercapnia: Physiological mechanisms and clinical implications. Monaldi Arch. Chest Dis. 2022, 93, 2399. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Datey, N.; Liacos, A.; Joosten, S.A.; Leong, P. Acute oxygen use in hospitalised patients with chronic obstructive pulmonary disease is guideline discordant. Intern. Med. J. 2021, 51, 780–783. [Google Scholar] [CrossRef] [PubMed]
- Kamran, A.; Chia, E.; Tobin, C. Acute oxygen therapy: An audit of prescribing and delivery practices in a tertiary hospital in Perth, Western Australia. Intern. Med. J. 2018, 48, 151–157. [Google Scholar] [CrossRef] [PubMed]
- McDonald, V.; Cousins, J.; Wark, P. Acute oxygen therapy: A review of prescribing and delivery practices. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1067–1075. [Google Scholar] [CrossRef]
- Cousins, J.L.; Wark, P.A.B.; Hiles, S.A.; McDonald, V.M. Understanding Clinicians’ Perceived Barriers and Facilitators to Optimal Use of Acute Oxygen Therapy in Adults. Int. J. Chron. Obs. Pulmon Dis. 2020, 15, 2275–2287. [Google Scholar] [CrossRef]
- Anderson, J.; Hoang, T.; Hay, K.; Tay, G. Evaluation of inpatient oxygen therapy in hypercapnic chronic obstructive pulmonary disease. Intern. Med. J. 2021, 51, 654–659. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. NIMC User Guide. National In-patient Medication Chart. Available online: https://www.safetyandquality.gov.au/ (accessed on 3 September 2024).
- Lee, C.C.; Mankodi, D.; Shaharyar, S.; Ravindranathan, S.; Danckers, M.; Herscovici, P.; Moor, M.; Ferrer, G. High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: A systematic review. Respir. Med. 2016, 121, 100–108. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Einav, S.; Pearse, R.; Jaber, S.; Kranke, P.; Overdyk, F.J.; Whitaker, D.K.; Gordo, F.; Dahan, A.; Hoeft, A. Improving detection of patient deterioration in the general hospital ward environment. Eur. J. Anaesthesiol. 2018, 35, 325–333. [Google Scholar] [CrossRef]
- Palmer, J.H.; James, S.; Wadsworth, D.; Gordon, C.J.; Craft, J. How registered nurses are measuring respiratory rates in adult acute care health settings: An integrative review. J. Clin. Nurs. 2023, 32, 4515–4527. [Google Scholar] [CrossRef]
- Churpek, M.M.; Adhikari, R.; Edelson, D.P. The value of vital sign trends for detecting clinical deterioration on the wards. Resuscitation 2016, 102, 1–5. [Google Scholar] [CrossRef]
- Le Lagadec, M.D.; Dwyer, T.; Browne, M. The efficacy of twelve early warning systems for potential use in regional medical facilities in Queensland, Australia. Aust. Crit. Care 2020, 33, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Jones, D. The medical emergency team—Current status and future directions: A perspective for acute care physicians. Intern. Med. J. 2023, 53, 888–891. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, L.T.; Grion, C.M.; Matsuo, T.; Anami, E.H.; Kauss, I.A.; Seko, L.; Bonametti, A.M. Impact of delayed admission to intensive care units on mortality of critically ill patients: A cohort study. Crit. Care 2011, 15, R28. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Coello, P.; Martínez García, L.; Carrasco, J.M.; Solà, I.; Qureshi, S.; Burgers, J.S. The updating of clinical practice guidelines: Insights from an international survey. Implement. Sci. 2011, 6, 107. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, B.R.; Howard, L.S.; Bucknall, C.; Welham, S.A.; Davison, A.G. British Thoracic Society emergency oxygen audits. Thorax 2011, 66, 734–735. [Google Scholar] [CrossRef]
- O’Driscoll, R.; Bakerly, N.D. Automated audit of hospital oxygen use devised during the COVID-19 pandemic. BMJ Open Respir. Res. 2023, 10, e001866. [Google Scholar] [CrossRef]
- Foley, C. A Study of the Relationship bewteen Hospital Policy and Nursing Practice. Ph.D. Thesis, University of Tasmania, Hobart, Australia, 2020. [Google Scholar]
- Talat, U.; Schmidtke, K.A.; Khanal, S.; Turner, A.M.; Vlaev, I. Can guidelines rein in oxygen use? A retrospective cross-sectional study using routinely collected data. Int. J. Qual. Health Care 2023, 35, 1–7. [Google Scholar] [CrossRef]
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N. Tailored interventions to overcome identified barriers to change: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2010, 3, 1–86. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National, State and Territory Population, December 2023. Available online: https://population.gov.au/data-and-forecasts/key-data-releases/national-state-and-territory-population-december-2023 (accessed on 29 June 2024).

{kind=link}
| Count (n) | Frequency (%) | |
|---|---|---|
| Indications for COT * | ||
| -Hypoxemia | 37 | 100 |
| -Hypercapnic respiratory failure | 31 | 87.8 |
| -Cyanosis | 11 | 29.7 |
| -Respiratory distress | 10 | 27.0 |
| -Chest pain | 4 | 10.8 |
| -Cardiac arrest | 4 | 10.8 |
| -Trauma | 4 | 10.8 |
| -Haemorrhage and shock | 4 | 10.8 |
| -Sepsis | 3 | 8.1 |
| -Seizure | 3 | 8.1 |
| -Carbon monoxide poisoning | 2 | 5.4 |
| -Stroke and SpO2 < 95% | 2 | 5.4 |
| -Post-operative | 1 | 2.7 |
| SpO2 hypoxemia definition to trigger COT consideration | ||
| -<92% | 22 | 59.5 |
| -<94% | 9 | 24.3 |
| -Definition not specified | 6 | 16.2 |
| -<88% ⱡ | 0 | 0 |
| PaO2 (ABG) hypoxemia definition to trigger COT | ||
| -Definition not specified | 23 | 62.2 |
| -<80 mmHg | 14 | 37.8 |
| Hypoxemia assessed with * | ||
| -Pulse oximetry | 23 | 62.2 |
| -Arterial blood gas | 13 | 35.1 |
| -Not specified | 2 | 5.4 |
| Indications for performing an ABG | ||
| -Not stated | 20 | 54.1 |
| -Hypoxaemia | 13 | 35.1 |
| -Risk of hypercapnia | 10 | 27.0 |
| -Reliable SpO2 not obtainable | 5 | 13.5 |
| SpO2 targets (lowest range level) once COT initiated | ||
| -Not specified | 8 | 21.6 |
| -92%+ | 22 | 59.5 |
| -94%+ | 7 | 18.9 |
| SpO2 targets (highest range level) once COT initiated | ||
| -Not specified | 19 | 51.4 |
| -96%+ | 11 | 29.7 |
| -98%+ | 7 | 18.9 |
| At Initiation—COT | Post-Initiation—COT | |||
|---|---|---|---|---|
| Count (n) | Frequency (%) | Count (n) | Frequency (%) | |
| ABG required | 0 | 0 | 3 | 8.1 |
| VBG used to assess need for COT | 0 | 0 | 1 | 2.7 |
| SpO2 target range | 29 | 78.4 | 29 | 78.4 |
| Additional SpO2 target range specified for patients identified as vulnerable to hypercapnic respiratory failure | 25 | 67.6 | 25 | 67.6 |
| COT device rate * | N/A | N/A | ||
| -Not specified | 4 | 10.8 | ||
| -1–2 LPM | 33 | 89.2 | ||
| -2–4 LPM | 33 | 89.2 | ||
| ->5 LPM | 33 | 89.2 | ||
| Mode of delivery COT | N/A | N/A | ||
| -Not specified | ||||
| -Nasal cannulae | 34 | 91.9 | ||
| -Face mask | 34 | 91.9 | ||
| -Non-rebreather mask | 26 | 70.3 | ||
| -HFNO | 18 | 48.6 | ||
| -Venturi device | 13 | 35.1 | ||
| -Oximiser (oxygen reservoir) | 2 | 5.4 | ||
| Documentation of COT settings * | N/A | N/A | ||
| -Target SpO2 range | 25 | 67.5 | ||
| -Device flow rate | 22 | 59.4 | ||
| -Delivery system | 21 | 56.7 | ||
| -Frequency of observations | 15 | 40.5 | ||
| Documentation of patient observations * | N/A | N/A | ||
| 0 | 36 | 97.3 | ||
| -Respiratory rate | 21 | 56.7 | ||
| -‘Vital signs’ stated in the LHGD | 13 | 35.1 | ||
| -Heart rate | 12 | 32.4 | ||
| -Blood pressure | 11 | 29.7 | ||
| -Temperature | 6 | 16.2 | ||
| Time until first observations | N/A | N/A | ||
| -Clinical discretion | 26 | 70.3 | ||
| -Not specified | 9 | 24.3 | ||
| -0–1 h | 1 | 2.7 | ||
| -2–4 h | 0 | 0 | ||
| Observation frequency | N/A | N/A | ||
| -Clinical discretion | 27 | 73.0 | ||
| -0–1 h | 3 | 8.1 | ||
| -2–4 h | 2 | 5.4 | ||
| -4+ h | 5 | 13.5 | ||
| Flow diagram provided for COT initiation | 8 | 21.6 | N/A | N/A |
| Characteristic | Count (n) | Frequency (%) |
|---|---|---|
| Maintain target SpO2 range when weaning | ||
| Not specified | 28 | 75.7 |
| ->92% | 9 | 24.3 |
| Patient observations to be documented * | ||
| -Not specified | 26 | 70.3 |
| 0 | 8 | 21.6 |
| -Respiratory rate | 4 | 10.8 |
| -Heart rate | 4 | 10.8 |
| -‘Vital signs’ | 2 | 5.4 |
| Flow rate targets before COT cessation ** | ||
| -Not specified | 34 | 91.9 |
| -1–4 LPM | 3 | 8.1 |
| Device to use prior to COT cessation ** | ||
| -Not specified | 29 | 78.4 |
| -Face mask and/or nasal cannulae | 8 | 21.6 |
| Document purpose | To provide essential clinical guidance for ward-delivered implementation of COT (including core information for initiation, monitoring, escalation, and weaning) for ARF in adults |
| Target audience | Clinical staff that are educated in adult COT implementation, including doctors, nurses, and physiotherapists |
| Definitions | Hypoxaemia, as defined by ABG or SpO2 values, requires COT ABG PaO2 < 60 mmHg or SpO2 < 92% * * Target SpO2 may vary and is based on assessment and clinical judgement on individual patient circumstances such as hypercapnia, i.e., SpO2 < 88% |
| Indications | COT is the first strategy for patients with hypoxaemic ARF
Prior to COT initiation, consideration and discussion with patients and carers of treatment preferences, including the goals of care, are essential and must be documented for all patients * Consideration for HFNO where local resources permit |
| Contraindications | Normoxia associated with dysfunctional breathing (i.e., breathlessness) Active reoccurring nasal bleeding Surgical procedures—nasal and sinus (i.e., recent) Trauma—maxillofacial (i.e., recent) Fractures—base of skull (including suspected) |
| Prescription | COT prescription chart * Preference integrated into the electronic medical record Target SpO2 range
Monitoring and maintenance (e.g., titration and weaning) of treatment aims |
| COT devices’ characteristics | Low-flow nasal cannulae
Simple mask
Non-rebreather mask
Venturi mask
Consider humidification if flows above 2–4 litres per minute used for more than 24 h as medical oxygen has a drying effect on mucous membranes * Recommend including device pictures and instructional videos |
| Initiation | ABG measurement should be considered clinically indicated, particularly in patients suspected of hypercapnia, as there are considerable limitations with SpO2 and venous blood gases COT equipment preparation methods for initiation (local service to add detailed step-by-step information and pictures) COT device titration parameters (i.e., flow litres) to maintain specified target SpO2 range:
* Consider known disorders that have an increased susceptibility to hypercapnic respiratory failure. Examples include but are not limited to severe kyphoscoliosis, severe chronic obstructive pulmonary disease, obesity hypoventilation syndrome, neuromuscular disorders and respiratory muscle weakness, or patients with a known previous episode of hypercapnia (i.e., acute or chronic) The clinical monitoring required, including the frequency needed, is based on individual patient assessment within the therapy targets. Documentation of the COT therapy response should include the following essential clinical physiological parameters -Respiratory and heart rate, oxygen saturation, and temperature Initiation assessment and monitoring to be conducted every 15 min in the first 60 min of therapy. This recommendation may be influenced by local service resources, including nurse-to-patient ratios, acuity of the patient, goals of care, and the clinical indication Assessment and maintenance to include COT device used, the titration (upwards or downwards) of the device flow rate (litres per minute) in order to achieve the target SpO2 ranges (as stated above) |
| Maintenance | Physiological parameter observation intervals will vary based on individual patient clinical requirements. As the patient improves and stabilises, the frequency of observations will lessen * (i.e., from 1 to 4 h) * Based on local service resources (as above) The change in observation frequency is to be documented alongside the essential clinical physiological parameters of the respiratory and heart rate, oxygen saturation and temperature, and the COT device used to include the device flow rate (litres per minute) in order to achieve the target SpO2 ranges (as stated above) Clinical consideration for an ABG should be based on the individual patient assessment, including the frequency required |
| Criteria for medical review | Physiological parameters changes, including increased
Increased oxygen flow to meet the SpO2 target range Maximal oxygen flow to meet the SpO2 target range Unable to meet the SpO2 target range Clinical uncertainty using COT Other: As directed by local service early warning system [add local hospital alert system] |
| Escalation pathway | Clinical deterioration may occur in adults with ARF using ward-delivered COT. As such, they required ongoing regular assessment and monitoring Local service early warning scores should be used to assist clinical decisions for deteriorating patients and to escalate care [Add in the local service clinical tool], i.e., modified early warning score (medical emergency team), including the referral mechanism to ICU (include how to contact the ICU junior and senior doctors, e.g., pager number) [Add in the local work instruction] local ward upper limits for ward-delivered COT, i.e., device flow or level of oxygen delivered |
| Weaning | Weaning is essential strategy to assess response to therapy When weaning, decrease the oxygen flow rate to maintain the SpO2 target range, e.g., flow of <1–2 litres per minute Perform a room air assessment when clinically indicated, including assessment of desaturation (SpO2) episode (i.e., the time to desaturate), including the documentation of the essential physiological parameters of the respiratory and heart rate, oxygen saturation, and temperature If patient is a known long-term COT user, consideration for ongoing COT requirement, i.e., do not wean and cease COT to room air. Provide a new revised COT prescription for rest, activity, and sleep as indicated Referral pathway for known or suspected long-term COT use (include contact method, e.g., respiratory registrar pager) On cessation of COT, transition the patient to room air. Individual patient assessment and monitoring is required. Recommend lessening the frequency of essential physiological parameters of the respiratory and heart rate, oxygen saturation, and temperature to four to six hourly (or as indicated) |
| COT ward-delivered palliation | Clinical discretion is required for COT utilisation to manage non-hypoxaemic dyspnoea at the very end of life in some patients. Patient preference should be considered (see above). COT is usually well tolerated as the patients can communicate while using most COT devices Monitoring and escalation criteria are not routinely used for COT users at the end of life. COT used in this setting is to provide symptom support. COT adjustment or cessation should be considered when the patient is comfortable |
| Associated documents | e.g., HFNO LHGD, NIV LHGD, escalation of care LHGD, COT manufacturer instructions |
| References | e.g., TSANZ Acute Oxygen Position Statement [7], BTS Guideline for oxygen [9], ERS HFNO clinical practice guidelines [19] |
| Authors and review | Clinical staff positions and professional groups Review date Planned next review date Planned monitoring aligned to updated national and international guidelines |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchan, C.; Khor, Y.H.; Thomas, T.; Smallwood, N. Implementing Oxygen Therapy in Medical Wards—A Scoping Review to Understand Health Services Protocols and Procedures. J. Clin. Med. 2024, 13, 5506. https://doi.org/10.3390/jcm13185506
Buchan C, Khor YH, Thomas T, Smallwood N. Implementing Oxygen Therapy in Medical Wards—A Scoping Review to Understand Health Services Protocols and Procedures. Journal of Clinical Medicine. 2024; 13(18):5506. https://doi.org/10.3390/jcm13185506
Chicago/Turabian StyleBuchan, Catherine, Yet Hong Khor, Toby Thomas, and Natasha Smallwood. 2024. "Implementing Oxygen Therapy in Medical Wards—A Scoping Review to Understand Health Services Protocols and Procedures" Journal of Clinical Medicine 13, no. 18: 5506. https://doi.org/10.3390/jcm13185506
APA StyleBuchan, C., Khor, Y. H., Thomas, T., & Smallwood, N. (2024). Implementing Oxygen Therapy in Medical Wards—A Scoping Review to Understand Health Services Protocols and Procedures. Journal of Clinical Medicine, 13(18), 5506. https://doi.org/10.3390/jcm13185506