
Condylar Remodeling and Skeletal Changes Following Occlusal Splint and Manual Therapy: A Cone Beam Computed Tomography Study in Temporomandibular Disorders

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Inclusion Criteria
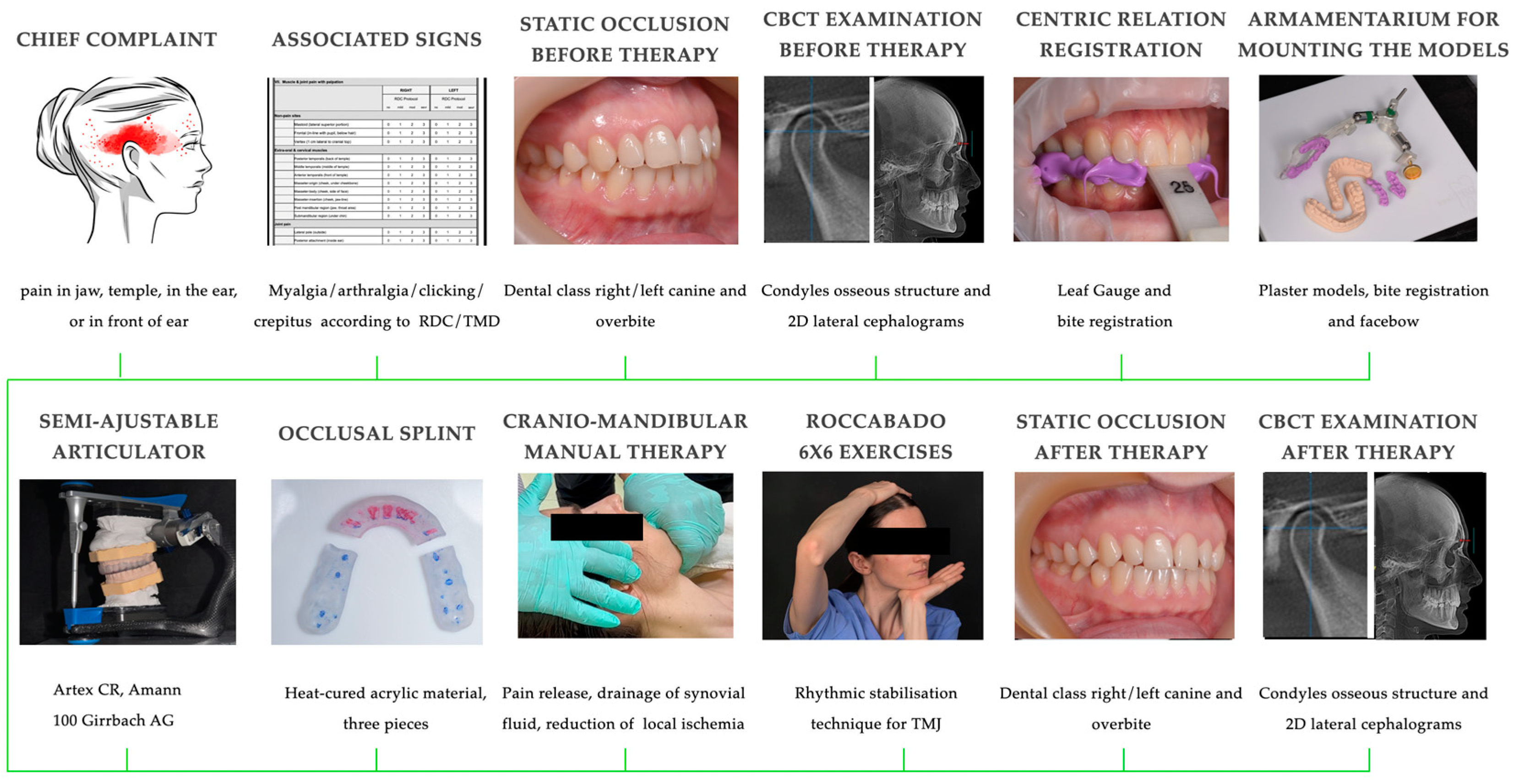
2.2. Clinical and Paraclinical Interventions
2.3. Outcomes Assessed
2.3.1. CBCT Analysis
Osseous Condylar Structure
Cephalometric Parameters
2.3.2. Static Occlusion Parameters
2.4. Statistical Analysis
3. Results
3.1. Condylar Remodeling
3.2. Vertical and Sagittal Skeletal Changes
3.3. Vertical and Sagittal Occlusion Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMD | Temporomandibular disorders |
| TMJ | Temporomandibular joint |
| CBCT | Cone beam computed tomography |
| SNA | Sella-Nasion-A point |
| SNB | Sella-Nasion-B point |
| ANB | A point-Nasion-B point |
| AFH | Anterior facial height |
| PFH | Posterior facial height |
| DC/TMD | Diagnostic Criteria for Temporomandibular Disorders |
| 2D | Two-dimensional |
| CT | Computed tomography |
| CI | Confidence interval |
| CR | Centric relation |
| RDC/TMD | Research Diagnostic Criteria for Temporomandibular Disorders |
| 3D | Tridimensional |
| ALARA | As Low As Reasonably Achievable |
| S | Sella |
| N | Nasion |
| Me | Menton |
| Go | Gonion |
| Ar | Articulare |
| ICC | Intra-observer correlation coefficient |
| 1 | Class I |
| D ½ c | Class II with one-half cusp distalization |
| D 1 c | Class II with one cusp distalization |
| M ½ c | Class III with one-half cusp mesialization |
| M 1 c | Class III with one cusp mesialization |
| NOB | Normal overbite |
| DB | Deep bite |
| OB | Open bite |
References
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Yasan, G.T.; Adiloglu, S.; Tuz, H.H.; Sahar, D. Evaluation of clinical signs and magnetic resonance imaging findings in patients with temporomandibular disorders. J. Craniomaxillofac. Surg. 2023, 51, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Alrizqi, A.H.; Aleissa, B.M. Prevalence of Temporomandibular Disorders Between 2015–2021: A Literature Review. Cureus 2023, 15, e37028. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.C.; Yap, A.U.; Türp, J.C. Prevalence of temporomandibular disorders in patients seeking orthodontic treatment: A systematic review. J. Oral Rehabil. 2020, 47, 270–280. [Google Scholar] [CrossRef]
- Romero-Reyes, M.; Bassiur, J.P. Temporomandibular Disorders, Bruxism and Headaches. Neurol. Clin. 2024, 42, 573–584. [Google Scholar] [CrossRef]
- Tanaka, E.; Detamore, M.S.; Mercuri, L.G. Degenerative disorders of the temporomandibular joint: Etiology, diagnosis, and treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef]
- Derwich, M.; Mitus-Kenig, M.; Pawlowska, E. Interdisciplinary Approach to the Temporomandibular Joint Osteoarthritis-Review of the Literature. Medicina 2020, 56, 225. [Google Scholar] [CrossRef]
- Wahaj, A.; Hafeez, K.; Zafar, M.S. Association of bone marrow edema with temporomandibular joint (TMJ) osteoarthritis and internal derangements. Cranio 2017, 35, 4–9. [Google Scholar] [CrossRef]
- Toshima, H.; Ogura, I. Characteristics of patients with temporomandibular joint osteoarthrosis on magnetic resonance imaging. J. Med. Imaging Radiat. Oncol. 2020, 64, 615–619. [Google Scholar] [CrossRef]
- Li, C.; Zhang, Q. Comparison of imaging findings of 714 symptomatic and asymptomatic temporomandibular joints: A retrospective study. BMC Oral Health 2023, 23, 79. [Google Scholar] [CrossRef]
- Seo, Y.J.; Park, S.B.; Kim, Y.I.; Ok, S.M.; Kim, S.S.; Son, W.S. Effects of condylar head surface changes on mandibular position in patients with temporomandibular joint osteoarthritis. J. Craniomaxillofac. Surg. 2015, 43, 1380–1383. [Google Scholar] [CrossRef] [PubMed]
- Min, C.K.; Kim, K.A.; Lee, K.E.; Suh, B.J.; Jung, W. A study on volumetric change of mandibular condyles with osteoarthritis using cone-beam computed tomography. Sci. Rep. 2024, 14, 10232. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Lee, J.Y.; Huh, K.H.; Park, J.W. Long-term Changes of Temporomandibular Joint Osteoarthritis on Computed Tomography. Sci. Rep. 2020, 10, 6731. [Google Scholar] [CrossRef]
- Lei, J.; Liu, M.Q.; Yap, A.U.; Fu, K.Y. Condylar subchondral formation of cortical bone in adolescents and young adults. Br. J. Oral Maxillofac. Surg. 2013, 51, 63–68. [Google Scholar] [CrossRef]
- Mélou, C.; Pellen-Mussi, P.; Jeanne, S.; Novella, A.; Tricot-Doleux, S.; Chauvel-Lebret, D. Osteoarthritis of the Temporomandibular Joint: A Narrative Overview. Medicina 2022, 59, 8. [Google Scholar] [CrossRef]
- Musa, M.; Zhang, Q.; Awad, R.; Wang, W.; Ahmed, M.M.S.; Zhao, Y.; Almashraqi, A.A.; Chen, X.; Alhammadi, M.S. Quantitative and qualitative condylar changes following stabilization splint therapy in patients with temporomandibular joint disorders. Clin. Oral Investig. 2023, 27, 2299–2310. [Google Scholar] [CrossRef]
- Yap, A.U.; Lei, J.; Zhang, X.H.; Fu, K.Y. TMJ degenerative joint disease: Relationships between CBCT findings, clinical symptoms, and signs. Acta Odontol. Scand. 2023, 81, 562–568. [Google Scholar] [CrossRef]
- Reia, V.C.B.; de Toledo Telles-Araujo, G.; Peralta-Mamani, M.; Biancardi, M.R.; Rubira, C.M.F.; Rubira-Bullen, I.R.F. Diagnostic accuracy of CBCT compared to panoramic radiography in predicting IAN exposure: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 4721–4733. [Google Scholar] [CrossRef]
- Raj, G.; Raj, M.; Saigo, L. Accuracy of conventional versus cone-beam CT-synthesised lateral cephalograms for cephalometric analysis: A systematic review. J. Orthod. 2024, 51, 160–176. [Google Scholar] [CrossRef]
- Ahmad, M.; Hollender, L.; Anderson, Q.; Kartha, K.; Ohrbach, R.; Truelove, E.L.; John, M.T.; Schiffman, E.L. Research diagnostic criteria for temporomandibular disorders (RDC/TMD): Development of image analysis criteria and examiner reliability for image analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 844–860. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Farea, R.; Qasem, K.A.; Al-Wadeai, M.S.; Al-Sabahi, M.E.; Al-Iryani, G.M. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: Network meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2020, 49, 1042–1056. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.L.; Velly, A.M.; Look, J.O.; Hodges, J.S.; Swift, J.Q.; Decker, K.L.; Anderson, Q.N.; Templeton, R.B.; Lenton, P.A.; Kang, W.; et al. Effects of four treatment strategies for temporomandibular joint closed lock. Int. J. Oral Maxillofac. Surg. 2014, 43, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Qvintus, V.; Suominen, A.L.; Huttunen, J.; Raustia, A.; Ylöstalo, P.; Sipilä, K. Efficacy of stabilisation splint treatment on facial pain—1-year follow-up. J. Oral Rehabil. 2015, 42, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Brantingham, J.W.; Cassa, T.K.; Bonnefin, D.; Pribicevic, M.; Robb, A.; Pollard, H.; Tong, V.; Korporaal, C. Manipulative and multimodal therapy for upper extremity and temporomandibular disorders: A systematic review. J. Manip. Physiol. Ther. 2013, 36, 143–201. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Pitance, L.; Singh, V.; Neto, F.; Thie, N.; Michelotti, A. Effectiveness of Manual Therapy and Therapeutic Exercise for Temporomandibular Disorders: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 9–25. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, L.; Wu, D.; Yu, C.; Fan, S.; Cai, B. Effectiveness of exercise therapy versus occlusal splint therapy for the treatment of painful temporomandibular disorders: A systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 6122–6132. [Google Scholar] [CrossRef]
- Murtza, S.; Noor, R.; Bashir, M.S.; Ikram, M. Effects of sustained natural apophyseal glides versus rocabado 6 × 6 program in subjects with cervicogenic headache. BMC Musculoskelet. Disord. 2024, 25, 169. [Google Scholar] [CrossRef]
- Albagieh, H.; Alomran, I.; Binakresh, A.; Alhatarisha, N.; Almeteb, M.; Khalaf, Y.; Alqublan, A.; Alqahatany, M. Occlusal splints-types and effectiveness in temporomandibular disorder management. Saudi Dent. J. 2023, 35, 70–79. [Google Scholar] [CrossRef]
- Kuzmanovic Pficer, J.; Dodic, S.; Lazic, V.; Trajkovic, G.; Milic, N.; Milicic, B. Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects. PLoS ONE. 2017, 12, e0171296. [Google Scholar] [CrossRef]
- Greene, C.S.; Menchel, H.F. The Use of Oral Appliances in the Management of Temporomandibular Disorders. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 265–277. [Google Scholar] [CrossRef]
- Ok, S.M.; Lee, J.; Kim, Y.I.; Lee, J.Y.; Kim, K.B.; Jeong, S.H. Anterior condylar remodeling observed in stabilization splint therapy for temporomandibular joint osteoarthritis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.Q.; Chen, H.M.; Yap, A.U.; Fu, K.Y. Condylar remodeling accompanying splint therapy: A cone-beam computerized tomography study of patients with temporomandibular joint disk displacement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.N.; Cui, S.J.; Zhou, Y.H.; Wang, X.D. An Overview of Anterior Repositioning Splint Therapy for Disc Displacement-related Temporomandibular Disorders. Curr. Med. Sci. 2021, 41, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Oppitz, L.R.; Arantes, A.C.M.; Garanhani, R.R.; Costa, C.A.; Araujo, C.M.; Tanaka, O.M.; Andreis, P.K.D.S.; Schappo, C.; Ignácio, S.A.; Johann, A.C.B.R.; et al. Efficiency of mixed and rigid occlusal stabilization splints: Randomized clinical trial. Braz. Oral Res. 2024, 38, e017. [Google Scholar] [CrossRef] [PubMed]
- The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [CrossRef]
- Dawson, P.E. Optimum TMJ condyle position in clinical practice. Int. J. Periodontics Restor. Dent. 1985, 5, 10–31. [Google Scholar] [PubMed]
- Ok, S.M.; Jeong, S.H.; Ahn, Y.W.; Kim, Y.I. Effect of stabilization splint therapy on glenoid fossa remodeling in temporomandibular joint osteoarthritis. J. Prosthodont. Res. 2016, 60, 301–307. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, D.J.; Lee, S.G.; Chung, J.W. A longitudinal study on the osteoarthritic change of the temporomandibular joint based on 1-year follow-up computed tomography. J. Craniomaxillofac. Surg. 2012, 40, e223–e228. [Google Scholar] [CrossRef]
- Al-Hadad, S.A.; Ahmed, M.M.S.; Zhao, Y.; Wang, L.; Hu, W.; Li, C.; Chen, X.; Alhammadi, M.S. Skeletal, dentoalveolar and soft tissue changes after stabilization splint treatment for patients with temporomandibular joint disorders. BMC Oral Health 2024, 24, 479. [Google Scholar] [CrossRef]
- Ahmed, M.M.S.; Shi, D.; Al-Somairi, M.A.A.; Alhashimi, N.; Almashraqi, A.A.; Musa, M.; Li, N.; Chen, X.; Alhammadi, M.S. Three dimensional evaluation of the skeletal and temporomandibular joint changes following stabilization splint therapy in patients with temporomandibular joint disorders and mandibular deviation: A retrospective study. BMC Oral Health 2023, 23, 18. [Google Scholar] [CrossRef]
- Lei, J.; Yap, A.U.; Liu, M.Q.; Fu, K.Y. Condylar repair and regeneration in adolescents/young adults with early-stage degenerative temporomandibular joint disease: A randomised controlled study. J. Oral Rehabil. 2019, 46, 704–714. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J., Jr. Occlusion. In Principles and Treatment; Quintessence Publ Co., Inc.: Chicago, IL, USA; Gerlin, Germany; Tokyo, Japan; London, UK; Paris, France; Milan, Italy; Barcelona, Spain; Istanbul, Turkey; Sao Paulo, Brazil; Mumbai, India; Moscow, Russia; Praque, Czech Republic; Warsaw, Poland, 2007; pp. 100–114. [Google Scholar]
- Kattadiyil, M.T.; Alzaid, A.A.; Campbell, S.D. What Materials and Reproducible Techniques May Be Used in Recording Centric Relation? Best Evidence Consensus Statement. J. Prosthodont. 2021, 30, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Wiens, J.P. A progressive approach for the use of occlusal devices in the management of temporomandibular disorders. Gen. Dent. 2016, 64, 29–36. [Google Scholar] [PubMed]
- Zonnenberg, A.J.; Mulder, J. The efficacy of a specific stabilization splint. Cranio 2014, 32, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Kalamir, A.; Graham, P.L.; Vitiello, A.L.; Bonello, R.; Pollard, H. Intra-oral myofascial therapy versus education and self-care in the treatment of chronic, myogenous temporomandibular disorder: A randomised, clinical trial. Chiropr. Man. Therap. 2013, 21, 17. [Google Scholar] [CrossRef]
- Kalamir, A.; Bonello, R.; Graham, P.; Vitiello, A.L.; Pollard, H. Intraoral myofascial therapy for chronic myogenous temporomandibular disorder: A randomized controlled trial. J. Manip. Physiol. Ther. 2012, 35, 26–37. [Google Scholar] [CrossRef]
- Mulet, M.; Decker, K.L.; Look, J.O.; Lenton, P.A.; Schiffman, E.L. A randomized clinical trial assessing the efficacy of adding 6 × 6 exercises to self-care for the treatment of masticatory myofascial pain. J. Orofac. Pain. 2007, 21, 318–328. [Google Scholar] [PubMed]
- Cevidanes, L.; Oliveira, A.E.; Motta, A.; Phillips, C.; Burke, B.; Tyndall, D. Head orientation in CBCT-generated cephalograms. Angle Orthod. 2009, 79, 971–977. [Google Scholar] [CrossRef]
- Steiner, C.C. Cephalometrics in clinical practice. Angle Orthod. 1959, 29, 8–29. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing (2013). Available online: https://cir.nii.ac.jp/crid/1370298755636824325 (accessed on 1 February 2024).
- Rosenthal, R. Parametric measures of effect size. In The Handbook of Research Synthesis; Cooper, H., Hedges, L.V., Eds.; Russell Sage Foundation: New York, NY, USA, 1994; pp. 231–244. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Brady, K.; Dickinson, S.C.; Hollander, A.P. Changes in Chondrogenic Progenitor Populations Associated with Aging and Osteoarthritis. Cartilage 2015, 6 (Suppl. 2), 5S–30S. [Google Scholar] [CrossRef]
- Wang, X.D.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current understanding of pathogenesis and treatment of TMJ osteoarthritis. J. Dent. Res. 2015, 94, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Kameoka, S.; Amemiya, T.; Yamada, H.; Araki, M.; Iwai, K.; Hashimoto, K.; Honda, K. Discrepancy of coronal morphology between mandibular condyle and fossa is related to pathogenesis of anterior disk displacement of the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Kim, Y.J.; Song, Y.H.; Tae, I.; Lim, H.K.; Jung, S.K. Assessment of Morphologic Change of Mandibular Condyle in Temporomandibular Joint Osteoarthritis Patients with Stabilization Splint Therapy: A Pilot Study. Healthcare 2022, 10, 1939. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Wojczyńska, A.; Lee, J.Y. The incidence of osteoarthritic change on computed tomography of Korean temporomandibular disorder patients diagnosed by RDC/TMD; a retrospective study. Acta Odontol. Scand. 2016, 74, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Derwich, M.; Gottesman, L.; Urbanska, K.; Pawlowska, E. Craniovertebral and Craniomandibular Changes in Patients with Temporomandibular Joint Disorders after Physiotherapy Combined with Occlusal Splint Therapy: A Prospective Case Control Study. Medicina 2022, 58, 684. [Google Scholar] [CrossRef]
- Ishaq, R.A.R.; AlHammadi, M.S.; Fayed, M.M. Fixed functional appliances with multibracket appliances have no skeletal effect on the mandible: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 612–624. [Google Scholar] [CrossRef]
- Rajbhoj, A.A.; Parchake, P.; Begnoni, G.; Willems, G.; Cadenas de Llano-Pérula, M. Dental changes in humans with untreated normal occlusion throughout lifetime: A systematic scoping review. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 340–362.e3. [Google Scholar] [CrossRef]
- Oh, J.W.; Ahn, Y.W.; Jeong, S.H.; Ju, H.M.; Song, B.S.; Ok, S.M. Prediction of anterior open-bite development after stabilization splint treatment in patients with temporomandibular disorder. Cranio 2022, 40, 324–333. [Google Scholar] [CrossRef]
- Hsu, L.F.; Liu, Y.J.; Wang, S.H.; Chen, Y.J.; Chen, Y.J.; Yao, C.J. Orthodontic correction of acquired open bite with TMJ degeneration: A retrospective study of outcomes and stability. J. Formos. Med. Assoc. 2024, 123, 452–460. [Google Scholar] [CrossRef]
- Ramachandran, A.; Jose, R.; Tunkiwala, A.; Varma, R.B.; MShanmugham, A.; Nair, P.K.; Kumar, K.S.; Sam, L.M. Effect of deprogramming splint and occlusal equilibration on condylar position of TMD patients—A CBCT assessment. Cranio 2021, 39, 294–302. [Google Scholar] [CrossRef]
- Derwich, M.; Pawlowska, E. Do the Mandibular Condyles Change Their Positions within Glenoid Fossae after Occlusal Splint Therapy Combined with Physiotherapy in Patients Diagnosed with Temporomandibular Joint Disorders? A Prospective Case Control Study. J. Pers. Med. 2022, 12, 254. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Conti, P.C.R.; Alyahya, A.; Alkebsi, K.; Elsharkawy, A.; Christidis, N. The hierarchy of different treatments for myogenous temporomandibular disorders: A systematic review and network meta-analysis of randomized clinical trials. Oral Maxillofac. Surg. 2022, 26, 519–533. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Pain in jaw, temple, in ear, or in front of ear | History of head or neck trauma |
| Associated pain-related signs according to RDC/TMD guidelines (arthralgia and myalgia) | Previous orthodontic or orthognathic treatment |
| Associated intra-articular signs according to RDC/TMD guidelines (clicking/popping/crepitus) | Presence of systematic diseases (e.g., autoimmune diseases, rheumatoid arthritis) |
| Older than 18 years old | Younger than 18 years old |
| Three or more stable pairs of opposing teeth in central incisors, premolars, and molars on both left and right side | Less than three stable pairs of opposing teeth in central incisors, premolars, and molars on both left and right side |
| Osseous Structure | Definition |
|---|---|
| Normal | No morphological changes: convex condylar shape, uninterrupted cortical bone, or no cavity in bone marrow |
| Flattening | Loss of condyle’s anterior region convex form |
| Erosion | Loss of continuity in the cortical bone |
| Subchondral cyst | Typical pattern of cavities in bone marrow |
| Position of the Mandible | Point/Angle | Definition |
|---|---|---|
| Point A | Subspinale—point localized in the deepest area of the anterior outline of the maxilla, below the anterior nasal spine | |
| Point B | Supramentale—point localized in the deepest area of the anterior outline of the mandible, above the pogonion | |
| Point S | Sella—geometrical center of Sella turcica | |
| Point N | Nasion—the most anterior point localized in the frontonasal suture | |
| Me | Menton—lowest point on the mandibular symphysis | |
| Go | Gonion—most posterior inferior point on angle of mandible | |
| Ar | Articulare—junction between inferior surface of the cranial base and the posterior border of the ascending rami of the mandible | |
| sagittal position of the mandible | SNA (°) | Sella–Nasion–A point |
| SNB (°) | Sella–Nasion–B point | |
| ANB (°) | A point–Nasion–B point | |
| vertical position of the mandible | AFH (mm) | N–Me |
| PFH (mm) | S–Go | |
| PFH/AFH (%) | PFH/AFH x 100 | |
| Condylar angle (°) | S–Ar–Go |
| Position of the Mandible | Canines/Incisors | Definition |
|---|---|---|
| sagittal | Class I (1) | the lower canine occluded between the upper canine and the lateral incisor |
| Class II with one-half cusp distalization (D ½ c) | the upper canine occludes with the lower canine | |
| Class II with one cusp distalization (D 1 c) | the lower canine occludes between the upper canine and the upper first premolar | |
| Class III with one-half cusp mesialization (M ½ c) | the upper canine occludes with the first lower premolar | |
| Class III with one cusp mesialization (M 1 c) | the upper canine occludes with the first and second lower premolar | |
| vertical | Normal overbite (NOB) | upper incisors vertically overlap 1/3–1/2 of the lower incisors |
| Deep bite (DB) | upper incisors vertically overlap more than 1/3–1/2 of the lower incisors | |
| Open bite (OB) | upper incisors vertically overlap less than 1/3–1/2 of the lower incisors |
| Category | Signs According to RDC/TMD | (%) |
|---|---|---|
| Associated pain-related signs | Arthralgia and myalgia | 14/24 (58.33%) |
| Arthralgia | 10/24 (41.66%) | |
| Associated intra-articular signs | Clicking/popping during opening and closing and during protrusive/laterotrusive movements (among arthralgia and myalgia patients) | 8/14 (57.1%) |
| Crepitus during opening/protrusive/laterotrusive movements (among arthralgia and myalgia patients) | 6/14 (42.9%) | |
| Clicking/popping during opening and closing and during protrusive/laterotrusive movements (among arthralgia patients) | 6/10 (60%) | |
| Crepitus during opening/protrusive/laterotrusive movements (among arthralgia patients) | 4/10 (40%) |
| Before Therapy | After Therapy | p-Value | Cohen G-Value | |
|---|---|---|---|---|
| Right TMJ | ||||
| Normal | 3/24 (12.5%) | 3/24 (12.5%) | NaN * | NaN * |
| Flattening | 21/24 (87.5%) | 21/24 (87.5%) | NaN * | NaN * |
| Surface erosion | 10/24 (41.6%) | 4/24 (16.6%) | 0.01 ** | 1 *** |
| Subcortical cyst | 9/24 (37.5%) | 3/24 (12.5%) | 0.02 ** | 1 *** |
| Left TMJ | ||||
| Normal | 4/24 (16.6%) | 4/24 (16.6%) | NaN * | NaN * |
| Flattening | 20/24 (83.3%) | 20/24 (83.3%) | NaN * | NaN * |
| Surface erosion | 6/24 (25%) | 2/24 (8.33%) | 0.05 ** | 1 *** |
| Subcortical cyst | 8/24 (33.3%) | 3/24 (12.5%) | 0.05 ** | 0.71 *** |
| Before Therapy | After Therapy |
|---|---|
| No surface erosion/subcortical cyst: 2/24 (8.33%) => | No surface erosion/subcortical cyst: 2/2 (100%) |
| Unilateral surface erosion/subcortical cyst: 0/2 (0%) | |
| Bilateral surface erosion/subcortical cyst: 0/2 (0%) | |
| Unilateral surface erosion/subcortical cyst: 11/24 (45.83%) => | No surface erosion/subcortical cyst: 5/11 (45.45%) |
| Unilateral surface erosion/subcortical cyst: 6/11 (54.54%) | |
| Bilateral surface erosion/subcortical cyst: 0/24 (0%) | |
| Bilateral surface erosion/subcortical cyst: 11/24 (45.83%) => | No surface erosion/subcortical cyst: 6/11 (54.54%) |
| Unilateral surface erosion/subcortical cyst: 4/11 (36.36%) | |
| Bilateral surface erosion/subcortical cyst: 1/11 (9.09%) | |
| p = 0.001 a | |
| Parameter | Before Therapy | After Therapy | p-Value | Effect Size |
|---|---|---|---|---|
| SNA (°), mean (SD) | 79.38 (2.91) | 79.77 (2.95) | 0.102 a | 0.35 * |
| SNB (°), mean (SD) | 75.61 (3.47) | 74.82 (3.41) | 0.002 a | 0.73 * |
| ANB (°), median (Q1, Q3) | 4.05 (3.35–4.9) | 4.8 (3.3–6.12) | <0.001 b | 0.48 ** |
| AFH (mm), median (Q1, Q3) | 112.85 (109.28–118.72) | 115.3 (112.58–118.88) | <0.001 b | 0.58 ** |
| PFH (mm), median (Q1, Q3) | 72.15 (67.38–78.05) | 71.7 (67.35–75.78) | 0.864 b | 0.02 ** |
| PFH/AFH (%), median (Q1, Q3) | 64.17 (61.39–66.1) | 63 (59.68–64.51) | 0.012 b | 0.36 ** |
| Condylar angle (°), mean (SD) | 140.84 (8.18) | 144.42 (8.87) | 0.007 a | 0.6 * |
| Unilateral Surface Erosion/Subcortical Cyst (11/24) | Bilateral Surface Erosion/Subcortical Cyst (11/24) | |||||
|---|---|---|---|---|---|---|
| Parameter | Before Therapy | After Therapy | p-Value | Before Therapy | After Therapy | p-Value |
| SNA (°) | 78.67 (3.08) | 79.17 (3.67) | 0.239 a | 80.29 (2.83) | 80.62 (2.19) | 0.331 a |
| SNB (°) | 74.20 (72.80–75.80) | 73.60 (71.80–75.50) | 0.059 b | 76.09 (3.46) | 75.15 (3.23) | 0.002 a |
| ANB (°) | 3.70 (2.10) | 4.93 (3.13) | 0.028 a | 4.10 (3.60–5.2) | 5 (4.5–6.5) | 0.006 b |
| AFH (mm) | 114.33 (9.33) | 117.01 (8.08) | 0.007 a | 112 (111.40–118.60) | 116.2 (112.7–118.7) | 0.006 b |
| PFH (mm) | 72.82 (6.51) | 72.14 (5.95) | 0.435 a | 71.84 (6.44) | 72.32 (7.09) | 0.691 a |
| PFH/AFH (%) | 64.38 (57.99–66.51) | 63.44 (56.74–65.59) | 0.286 b | 63.72 (3.06) | 61.65 (2.71) | 0.014 a |
| Condylar angle (°) | 142.5 (138.1–147.7) | 142.5 (134–152.7) | 0.444 b | 139.92 (7.32) | 144.73 (7.41) | 0.003 a |
| Right Canine Before Therapy | Right Canine After Therapy | Left Canine Before Therapy | Left Canine After Therapy | Incisors Overbite Before Therapy | Incisors Overbite After Therapy |
|---|---|---|---|---|---|
| 1: 11/24 (45.83%) => | 1: 4/24 (36.36%) | 1: 12/24 (50%) => | 1: 3/24 (25%) | NOB: 17/24 (70.83%) => | NOB: 2/24 (11.76%) |
| D ½ c: 6/24 (54.55%) | D ½ c: 9/24 (75%) | ||||
| D 1 c: 0/24 (0%) | D 1 c: 0/24 (0%) | NOB: 2/24 (11.76%) | |||
| M ½ c: 1/24 (9.09%) | M ½ c: 0/24 (0%) | DB: 0/24 (0%) | |||
| D ½ c: 11/24 (45.83%) => | 1: 0/24 (0%) | D ½ c: 9/24 (37.5%) => | 1: 0/24 (0%) | DB:5/24 (20.83%) => | NOB: 3/24 (60%) |
| D ½ c: 8/24 (72.73%) | D ½ c: 7/24 (77.78%) | ||||
| D 1 c: 3/24 (27.27%) | D 1 c: 1/24 (11.11%) | DB: 1/24 (20%) | |||
| M ½ c: 0/24 (0%) | M ½ c: 1/24 (11.11%) | OB: 1/24 (20%) | |||
| D 1 c: 1/24 (4.17%) => | 1: 0/24 (0%) | D 1 c: 3/24 (12.5%) => | 1: 1/24 (33.33%) | OB: 2/24 (8.33%) => | NOB: 0/24 (0%) |
| D ½ c: 1/24 (100%) | D ½ c: 0/24 (0%) | ||||
| D 1 c: 0 (0%) | D 1 c: 0 (0%) | ||||
| M ½ c: 0 (0%) | M ½ c: 2 (66.66%) | DB: 0/24 (0%) | |||
| M ½ c: 1/24 (4.17%) => | 1: 1 (100%) | M ½ c: 0/24 (0%) => | 1: 0 (0%) | ||
| D ½ c: 0 (0%) | D ½ c: 0 (0%) | ||||
| D 1 c: 0 (0%) | D 1 c: 0 (0%) | OB: 2/24 (100%) | |||
| M ½ c: 0 (0%) | M ½ c: 0 (0%) | ||||
| p = 0.038 a | p < 0.001 a | p < 0.001 a | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tăut, M.; Barbur, I.; Hedeșiu, M.; Ban, A.; Leucuța, D.; Negucioiu, M.; Buduru, S.D.; Ilea, A. Condylar Remodeling and Skeletal Changes Following Occlusal Splint and Manual Therapy: A Cone Beam Computed Tomography Study in Temporomandibular Disorders. J. Clin. Med. 2024, 13, 5567. https://doi.org/10.3390/jcm13185567
Tăut M, Barbur I, Hedeșiu M, Ban A, Leucuța D, Negucioiu M, Buduru SD, Ilea A. Condylar Remodeling and Skeletal Changes Following Occlusal Splint and Manual Therapy: A Cone Beam Computed Tomography Study in Temporomandibular Disorders. Journal of Clinical Medicine. 2024; 13(18):5567. https://doi.org/10.3390/jcm13185567
Chicago/Turabian StyleTăut, Manuela, Ioan Barbur, Mihaela Hedeșiu, Alina Ban, Daniel Leucuța, Marius Negucioiu, Smaranda Dana Buduru, and Aranka Ilea. 2024. "Condylar Remodeling and Skeletal Changes Following Occlusal Splint and Manual Therapy: A Cone Beam Computed Tomography Study in Temporomandibular Disorders" Journal of Clinical Medicine 13, no. 18: 5567. https://doi.org/10.3390/jcm13185567
APA StyleTăut, M., Barbur, I., Hedeșiu, M., Ban, A., Leucuța, D., Negucioiu, M., Buduru, S. D., & Ilea, A. (2024). Condylar Remodeling and Skeletal Changes Following Occlusal Splint and Manual Therapy: A Cone Beam Computed Tomography Study in Temporomandibular Disorders. Journal of Clinical Medicine, 13(18), 5567. https://doi.org/10.3390/jcm13185567