
Immediate Platelet Inhibition Strategy for Comatose Out-of-Hospital Cardiac Arrest Survivors Undergoing Percutaneous Coronary Intervention and Mild Therapeutic Hypothermia
Abstract
:1. Introduction
2. Materials and Methods
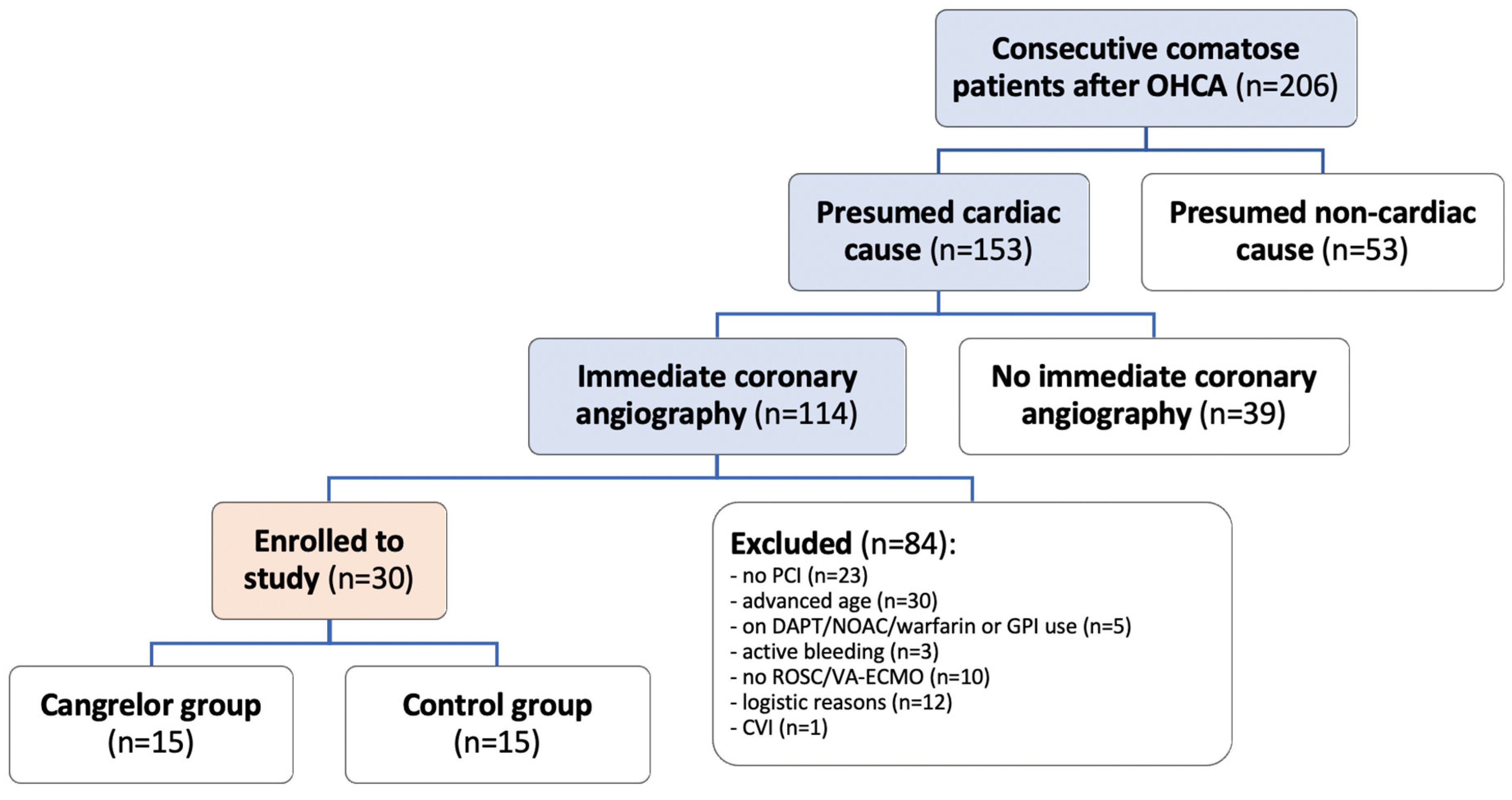
2.1. Study Setting and Patients
2.2. Platelet Reactivity
2.3. Primary Endpoints
2.4. Secondary Endpoints
- Angiographic result—Final Thrombolysis in Myocardial Infarction (TIMI) Flow. Final angiographic result at the end of the procedure was assessed by an independent blinded interventional cardiologist;
- Rate of stent thrombosis. Defined as definite or probable ST based on the Academic Research Consortium (ARC) classification during the index patient hospitalization. Definite ST was confirmed at angiography or autopsy, while probable stent thrombosis included unexplained death within 30 days after PCI or new myocardial infarction in the PCI vessel territory;
- Timing of ST. Stent thrombosis events were categorized as acute (within 24 h after stenting) or subacute (24 h to 30 days after stenting);
- Survival. We described survival to discharge from the hospital during the index hospitalization, up to 90 days;
- Survival with favorable neurological outcome—Cerebral Performance Category (CPC). We assessed survival to discharge from the hospital based on CPC scores, with CPC 1–2 indicating a favorable neurological outcome. Evaluation was conducted during the index hospitalization, up to 90 days.
2.5. Power Analysis and Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. Angiographic Characteristics
3.3. Platelet Inhibition and Stent Thrombosis
3.4. Secondary Endpoints
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Prüller, F.; Bis, L.; Milke, O.L.; Fruhwald, F.; Pätzold, S.; Altmanninger-Sock, S.; Siller-Matula, J.M.; Von Lewinski, F.; Ablasser, K.; Sacherer, M.; et al. Cangrelor Induces More Potent Platelet Inhibition without Increasing Bleeding in Resuscitated Patients. J. Clin. Med. 2018, 7, 442. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Shah, S.M.M.; Mubashir, A.; Khan, A.R.; Fatima, K.; Schenone, A.L.; Khosa, F.; Samady, H.; Menon, V. Early coronary angiography in patients resuscitated from out of hospital cardiac arrest without ST-segment elevation: A systematic review and meta-analysis. Resuscitation 2017, 121, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Parodi, G.; Bellandi, B.; Xanthopoulou, I.; Capranzano, P.; Capodanno, D.; Valenti, R.; Stavrou, K.; Migliorini, A.; Antoniucci, D.; Tamburino, C.; et al. Morphine is associated with a delayed activity of oral antiplatelet agents in patients with ST-elevation acute myocardial infarction undergoing primary percutaneous coronary intervention. Circ. Cardiovasc. Interv. 2014, 8, e001593. [Google Scholar] [CrossRef] [PubMed]
- Steblovnik, K.; Blinc, A.; Mijovski, M.B.; Fister, M.; Mikuz, U.; Noc, M. Ticagrelor Versus Clopidogrel in Comatose Survivors of Out-of-Hospital Cardiac Arrest Undergoing Percutaneous Coronary Intervention and Hypothermia: A Randomized Study. Circulation 2016, 134, 2128–2130. [Google Scholar] [CrossRef] [PubMed]
- Noc, M.; Fajadet, J.; Lassen, J.F.; Kala, P.; MacCarthy, P.; Olivecrona, G.K.; Windecker, S.; Spaulding, C. Invasive coronary treatment strategies for out-of-hospital cardiac arrest: A consensus statement from the European association for percutaneous cardiovascular interventions (EAPCI)/stent for life (SFL) groups. EuroIntervention 2014, 10, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Marquis-Gravel, G.; Zeitouni, M.; Kochar, A.; Jones, W.S.; Sketch, M.H.; Rao, S.V.; Patel, M.R.; Ohman, E.M. Technical consideration in acute myocardial infarction with cardiogenic shock: A review of antithrombotic and PCI therapies. Catheter. Cardiovasc. Interv. 2020, 95, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, T.; Sangiorgi, D.; Reggiani, L.B.; Kirtane, A.J.; Stone, G.W.; Serruys, P.W.; Smits, P.C.; Kedhi, E.; Kereiakes, D.; Kaiser, C.; et al. Stent thrombosis with everolimus-eluting stents: Meta-analysis of comparative randomized controlled trials. Circ. Cardiovasc. Interv. 2012, 5, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Rosillo, S.O.; Lopez-de-Sa, E.; Iniesta, A.M.; de Torres, F.; del Prado, S.; Rey, J.R.; Armada, E.; Moreno, R.; López-Sendón, J.L. Is therapeutic hypothermia a risk factor for stent thrombosis? J. Am. Coll. Cardiol. 2014, 63, 939–940. [Google Scholar] [CrossRef] [PubMed]
- Joffre, J.; Varenne, O.; Bougouin, W.; Rosencher, J.; Mira, J.P.; Cariou, A. Stent thrombosis: An increased adverse event after angioplasty following resuscitated cardiac arrest. Resuscitation 2014, 85, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Gouffran, G.; Rosencher, J.; Bougouin, W.; Jakamy, R.; Joffre, J.; Lamhaut, L.; Dumas, F.; Cariou, A.; Varenne, O. Stent thrombosis after primary percutaneous coronary intervention in comatose survivors of out-of-hospital cardiac arrest: Are the new P2Y12 inhibitors really more effective than clopidogrel? Resuscitation 2016, 98, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Penela, D.; Magaldi, M.; Fontanals, J.; Martin, V.; Regueiro, A.; Ortiz, J.T.; Bosch, X.; Sabaté, M.; Heras, M. Hypothermia in acute coronary syndrome: Brain salvage versus stent thrombosis? J. Am. Coll. Cardiol. 2013, 61, 686–687. [Google Scholar] [CrossRef] [PubMed]
- Rauber, M.; Nicol, P.; Sabic, E.; Joner, M.; Noc, M. Timing and predictors of definite stent thrombosis in comatose survivors of out-of-hospital cardiac arrest undergoing percutaneous coronary intervention and therapeutic hypothermia (ST-OHCA study). EuroIntervention 2022, 18, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Kander, T.; Schött, U. Effect of hypothermia on haemostasis and bleeding risk: A narrative review. J. Int. Med. Res. 2019, 47, 3559–3568. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 °C versus 36 °C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, K.; Christoph, M.; Schmeinck, S.; Schmieder, K.; Steiding, K.; Schoener, L.; Pfluecke, C.; Quick, S.; Mues, C.; Jellinghaus, S.; et al. High rates of prasugrel and ticagrelor non-responder in patients treated with therapeutic hypothermia after cardiac arrest. Resuscitation 2014, 85, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Tardiff, B.E.; Jennings, L.K.; Harrington, R.A.; Gretler, D.; Potthoff, R.F.; Vorchheimer, D.A.; Eisenberg, P.R.; Lincoff, A.M.; Labinaz, M.; Joseph, D.M.; et al. Pharmacodynamics and pharmacokinetics of eptifibatide in patients with acute coronary syndromes: Prospective analysis from PURSUIT. Circulation 2001, 104, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Radu, R.I.; Ben Gal, T.; Abdelhamid, M.; Antohi, E.; Adamo, M.; Ambrosy, A.P.; Geavlete, O.; Lopatin, Y.; Lyon, A.; Miro, O.; et al. Antithrombotic and anticoagulation therapies in cardiogenic shock: A critical review of the published literature. ESC Heart Fail. 2021, 8, 4717–4736. [Google Scholar] [CrossRef] [PubMed]
- Gorog, D.A.; Price, S.; Sibbing, D.; Baumbach, A.; Capodanno, D.; Gigante, B.; Halvorsen, S.; Huber, K.; Lettino, M.; Leonardi, S.; et al. Antithrombotic therapy in patients with acute coronary syndrome complicated by cardiogenic shock or out-of-hospital cardiac arrest: A joint position paper from the European Society of Cardiology (ESC) Working Group on Thrombosis, in association with the Acute Cardiovascular Care Association (ACCA) and European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. Cardiovasc. Pharmacother. 2021, 7, 125–140. [Google Scholar] [PubMed]
- Keating, G.M. Cangrelor: A Review in Percutaneous Coronary Intervention. Drugs 2015, 75, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Harrington, R.A.; Stone, G.W.; Deliargyris, E.N.; Steg, P.G.; Gibson, C.M.; Hamm, C.W.; Price, M.J.; Steg, G.; Gibson, M.; et al. Evaluation of Ischemic and Bleeding Risks Associated With 2 Parenteral Antiplatelet Strategies Comparing Cangrelor With Glycoprotein IIb/IIIa Inhibitors: An Exploratory Analysis From the CHAMPION Trials. JAMA Cardiol. 2017, 2, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.; Gerbaud, E.; Coste, P.; Cetran, L.; Marchand, H.; Seguy, B. Optimal platelet inhibition with cangrelor in comatose survivors of out-of-hospital cardiac arrest undergoing primary percutaneous coronary intervention. Resuscitation 2018, 130, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Franchi, F.; Rollini, F.; Rivas, A.; Wali, M.; Briceno, M.; Agarwal, M.; Shaikh, Z.; Nawaz, A.; Silva, G.; Been, L.; et al. Platelet Inhibition With Cangrelor and Crushed Ticagrelor in Patients With ST-Segment-Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. Circulation 2019, 139, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Kordis, P.; Bozic Mijovski, M.; Berden, J.; Steblovnik, K.; Blinc, A.; Noc, M. Cangrelor for comatose survivors of out-of-hospital cardiac arrest undergoing percutaneous coronary intervention: The CANGRELOR-OHCA study. EuroIntervention 2023, 18, 1269–1271. [Google Scholar]
- Kocjancic, S.T.; Jazbec, A.; Noc, M. Impact of intensified postresuscitation treatment on outcome of comatose survivors of out-of-hospital cardiac arrest according to initial rhythm. Resuscitation 2014, 85, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef] [PubMed]
- Tantry, U.S.; Bonello, L.; Aradi, D.; Price, M.J.; Jeong, Y.-H.; Angiolillo, D.J.; Stone, G.W.; Curzen, N.; Geisler, T.; ten Berg, J.; et al. Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding. J. Am. Coll. Cardiol. 2013, 62, 2261–2273. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef]
- Dézsi, D.A.; Merkely, B.; Skopál, J.; Barabás, E.; Várnai, K.; Faluközy, J.; Veress, G.; Alotti, N.; Aradi, D. Impact of Test Conditions on ADP-Induced Platelet Function Results With the Multiplate Assay: Is Further Standardization Required? J. Cardiovasc. Pharmacol. Ther. 2018, 23, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.J. Transition strategies from cangrelor to oral platelet P2Y12 receptor antagonists. Coron. Artery Dis. 2016, 27, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Franchi, F.; Rollini, F.; Ortega-Paz, L.; Been, L.; Giordano, S.; Galli, M.; Ghanem, G.; Garabedian, H.; Al Saleh, T.; Uzunoglu, E.; et al. Switching From Cangrelor to Prasugrel in Patients Undergoing Percutaneous Coronary Intervention: The Switching Antiplatelet-6 (SWAP-6) Study. JACC Cardiovasc. Interv. 2023, 16, 2528–2539. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.; Esposito, G.; Avvedimento, M.; Nagler, M.; Minuz, P.; Campo, G.; Gragnano, F.; Manavifar, N.; Piccolo, R.; Tebaldi, M.; et al. Cangrelor, Tirofiban, and Chewed or Standard Prasugrel Regimens in Patients With ST-Segment-Elevation Myocardial Infarction: Primary Results of the FABOLUS-FASTER Trial. Circulation 2020, 142, 441–454, Erratum in Circulation 2020, 142, e71. [Google Scholar] [CrossRef] [PubMed]
- Buchtele, N.; Herkner, H.; Schörgenhofer, C.; Merrelaar, A.; Laggner, R.; Gelbenegger, G.; Spiel, A.O.; Domanovits, H.; Lang, I.; Jilma, B.; et al. High Platelet Reactivity after Transition from Cangrelor to Ticagrelor in Hypothermic Cardiac Arrest Survivors with ST-Segment Elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 583. [Google Scholar] [CrossRef] [PubMed]
- Blaško, P.; Samoš, M.; Bolek, T.; Stančiaková, L.; Škorňová, I.; Péč, M.J.; Jurica, J.; Staško, J.; Mokáň, M. Resistance on the Latest Oral and Intravenous P2Y12 ADP Receptor Blockers in Patients with Acute Coronary Syndromes: Fact or Myth? J. Clin. Med. 2022, 11, 7211. [Google Scholar] [CrossRef] [PubMed]
- Cavender, M.A.; Harrington, R.A.; Stone, G.W.; Steg, P.G.; Gibson, C.M.; Hamm, C.W.; Price, M.J.; Lopes, R.D.; Leonardi, S.; Deliargyris, E.N.; et al. Ischemic Events Occur Early in Patients Undergoing Percutaneous Coronary Intervention and Are Reduced With Cangrelor: Findings From CHAMPION PHOENIX. Circ. Cardiovasc. Interv. 2022, 15, e010390. [Google Scholar] [CrossRef] [PubMed]
- Saint Croix, G.; Lacy, S.C.; Gazzhal, A.; Ibrahim, M.; Gjergjindreaj, M.; Perez, J.; Shehadeh, M.; Vedantam, K.; Torres, C.; Beohar, N.; et al. Dual Antiplatelet Therapy in Patients Aged 75 Years and Older with Coronary Artery Disease: A Meta-Analysis and Systematic Review. J. Interv. Cardiol. 2022, 2022, 3111840. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Elia, E.; de Filippo, O.; Manai, R.; Breviario, S.; Bruno, F.; Iannaccone, M.; Wańha, W.; Bianco, M.; Patti, G.; et al. Net clinical benefit of different strategies of dual antiplatelet therapy in elderly patients: Data from the praise registry. Int. J. Cardiol. 2022, 353, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Brítez, G.; Freixa, X.; Flores, E.; Penela, D.; Hernandez-Enríquez, M.; Antonio, R.S.; Caixal, G.; Garcia, J.; Roqué, M.; Martín, V.; et al. Safety of glycoprotein IIb/IIIa inhibitors in patients under therapeutic hypothermia admitted for an acute coronary syndrome. Resuscitation 2016, 106, 108–112. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
| Male gender | 14 (93%) | 15 (100%) | 1.000 |
| Age, years | 56 ± 7 | 58 ± 6 | 0.317 |
| BMI, kg/m2 | 27 ± 4 | 28 ± 7 | 0.547 |
| Arterial hypertension | 6 (40%) | 5 (33%) | 0.705 |
| Hyperlipidemia | 4 (27%) | 3 (20%) | 1.000 |
| Diabetes mellitus | 3 (20%) | 2 (13%) | 1.000 |
| Smoking | 7 (47%) | 5 (33%) | 0.456 |
| Known ischemic heart disease | 2 (13%) | 1 (7%) | 1.000 |
| Previous myocardial infarction | 0 (0%) | 1 (7%) | 1.000 |
| Previous PCI/CABG | 1 (7%) | 1 (7%) | 1.000 |
| Witnessed cardiac arrest | 14 (93%) | 12 (80%) | 0.598 |
| Lay BLS | 14 (93%) | 13 (87%) | 1.000 |
| Time to EMS arrival, min | 10 ± 6 | 8 ± 4 | 0.410 |
| Shockable rhythm on arrival | 14 (100%) | 15 (100%) | NA |
| Time from EMS arrival to ROSC, min | 12 ± 14 | 14 ± 8 | 0.522 |
| Total downtime, min | 21 ± 15 | 23 ± 9 | 0.758 |
| STEMI on 12-lead ECG | 9 (60%) | 12 (80%) | 0.427 |
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
| Arterial lactate, mmol/L | 3.7 ± 2.3 | 4.8 ± 4.4 | 0.404 |
| Arterial pH | 7.27 ± 0.08 | 7.20 ± 0.11 | 0.072 |
| Serum glucose, mmol/L | 11.1 ± 4.2 | 13.3 ± 3.9 | 0.149 |
| Creatinine, µmol/L | 104 ± 15 | 104 ± 21 | 0.907 |
| GFR < 60 mL/min | 3 (20%) | 5 (33%) | 0.682 |
| Hemoglobin, g/L | 148 ± 12 | 145 ± 15 | 0.554 |
| Platelet count, ×109/L | 243 ± 84 | 223 ± 66 | 0.484 |
| Troponin I on admission, ng/L | 3.424 ± 3.349 | 14.233 ± 24.884 | 0.107 |
| Peak troponin I value, ng/L | 77.179 ± 164.499 | 95.018 ± 112.963 | 0.732 |
| LVEF < 40% on admission | 5 (36%) | 3 (23%) | 0.678 |
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
| Multivessel coronary disease | 11 (73%) | 4 (27%) | 0.011 * |
| Acute lesion | |||
| Left main | 1 (7%) | 0 (0%) | 1.000 |
| LAD | 7 (47%) | 10 (67%) | 0.269 |
| LCX/Ramus | 3 (20%) | 2 (13%) | 1.000 |
| RCA | 3 (20%) | 3 (20%) | 1.000 |
| TIMI flow 0–1 in acute lesion | 10 (71%) | 12 (80%) | 0.682 |
| PCI characteristics | |||
| Lesions treated per patient | 1.2 ± 0.7 | 1.0 ± 0 | 0.279 |
| Number of stents per patient | 1.5 ± 1.1 | 1.3 ± 1.2 | 0.753 |
| Mean stent diameter, mm | 2.5 ± 1.1 | 2.8 ± 0.8 | 0.387 |
| Mean length of stented segments, mm | 34.8 ± 19.0 | 29.2 ± 24.7 | 0.521 |
| Successful PCI | 13 (87%) | 15 (100%) | 0.483 |
| Multivessel PCI | 2 (13%) | 0 (0%) | 0.483 |
| TIMI flow 2–3 at the end of PCI | 13 (100%) | 15 (100%) | 1.000 |
| Start of PCI to ticagrelor interval, min | 56 ± 19 | 64 ± 19 | 0.252 |
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
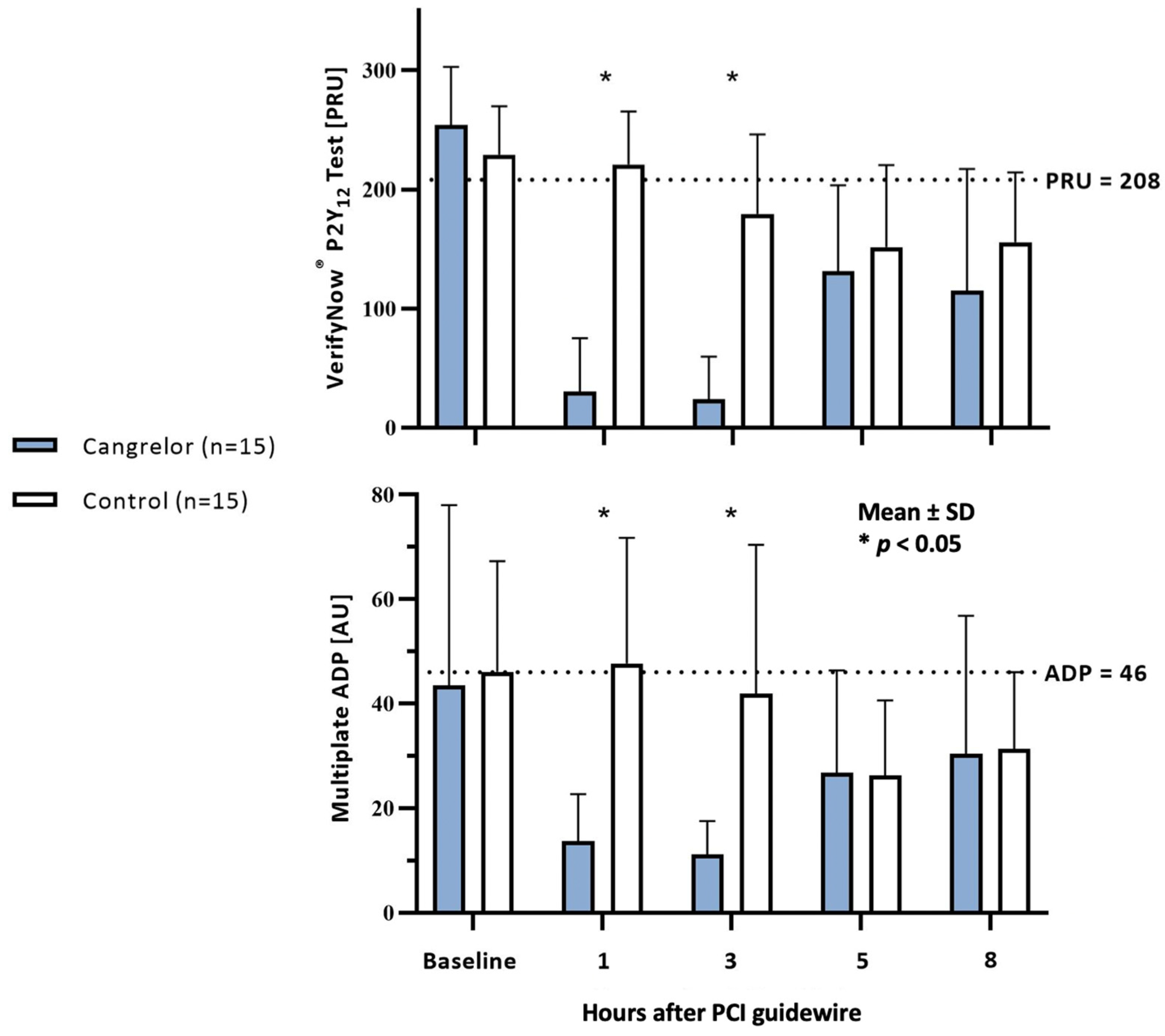
| Baseline VerifyNow® HPR | 12 (80%) | 11 (73%) | 1.000 |
| 1 h | 0 (0%) | 10 (67%) | 0.001 * |
| 3 h | 0 (0%) | 7 (47%) | 0.007 * |
| 5 h | 1 (8%) | 4 (27%) | 0.342 |
| 8 h | 1 (20%) | 2 (25%) | 1.000 |
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
| Baseline Multiplate® HPR | 5 (33%) | 4 (29%) | 1.000 |
| 1 h | 0 (0%) | 5 (39%) | 0.013 * |
| 3 h | 0 (0%) | 5 (33%) | 0.044 * |
| 5 h | 1 (8%) | 2 (13%) | 1.000 |
| 8 h | 1 (20%) | 1 (17%) | 1.000 |
| Cangrelor Group (n = 15) | Control Group (n = 15) | p-Value | |
|---|---|---|---|
| Bleeding events | 3 (20%) | 1 (7%) | 0.589 |
| BARC 2/3/5 or need for cangrelor discontinuation | |||
| TIMI flow 2–3 at the end of PCI | 13 (100%) | 15 (100%) | 1.000 |
| Stent thrombosis | 2 (14%) | 3 (20%) | 1.000 |
| Survival to hospital discharge | 10 (67%) | 9 (60%) | 1.000 |
| Survival with CPC 1/2 | 10 (67%) | 9 (60%) | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kordis, P.; Berden, J.; Mikuz, U.; Noc, M. Immediate Platelet Inhibition Strategy for Comatose Out-of-Hospital Cardiac Arrest Survivors Undergoing Percutaneous Coronary Intervention and Mild Therapeutic Hypothermia. J. Clin. Med. 2024, 13, 2121. https://doi.org/10.3390/jcm13072121
Kordis P, Berden J, Mikuz U, Noc M. Immediate Platelet Inhibition Strategy for Comatose Out-of-Hospital Cardiac Arrest Survivors Undergoing Percutaneous Coronary Intervention and Mild Therapeutic Hypothermia. Journal of Clinical Medicine. 2024; 13(7):2121. https://doi.org/10.3390/jcm13072121
Chicago/Turabian StyleKordis, Peter, Jernej Berden, Ursa Mikuz, and Marko Noc. 2024. "Immediate Platelet Inhibition Strategy for Comatose Out-of-Hospital Cardiac Arrest Survivors Undergoing Percutaneous Coronary Intervention and Mild Therapeutic Hypothermia" Journal of Clinical Medicine 13, no. 7: 2121. https://doi.org/10.3390/jcm13072121