

Anatomical Safety Area for Periarticular Analgesic Infiltration through the Posterior Capsule in Total Knee Arthroplasty: Radiological Study in Magnetic Resonance
 ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Inclusion Criteria
- -
- Age between 18 and 75 years old;
- -
- Subjects with no trauma history or previous knee surgery, osteoarthritis, malformation, or tumors (including Baker’s cyst), which could alter the normal anatomy of the popliteal fossa;
- -
- Sufficient image quality to perform measurements.
2.3. Exclusion Criteria
- -
- Age under 18 years old or over 75 years old;
- -
- Subjects with trauma history or previous knee surgery, osteoarthritis, malformation or tumors (including Baker’s cyst), which could alter the normal anatomy of the popliteal fossa;
- -
- Insufficient image quality to perform measurements.
2.4. Ethics
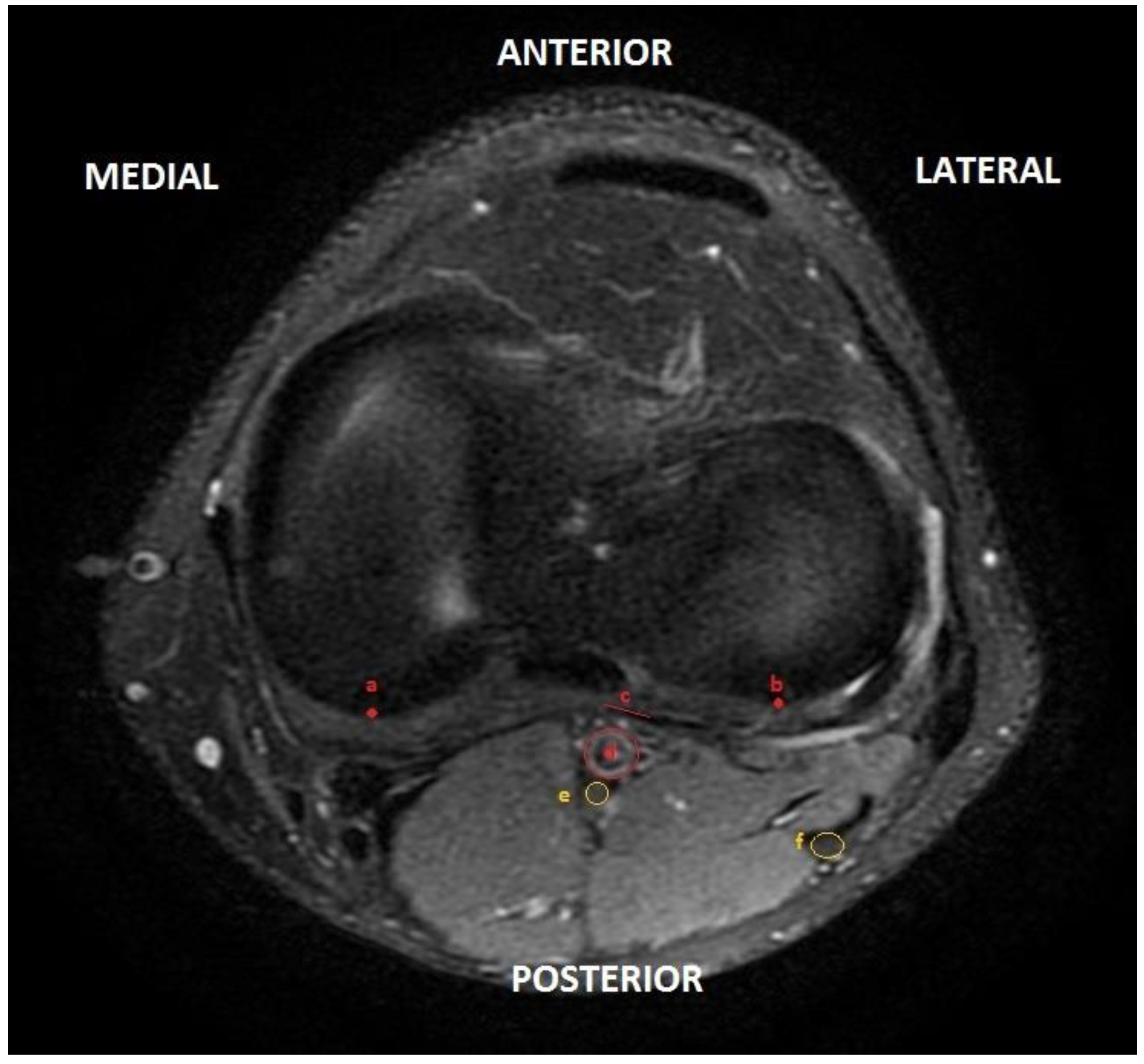
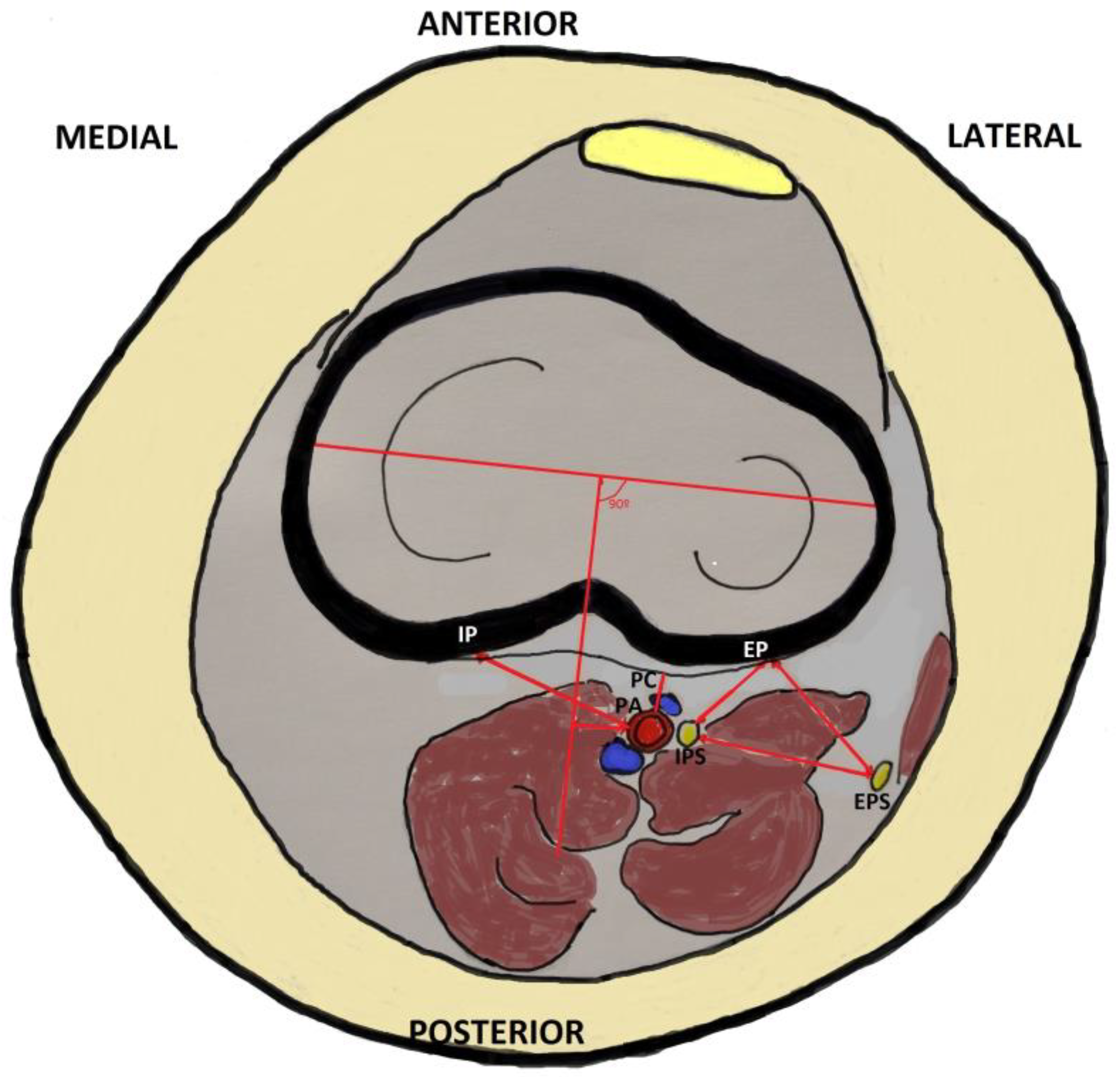
2.5. MRI Analysis
- Distance from the center of the posterior edge of the external tibial plateau to the common peroneal or external popliteal sciatic nerve (EP–EPS);
- Distance from the center of the posterior edge of the external tibial plateau to the internal popliteal sciatic nerve (EP–IPS);
- Distance between common and tibial peroneal nerve (external and internal popliteal sciatic nerve) (EPS–IPS);
- Distance from central posterior capsule to popliteal artery (PC–PA);
- Distance from the center of the posterior border of the internal tibial plateau to the popliteal artery (IP–PA).
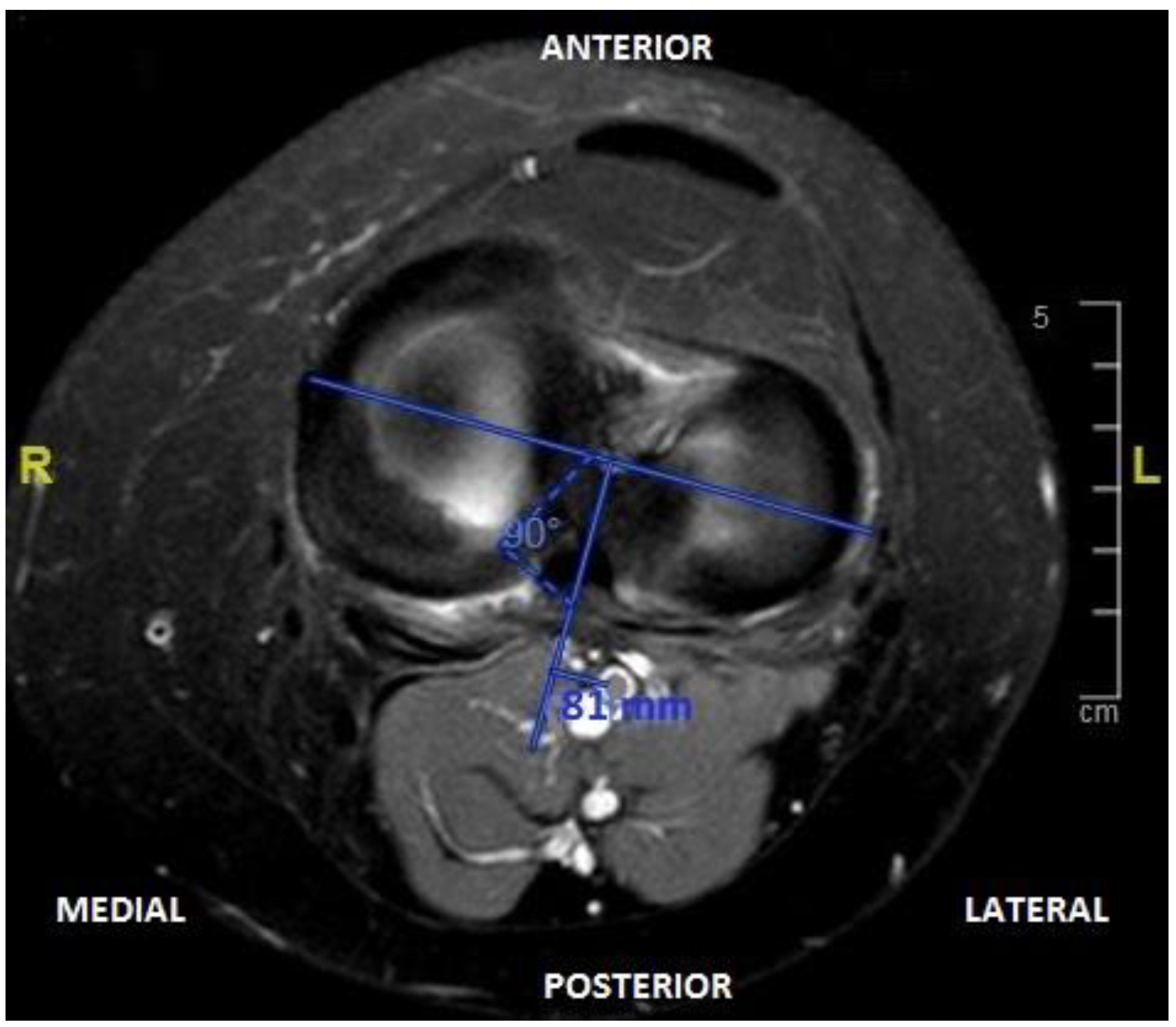
- Distance from the intercondylar midline to the center of the popliteal artery (IM–PA). To perform this measurement, the line perpendicular to the coronal axis of both tibial plateaus was drawn at 90° and the distance from the center of the popliteal artery to this line was measured (Figure 3).
2.6. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Relevance Statement
Key Points
Abbreviations
| MRI | Magnetic resonance imaging |
| EP | External tibial plateau |
| EPS | External popliteal sciatic nerve |
| IPS | Internal popliteal sciatic nerve |
| PC | Posterior capsule |
| PA | Popliteal artery |
| IP | Internal tibial plateau |
| IM | Intercondylar midline |
| TKA | Total knee arthroplasty |
| IPA | Intraoperative periarticular analgesic |
| SEM | Standard error mean |
References
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Chiu, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J. The Epidemiology of Revision Total Knee Arthroplasty in the United States. Clin. Orthop. Relat. Res. 2010, 468, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Greimel, F.; Maderbacher, G.; Baier, C.; Schwarz, T.; Zeman, F.; Meissner, W.; Grifka, J.; Benditz, A. Matched-Pair Analysis of Local Infiltration Analgesia in Total Knee Arthroplasty: Patient Satisfaction and Perioperative Pain Management in 846 Cases. J. Knee Surg. 2018, 32, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Barastegui, D.; Robert, I.; Palau, E.; Haddad, S.; Reverte-Vinaixa, M.; Lorente, L.; Cots, M. Can local infiltration analgesia increase satisfaction in postoperative short-term pain control in total knee arthroplasty? J. Orthop. Surg. 2017, 25, 2309499017690461. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.R.; Kohan, L. Local infiltration analgesia: A technique for the control of acute postoperative pain following knee and hip surgery: A case study of 325 patients. Acta Orthop. 2008, 79, 174–183. [Google Scholar] [CrossRef]
- Hadzic, A.; Houle, T.T.; Capdevila, X.; Ilfeld, B.M. Femoral nerve block for analgesia in patients having knee arthroplasty. Anesthesiology 2010, 113, 1014–1015. [Google Scholar] [CrossRef]
- Zaric, D.; Boysen, K.; Christiansen, C.; Christiansen, J.; Stephensen, S.; Christensen, B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth. Analg. 2006, 10, 1240–1246. [Google Scholar] [CrossRef]
- Campbell, A.; McCormick, M.; McKinlay, K.; Scott, N.B. Epidural vs. lumbar plexus infusions following total knee arthroplasty: Randomized controlled trial. Eur. J. Anaesthesiol. 2008, 25, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Shakespeare, D.; Kinzel, V. Rehabilitation after total knee replacement: Time to go home? Knee 2005, 12, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Essving, P.; Axelsson, K.; Kjellberg, J.; Wallgren, Ö.; Gupta, A.; Lundin, A. Reduced hospital stay, morphine consumption, and pain intensity with local infiltration analgesia after unicompartmental knee arthroplasty: A randomised double blind study of 40 patients. Acta Orthop. 2009, 80, 213–219. [Google Scholar] [CrossRef]
- Dahl, J.B.; Møiniche, S. Relief of postoperative pain by local anaesthetic infiltration: Efficacy for major abdominal and orthopaedic surgery. Pain 2009, 143, 7–11. [Google Scholar] [CrossRef]
- Pasero, C.; McCaffery, M. Orthopaedic postoperative pain management. J. Perianesth. Nurs. 2007, 22, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Busch, C.A.; Shore, B.J.; Bhandari, R.; Ganapathy, S.; MacDonald, S.J.; Bourne, R.B.; Rorabeck, C.H.; McCalden, R.W. Efficacy of periarticular multimodal drug injection in total knee arthroplasty. A randomised trial. J. Bone Joint Surg. Am. 2006, 88, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Otte, K.S.; Husted, H.; Andersen, L.Ø.; Kristensen, B.B.; Kehlet, H. Local Infiltration analgesia in total knee arthroplasty and hip resurfacing: A methodological study. Acute Pain 2008, 10, 111–116. [Google Scholar] [CrossRef]
- Andersen, L.Ø.; Husted, H.; Otte, K.S.; Kristensen, B.; Kehlet, H. High volume infiltration analgesia in total knee arthroplasty: A randomised, double-blind, placebo controlled trial. Acta Anaesthesiol. Scand. 2008, 52, 1331–1335. [Google Scholar] [CrossRef] [PubMed]
- Kandasami, M.; Kinninmonth, A.W.G.; Sarungi, M.; Baines, J.; Scott, N.B. Femoral nerve block for total knee replacement—A word of caution. Knee 2009, 16, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Vendittoli, P.A.; Makinen, P.; Drolet, P.; Lavigne, M.; Fallaha, M.; Guertin, M.C.; Varin, F. A multimodal analgesia protocol for total knee arthroplasty. A randomised, controlled study. J. Bone Joint Surg. Am. 2006, 88, 282. [Google Scholar] [CrossRef] [PubMed]
- McDonald, D.A.; Siegmeth, R.; Deakin, A.H.; Kinninmonth, A.W.G.; Scott, N.B. An enhanced recovery programme for primary total knee arthroplasty in the United Kingdom follow up at one year. Knee 2012, 19, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.; Deakin, A.H.; McDonald, D.A.; Cunningham, I.K.T.; Payne, A.P.; Picard, F. An anatomic study of local infiltration analgesia in total knee arthroplasty. Knee 2013, 20, 319–323. [Google Scholar] [CrossRef]
- Hirasawa, Y.; Okajima, S.; Ohta, M.; Tokioka, T. Nerve distribution to the human knee joint: Anatomical and immunohistochemical study. Int. Orthop. 2000, 24, 1–4. [Google Scholar] [CrossRef]
- Horner, G.; Dellon, L. Innervation of the human knee joint and implications for surgery. Clin. Orthop. 1994, 301, 221–226. [Google Scholar] [CrossRef]
- Ferguson, L.; Paterson, T.; Ramsay, F.; Arrol, K.; Dabernig, J.; Shaw-Dunn, J.; Morley, S. Applied anatomy of the latissimus dorsi free flap for refinement in one-stage facial reanimation. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Tubtim, C.H.; Laupattarakasem, P.; Laupattarfakasem, W.; Chaisiwamongkol, K. A comparative study comparing area of extension of posterior knee capsule via posteromedial injection: A cadaveric study. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1095–1100. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
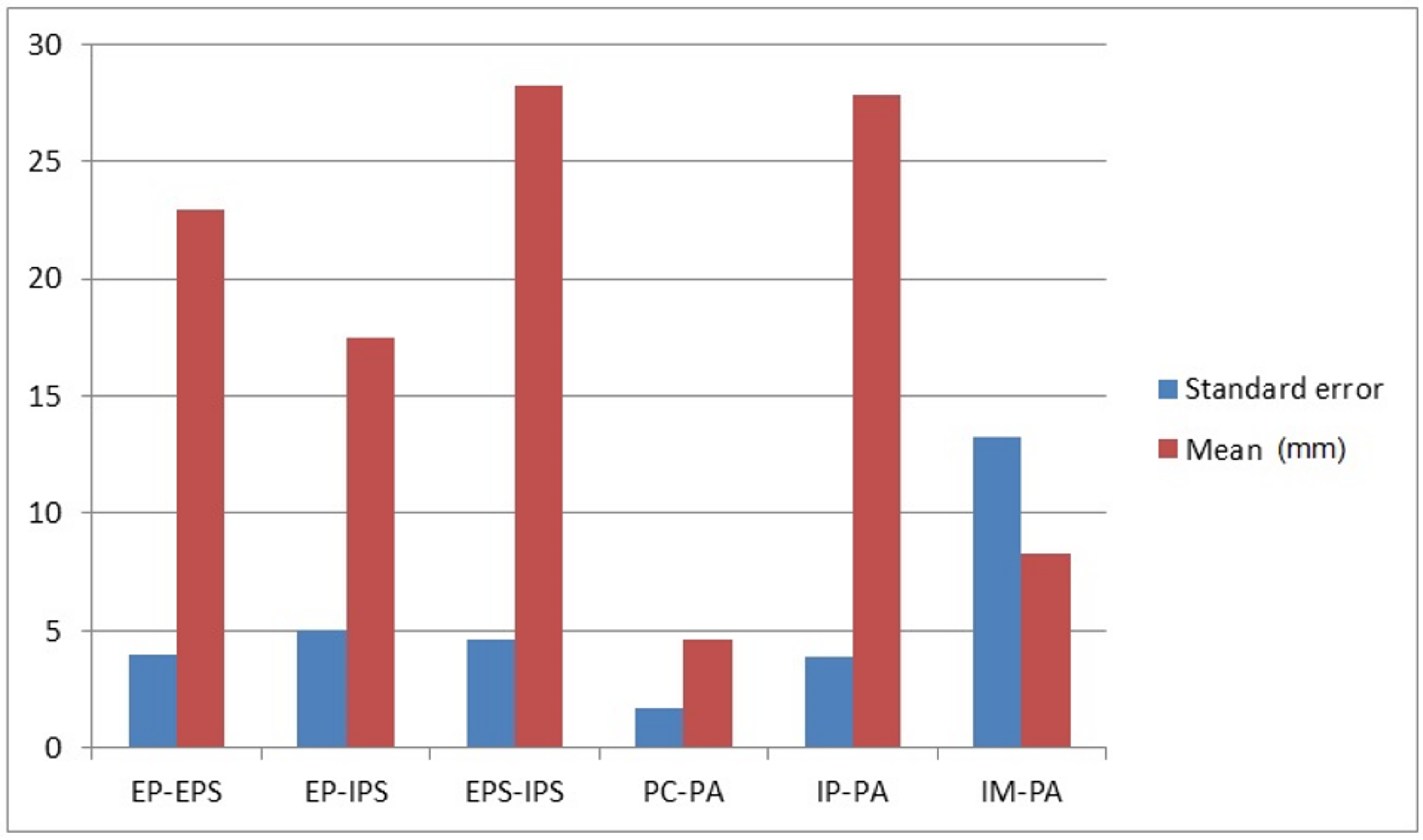
| Measurement | Mean | Minimum | Maximum | Standard Error |
|---|---|---|---|---|
| EP-EPS distance | 22.90 mm | 7.6 mm | 31.0 mm | 3.92 |
| EP-IPS distance | 17.46 mm | 8.5 mm | 34.8 mm | 4.99 |
| EPS-IPS distance | 28.23 mm | 12.1 mm | 39.9 mm | 4.61 |
| PC-PA distance | 4.59 mm | 1.5 mm | 10.3 mm | 1.64 |
| IP-PA distance | 27.79 mm | 15.3 mm | 37.9 mm | 3.9 |
| IM-PA distance | 8.3 mm | 1.6 mm | 18.2 mm | 13.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mifsut-Aleixandre, M.; Mifsut, D.; González-Soler, E.M.; Blasco-Serra, A.; Valverde, A.A. Anatomical Safety Area for Periarticular Analgesic Infiltration through the Posterior Capsule in Total Knee Arthroplasty: Radiological Study in Magnetic Resonance. J. Clin. Med. 2024, 13, 2123. https://doi.org/10.3390/jcm13072123
Mifsut-Aleixandre M, Mifsut D, González-Soler EM, Blasco-Serra A, Valverde AA. Anatomical Safety Area for Periarticular Analgesic Infiltration through the Posterior Capsule in Total Knee Arthroplasty: Radiological Study in Magnetic Resonance. Journal of Clinical Medicine. 2024; 13(7):2123. https://doi.org/10.3390/jcm13072123
Chicago/Turabian StyleMifsut-Aleixandre, Marta, Damián Mifsut, Eva María González-Soler, Arantxa Blasco-Serra, and Alfonso Amador Valverde. 2024. "Anatomical Safety Area for Periarticular Analgesic Infiltration through the Posterior Capsule in Total Knee Arthroplasty: Radiological Study in Magnetic Resonance" Journal of Clinical Medicine 13, no. 7: 2123. https://doi.org/10.3390/jcm13072123
APA StyleMifsut-Aleixandre, M., Mifsut, D., González-Soler, E. M., Blasco-Serra, A., & Valverde, A. A. (2024). Anatomical Safety Area for Periarticular Analgesic Infiltration through the Posterior Capsule in Total Knee Arthroplasty: Radiological Study in Magnetic Resonance. Journal of Clinical Medicine, 13(7), 2123. https://doi.org/10.3390/jcm13072123