
Impact of Minimally Invasive Intra-Capsular Metatarsal Osteotomy on Plantar Pressure Decrease: A Cross-Sectional Study

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
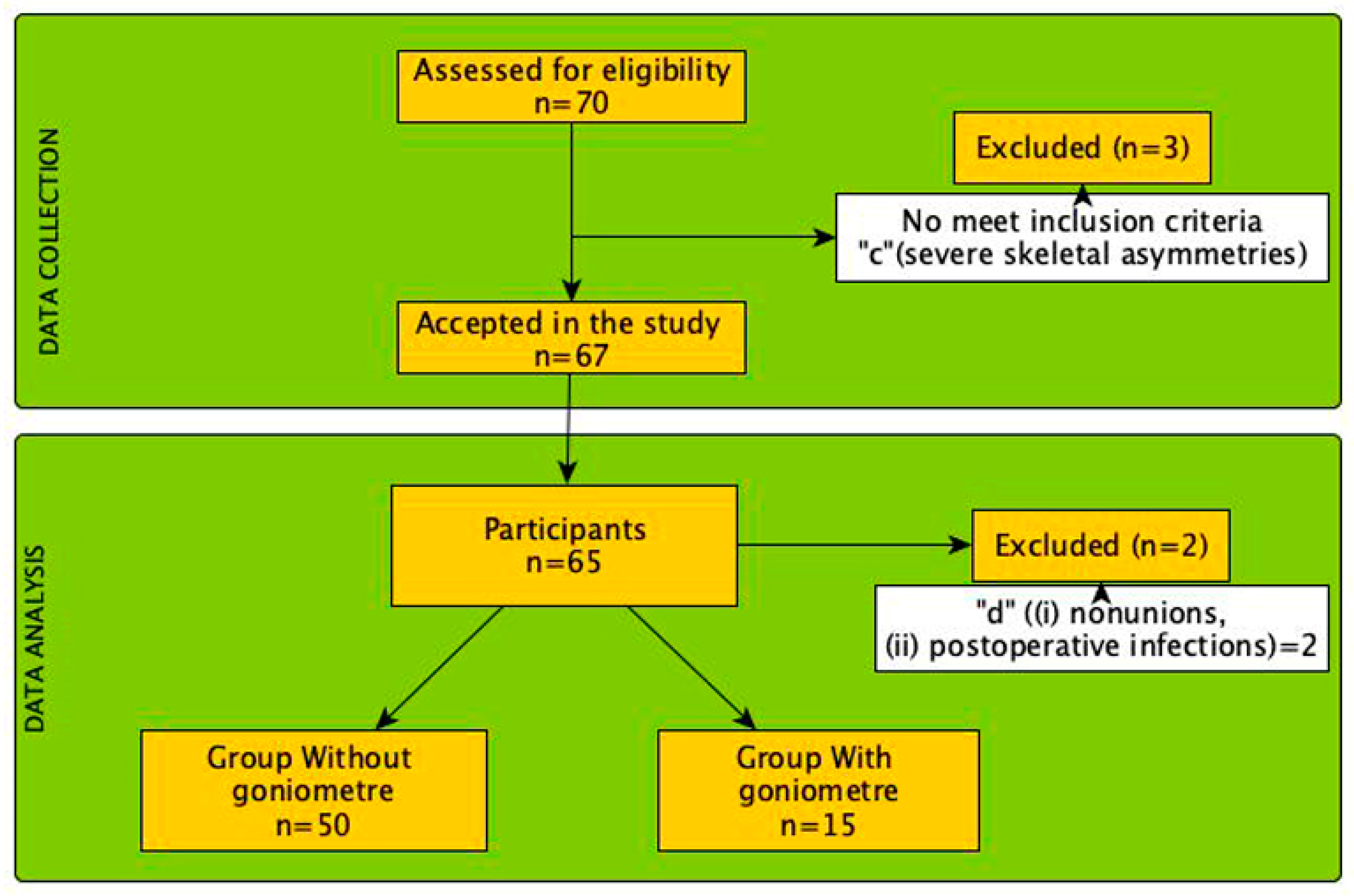
2.1. Study Design
2.2. Sample Size
2.3. Participants
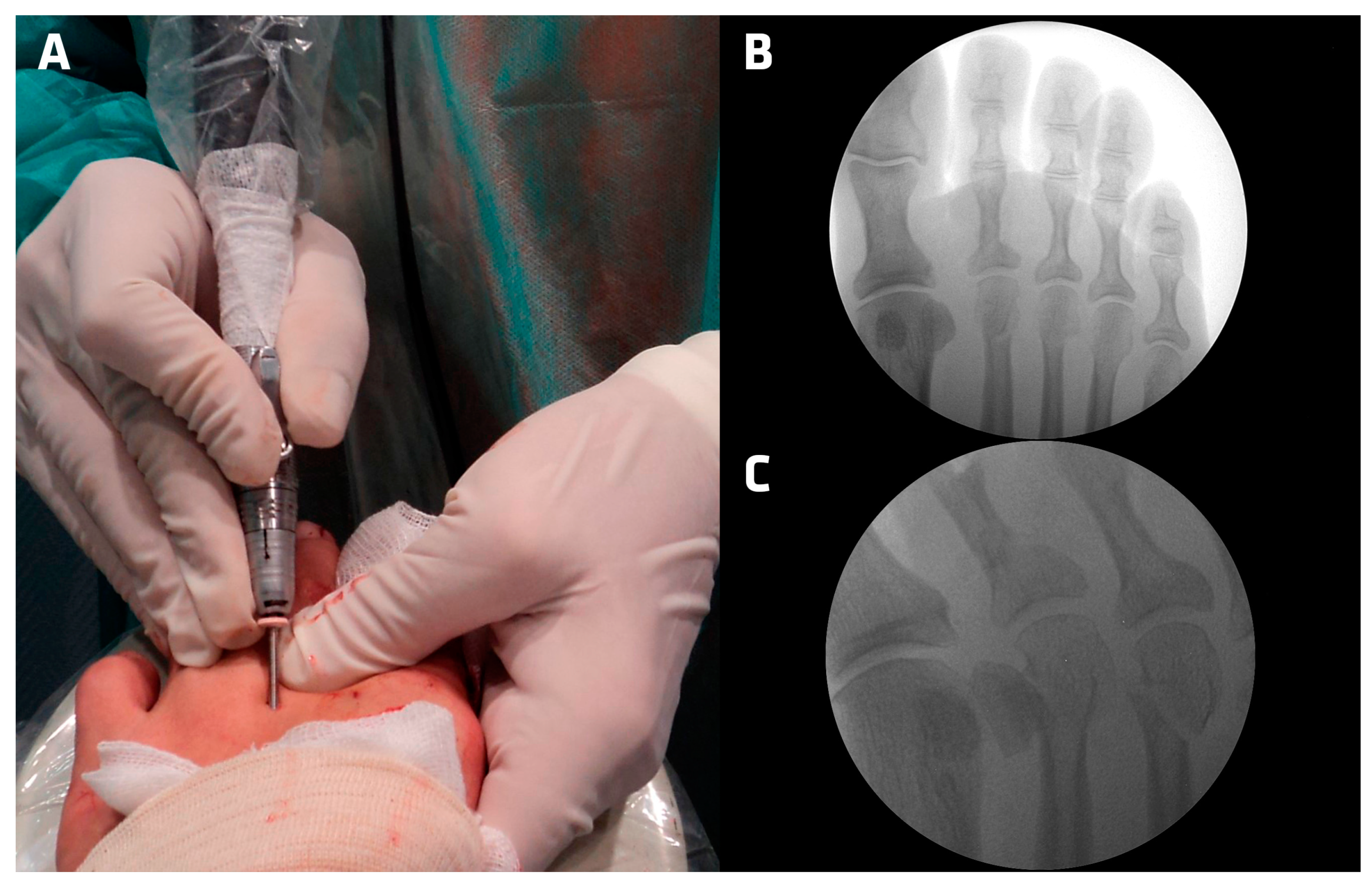
2.4. Surgical Technique—Minimally Invasive Intracapsular Metaphyseal Osteotomy (DICMO)
2.5. Digital Goniometer Subgroup
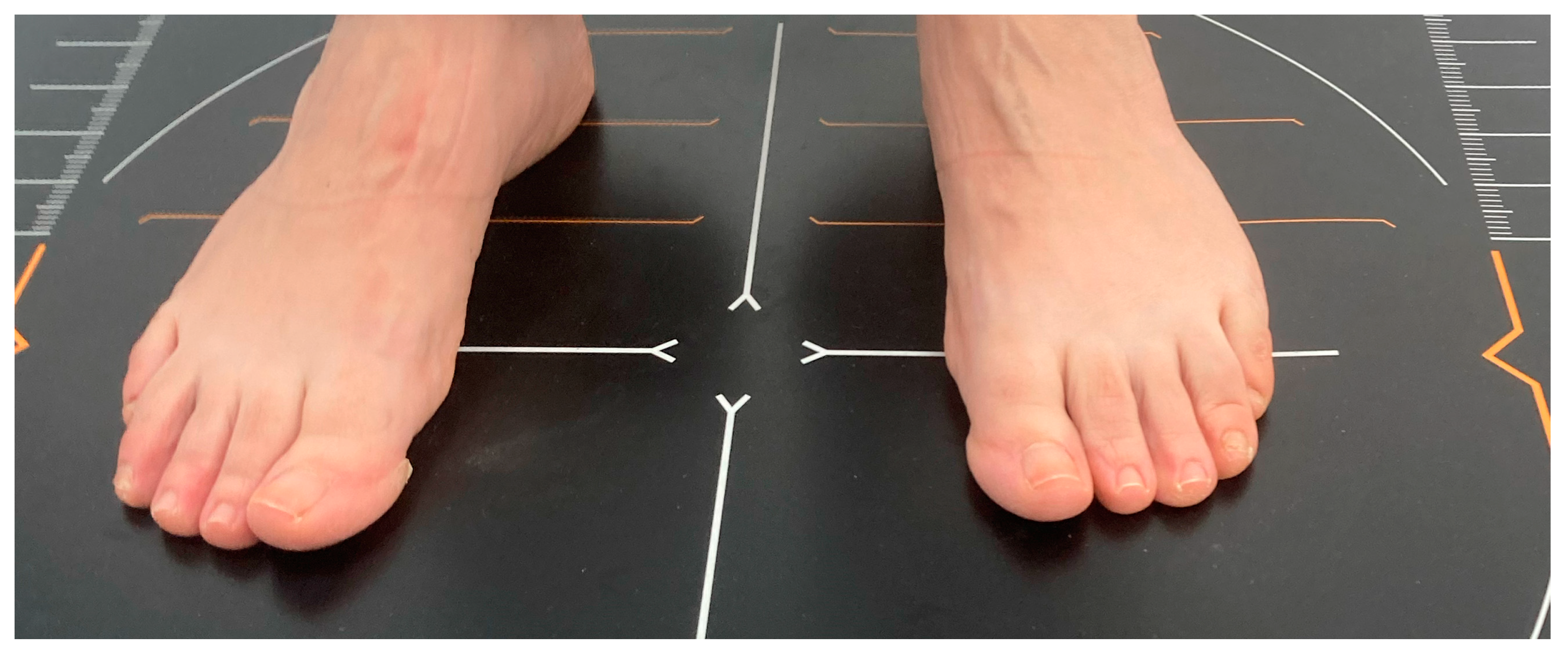
2.6. Assessment Baropodometric Study
2.7. Assessment AOFAS-MTP-IP and VAS
2.8. Statistical Analysis
3. Results
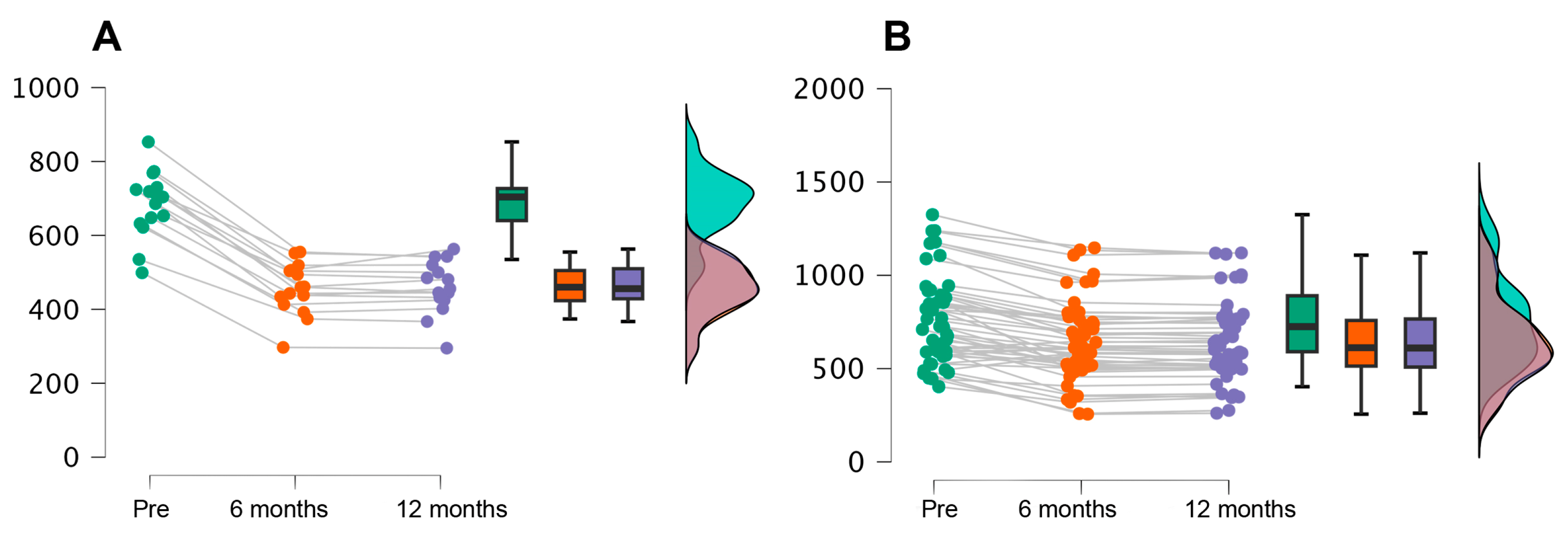
3.1. Plantar Pressures
3.2. AOFAS-MTP-IP Results
3.3. VAS Variable
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vandeputte, G.; Dereymaeker, G.; Steenwerckx, A.; Peeraer, L. The Weil Osteotomy of the Lesser Metatarsals: A Clinical and Pedobarogaphic Follow-up Study. Foot Ankle Int. 2000, 21, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.K.; Roy, N.; Shenolikar, A. Weil Osteotomy of Lesser Metatarsals for Metatarsalgia: A Clinical and Radiological Follow-Up. Foot 2005, 15, 202–205. [Google Scholar] [CrossRef]
- Redfern, D.J.; Vernois, J. Percutaneous Surgery for Metatarsalgia and the Lesser Toes. Foot Ankle Clin. 2016, 21, 527–550. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.; Jordan, M. Minimally Invasive Correction of Lesser Toe Deformities and Treatment of Metatarsalgia. Oper. Orthop. Traumatol. 2018, 30, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T. Percutaneous Forefoot Surgery. Orthop. Traumatol. Surg. Res. 2014, 100, S191–S204. [Google Scholar] [CrossRef] [PubMed]
- Barouk, P.; Dias, M. Lateral Metatarsal Osteotomy. Orthop. Traumatol. Surg. Res. 2024, 110, 103782. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Ayora, Á.; Cuervas-Mons Cantón, M.; Benjumea-Carrasco, A.; Arnal-Burró, J.; Sobrón-Caminero, F.B.; Vaquero, J. Tips, Quips and Pearls: Ultrasound-Guided Distal Metatarsal Minimal Invasive Osteotomy (US-DMMO). Foot Ankle Surg. 2021, 27, 30–34. [Google Scholar] [CrossRef]
- Martínez-Ayora, A.; Cuervas-Mons, M.; Fajardo-Ruiz, A.; Rodríguez-López, T.; Vaquero, J.; Sanz-Ferrando, L. Ultrasound-Guided Distal Minimally Invasive Metatarsal Osteotomies (US-DMMO): A Cadaveric Study about Its Safety and Accuracy. Foot Ankle Surg. 2022, 28, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Vigil, M.; Suarez-Garnacho, S.; Martín, V.; Naranjo-Ruiz, C.; Rodriguez, C. Evaluation of Results after Distal Metatarsal Osteotomy by Minimal Invasive Surgery for the Treatment of Metatarsalgia: Patient and Anatomical Pieces Study. J. Orthop. Surg. Res. 2019, 14, s13018–s13019. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, C.; Stiglitz, Y. Minimally Invasive and Percutaneous Surgery of the Forefoot Current Techniques in 2018. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.D.; Ripoll, P.L.; Golanó, P. Cirugía Percutánea Del Pie: Técnicas Quirúrgicas, Indicaciones, Bases Anatómicas; Masson: Paris, France, 2003; ISBN 9788445812846. [Google Scholar]
- Coillard, J.Y.; Laffenetre, O.; Cermolacce, C.; Determe, P.; Guillo, S.; de Lavigne, C. Percutaneous Treatment of Static Metatarsalgia with Distal Metatarsal Mini-Invasive Osteotomy. In Minimally Invasive Forefoot Surgery in Clinical Practice; Springer: London, UK, 2013; pp. 149–160. [Google Scholar]
- de Prado, M. Minimally Invasive Foot Surgery: To Paradigm Shift. In Minimally Invasive Surgery of the Foot and Ankle; Springer: Berlin, Germany, 2011; pp. 3–11. [Google Scholar]
- De Prado, M.; Cuervas-Mons, M.; Golanó, P.; Vaquero, J. Distal Metatarsal Minimal Invasive Osteotomy (DMMO) for the Treatment of Metatarsalgia. Tech. Foot Ankle Surg. 2016, 15, 12–18. [Google Scholar] [CrossRef]
- Laffenêtre, O. Distal Minimally Invasive Metatarsal Osteotomy. In Minimally Invasive Foot and Ankle Surgery. A Percutaneous Approach, 1st ed.; Vulcano, E., Johnson, A.H., Schipper, O.N., Eds.; Wolters Kluwer Health: Waltham, MA, USA, 2023; pp. 77–86. [Google Scholar]
- Laffenêtre, O.; Perera, A. Distal Minimally Invasive Metatarsal Osteotomy (“DMMO” Procedure). Foot Ankle Clin. 2019, 24, 615–625. [Google Scholar] [CrossRef]
- Laffenêtre, O.; Dalmau-Pastor, M.; Bauer, T. Osteotomías de Los Metatarsianos Laterales. EMC Técnicas Quirúrgicas Ortopedia Y Traumatología 2019, 11, 1–10. [Google Scholar] [CrossRef]
- Nieto García, E.; Rodríguez Baeza, A.; González Castillo, A.M. Estructuras Anatómicas Implicadas En La Práctica de La Cirugía de Mínima Incisión Del Pie; Glosa: Madrid, Spain, 2009. [Google Scholar]
- Giannini, S.; Faldini, C.; Vannini, F.; Digennaro, V.; Bevoni, R.; Luciani, D. The Minimally Invasive Osteotomy “S.E.R.I.” (Simple, Effective, Rapid, Inexpensive) for Correction of Bunionette Deformity. Foot Ankle Int. 2008, 29, 282–286. [Google Scholar] [CrossRef]
- Giannini, S.; Faldini, C.; Nanni, M.; Di Martino, A.; Luciani, D.; Vannini, F. A Minimally Invasive Technique for Surgical Treatment of Hallux Valgus: Simple, Effective, Rapid, Inexpensive (SERI). Int. Orthop. 2013, 37, 1805–1813. [Google Scholar] [CrossRef]
- Ruggieri, P.; Uccioli, L.; Mazzotti, A.; Arceri, A.; Artioli, E.; Langone, L.; Zielli, S.O.; Martini, B.; Traina, F.; Faldini, C.; et al. Hallux Valgus Plantar Pressure Distribution before and after a Distal Metatarsal Osteotomy. J. Clin. Med. 2024, 13, 1731. [Google Scholar] [CrossRef]
- Biz, C.; Ruggieri, P. Distal Metatarsal Osteotomies for Chronic Plantar Diabetic Foot Ulcers. Foot Ankle Clin. 2022, 27, 545–566. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef]
- Fernández-Vizcaino, C.; Nieto-García, E.; Fernández-Ehrling, N.; Ferrer-Torregrosa, J. Improving the Accuracy of Metatarsal Osteotomies in Minimally Invasive Foot Surgery Using a Digital Inclinometer: Preliminary Study. Sensors 2024, 24, 1022. [Google Scholar] [CrossRef]
- Paget, L.D.A.; Sierevelt, I.N.; Tol, J.L.; Kerkhoffs, G.M.M.J.; Reurink, G. The Completely Patient-Reported Version of the American Orthopaedic Foot and Ankle Society (AOFAS) Score: A Valid and Reliable Measurement for Ankle Osteoarthritis. J. ISAKOS 2023, 8, 345–351. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; Nunley, J.A.; Myerson, M.S.; Sanders, M. Clinical Rating Systems for the Ankle-Hindfoot, Midfoot, Hallux, and Lesser Toes. Foot Ankle Int. 1994, 15, 349–353. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the Visual Analog Scale for Measurement of Acute Pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Hopkins, W. A Scale of Magnitudes for Effect Statistics. Available online: http://www.sportsci.org/resource/stats/effectmag.html (accessed on 9 September 2021).
- Snyder, J.; Owen, J.; Wayne, J.; Adelaar, R. Plantar Pressure and Load in Cadaver Feet After a Weil or Chevron Osteotomy. Foot Ankle Int. 2005, 26, 158–165. [Google Scholar] [CrossRef]
- Khalafi, A.; Landsman, A.S.; Lautenschlager, E.P.; Kelikian, A.S. Plantar Forefoot Pressure Changes After Second Metatarsal Neck Osteotomy. Foot Ankle Int. 2005, 26, 550–555. [Google Scholar] [CrossRef]
- Trask, D.J.; Ledoux, W.R.; Whittaker, E.C.; Roush, G.C.; Sangeorzan, B.J. Second Metatarsal Osteotomies for Metatarsalgia: A Robotic Cadaveric Study of the Effect of Osteotomy Plane and Metatarsal Shortening on Plantar Pressure. J. Orthop. Res. 2014, 32, 385–393. [Google Scholar] [CrossRef]
- Malhotra, K.; Joji, N.; Mordecai, S.; Rudge, B. Minimally Invasive Distal Metaphyseal Metatarsal Osteotomy (DMMO) for Symptomatic Forefoot Pathology—Short to Medium Term Outcomes from a Retrospective Case Series. Foot 2019, 38, 43–49. [Google Scholar] [CrossRef]
- Biz, C.; Kuete, W.; Kanah, T.; Corradin, M.; Zornetta, A.; Petretta, I.; Ruggieri, P. The Treatment of Metatarsalgia by Minimally Invasive Surgery: A Cross-Sectional Study. Foot Ankle Surg. 2017, 23, 147. [Google Scholar] [CrossRef]
- Haque, S.; Kakwani, R.; Chadwick, C.; Davies, M.B.; Blundell, C.M. Outcome of Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Lesser Toe Metatarsalgia. Foot Ankle Int. 2015, 37, 58–63. [Google Scholar] [CrossRef]
- de Prado, M. Complications in Minimally Invasive Foot Surgery. Fuß Sprunggelenk 2013, 11, 83–94. [Google Scholar] [CrossRef]
- Henry, J.; Besse, J.L.; Fessy, M.H. Distal Osteotomy of the Lateral Metatarsals: A Series of 72 Cases Comparing the Weil Osteotomy and the DMMO Percutaneous Osteotomy. Orthop. Traumatol. Surg. Res. 2011, 97, S57–S65. [Google Scholar] [CrossRef]
- Magnan, B.; Bonetti, I.; Negri, S.; Maluta, T.; Dall’Oca, C.; Samaila, E. Percutaneous Distal Osteotomy of Lesser Metatarsals (DMMO) for Treatment of Metatarsalgia with Metatarsophalangeal Instability. Foot Ankle Surg. 2018, 24, 400–405. [Google Scholar] [CrossRef]
- Vulcano, E.; Johnson, H. Oliver Schipper Minimally Invasive Foot and Ankle Surgery. In Minimally Invasive Foot and Ankle Surgery; Lippincott Williams & Wilkins: Philadelphia, PA, USA; ISBN 9781975198701.
- Krenn, S.; Albers, S.; Bock, P.; Mansfield, C.; Chraim, M.; Trnka, H.-J.J. Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy of the Lesser Toes: Learning Curve. Foot Ankle Spec. 2018, 11, 263–268. [Google Scholar] [CrossRef]
- Harris, J.; Betts, R.; Smith, T.W.D. A Prospective Clinical and Pedobarographic Evaluation of Metatarsal Shortening for the Treatment of Intractable Plantar Keratosis. Foot Ankle Surg. 1998, 4, 201–205. [Google Scholar] [CrossRef]
- Leigheb, M.; Vaiuso, D.; Rava, E.; Pogliacomi, F.; Samaila, E.M.; Grassi, F.A.; Sabbatini, M. Translation, Cross-Cultural Adaptation, Reliability, and Validation of the Italian Version of the American Orthopaedic Foot and Ankle Society-Meta Tarsophalangealinterphalangeal Scale (AOFAS-MTP-IP) for the Hallux. Acta Biomed. 2019, 90, 118–126. [Google Scholar] [CrossRef]
- SooHoo, N.F.; Shuler, M.; Fleming, L.L. Evaluation of the Validity of the AOFAS Clinical Rating Systems by Correlation to the SF-36. Foot Ankle Int. 2003, 24, 50–55. [Google Scholar] [CrossRef]
- Nieto-García, E.; Ferrer-Torregrosa, J.; Ramírez-Andrés, L.; Nieto-González, E.; Martinez-Nova, A.; Barrios, C. The Impact of Associated Tenotomies on the Outcome of Incomplete Phalangeal Osteotomies for Lesser Toe Deformities. J. Orthop. Surg. Res. 2019, 14, 1–10. [Google Scholar] [CrossRef]
- Biz, C.; Corradin, M.; Kanah, W.T.K.; Dalmau-Pastor, M.; Zornetta, A.; Volpin, A.; Ruggieri, P. Medium-Long-Term Clinical and Radiographic Outcomes of Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Central Primary Metatarsalgia: Do Maestro Criteria Have a Predictive Value in the Preoperative Planning for This Percutaneous Technique? Biomed. Res. Int. 2018, 2018, 1947024. [Google Scholar] [CrossRef]
- Naranjo-Ruiz, C.; Martínez-Nova, A.; Canel-Pérez, M.d.l.Á.; López-Vigil, M.; Ferrer-Torregrosa, J.; Barrios, C. Influence of Foot Type on the Clinical Outcome of Minimally Invasive Surgery for Metatarsalgia. A Prospective Pilot Study. Front. Surg. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring Acute Postoperative Pain Using the Visual Analog Scale: The Minimal Clinically Important Difference and Patient Acceptable Symptom State. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Participants (n= 65) | Non Goniometer (n = 50) | Goniometer (n = 15) | p-Value |
|---|---|---|---|---|
| Age (mean ± sd) | 54.69 ± 13.75 | 55.06 ± 13.63 | 53.47 ± 14.57 | 0.70 |
| Height (m) | 1.64 ± 0.09 | 1.64 ± 0.09 | 1.63 ± 0.08 | 0.64 |
| Weight (Kg) | 66.58 ± 10.22 | 66.28 ± 10.49 | 67.57 ± 9.56 | 0.67 |
| Body mass index (kg/m2) | 24.85 ± 3.60 | 24.62 ± 3.44 | 25.60 ± 4.10 | 0.36 |
| Sex, n (%) | ||||
| Men | 17 (26.15%) | 14 (21.54%) | 3 (4.62%) | 0.54 |
| Women | 48 (73.85%) | 36 (55.38%) | 12 (18.46%) | |
| Laterality, n (%) | ||||
| Right | 38 (58.46%) | 28 (43.08%) | 10 (15.38%) | 0.46 |
| Left | 27 (41.54%) | 22 (33.85%) | 5 (7.69%) | |
| Diabetes | 8 (12.3%) | 6 (12%) | 2 (13%) | 0.89 |
| Smoking | 6 (9.23%) | 5 (10%) | 1 (6.67) | 0.70 |
| All Participants (n= 65) | Non Goniometer (n = 50) | Goniometer (n = 15) | |
|---|---|---|---|
| Pressure Previous (g/cm) | 747.63 ± 215.13 | 766.68 ± 237.68 | 684.13 ± 90.73 |
| Pressure 6 months (g/cm) | 601.86 ± 208.06 | 645.58 ± 216.09 | 456.13 ± 69.80 |
| Pressure 12 months (g/cm) | 602.83 ± 206.20 | 645.66 ± 214.36 | 460.07 ± 71.81 |
| Time | Mean | ET | Difference | t | Cohen’s d | p-Value | |
|---|---|---|---|---|---|---|---|
| Group SI | Pre | - | - | - | - | - | - |
| 6 months | −42.96 | 2.06 | −42.96 | −20.85 | −3.72 | <0.001 | |
| 12 months | −49.00 | 2.06 | −49.00 | −23.78 | −4.24 | <0.001 | |
| Group No | Pre | −2.31 | 3.40 | −2.31 | −0.68 | −0.20 | 0.98 |
| 6 months | −43.78 | 3.40 | −41.47 | −12.87 | −3.79 | <0.001 | |
| 12 months | −51.38 | 3.40 | −49.07 | −15.11 | −4.45 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Vizcaino, C.; Naranjo-Ruiz, C.; Fernández-Ehrling, N.; García-Vicente, S.; Nieto-García, E.; Ferrer-Torregrosa, J. Impact of Minimally Invasive Intra-Capsular Metatarsal Osteotomy on Plantar Pressure Decrease: A Cross-Sectional Study. J. Clin. Med. 2024, 13, 2180. https://doi.org/10.3390/jcm13082180
Fernández-Vizcaino C, Naranjo-Ruiz C, Fernández-Ehrling N, García-Vicente S, Nieto-García E, Ferrer-Torregrosa J. Impact of Minimally Invasive Intra-Capsular Metatarsal Osteotomy on Plantar Pressure Decrease: A Cross-Sectional Study. Journal of Clinical Medicine. 2024; 13(8):2180. https://doi.org/10.3390/jcm13082180
Chicago/Turabian StyleFernández-Vizcaino, Carlos, Carmen Naranjo-Ruiz, Nadia Fernández-Ehrling, Sergio García-Vicente, Eduardo Nieto-García, and Javier Ferrer-Torregrosa. 2024. "Impact of Minimally Invasive Intra-Capsular Metatarsal Osteotomy on Plantar Pressure Decrease: A Cross-Sectional Study" Journal of Clinical Medicine 13, no. 8: 2180. https://doi.org/10.3390/jcm13082180
APA StyleFernández-Vizcaino, C., Naranjo-Ruiz, C., Fernández-Ehrling, N., García-Vicente, S., Nieto-García, E., & Ferrer-Torregrosa, J. (2024). Impact of Minimally Invasive Intra-Capsular Metatarsal Osteotomy on Plantar Pressure Decrease: A Cross-Sectional Study. Journal of Clinical Medicine, 13(8), 2180. https://doi.org/10.3390/jcm13082180