
Integrating the PD-L1 Prognostic Biomarker in Non-Muscle Invasive Bladder Cancer in Clinical Practice—A Comprehensive Review on State-of-the-Art Advances and Critical Issues

 ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
1.1. Clinical Aspects of Non-Muscle Invasive Bladder Cancer (NMIBC)
1.2. PD-L1: Biological Mechanisms
1.3. PD-L1 in Bladder Cancer: Clinical Implications
1.4. Prognostic Role of PD-L1 in BC: The Big Picture
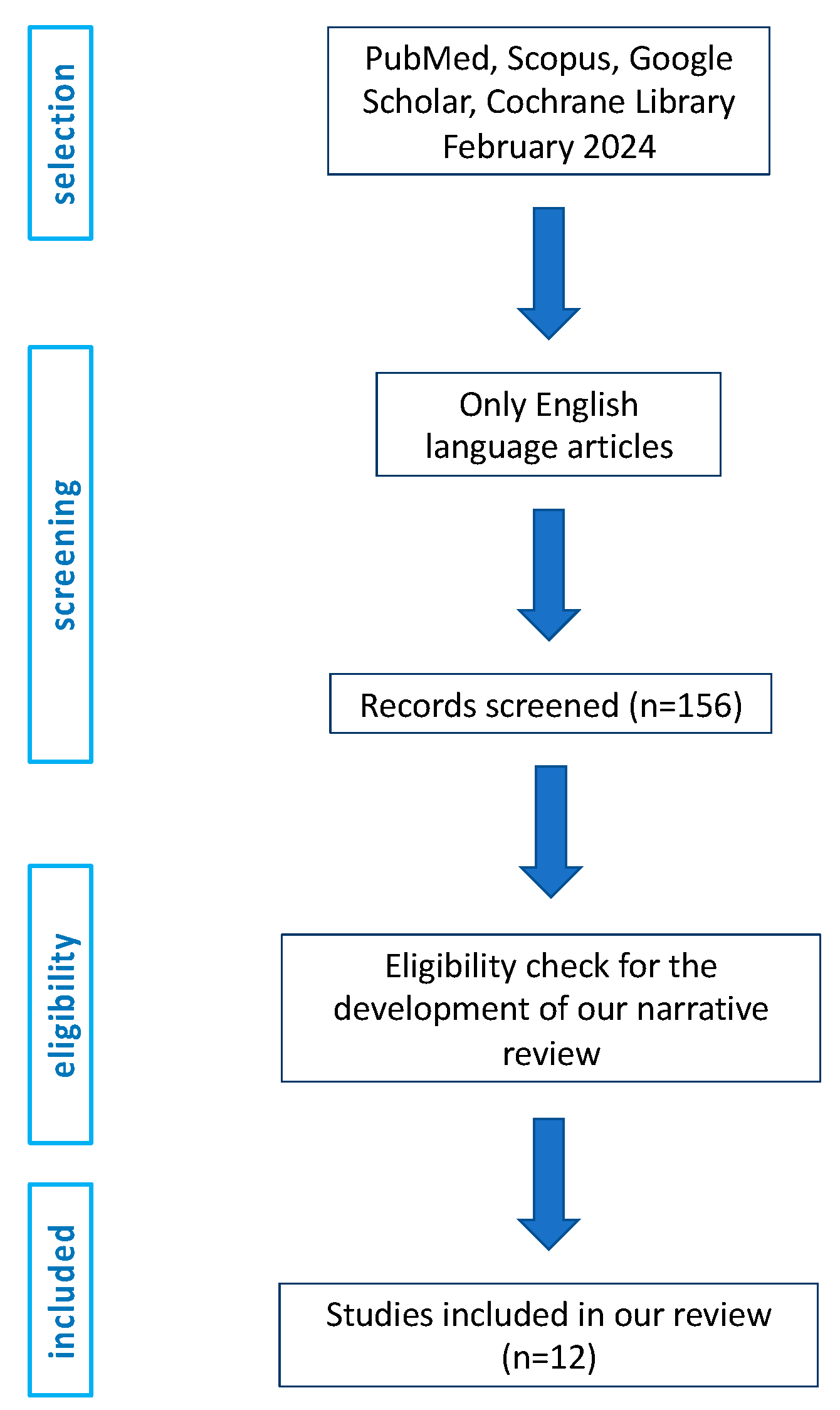
2. Materials and Methods
3. Results and Discussion
3.1. Prognostic Role of PD-L1 in NMIBC: Main Findings
3.2. Prognostic Role of PD-L1 in NMIBC: Focus on BCG Immunotherapy
3.3. PD-L1 Expression on Immune Cells and Interaction with BCG Immunotherapy
3.4. Critical Issues in PD-L1 Assessment
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BC | Bladder cancer |
| BCG | Bacillus Calmette-Guérin |
| CIS | Carcinoma in situ |
| CSS | Cancer-specific survival |
| DFS | Disease-free survival |
| EMT | Epithelial-mesenchymal transition |
| HER2 | Human Epidermal Growth Factor Receptor 2 |
| HR-NMIBC | High-risk non-muscle-invasive bladder cancer |
| IHC | Immunohistochemistry |
| ICI | Immune checkpoint inhibitor |
| IC | Immune cells |
| IL-6 | Interleukin 6 |
| IFN-γ | Interferon γ |
| IFN-α | Interferon α |
| JAK | Janus kinases |
| LN | Lymph node |
| MeSH | Medical Subject Headings |
| MIBC | Muscle-invasive bladder cancer |
| NMIBC | Non-muscle-invasive bladder cancer |
| NLR | Neutrophil-to-lymphocyte ratio |
| OS | Overall survival |
| PD-L1 | Programmed cell death ligand 1 |
| PI3K | Phosphatidylinositol 3-kinases |
| PFS | Progression-free survival |
| re-TURB | re-transurethral resection of the bladder |
| RT-PCR | Reverse transcriptase-polymerase chain reaction |
| RFS | Recurrence-free survival |
| STAT3 | Signal transducer and activator of transcription 3 |
| STAT | Signal transducers and activators of transcription |
| TC | Tumor cells |
| TMA | Tissue microarray |
| TUR | Transurethral resection |
| TURB | Transurethral resection of tumor bladder |
References
- IARC-WHO Global Cancer Observatory. Available online: https://gco.iarc.fr (accessed on 10 February 2024).
- Netto, G.J.; Amin, M.B.; Berney, D.M.; Comperat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization classification of tumors of the urinary system and male genital organs-part B: Prostate and urinary tract tumors. Eur. Urol. 2022, 82, 469–482. [Google Scholar] [CrossRef]
- Compérat, E.; Larré, S.; Roupret, M.; Neuzillet, Y.; Pignot, G.; Quintens, H.; Houéde, N.; Roy, C.; Durand, X.; Varinot, J.; et al. Clinicopathological characteristics of urothelial bladder cancer in patients less than 40 years old. Virchows Arch. 2015, 466, 589–594. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Calò, B.; Chirico, M.; Fortunato, F.; Sanguedolce, F.; Carvalho-Dias, E.; Autorino, R.; Carrieri, G.; Cormio, L. Is Repeat Transurethral Resection Always Needed in High-Grade T1 Bladder Cancer? Front. Oncol. 2019, 9, 465. [Google Scholar] [CrossRef]
- Larsen, E.S.; Nordholm, A.C.; Lillebaek, T.; Holden, I.K.; Johansen, I.S. The epidemiology of bacille Calmette-Guérin infections after bladder instillation from 2002 through 2017: A nationwide retrospective cohort study. BJU Int. 2019, 124, 910–916. [Google Scholar] [CrossRef]
- Sanguedolce, F.; Russo, D.; Mancini, V.; Selvaggio, O.; Calo, B.; Carrieri, G.; Cormio, L. Prognostic and therapeutic role of HER2 expression in micropapillary carcinoma of the bladder. Mol. Clin. Oncol. 2019, 10, 205–213. [Google Scholar] [CrossRef]
- Sanguedolce, F.; Cormio, A.; Massenio, P.; Pedicillo, M.C.; Cagiano, S.; Fortunato, F.; Calò, B.; Di Fino, G.; Carrieri, G.; Bufo, P.; et al. Altered expression of HER-2 and the mismatch repair genes MLH1 and MSH2 predicts the outcome of T1 high-grade bladder cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 637–644. [Google Scholar] [CrossRef]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef]
- Afreen, S.; Dermime, S. The immunoinhibitory B7-H1 molecule as a potential target in cancer: Killing many birds with one stone. Hematol. Oncol. Stem Cell Ther. 2014, 7, 1–17. [Google Scholar] [CrossRef]
- Zou, W.; Wolchok, J.D.; Chen, L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328rv4. [Google Scholar] [CrossRef]
- Riley, J.L. PD-1 signaling in primary T cells. Immunol. Rev. 2009, 229, 114–125. [Google Scholar] [CrossRef]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, H.E.; Cho, N.Y.; Lee, H.S.; Kang, G.H. Characterisation of PD-L1-positive subsets of microsatellite-unstable colorectal cancers. Br. J. Cancer 2016, 115, 490–496. [Google Scholar] [CrossRef]
- Zhang, W.T.; Zhang, J.F.; Zhang, Z.W.; Guo, Y.D.; Wu, Y.; Wang, R.; Wang, L.; Mao, S.; Yao, X. Overexpression of indoleamine 2,3-dioxygenase 1 promotes epithelial–mesenchymal transition by activation of the IL-6/STAT3/PD-L1 pathway in bladder cancer. Transl. Oncol. 2019, 12, 485–492. [Google Scholar] [CrossRef]
- Parsa, A.T.; Waldron, J.S.; Panner, A.; Crane, C.A.; Parney, I.F.; Barry, J.J.; Cachola, K.E.; Murray, J.C.; Tihan, T.; Jensen, M.C.; et al. Loss of tumor suppressor PTEN function increases B7-H1 expression and immunoresistance in glioma. Nat. Med. 2007, 13, 84–88. [Google Scholar] [CrossRef]
- Van Allen, E.M.; Golay, H.G.; Liu, Y.; Koyama, S.; Wong, K.; Taylor-Weiner, A.; Giannakis, M.; Harden, M.; Rojas-Rudilla, V.; Chevalier, A.; et al. Long-term benefit of PD-L1 blockade in lung cancer associated with JAK3 activation. Cancer Immunol. Res. 2015, 3, 855–863. [Google Scholar] [CrossRef]
- Powles, T.; Eder, J.P.; Fine, G.D.; Braiteh, F.S.; Loriot, Y.; Cruz, C.; Bellmunt, J.; Burris, H.A.; Petrylak, D.P.; Teng, S.L.; et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 2014, 515, 558–562. [Google Scholar] [CrossRef]
- Parvez, A.; Choudhary, F.; Mudgal, P.; Khan, R.; Qureshi, K.A.; Farooqi, H.; Aspatwar, A. PD-1 and PD-L1: Architects of immune symphony and immunotherapy breakthroughs in cancer treatment. Front. Immunol. 2023, 14, 1296341. [Google Scholar] [CrossRef]
- Nadal, R.; Valderrama, B.P.; Bellmunt, J. Progress in systemic therapy for advanced-stage urothelial carcinoma. Nat. Rev. Clin. Oncol. 2024, 21, 8–27. [Google Scholar] [CrossRef]
- de Jong, F.C.; Rutten, V.C.; Zuiverloon, T.C.M.; Theodorescu, D. Improving Anti-PD-1/PD-L1 Therapy for Localized Bladder Cancer. Int. J. Mol. Sci. 2021, 22, 2800. [Google Scholar] [CrossRef]
- Huang, S.; Huang, Y.; Li, C.; Liang, Y.; Huang, M.; Luo, R.; Liang, W. Efficacy and safety of neoadjuvant PD-1 inhibitors or PD-L1 inhibitors for muscle invasive bladder cancer: A systematic review and meta-analysis. Front. Immunol. 2024, 14, 1332213. [Google Scholar] [CrossRef]
- Song, M.; Chen, D.; Lu, B.; Wang, C.; Zhang, J.; Huang, L.; Wang, X.; Timmons, C.L.; Hu, J.; Liu, B.; et al. PTEN loss increases PD-L1 protein expression and affects the correlation between PD-L1 expression and clinical parameters in colorectal cancer. PLoS ONE 2013, 8, e65821. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Fay, A.P.; Gray, K.P.; Callea, M.; Ho, T.H.; Albiges, L.; Bellmunt, J.; Song, J.; Carvo, I.; Lampron, M.; et al. PD-L1 expression in nonclear-cell renal cell carcinoma. Ann. Oncol. 2014, 25, 2178–2184. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Kiesel, B.; Widhalm, G.; Rajky, O.; Ricken, G.; Wöhrer, A.; Dieckmann, K.; Filipits, M.; Brandstetter, A.; Weller, M.; et al. Programmed death ligand 1 expression and tumor-infiltrating lymphocytes in glioblastoma. Neuro Oncol. 2015, 17, 1064–1075. [Google Scholar] [CrossRef]
- Riobello, C.; Vivanco, B.; Reda, S.; López-Hernández, A.; García-Inclán, C.; Potes-Ares, S.; Cabal, V.N.; López, F.; Llorente, J.L.; Hermsen, M.A. Programmed death ligand-1 expression as immunotherapeutic target in sinonasal cancer. Head Neck 2018, 40, 818–827. [Google Scholar] [CrossRef]
- Cha, Y.J.; Kim, H.R.; Lee, C.Y.; Cho, B.C.; Shim, H.S. Clinicopathological and prognostic significance of programmed cell death ligand-1 expression in lung adenocarcinoma and its relationship with p53 status. Lung Cancer 2016, 97, 73–80. [Google Scholar] [CrossRef]
- Jiang, D.; Xu, Y.Y.; Li, F.; Xu, B.; Zhang, X.G. The role of B7-H1 in gastric carcinoma: Clinical significance and related mechanism. Med. Oncol. 2014, 31, 268. [Google Scholar] [CrossRef]
- Zhao, L.W.; Li, C.; Zhang, R.L.; Xue, H.G.; Zhang, F.X.; Zhang, F.; Gai, X.D. B7-H1 and B7-H4 expression in colorectal carcinoma: Correlation with tumor FOXP3(+) regulatory T-cell infiltration. Acta Histochem. 2014, 116, 1163–1168. [Google Scholar] [CrossRef]
- Gao, H.L.; Liu, L.; Qi, Z.H.; Xu, H.X.; Wang, W.Q.; Wu, C.T.; Zhang, S.R.; Xu, J.Z.; Ni, Q.X.; Yu, X.J. The clinicopathological and prognostic significance of PD-L1 expression in pancreatic cancer: A meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 95–100. [Google Scholar] [CrossRef]
- Inman, B.A.; Sebo, T.J.; Frigola, X.; Dong, H.; Bergstralh, E.J.; Frank, I.; Fradet, Y.; Lacombe, L.; Kwon, E.D. PD-L1 (B7-H1) expression by urothelial carcinoma of the bladder and BCG-induced granulomata: Associations with localized stage progression. Cancer 2007, 109, 1499–1505. [Google Scholar] [CrossRef]
- Boorjian, S.A.; Frank, I.; Lohse, C.M.; Kuntz, S.M.; Leibovich, B.C.; Kwon, E.D.; Frank, I. T cell coregulatory molecule expression in urothelial cell carcinoma: A potential target for therapy. J. Urol. 2008, 179, 265. [Google Scholar] [CrossRef]
- Xylinas, E.; Robinson, B.D.; Kluth, L.A.; Volkmer, B.G.; Hautmann, R.; Küfer, R.; Zerbib, M.; Kwon, E.; Thompson, R.H.; Boorjian, S.A.; et al. Association of T-cell co-regulatory protein expression with clinical outcomes following radical cystectomy for urothelial carcinoma of the bladder. Eur. J. Surg. Oncol. 2014, 40, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Faraj, S.F.; Munari, E.; Guner, G.; Taube, J.; Anders, R.; Hicks, J.; Meeker, A.; Schoenberg, M.; Bivalacqua, T.; Drake, C.; et al. Assessment of tumoral PD-L1 expression and intratumoral CD8+ T cells in urothelial carcinoma. Urology 2015, 85, 703e1–703e6. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, J.; Wada, Y.; Matsumoto, K.; Azuma, M.; Kikuchi, K.; Ueda, S. Overexpression of B7-H1 (PD-L1) significantly associates with tumor grade and postoperative prognosis in human urothelial cancers. Cancer Immunol. Immunol. 2007, 56, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Boorjian, S.A.; Sheinin, Y.; Crispen, P.L.; Farmer, S.A.; Lohse, C.M.; Kuntz, S.M.; Leibovich, B.C.; Kwon, E.D.; Frank, I. T-cell coregulatory molecule expression in urothelial cell carcinoma: Clinicopathologic correlations and association with survival. Clin. Cancer Res. 2008, 14, 4800–4808. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Heidegger, I.; Fritz, J.; Danzl, M.; Sprung, S.; Zelger, B.; Brunner, A.; Pircher, A. PD-L1 expression in bladder cancer and metastasis and its influence on oncologic outcome after cystectomy. Oncotarget. 2017, 8, 66849–66864. [Google Scholar] [CrossRef]
- Sharma, P.; Retz, M.; Siefker-Radtke, A.; Baron, A.; Necchi, A.; Bedke, J.; Plimack, E.R.; Vaena, D.; Grimm, M.O.; Bracarda, S.; et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (Check-Mate 275): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017, 18, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Erlmeier, F.; Seitz, A.K.; Hatzichristodoulou, G.; Stecher, L.; Retz, M.; Gschwend, J.E.; Weichert, W.; Kübler, H.R.; Horn, T. The role of PD-L1 expression and intratumoral lymphocytes in response to perioperative chemotherapy for urothelial carcinoma. Bladder Cancer 2016, 2, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Mullane, S.A.; Werner, L.; Fay, A.P.; Callea, M.; Leow, J.J.; Taplin, M.E.; Choueiri, T.K.; Hodi, F.S.; Freeman, G.J.; et al. Association of PD-L1 expression on tumor-infiltrating mononuclear cells and overall survival in patients with urothelial carcinoma. Ann. Oncol. 2015, 26, 812–817. [Google Scholar] [CrossRef]
- Wen, Y.; Chen, Y.; Duan, X.; Zhu, W.; Cai, C.; Deng, T.; Zeng, G. The clinicopathological and prognostic value of PD-L1 in urothelial carcinoma: A meta-analysis. Clin. Exp. Med. 2019, 19, 407–416. [Google Scholar] [CrossRef]
- Ding, X.; Chen, Q.; Yang, Z.; Li, J.; Zhan, H.; Lu, N.; Chen, M.; Yang, Y.; Wang, J.; Yang, D. Clinicopathological and prognostic value of PD-L1 in urothelial carcinoma: A meta-analysis. Cancer Manag. Res. 2019, 11, 4171–4184. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Sun, J.; Wang, L.; Li, Z.; Wang, L.; Li, Z. Prognostic and Clinicopathological Significance of PD-L1 in Patients With Bladder Cancer: A Meta-Analysis. Front. Pharmacol. 2019, 10, 962. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ye, T.; Yang, X.; Lv, P.; Wu, X.; Zhou, H.; Lu, H.; Tang, K.; Ye, Z. Predictive and Prognostic Role of PD-L1 in Urothelial Carcinoma Patients with Anti-PD-1/PD-L1 Therapy: A Systematic Review and Meta-Analysis. Dis. Markers 2020, 2020, 8375348. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Song, L.; Zhu, H.; Liu, Q.; Wang, D. Prognostic value of programmed cell death ligand-1 expression in patients with bladder urothelial carcinoma undergoing radical cystectomy: A meta-analysis. Front. Immunol. 2022, 13, 986911. [Google Scholar] [CrossRef] [PubMed]
- Semeniuk-Wojtaś, A.; Modzelewska, M.; Poddębniak-Strama, K.; Kołaczyńska, S.; Lubas, A.; Górnicka, B.; Jakieła, A.; Stec, R. CD4, CD20 and PD-L1 as Markers of Recurrence in Non-Muscle-Invasive Bladder Cancer. Cancers 2023, 15, 5529. [Google Scholar] [CrossRef] [PubMed]
- Roumiguié, M.; Compérat, E.; Chaltiel, L.; Nouhaud, F.X.; Verhoest, G.; Masson-Lecomte, A.; Colin, P.; Audenet, F.; Houédé, N.; Larré, S.; et al. PD-L1 expression and pattern of immune cells in pre-treatment specimens are associated with disease-free survival for HR-NMIBC undergoing BCG treatment. World J. Urol. 2021, 39, 4055–4065. [Google Scholar] [CrossRef] [PubMed]
- Eich, M.L.; Chaux, A.; Guner, G.; Taheri, D.; Mendoza Rodriguez, M.A.; Rodriguez Peña, M.D.C.; Baras, A.S.; Hahn, N.M.; Drake, C.; Sharma, R.; et al. Tumor immune microenvironment in non-muscle-invasive urothelial carcinoma of the bladder. Hum. Pathol. 2019, 89, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.; Wirtz, R.M.; Pfannstil, C.; Wach, S.; Stoehr, R.; Breyer, J.; Erlmeier, F.; Günes, C.; Nitschke, K.; Weichert, W.; et al. A multicenter round robin test of PD-L1 expression assessment in urothelial bladder cancer by immunohistochemistry and RT-qPCR with emphasis on prognosis prediction after radical cystectomy. Oncotarget 2018, 9, 15001–15014. [Google Scholar] [CrossRef] [PubMed]
- Martınez, R.; Tapia, G.; De Muga, S.; Hernandez, A.; Cao, M.G.; Teixido, C.; Urrea, V.; García, E.; Pedreño-López, S.; Ibarz, L.; et al. Combined assessment of peritumoral Th1/Th2 polarization peripheral immunity as a new biomarker in the prediction of BCG response in patients with high-risk, NMIBC. Oncoimmunology 2019, 8, 1602460. [Google Scholar] [CrossRef]
- Wankowicz, S.A.M.; Werner, L.; Orsola, A.; Novak, J.; Bowden, M.; Choueiri, T.K.; de Torres, I.; Morote, J.; Freeman, G.J.; Signoretti, S.; et al. Differential Expression of PD-L1 in High Grade T1 vs Muscle Invasive Bladder Carcinoma and its Prognostic Implications. J. Urol. 2017, 198, 817–823. [Google Scholar] [CrossRef]
- Blinova, E.; Enikeev, D.; Roshchin, D.; Samyshina, E.; Deryabina, O.; Tertychnyy, A.; Blinov, D.; Kogan, E.; Dudina, M.; Barakat, H.; et al. Relapse-Free Survival and PD-L1 Expression in First High- and Low-Grade Relapsed Luminal, Basal and Double-Negative P53-Mutant Non-Muscular Invasive Bladder Cancer Depending on Previous Chemo- and Immunotherapy. Cancers 2020, 12, 1316. [Google Scholar] [CrossRef] [PubMed]
- Civriz, A.H.; Teke, K.; Akdas, E.M.; Dillioglugil, O.; Vural, C.; Yaprak Bayrak, B. The prognostic value of expressions of STAT3, PD-L1, and PD-L2 in Ta/T1 urothelial carcinoma before and after BCG treatment. Urol. Oncol. 2023, 41, 486.e1–486.e13. [Google Scholar] [CrossRef]
- van der Horst, G.; Bos, L.; van der Pluijm, G. Epithelial plasticity, cancer stem cells, and the tumor-supportive stroma in bladder carcinoma. Mol. Cancer Res. 2012, 10, 995–1009. [Google Scholar] [CrossRef]
- Huang, Y.; Zhang, S.D.; McCrudden, C.; Chan, K.W.; Lin, Y.; Kwok, H.F. The prognostic significance of PD-L1 in bladder cancer. Oncol. Rep. 2015, 33, 3075–3084. [Google Scholar] [CrossRef]
- Powles, T.; Duran, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Powles, T.; O’Donnell, P.H.; Massard, C.; Arkenau, H.T.; Friedlander, T.W.; Hoimes, C.J.; Lee, J.L.; Ong, M.; Sridhar, S.S.; Vogelzang, N.J.; et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: Updated results from a phase 1/2 OPEN-LABEL STUDY. JAMA Oncol. 2017, 3, e172411. [Google Scholar] [CrossRef]
- Delcourt, C.; Gemival, P.; Nouhaud, F.X.; Gobet, F.; Gillibert, A.; Ferlicot, S.; Sabourin, J.C.; Irani, J.; Pfister, C. Clinical interest of PD-L1 immuno-histochemistry expression as a predictive factor of Bacillus Calmette Guerin (BCG) efficacy in refractory high-risk non-muscle-invasive bladder cancer (NMIBC). World J. Urol. 2020, 38, 1517–1524. [Google Scholar] [CrossRef]
- Aydin, A.M.; Baydar, D.E.; Hazir, B.; Babaoglu, B.; Bilen, C.Y. Prognostic significance of pre- and post-treatment PD-L1 expression in patients with primary high-grade non-muscle-invasive bladder cancer treated with BCG immunotherapy. World J. Urol. 2020, 38, 2537–2545. [Google Scholar] [CrossRef]
- Kates, M.; Matoso, A.; Choi, W.; Baras, A.S.; Daniels, M.J.; Lombardo, K.; Brant, A.; Mikkilineni, N.; McConkey, D.J.; Kamat, A.M.; et al. Adaptive immune resistance to intravesical BCG in non-muscle invasive bladder cancer: Implications for prospective BCG unresponsive trials. Clin. Cancer Res. 2020, 26, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Pierconti, F.; Raspollini, M.R.; Martini, M.; Larocca, L.M.; Bassi, P.F.; Bientinesi, R.; Baroni, G.; Minervini, A.; Petracco, G.; Pini, G.M.; et al. PD-L1 expression in bladder primary in situ urothelial carcinoma: Evaluation in BCG-unresponsive patients and BCG responders. Virchows Arch. 2020, 477, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, A.; Umemoto, S.; Yokose, T.; Nakamura, Y.; Yoshihara, M.; Shoji, K.; Wada, S.; Miyagi, Y.; Kishida, T.; Sasada, T. Enhanced expression of PD-L1 in non-muscle-invasive bladder cancer after treatment with Bacillus Calmette-Guerin. Oncotarget 2018, 25, 34066–34078. [Google Scholar] [CrossRef]
- Kamat, A.M.; Shore, N.; Hahn, N.; Alanee, S.; Nishiyama, H.; Shariat, S.; Nam, K.; Kapadia, E.; Frenkl, T.; Steimberg, G. KEYNOTE-676: Phase III study of BCG and pembrolizumab for persistent/recurrent high-risk NMIBC. Future Oncol. 2020, 16, 507–516. [Google Scholar] [CrossRef]
- A Phase III Randomized, Open-Label, Multi-Center, Global Study of Durvalumab and Bacillus Calmette-Guerin (BCG) Administered as Combination Therapy Versus BCG Alone in High-Risk, BCG Naïve Non-Muscle Invasive Bladder Cancer Patients (POTOMAC) EudraCT Number: L2017-002979-26. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-002979-26/SK (accessed on 14 September 2023).
- An Open Label, Randomized, Phase III Trial, Evaluating Efficacy of Atezolizumab in Addition to One Year BCG (Bacillus Calmette-Guérin) Bladder Instillation in BCG-Naive Patients with High-Risk Non-Muscle Invasive Bladder Cancer. Eudract Number: 2017-004512-19. Available online: https://www.clinicaltrialsregister.eu/ctr-search/trial/2017-004512-19/ES (accessed on 14 September 2023).
- Nowak, Ł.; Krajewski, W.; Poterek, A.; Śliwa, A.; Zdrojowy, R. The prognostic value of programmed cell death protein ligand 1 in patients with non-muscle-invasive bladder cancer treated with bacille Calmette-Guérin immunotherapy: Current status. Arab J. Urol. 2020, 19, 67–70. [Google Scholar] [CrossRef]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef]
- Miller, E.J.; Galsky, M.D. Precision Medicine in Urothelial Carcinoma: Current Markers to Guide Treatment and Promising Future Directions. Curr. Treat. Options Oncol. 2023, 24, 1870–1888. [Google Scholar] [CrossRef]
- Goutas, D.; Palamaris, K.; Stofas, A.; Politakis, N.; Despotidi, A.; Giannopoulou, I.; Goutas, N.; Vlachodimitropoulos, D.; Kavantzas, N.; Lazaris, A.C.; et al. Immunohistochemical Study of Bladder Cancer Molecular Subtypes and Their Association with PD-L1 Expression. Cancers 2022, 15, 188. [Google Scholar] [CrossRef]
- Breyer, J.; Wirtz, R.M.; Otto, W.; Erben, P.; Worst, T.S.; Stoehr, R.; Eckstein, M.; Denzinger, S.; Burger, M.; Hartmann, A. High PDL1 mRNA expression predicts better survival of stage pT1 non-muscle-invasive bladder cancer (NMIBC) patients. Cancer Immunol. Immunother. 2018, 67, 403–412. [Google Scholar] [CrossRef]
- Agarwal, A.; Agrawal, U.; Verma, S.; Mohanty, N.K.; Saxena, S. Serum Th1 and Th2 cytokine balance in patients of superficial transitional cell carcinoma of bladder pre- and post-intravesical combination immunotherapy. Immunopharmacol. Immunotoxicol. 2010, 32, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Gruenbacher, G.; Culig, Z.; Brunner, A.; Fuchs, D.; Fritz, J.; Gander, H.; Rahm, A.; Thurnher, M. Intratumoral Th2 predisposition combines with an increased Th1 functional phenotype in clinical response to intravesical BCG in bladder cancer. Cancer Immunol. Immunother. 2017, 66, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, M.F.; Schneider, A.K.; Cesson, V.; Dartiguenave, F.; Lucca, I.; Jichlinski, P.; Nardelli-Haefliger, D.; Derré, L. Conventional and PD-L1-expressing Regulatory T Cells are Enriched During BCG Therapy and may Limit its Efficacy. Eur. Urol. 2018, 74, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Paver, E.C.; Cooper, W.A.; Colebatch, A.J.; Ferguson, P.M.; Hill, S.K.; Lum, T.; Shin, J.S.; O’Toole, S.; Anderson, L.; Scolyer, R.A.; et al. Programmed death ligand-1 (PD-L1) as a predictive marker for immunotherapy in solid tumours: A guide to immunohistochemistry implementation and interpretation. Pathology 2021, 53, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Rouanne, M.; Radulescu, C.; Adam, J.; Allory, Y. PD-L1 testing in urothelial bladder cancer: Essentials of clinical practice. World J. Urol. 2021, 39, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Rouanne, M.; Lebret, T.; Radulescu, C.; Adam, J. Re: Differential Expression of PD-L1 in High Grade T1 vs. Muscle Invasive Bladder Carcinoma and its Prognostic Implications: Wankowicz, S.A.M.; Werner, L.; Orsola, A.; Novak, J.; Bowden, M.; Choueiri, T.K.; de Torres, I.; Morote, J.; Freeman, G.J.; Signoretti, S.; Bellmunt, J. J. Urol. 2017, 198, 817–823. J. Urol. 2018, 199, 854–856. [Google Scholar]
- Yu, S.L.; Hsiao, Y.J.; Cooper, W.A.; Choi, Y.L.; Avilés-Salas, A.; Chou, T.Y.; Coudry, R.; Raskin, G.A.; Fox, S.B.; Huang, C.C.; et al. The Ring Study: An international comparison of PD-L1 diagnostic assays and their interpretation in non-small cell lung cancer, head and neck squamous cell cancer and urothelial cancer. Pathology 2023, 55, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Tretiakova, M.; Fulton, R.; Kocherginsky, M.; Long, T.; Ussakli, C.; Antic, T.; Gown, A. Concordance study of PD-L1 expression in primary and metastatic bladder carcinomas: Comparison of four commonly used antibodies and RNA expression. Mod. Pathol. 2018, 31, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Zajac, M.; Boothman, A.M.; Ben, Y.; Gupta, A.; Jin, X.; Mistry, A.; Sabalos, C.; Nielsen, A.; Manriquez, G.; Barker, C.; et al. Analytical validation and clinical utility of an immunohistochemical programmed death ligand-1 diagnostic assay and combined tumor and immune cell scoring algorithm for durvalumab in urothelial carcinoma. Arch. Pathol. Lab. Med. 2019, 143, 722–731. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Bladder Cancer. Version 1.2024—30 January 2024. Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 17 February 2024).
- de Jong, J.J.; Stoop, H.; Boormans, J.L.; van Leenders, G.J.L.H. PD-L1 expression in urothelial bladder cancer varies more among specimen types than between companion assays. Virchows Arch. 2021, 479, 705–713. [Google Scholar] [CrossRef]
- Rijnders, M.; van der Veldt, A.A.M.; Zuiverloon, T.C.M.; Grünberg, K.; Thunnissen, E.; de Wit, R.; van Leenders, G.J.L.H. PD-L1 anti-body comparison in urothelial carcinoma. Eur. Urol. 2019, 75, 538–540. [Google Scholar] [CrossRef]
- Wang, C.; Hahn, E.; Slodkowska, E.; Eskander, A.; Enepekides, D.; Higgins, K.; Vesprini, D.; Liu, S.K.; Downes, M.R.; Xu, B. Reproducibility of PD-L1 immunohistochemistry interpretation across various types of genitourinary and head/neck carcinomas, antibody clones, and tissue types. Hum. Pathol. 2018, 82, 131–139. [Google Scholar] [CrossRef]
- Eckstein, M.; Erben, P.; Kriegmair, M.C.; Worst, T.S.; Weiß, C.A.; Wirtz, R.M.; Wach, S.; Stoehr, R.; Sikic, D.; Geppert, C.I.; et al. Performance of the Food and Drug Administration/EMA-approved programmed cell death ligand-1 assays in urothelial carcinoma with emphasis on therapy stratification for first-line use of atezolizumab and pembrolizumab. Eur. J. Cancer 2019, 106, 234–243. [Google Scholar] [CrossRef]
- Hodgson, A.; Slodkowska, E.; Jungbluth, A.; Liu, S.K.; Vesprini, D.; Enepekides, D.; Higgins, K.; Katabi, N.; Xu, B.; Downes, M.R. PD-L1 immunohistochemistry assay concordance in urothelial carcinoma of the bladder and hypopharyngeal squamous cell carcinoma. Am. J. Surg. Pathol. 2018, 42, 1059–1066. [Google Scholar] [CrossRef]
- Lawson, N.L.; Dix, C.I.; Scorer, P.W.; Stubbs, C.J.; Wong, E.; Hutchinson, L.; McCall, E.J.; Schimpl, M.; DeVries, E.; Walker, J.; et al. Mapping the binding sites of antibodies utilized in programmed cell death ligand-1 predictive immunohistochemical assays for use with immuno-oncology therapies. Mod. Pathol. 2019. [Google Scholar] [CrossRef]
- McLaughlin, J.; Han, G.; Schalper, K.A.; Carvajal-Hausdorf, D.; Pele-kanou, V.; Rehman, J.; Velcheti, V.; Herbst, R.; LoRusso, P.; Rimm, D.L. Quantitative assessment of the heterogeneity of PD-L1 expression in non-small-cell lung cancer. JAMA Oncol. 2016, 2, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Kubon, J.; Sikic, D.; Eckstein, M.; Weyerer, V.; Stöhr, R.; Neumann, A.; Keck, B.; Wullich, B.; Hartmann, A.; Wirtz, R.M.; et al. Analysis of CXCL9, PD1 and PD-L1 mRNA in Stage T1 Non-Muscle Invasive Bladder Cancer and Their Association with Prognosis. Cancers 2020, 12, 2794. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Prevalence | Significant Correlation | Independent Predictor | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | N# Cases | Stage | Grade | Antibody Clone | Scoring System/Cut-off | TC | IC | TC | IC | TC | IC |
| [46] | 55 | Tis, Ta, T1 | LG, HG | 28-8 | <1%—low; 1–5%—moderate; >5%—high expression | low 84%, moderate 10%, high 6% | low 34%, moderate 34%, high 32% | time to cystectomy, many recurrences | age, depth of bladder wall invasion | shorter RFS (high and moderate vs. low expression) | |
| [47] | 140 | Ta, T1 | HG | SP142, SP263, 28-8, E1L3N | ≥5% IC (SP142), ≥25% TC-IC (SP263), ROC curve (E1L3N) | recurrence/progression (E1L3N), pT1 stage (E1L3N, SP263) | pT1 stage (all antibodies) | shorter DFS (E1L3N) | |||
| [48] | 61 | CIS, Ta | LG, HG | E1L3N | 1%, 5% | LG, lower recurrence risk | higher stage | ||||
| [50] | 22 | T1 | HG | SP142 | >1% | 9% | 73% | low peripheral blood lymphocytes | |||
| [51] | 140 | T1 | HG | 405.9A11 | 5%(TC) | 4% | 34.3% | muscle invasion | |||
| [52] | 240 | CIS, T1 | LG, HG | SP263 | ≥25% TC-IC | shorter RFS in luminal tumors after no or BCG treatment | |||||
| [53] | 59 | Ta, T1 | LG, HG | E1L3N | TCS, ICS, CS | 18.6% | - | T1 | |||
| [58] | 186 | CIS, Ta, T1 | E1L3N | >1%, >5% | 18.8% | 32.3% | immune infiltrate density, increased PD-L1 after BCG | ||||
| [59] | 117 | CIS, Ta, T1 | HG | SP142 | >1% | 46.2% | refractory recurrence (inverse association) | ||||
| [60] | 63 | CIS, Ta, T1 | HG | 22C3, SP142 | >5%, CPS | non responsiveness to BCG | |||||
| [61] | 60 | CIS | 22C3, SP142, SP263 | TPS, IC | 16.7% | 38.3% | failure to BCG therapy/recurrence (22C3) | ||||
| [62] | 22 | Tis, Ta, T1 | G2, G3 | E1L3N | IS, PS | 9% | 50% | BCG treatment | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanguedolce, F.; Falagario, U.G.; Zanelli, M.; Palicelli, A.; Zizzo, M.; Busetto, G.M.; Cormio, A.; Carrieri, G.; Cormio, L. Integrating the PD-L1 Prognostic Biomarker in Non-Muscle Invasive Bladder Cancer in Clinical Practice—A Comprehensive Review on State-of-the-Art Advances and Critical Issues. J. Clin. Med. 2024, 13, 2182. https://doi.org/10.3390/jcm13082182
Sanguedolce F, Falagario UG, Zanelli M, Palicelli A, Zizzo M, Busetto GM, Cormio A, Carrieri G, Cormio L. Integrating the PD-L1 Prognostic Biomarker in Non-Muscle Invasive Bladder Cancer in Clinical Practice—A Comprehensive Review on State-of-the-Art Advances and Critical Issues. Journal of Clinical Medicine. 2024; 13(8):2182. https://doi.org/10.3390/jcm13082182
Chicago/Turabian StyleSanguedolce, Francesca, Ugo Giovanni Falagario, Magda Zanelli, Andrea Palicelli, Maurizio Zizzo, Gian Maria Busetto, Angelo Cormio, Giuseppe Carrieri, and Luigi Cormio. 2024. "Integrating the PD-L1 Prognostic Biomarker in Non-Muscle Invasive Bladder Cancer in Clinical Practice—A Comprehensive Review on State-of-the-Art Advances and Critical Issues" Journal of Clinical Medicine 13, no. 8: 2182. https://doi.org/10.3390/jcm13082182
APA StyleSanguedolce, F., Falagario, U. G., Zanelli, M., Palicelli, A., Zizzo, M., Busetto, G. M., Cormio, A., Carrieri, G., & Cormio, L. (2024). Integrating the PD-L1 Prognostic Biomarker in Non-Muscle Invasive Bladder Cancer in Clinical Practice—A Comprehensive Review on State-of-the-Art Advances and Critical Issues. Journal of Clinical Medicine, 13(8), 2182. https://doi.org/10.3390/jcm13082182