
Trapeziometacarpal Dislocations in Pediatric Age, Is There a Better Treatment? Series of Cases and a Systematic Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
- -
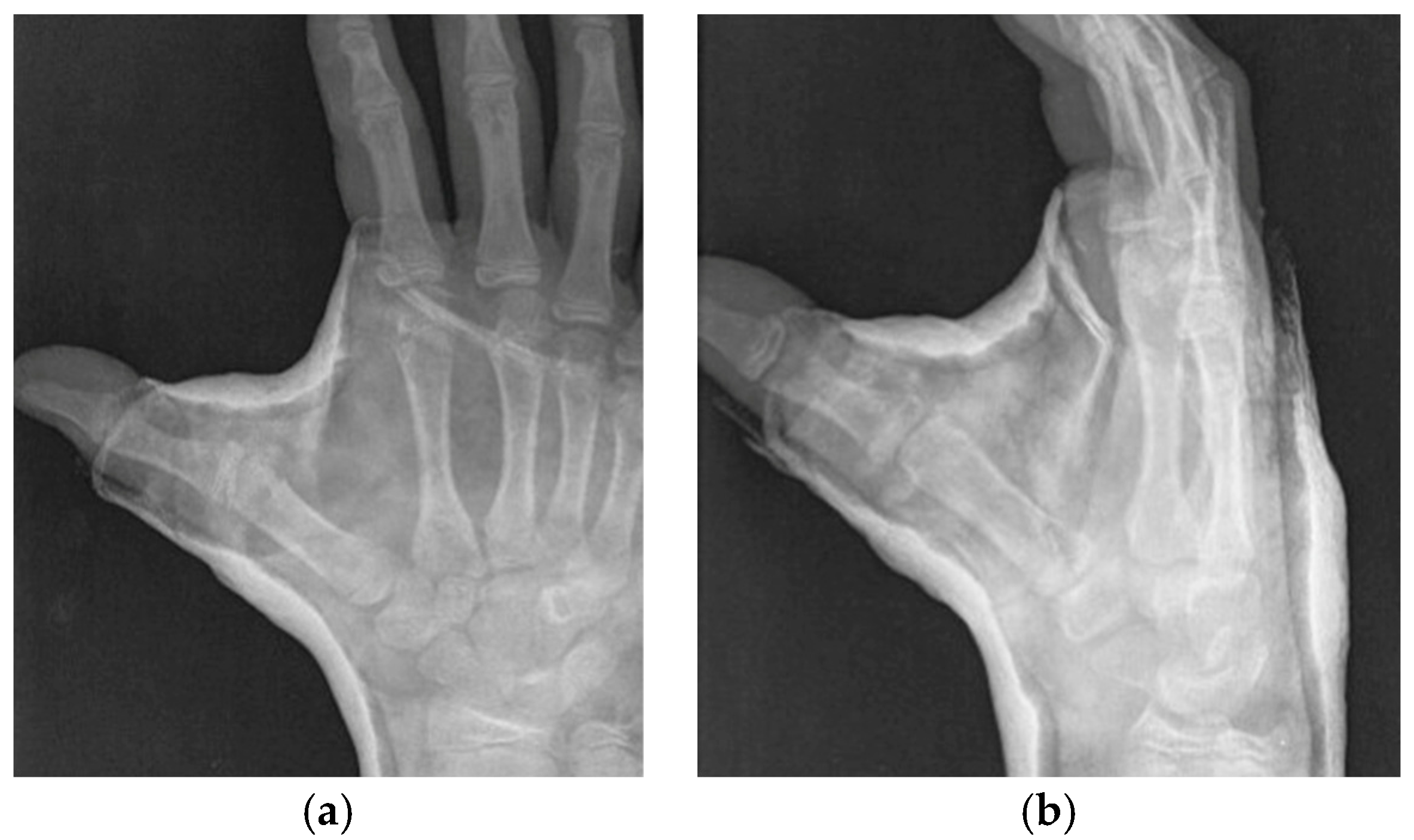
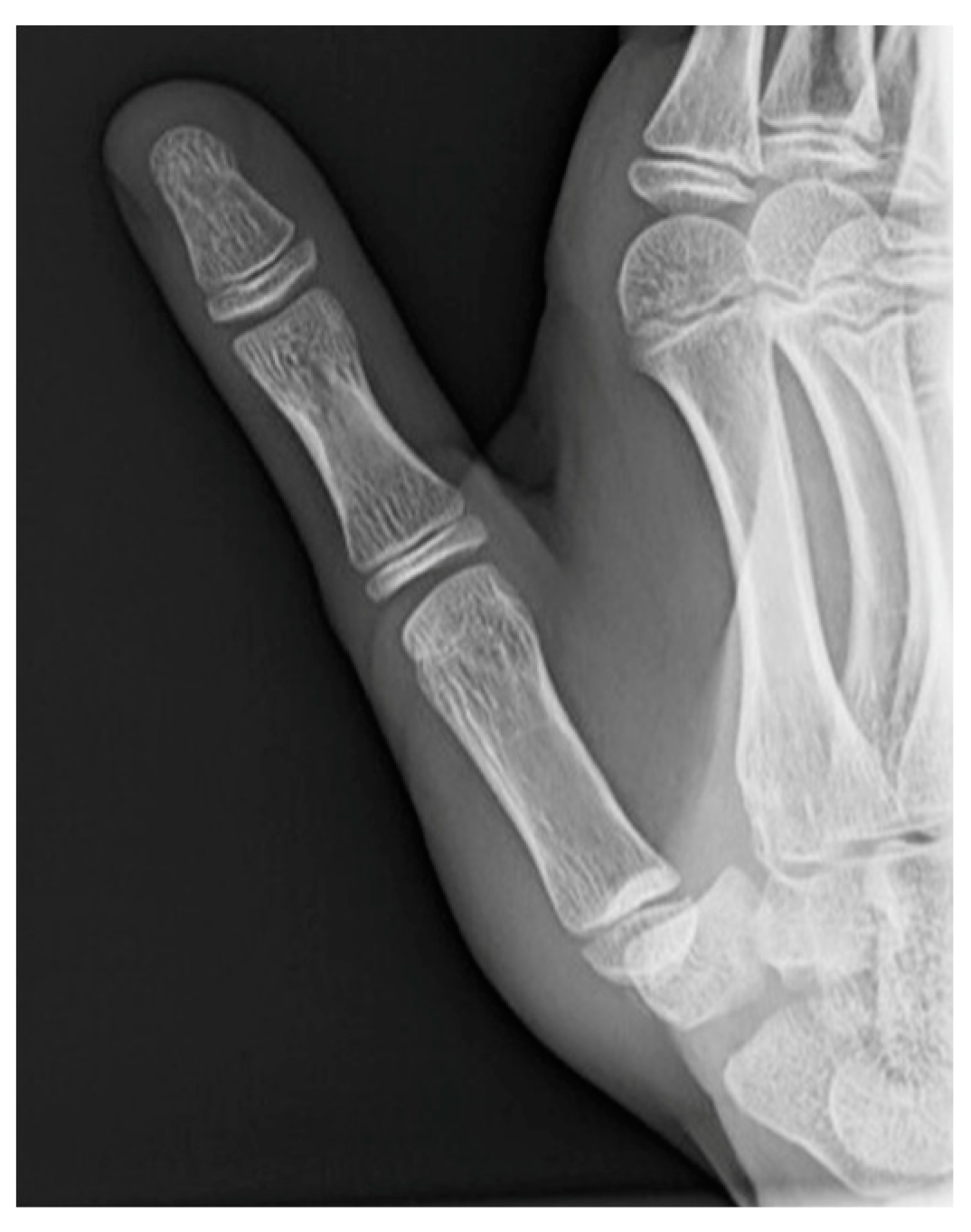
- Roberts projection—strict AP view of the TMC joint. Roberts proposed forced pronation of the wrist and forearm to compensate for the obliquity of the longitudinal axis of the TMC joint in relation to the anatomical axis of the hand. This projection provides a strict profile of the interline of the trapeziometacarpal and scaphotrapezial joints and allows better visualization of the trapezium without carpal superimposition [21] (Figure 2a).
- -
- -
- Placement of hands flat on the floor with legs straight;
- -
- Left knee bent backwards; right knee bent backwards; left elbow bent backwards; left knee bent backwards;
- -
- Left elbow bent backwards; right elbow bent backwards; right elbow bent backwards;
- -
- Right thumb touching the forearm; left thumb touching the forearm;
- -
- Left little finger bent backwards beyond 90 degrees; right little finger bent backwards beyond 90 degrees.
3. Results
3.1. Summary of the Results
3.2. Systematic Literature Review
4. Discussion
5. Conclusions
- -
- Without being able to draw conclusive data, the literature and our series report a higher rate of reluxation associated with closed reduction and plaster cast. On the other hand, there are also good results in our series and in the literature associated with this technique.
- -
- Without being able to draw conclusive data, the literature and our series provide good clinical, radiological, and functional results that are very favorable in patients treated by closed reduction and needle fixation. Authors suggest reduction and pinning for all pediatric/adolescent cases at any time point for the acute and subacute stage.
- -
- Without being able to draw conclusive data, in our series, open reduction and ligamentous reconstruction provide favorable results, but with significantly inferior functional results. Therefore, given this and the risk of physeal injury, we might question the suitability of this technique as a first choice, even in cases of hyperlaxity, in view of the good results of closed techniques.
- -
- It is necessary to rule out hyperlaxity and associated trapezius dysplasia, especially in cases of very low-energy trauma and self-induced or recurrent dislocations. Whether or not there is hyperlaxity/trapezius dysplasia, TMC dislocation must be considered an injury and thus treated. However, it should not be forgotten that the coexistence of associated hyperlaxity or associated trapezius dysplasia could condition the treatment and/or evolution.
- -
- If conservative treatment is chosen, close follow-up radiographs or, better still, CT or MRI is necessary because of the possibility of loss of reduction in initial revisions or misdiagnosis of reduction failure. Also, the literature recommends maintaining the cast for 6 weeks.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mueller, J.J. Carpometacarpal dislocations: Report of five cases and review of the literature. J. Hand Surg. Am. 1986, 11, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, J.; Fitoussi, F. Recurrent posttraumatic trapeziometacarpal joint dislocation in a child: A case report. Hand Surg. Rehabil. 2016, 35, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Varitimidis, S.E.; Sotereanos, D.G. Palmar oblique ligament reconstruction for carpometacarpal joint dislocation in an 11-year-old: A case report. J. Hand Surg. Am. 1999, 24, 505–507. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, P.C.; Smutz, W.P.; Linscheid, R.L.; Cooney, W.P., III; An, K.N. Material properties of the trapezial and trapeziometacarpal ligaments. J. Hand Surg. Am. 2000, 25, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, J.O. Traumatic Dislocations and Instability of the Trapeziometacarpal Joint of the Thumb. Hand Clin. 2006, 22, 365–392. [Google Scholar] [CrossRef]
- Napier, J.R. The form and function of the carpo-metacarpal joint of the thumb. J. Anat. 1955, 89, 362–369. [Google Scholar] [PubMed]
- Eaton, R.G.; Littler, J.W. Ligament reconstruction for the painful thumb carpometacarpal joint. J. Bone Jt. Surg. Am. 1973, 55, 1655–1666. [Google Scholar] [CrossRef]
- Pellegrini, V.D. Osteoarthritis of the trapeziometacarpal joint: The pathophysiology of articular cartilage degeneration. I. Anatomy and pathology of the aging joint. J. Hand Surg. Am. 1991, 16, 967–974. [Google Scholar] [CrossRef]
- Esplugas, M.; Lluch-Bergada, A.; Mobargha, N.; Llusa-Perez, M.; Hagert, E.; Garcia-Elias, M. Trapeziometacarpal Ligaments Biomechanical Study: Implications in Arthroscopy. J. Wrist Surg. 2016, 05, 277–283. [Google Scholar] [CrossRef]
- Lamas, M.R.M.; Llusà, M.; Mustafa, A.; Proubasta, I. Relación de la inestabilidad, la laxitud ligamentosa y la traslación del metacarpiano sobre el trapecio en la aparición de artrosis trapecio metacarpiana: Estudio anatómico. Rev. Iberoam Cirugía La Mano 2013, 41, 40–45. [Google Scholar] [CrossRef][Green Version]
- Strauch, R.J.; Behrman, M.J.; Rosenwasser, M.P. Acute dislocation of the carpometacarpal joint of the thumb: An anatomic and cadaver study. J. Hand Surg. Am. 1994, 19, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Norose, M.; Nimura, A.; Tsutsumi, M.; Fujita, K.; Okawa, A.; Akita, K. Anatomical study for elucidating the stabilization mechanism in the trapeziometacarpal joint. Sci. Rep. 2022, 12, 20790. [Google Scholar] [CrossRef] [PubMed]
- Pagalidis, T.; Kuczynski, K.; Lamb, D.W. Ligamentous Stability of the Base of the Thumb. Hand 1981, 13, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Ladd, A.L.; Lee, J.; Hagert, E. Macroscopic and Microscopic Analysis of the Thumb Carpometacarpal Ligaments. J. Bone Jt. Surg. 2012, 94, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, M.J.; Abouzahr, M.K. Acute dislocation of the trapeziometacarpal joint in a child. J. Hand Surg. Am. 1998, 23, 1097–1099. [Google Scholar] [CrossRef]
- Simonian, P.T.; Trumble, T.E. Traumatic dislocation of the thumb carpometacarpal joint: Early ligamentous reconstruction versus closed reduction and pinning. J. Hand Surg. Am. 1996, 21, 802–806. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Hussain, K.; Higginbotham, D.O.; Tsai, A.G. Management of thumb carpometacarpal joint dislocations: A systematic review. J. Orthop. 2021, 25, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Kapandji, A. Cotation clinique de l’opposition et de la contre-opposition du pouce. Ann. Chir. La Main 1986, 5, 67–73. [Google Scholar] [CrossRef]
- Kurumadani, H.; Kurauchi, K.; Date, S.; Ishii, Y.; Sunagawa, T. Effect of the position of the interphalangeal joint on movements of the trapeziometacarpal joint during thumb opposition. J. Hand Surg. 2022, 47, 495–500. [Google Scholar] [CrossRef]
- Roberts, P. Bulletins et Memoires de la Societe de Radiologie Medicale de France; Societe de Radiologie Medicale de France: Paris, France, 1936. [Google Scholar]
- Billing, L.; Gedela, K.-O. Roentgen Examination of Bennetts Fracture. Acta Radiol. 1952, 38, 471–476. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jupiter, J.; Axelrod, T.; Belsky, M.C. Fractures and dislocations of the hand, metacarpal fractures. In Skeletaltrauma, Basic Science, Management, and Reconstruction, 3rd ed.; Browner, B.D., Ed.; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Taleisnik, J. The Wrist; Churchill Livingston: New York, NY, USA, 1985. [Google Scholar]
- Simpson, M.R. Benign joint hypermobility syndrome: Evaluation, diagnosis, and management. J. Am. Osteopath. Assoc. 2006, 106, 531–536. [Google Scholar] [PubMed]
- Gilula, L. Carpal injuries: Analytic approach and case exercises. Am. J. Roentgenol. 1979, 133, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Peh, W.C.G.; Gilula, L.A. Normal disruption of carpal Arcs. J. Hand Surg. Am. 1996, 21, 561–566. [Google Scholar] [CrossRef]
- Rubin, D.; Louis, A.; Gilula, M.D. In Memoriam. Radiology 2015, 274, 308. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Wright, J.G.; Katz, J.N. Development of the QuickDASH. J. Bone Jt. Surg. 2005, 87, 1038–1046. [Google Scholar] [CrossRef]
- Manterola, C.; Astudillo, P.; Arias, E.; Claros, N. Systematic Reviews of the Literature: What Should be Known About Them. Cirugía Española 2013, 91, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kolaski, K.; Logan, L.R.; Ioannidis, J.P.A. Guidance to best tools and practices for systematic reviews. Syst. Rev. 2023, 12, 96. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Alamino, J.M.; Lopez-Cano, M. Systematic reviews with meta-analysis of clinical trials: Is there enough evidence? Cir. Esp. 2020, 98, 4–8. [Google Scholar] [CrossRef]
- Watt, N.; Hooper, G. Dislocation of the Trapezio-Metacarpal Joint. J. Hand Surg. Am. 1987, 12, 242–245. [Google Scholar] [CrossRef]
- Nusem, I.; Lokiec, F.; Wientroub, S.; Ezra, E. Isolated dislocation of the thumb carpometacarpal joint in a child. J. Pediatr. Orthop. Part B 2001, 10, 158–160. [Google Scholar] [CrossRef]
- Soldado, F.; Mascarenhas, V.V.; Knörr, J. Paediatric trapeziometacarpal dislocation: A case report. J. Hand Surg. 2016, 41, 999–1000. [Google Scholar] [CrossRef] [PubMed]
- Knoedler, T.G.; Condit, K.M.; Zachary, S.V. Recurrent Bilateral Basilar Joint Subluxation in a Teenage Boy. J. Hand Surg. Glob. Online 2021, 3, 363–367. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Sex (Female, Male) | Treatment | Loss of Reduction | CT/MRN | Thumb Intestability | Quick Dash |
|---|---|---|---|---|---|---|---|
| 1 | 12 | F | Closed Reduction + Cast Short arm cast including the thumb 6 weeks | NO | CT at two weeks shows congruency | NO | 52 |
| 2 | 13 | M | Closed Reduction + Cast Short arm cast including the thumb 6 weeks | YES * | CT at two weeks shows congruency | 0 | |
| 3 | 10 | F | Closed Reduction + Cast 1. Short arm cast is intolerated after 3 weeks and changed for a brace. 2. Eaton-Litter procedure | YES | 1. CT at two weeks shows congruency 2. MRN without findings | YES ** | 22 |
| 4 *** | 12 | M | Closed Reduction + KW Closed reduction and fixation with percutaneous K-wires | NO | X-ray shows favorable evolution (follow up at origin center) | NO | 0 |
| Autor | N° Cases | Age (Years) | Sex | Presentation | Treatment | Clinical Results | Follow Up |
|---|---|---|---|---|---|---|---|
| Watt, 1987 [33] | 2 | 14 12 | M M | Same day 7 days | Closed reduction + KW + Cast Closed reduction + Cast | Asymptomatic and stable Painful and unstable * | - - |
| McLaughlin, 1998 [15] | 1 | 11 | M | Same day | Closed reduction + Cast for 6 weeks | Asymptomatic and stable | 14 months |
| Varitimidis, 1999 [3] | 1 | 11 | M | 2 months | Ligament reconstruction + KW + Cast for 6 weeks | Asymptomatic and stable | 18 months |
| Nusem, 2001 [34] | 1 | Closed reduction + Cast | Asymptomatic and stable | ||||
| Gaillard, 2016 [2] | 1 | 8 | F | 8 months | Ligament reconstruction + KW, after traumatic reluxation previously treated by closed methods | Asymptomatic and stable | 12 months |
| Soldado, 2016 [35] | 1 | 10 | F | 3 days | Closed reduction + KW + Cast for 6 weeks | Asymptomatic and stable | 12 months |
| Knoedler, 2021 [36] | 1 | 14 | M | 1 year | Ligament reconstruction + Mini Tightrope, (bilateral TMC) after failed closed methods | Asymptomatic and stable | 5 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Diaz, P.; Perez-Lopez, L.M.; Gutierrez-de la Iglesia, D.; Miron-Dominguez, B.; Domínguez, E.; Perez-Abad, M. Trapeziometacarpal Dislocations in Pediatric Age, Is There a Better Treatment? Series of Cases and a Systematic Review. J. Clin. Med. 2024, 13, 2197. https://doi.org/10.3390/jcm13082197
Martin-Diaz P, Perez-Lopez LM, Gutierrez-de la Iglesia D, Miron-Dominguez B, Domínguez E, Perez-Abad M. Trapeziometacarpal Dislocations in Pediatric Age, Is There a Better Treatment? Series of Cases and a Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2197. https://doi.org/10.3390/jcm13082197
Chicago/Turabian StyleMartin-Diaz, Pablo, Laura M. Perez-Lopez, Diego Gutierrez-de la Iglesia, Beatriz Miron-Dominguez, Enric Domínguez, and Miguel Perez-Abad. 2024. "Trapeziometacarpal Dislocations in Pediatric Age, Is There a Better Treatment? Series of Cases and a Systematic Review" Journal of Clinical Medicine 13, no. 8: 2197. https://doi.org/10.3390/jcm13082197
APA StyleMartin-Diaz, P., Perez-Lopez, L. M., Gutierrez-de la Iglesia, D., Miron-Dominguez, B., Domínguez, E., & Perez-Abad, M. (2024). Trapeziometacarpal Dislocations in Pediatric Age, Is There a Better Treatment? Series of Cases and a Systematic Review. Journal of Clinical Medicine, 13(8), 2197. https://doi.org/10.3390/jcm13082197