
Mid-Term Outcome after Extracorporeal Life Support in Postcardiotomy Cardiogenic Shock: Recovery and Quality of Life

 , , , ,
, , , ,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. ECLS Implantation Strategy and Technique
2.3. Data Acquisition and Baseline Definitions
2.4. Statistical Analysis
3. Results
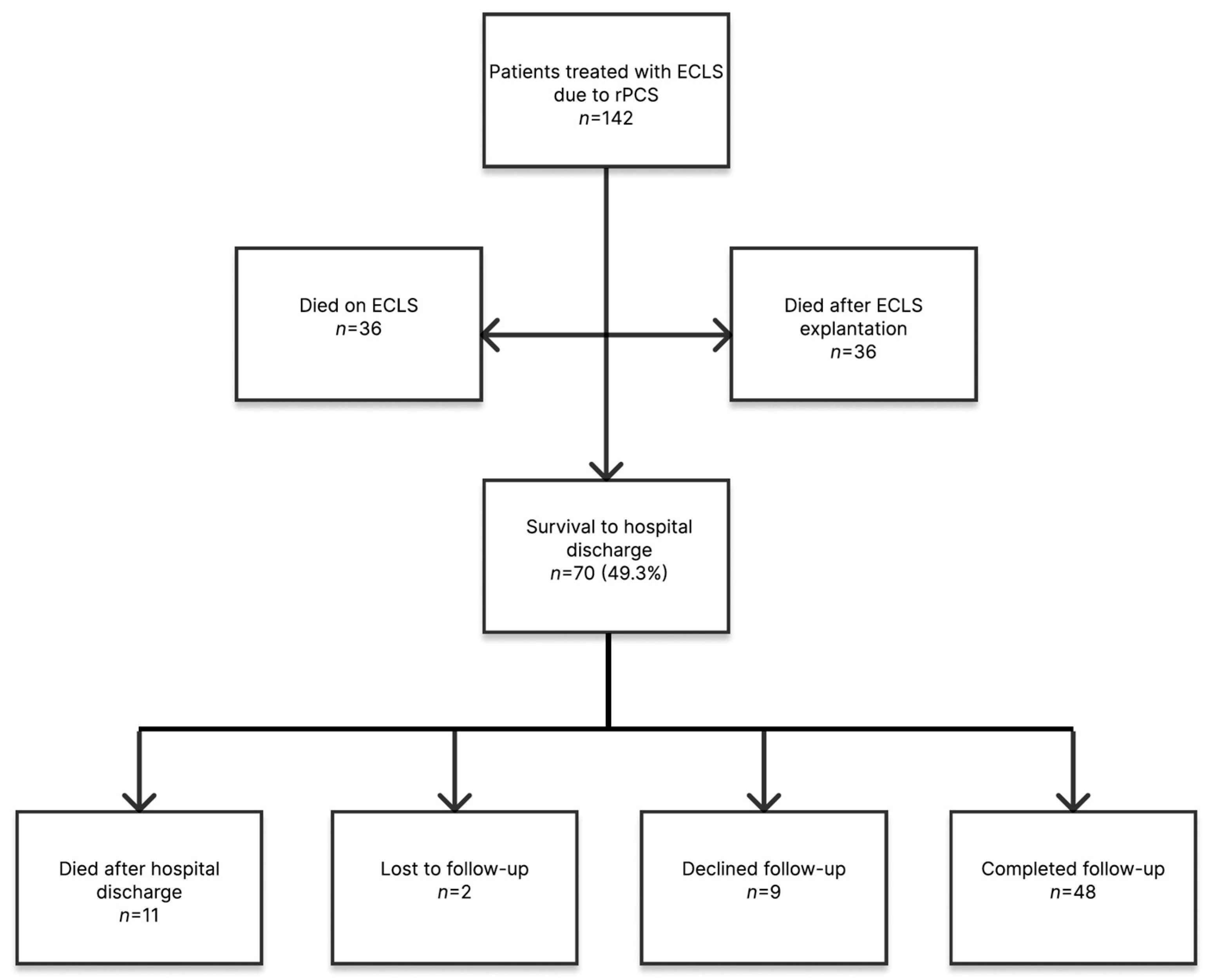
3.1. Early Outcome
3.2. Mid-Term Outcome
3.3. Patient Status at Follow-Up
4. Discussion
- (1)
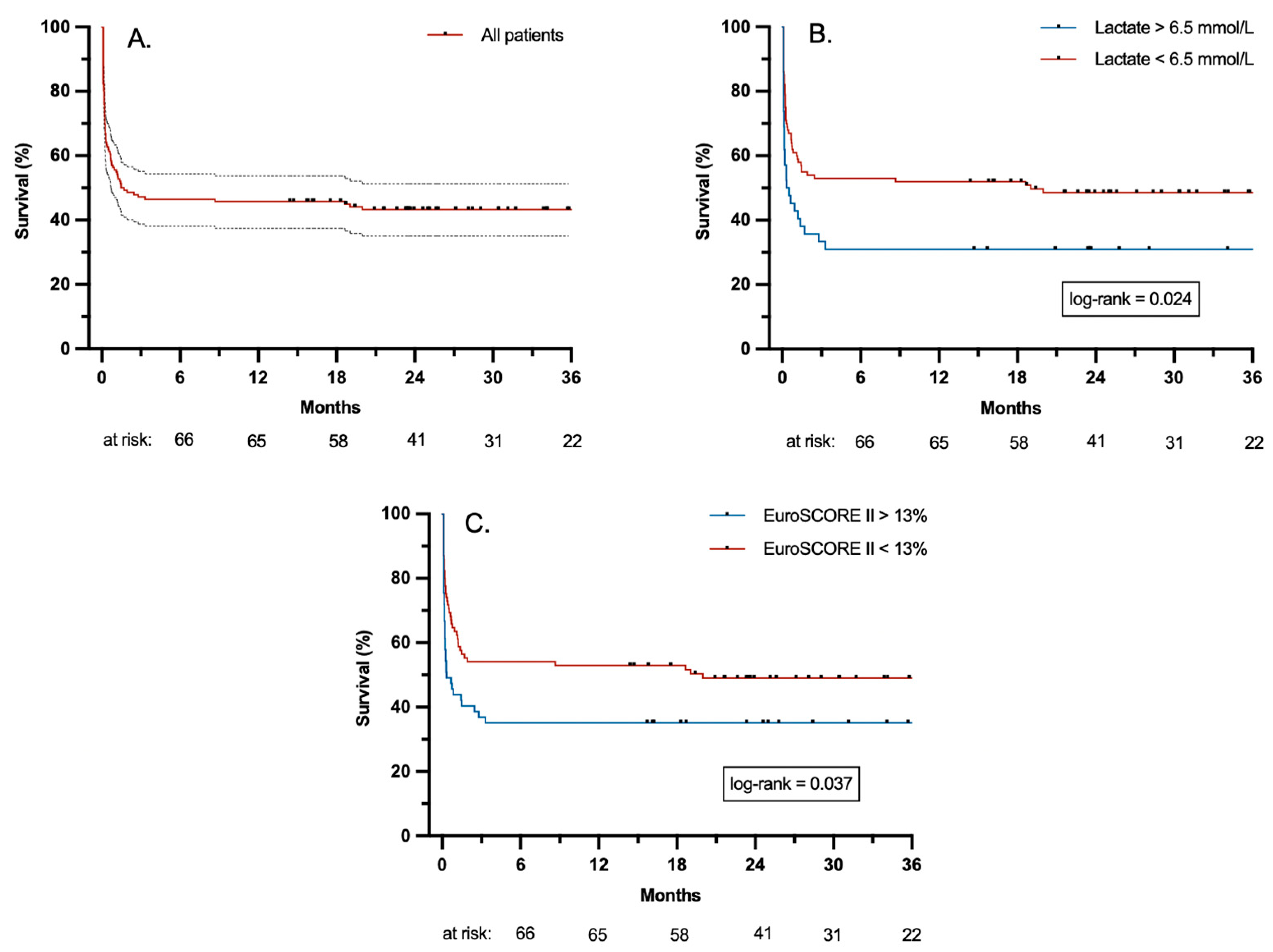
- ECLS therapy for rPCS was associated with high mortality within the first 3 months, but survival rates stabilized thereafter.
- (2)
- Mid-term prognosis was significantly compromised in patients with preoperatively impaired RF, higher EuroSCORE II and pre-ECLS lactate levels as well as longer CPB duration. Furthermore, patients with pre-ECLS lactate levels > 6.5 mmol/L and an EuroSCORE II > 13% had worse outcomes.
- (3)
- HRQoL 2 years after ECLS therapy was decent. In patients with reduced HRQoL, the impairment was mostly attributed to physical restrictions (low PCS scores). Overall recovery was positive and only a small proportion (mostly affecting patients older than 65 years at the time of follow up) suffered from moderate to severe physical disability.
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BIVAD | biventricular assist device |
| BP | bodily pain |
| CPB | cardiopulmonary bypass |
| ECLS | extracorporeal life support |
| GH | general health |
| HRQoL | health-related quality of life |
| ICU | intensive care unit |
| LVAD | left ventricular assist device |
| MCS | mental component summary |
| MH | mental health |
| mRS | modified Rankin Scale |
| PCS | physical component summary |
| PF | physical functioning |
| RE | role emotional |
| RF | renal function |
| RP | role physical |
| rPCS | refractory postcardiotomy cardiogenic shock |
| SF | social functioning |
| SF-36 | 36-Item Short Form Survey |
| VIS | vasoactive-inotropic score |
| VT | vitality |
| VV-ECMO | veno-venous extracorporeal membrane oxygenation |
References
- Lorusso, R.; Whitman, G.; Milojevic, M.; Raffa, G.; McMullan, D.M.; Boeken, U.; Haft, J.; A Bermudez, C.; Shah, A.S.; D’alessandro, D.A. 2020 EACTS/ELSO/STS/AATS expert consensus on post-cardiotomy extracorporeal life support in adult patients. Eur. J. Cardio-Thoracic Surg. 2021, 59, 12–53. [Google Scholar] [CrossRef]
- Rastan, A.J.; Dege, A.; Mohr, M.; Doll, N.; Falk, V.; Walther, T.; Mohr, F.W. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2010, 139, 302–311.e1. [Google Scholar] [CrossRef] [PubMed]
- Biancari, F.; Dalén, M.; Fiore, A.; Ruggieri, V.G.; Saeed, D.; Jónsson, K.; Gatti, G.; Zipfel, S.; Perrotti, A.; Bounader, K.; et al. Multicenter study on postcardiotomy venoarterial extracorporeal membrane oxygenation. J. Thorac. Cardiovasc. Surg. 2020, 159, 1844–1854.e6. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, M.; Alvau, F.; Armoiry, X.; Grinberg, D.; Hugon-Vallet, E.; Koffel, C.; Portran, P.; Scollo, G.; Fellahi, J.L.; Obadia, J.F. Outcomes after extracorporeal life support for postcardiotomy cardiogenic shock. J. Card. Surg. 2019, 34, 74–81. [Google Scholar] [CrossRef]
- Li, C.-L.; Wang, H.; Jia, M.; Ma, N.; Meng, X.; Hou, X.-T. The early dynamic behavior of lactate is linked to mortality in postcardiotomy patients with extracorporeal membrane oxygenation support: A retrospective observational study. J. Thorac. Cardiovasc. Surg. 2015, 149, 1445–1450. [Google Scholar] [CrossRef]
- Schrutka, L.; Rohmann, F.; Binder, C.; Haberl, T.; Dreyfuss, B.; Heinz, G.; Lang, I.M.; Felli, A.; Steinlechner, B.; Niessner, A.; et al. Discriminatory power of scoring systems for outcome prediction in patients with extracorporeal membrane oxygenation following cardiovascular surgery†. Eur. J. Cardio-Thoracic Surg. 2019, 56, 534–540. [Google Scholar] [CrossRef]
- Kowalewski, M.; Zieliński, K.; Brodie, D.; MacLaren, G.; Whitman, G.; Raffa, G.M.; Boeken, U.; Shekar, K.; Chen, Y.-S.; Bermudez, C.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Postcardiotomy Shock—Analysis of the Extracorporeal Life Support Organization Registry. Crit. Care Med. 2021, 49, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Khorsandi, M.; Dougherty, S.; Bouamra, O.; Pai, V.; Curry, P.; Tsui, S.; Clark, S.; Westaby, S.; Al-Attar, N.; Zamvar, V. Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2017, 12, 55. [Google Scholar] [CrossRef]
- Norkiene, I.; Jovaisa, T.; Scupakova, N.; Janusauskas, V.; Rucinskas, K.; Serpytis, P.; Laurusonis, K.; Samalavicius, R. Long-term quality of life in patients treated with extracorporeal membrane oxygenation for postcardiotomy cardiogenic shock. Perfusion 2019, 34, 285–289. [Google Scholar] [CrossRef]
- Meani, P.; Matteucci, M.; Jiritano, F.; Fina, D.; Panzeri, F.; Raffa, G.M.; Kowaleski, M.; Morici, N.; Viola, G.; Sacco, A.; et al. Long-term survival and major outcomes in post-cardiotomy extracorporeal membrane oxygenation for adult patients in cardiogenic shock. Ann. Cardiothorac. Surg. 2019, 8, 116–122. [Google Scholar] [CrossRef]
- Shao, C.; Wang, L.; Yang, F.; Wang, J.; Wang, H.; Hou, X. Quality of Life and Mid-Term Survival in Patients Receiving Extracorporeal Membrane Oxygenation After Cardiac Surgery. ASAIO J. 2022, 68, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Lüsebrink, E.; Stremmel, C.; Stark, K.; Joskowiak, D.; Czermak, T.; Born, F.; Kupka, D.; Scherer, C.; Orban, M.; Petzold, T.; et al. Update on Weaning from Veno-Arterial Extracorporeal Membrane Oxygenation. J. Clin. Med. 2020, 9, 992. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardiothorac. Surg. 2012, 41, 734–745. [Google Scholar] [CrossRef] [PubMed]
- Gaies, M.G.; Gurney, J.G.; Yen, A.H.; Napoli, M.L.; Gajarski, R.J.; Ohye, R.G.; Charpie, J.R.; Hirsch, J.C. Vasoactive–inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr. Crit. Care Med. 2010, 11, 234–238. [Google Scholar] [CrossRef]
- Papadopoulos, N.; Marinos, S.; Ahmad, A.E.-S.; Keller, H.; Meybohm, P.; Zacharowski, K.; Moritz, A.; Zierer, A. Risk factors associated with adverse outcome following extracorporeal life support: Analysis from 360 consecutive patients. Perfusion 2015, 30, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Fux, T.; Holm, M.; Corbascio, M.; Lund, L.H.; van der Linden, J. Venoarterial extracorporeal membrane oxygenation for postcardiotomy shock: Risk factors for mortality. J. Thorac. Cardiovasc. Surg. 2018, 156, 1894–1902.e3. [Google Scholar] [CrossRef] [PubMed]
- Hedley, A.J.; Roberts, M.A.; Hayward, P.A.; Shaw, M.; Matalanis, G.; Buxton, B.F.; Farouque, O.; Ierino, F.L. Impact of chronic kidney disease on patient outcome following cardiac surgery. Heart Lung Circ. 2010, 19, 453–459. [Google Scholar] [CrossRef]
- Mashiko, Y.; Abe, T.; Tokuda, Y.; Oshima, H.; Usui, A. Extracorporeal membrane oxygenation support for postcardiotomy cardiogenic shock in adult patients: Predictors of in-hospital mortality and failure to be weaned from extracorporeal membrane oxygenation. J. Artif. Organs 2020, 23, 225–232. [Google Scholar] [CrossRef]
- Guenther, S.P.W.; Hornung, R.; Joskowiak, D.; Vlachea, P.; Feil, K.; Orban, M.; Peterss, S.; Born, F.; Hausleiter, J.; Massberg, S.; et al. Extracorporeal life support in therapy-refractory cardiocirculatory failure: Looking beyond 30 days. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 607–615. [Google Scholar] [CrossRef]
- Anselmi, A.; Flécher, E.; Corbineau, H.; Langanay, T.; Le Bouquin, V.; Bedossa, M.; Leguerrier, A.; Verhoye, J.-P.; Ruggieri, V.G. Survival and quality of life after extracorporeal life support for refractory cardiac arrest: A case series. J. Thorac. Cardiovasc. Surg. 2015, 150, 947–954. [Google Scholar] [CrossRef]
- Combes, A.; Leprince, P.; Luyt, C.-E.; Bonnet, N.; Trouillet, J.-L.; Léger, P.; Pavie, A.; Chastre, J. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit. Care Med. 2008, 36, 1404–1411. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients n = 142, n (%) | Survivors n = 59,n (%) | Non-Survivors n = 83, n (%) | HR | p-Value |
|---|---|---|---|---|---|
| Male | 96 (67.6) | 39 (66.1) | 57 (68.7) | 0.98 (0.6–1.6) | 0.935 |
| Age (years) | 66.0 (57.0–73.0) | 66.0 (58.0–72.0) | 67.0 (57.0–75.0) | 1.01 (0.99–1.04) | 0.262 |
| BMI (kg/m2) | 26.5 (23.7–30.6) | 27.8 (24.3–31.7) | 26.1 (23.1–29.5) | 0.96 (0.91–1.00) | 0.067 |
| EuroSCORE II | 10.5 (4.2–21.3) | 9.2 (3.0–16.7) | 11.6 (6.4–27.7) | 1.03 (1.02–1.05) | <0.001 |
| CAD | 86 (60.6) | 36 (61.0) | 50 (60.2) | 0.96 (0.62–1.49) | 0.852 |
| Triple-vessel CAD | 59 (41.5) | 24 (40.7) | 35 (42.2) | 0.98 (0.63–1.52) | 0.930 |
| ACS in the last 90 days | 39 (27.5) | 20 (33.9) | 19 (22.9) | 0.74 (0.44–1.23) | 0.241 |
| LM stenosis > 50% | 26 (18.3) | 11 (18.6) | 15 (18.1) | 1.03 (0.59–1.80) | 0.921 |
| Cardiomyopathy | 45 (31.7) | 21 (35.6) | 24 (28.9) | 0.72 (0.45–1.16) | 0.179 |
| Ischemic cardiomyopathy | 27 (19.0) | 13 (22.0) | 14 (16.9) | 0.74 (0.41–1.31) | 0.296 |
| Dilated cardiomyopathy | 17 (12.0) | 7 (11.9) | 10 (12.0) | 0.89 (0.46–1.73) | 0.729 |
| Other cardiomyopathy * | 1 (0.7) | 1 (1.7) | 0 (0) | ||
| Cardiovascular risk factors | |||||
| Arterial hypertension | 111 (78.2) | 44 (74.6) | 67 (80.7) | 1.29 (0.75–2.23) | 0.361 |
| Hyperlipoproteinemia | 95 (66.9) | 40 (67.8) | 55 (66.3) | 0.97 (0.62–1.53) | 0.895 |
| Diabetes mellitus § | 38 (26.8) | 14 (23.7) | 24 (28.9) | 1.15 (0.72–1.85) | 0.563 |
| Smoking | 60 (42.3) | 27 (45.8) | 33 (39.8) | 0.84 (0.54–1.30) | 0.426 |
| Preexistent comorbidities | |||||
| COPD & | 11 (7.7) | 3 (5.1) | 8 (9.6) | 1.51 (0.73–3.13) | 0.271 |
| Impaired RF | 73 (51.4) | 25 (42.4) | 48 (57.8) | 1.79 (1.15–2.77) | 0.009 |
| RRT † | 7 (4.9) | 4 (6.8) | 3 (3.6) | 0.63 (0.20–1.98) | 0.426 |
| Stroke | 31 (21.8) | 15 (25.4) | 16 (19.3) | 0.87 (0.51–1.50) | 0.621 |
| Peripheral artery disease # | 19 (13.4) | 8 (13.6) | 11 (13.3) | 1.15 (0.61–2.17) | 0.664 |
| Pulmonary hypertension | 52 (36.6) | 23 (39.0) | 29 (34.9) | 0.88 (0.56–1.39) | 0.584 |
| Atrial fibrillation | 52 (36.6) | 19 (32.2) | 33 (39.8) | 1.21 (0.78–1.88) | 0.392 |
| Endocarditis | 18 (12.7) | 4 (6.8) | 14 (16.9) | 2.13 (1.20–3.81) | 0.010 |
| Echocardiography | |||||
| LVEF (%) | 50.0 (30.0–60.0) | 50.0 (29.5–60.0) | 49.0 (30.0–60.0) | 1.00 (0.99–1.02) | 0.582 |
| Normal LVEF | 60 (42.3) | 27 (45.8) | 33 (39.8) | 0.87 (0.56–1.36) | 0.545 |
| Mildly impaired LVEF | 20 (14.1) | 7 (11.9) | 13 (15.7) | 1.38 (0.76–2.49) | 0.291 |
| Moderately impaired LVEF | 18 (12.7) | 6 (10.2) | 12 (14.5) | 1.49 (0.80–2.74) | 0.206 |
| Severely impaired LVEF | 44 (31.0) | 19 (32.2) | 25 (30.1) | 0.81 (0.50–1.29) | 0.367 |
| TAPSE < 16 mm | 49 (34.5) | 15 (25.4) | 34 (41.0) | 1.40 (0.90–2.17) | 0.135 |
| Severe AV regurgitation | 14 (9.9) | 4 (6.8) | 10 (12.0) | 2.02 (1.04–3.91) | 0.039 |
| Severe MV regurgitation | 33 (23.2) | 18 (30.5) | 15 (18.1) | 0.63 (0.36–1.10) | 0.106 |
| Severe TV regurgitation | 23 (16.2) | 8 (13.6) | 15 (18.1) | 1.42 (0.81–2.50) | 0.218 |
| Invasive ventilation | 20 (14.1) | 8 (13.6) | 12 (14.5) | 1.18 (0.64–2.17) | 0.599 |
| Variable | All Patients n = 142, n (%) | Survivors n = 59, n (%) | Non-Survivors n = 83, n (%) | HR | p-Value |
|---|---|---|---|---|---|
| Cardiac reoperation | 50 (35.2) | 16 (27.1) | 34 (41.0) | 1.44 (0.93–2.24) | 0.104 |
| Elective surgery | 46 (32.4) | 17 (28.8) | 29 (34.9) | 1.07 (0.68–1.69) | 0.755 |
| Urgent surgery | 65 (45.8) | 28 (47.5) | 37 (44.6) | 0.95 (0.61–1.46) | 0.811 |
| Emergency surgery | 31 (21.8) | 14 (23.7) | 17 (20.5) | 0.98 (0.58–1.67) | 0.945 |
| Combined surgery | 71 (50.0) | 29 (49.2) | 42 (50.6) | 1.20 (0.78–1.85) | 0.399 |
| CPB times | |||||
| CPB duration (min) | 215.0 (145.5–283.5) | 204.0 (134.0–280.0) | 223.5 (160.8–286.8) | 1.00 (1.00–1.01) | 0.028 |
| Cross clamp time (min) | 118.0 (78.0–165.3) | 107.0 (70.0–157.0) | 131.0 (85.5–171.0) | 1.00 (1.00–101) | 0.021 |
| Circulatory arrest | 25 (17.6) | 9 (15.3) | 16 (19.3) | 1.39 (0.80–2.40) | 0.240 |
| Pre-ECLS data | |||||
| CPR | 25 (17.6) | 10 (16.9) | 15 (18.1) | 1.11 (0.64–1.95) | 0.710 |
| pH | 7.36 (7.31–7.40) | 7.36 (7.32–7.40) | 7.36 (7.29–7.41) | 0.73 (0.05–10.13) | 0.814 |
| Lactate (mmol/L) | 4.7 (3.1–6.9) | 4.3 (2.8–6.4) | 5.0 (3.2–7.2) | 1.07 (1.01–1.12) | 0.014 |
| PEEP (cmH2O) | 10.0 (8.0–12.0) | 10.0 (10.0–12.0) | 10.0 (8.0–12.0) | 0.94 (0.87–1.02) | 0.161 |
| Pinsp (cmH2O) | 20.0 (18.0–25.0) | 20.0 (18.0–24.0) | 20.0 (18.0–27.0) | 1.01 (0.97–1.04) | 0.731 |
| VIS | 43.2 (30.4–60.2) | 43.9 (31.3–59.4) | 41.0 (29.2–62.8) | 1.00 (0.99–1.01) | 0.904 |
| Variable | Univariable Regression | Multivariable Regression | ||
|---|---|---|---|---|
| HR | p-Value | HR | p-Value | |
| BMI (kg/m2) | 0.96 (0.91–1.00) | 0.067 | 0.97 (0.92–1.01) | 0.119 |
| EuroSCORE II | 1.03 (1.02–1.05) | <0.001 | 1.02 (1.00–1.04) | 0.013 |
| Impaired RF | 1.79 (1.15–2.77) | 0.009 | 1.93 (1.17–3.20) | 0.010 |
| Severe AV regurgitation | 2.02 (1.04–3.91) | 0.039 | 1.34 (0.64–2.81) | 0.432 |
| Endocarditis | 2.13 (1.20–3.81) | 0.010 | 1.04 (0.51–2.12) | 0.920 |
| CPB duration (min) | 1.00 (1.00–1.01) | 0.028 | 1.003 (1.00–1.01) | 0.015 |
| Lactate (mmol/L) | 1.07 (1.01–1.12) | 0.014 | 1.08 (1.02–1.14) | 0.004 |
| 36-Item Short Form Survey | Mean ± SD | Below Normal Range n (%) |
|---|---|---|
| Physical component summary | 45.5 ± 10.2 | 13 (27.1) |
| Mental component summary | 50.6 ± 12.5 | 7 (14.6) |
| Physical functioning | 71.9 ± 27.3 | 6 (12.5) |
| Role physical | 71.9 ± 37.1 | 9 (18.8) |
| Bodily pain | 71.9 ± 32.5 | 9 (18.8) |
| General health | 67.2 ± 22.6 | 6 (12.5) |
| Vitality | 60.9 ± 25.2 | 8 (16.7) |
| Social functioning | 80.2 ± 26.1 | 6 (12.5) |
| Role emotional | 88.9 ± 29.4 | 5 (10.4) |
| Mental health | 76.0 ± 19.1 | 2 (4.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanuna, M.; Herz, G.; Stanzl, A.L.; Li, Y.; Mueller, C.S.; Kamla, C.E.; Scherer, C.; Wassilowsky, D.; Juchem, G.; Orban, M.; et al. Mid-Term Outcome after Extracorporeal Life Support in Postcardiotomy Cardiogenic Shock: Recovery and Quality of Life. J. Clin. Med. 2024, 13, 2254. https://doi.org/10.3390/jcm13082254
Hanuna M, Herz G, Stanzl AL, Li Y, Mueller CS, Kamla CE, Scherer C, Wassilowsky D, Juchem G, Orban M, et al. Mid-Term Outcome after Extracorporeal Life Support in Postcardiotomy Cardiogenic Shock: Recovery and Quality of Life. Journal of Clinical Medicine. 2024; 13(8):2254. https://doi.org/10.3390/jcm13082254
Chicago/Turabian StyleHanuna, Maja, German Herz, Andre L. Stanzl, Yupeng Li, Christoph S. Mueller, Christine E. Kamla, Clemens Scherer, Dietmar Wassilowsky, Gerd Juchem, Martin Orban, and et al. 2024. "Mid-Term Outcome after Extracorporeal Life Support in Postcardiotomy Cardiogenic Shock: Recovery and Quality of Life" Journal of Clinical Medicine 13, no. 8: 2254. https://doi.org/10.3390/jcm13082254
APA StyleHanuna, M., Herz, G., Stanzl, A. L., Li, Y., Mueller, C. S., Kamla, C. E., Scherer, C., Wassilowsky, D., Juchem, G., Orban, M., Peterss, S., Hagl, C., & Joskowiak, D. (2024). Mid-Term Outcome after Extracorporeal Life Support in Postcardiotomy Cardiogenic Shock: Recovery and Quality of Life. Journal of Clinical Medicine, 13(8), 2254. https://doi.org/10.3390/jcm13082254