

Diagnostic Ability of Manual Calcification Length Assessment on Non-Electrocardiographically Gated Computed Tomography for Estimating the Presence of Coronary Artery Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
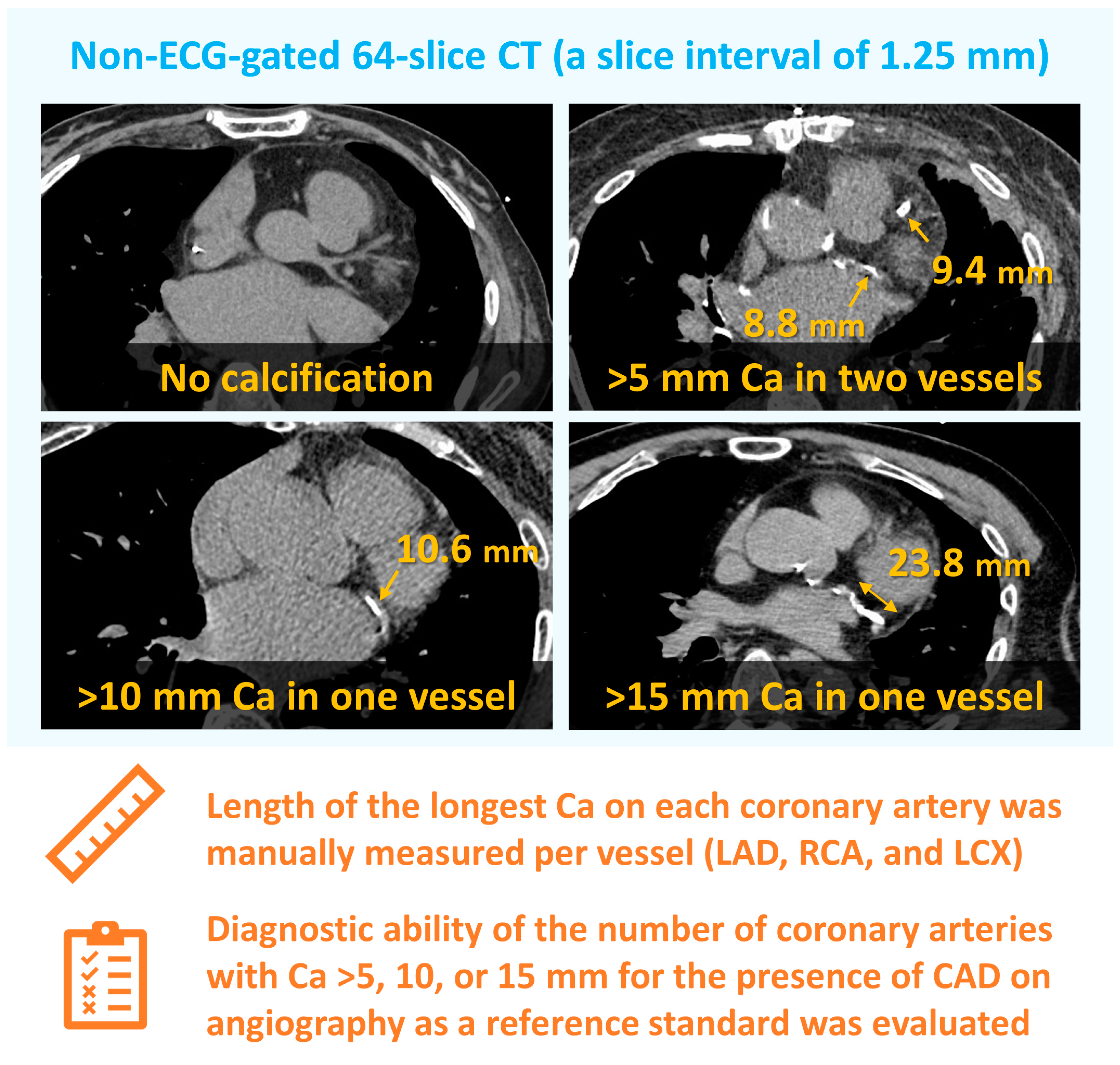
2.2. Computed Tomography Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- He, Z.X.; Hedrick, T.D.; Pratt, C.M.; Verani, M.S.; Aquino, V.; Roberts, R.; Mahmarian, J.J. Severity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemia. Circulation 2000, 101, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Nasir, K.; Rubin, J.; Blaha, M.J.; Shaw, L.J.; Blankstein, R.; Rivera, J.J.; Khan, A.N.; Berman, D.; Raggi, P.; Callister, T.; et al. Interplay of coronary artery calcification and traditional risk factors for the prediction of all-cause mortality in asymptomatic individuals. Circ. Cardiovasc. Imaging 2012, 5, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Kelkar, A.A.; Schultz, W.M.; Khosa, F.; Schulman-Marcus, J.; O’Hartaigh, B.W.; Gransar, H.; Blaha, M.J.; Knapper, J.T.; Berman, D.S.; Quyyumi, A.; et al. Long-Term Prognosis after Coronary Artery Calcium Scoring among Low-Intermediate Risk Women and Men. Circ. Cardiovasc. Imaging 2016, 9, e003742. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Golub, I.S.; Termeie, O.G.; Kristo, S.; Schroeder, L.P.; Lakshmanan, S.; Shafter, A.M.; Hussein, L.; Verghese, D.; Aldana-Bitar, J.; Manubolu, V.S.; et al. Major Global Coronary Artery Calcium Guidelines. JACC Cardiovasc. Imaging 2023, 16, 98–117. [Google Scholar] [CrossRef]
- Suzuki, Y.; Matsumoto, N.; Yoda, S.; Amano, Y.; Okumura, Y. Coronary artery calcium score: Current status of clinical application and how to handle the results. J. Cardiol. 2022, 79, 567–571. [Google Scholar] [CrossRef]
- Gupta, A.; Bera, K.; Kikano, E.; Pierce, J.D.; Gan, J.; Rajdev, M.; Ciancibello, L.M.; Gupta, A.; Rajagopalan, S.; Gilkeson, R.C. Coronary Artery Calcium Scoring: Current Status and Future Directions. Radiographics 2022, 42, 947–967. [Google Scholar] [CrossRef]
- Xie, X.; Zhao, Y.; de Bock, G.H.; de Jong, P.A.; Mali, W.P.; Oudkerk, M.; Vliegenthart, R. Validation and prognosis of coronary artery calcium scoring in nontriggered thoracic computed tomography: Systematic review and meta-analysis. Circ. Cardiovasc. Imaging 2013, 6, 514–521. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef]
- Greenland, P.; Blaha, M.J.; Budoff, M.J.; Erbel, R.; Watson, K.E. Coronary Calcium Score and Cardiovascular Risk. J. Am. Coll. Cardiol. 2018, 72, 434–447. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Chmura Kraemer, H.; Periyakoil, V.S.; Noda, A. Kappa coefficients in medical research. Stat. Med. 2002, 21, 2109–2129. [Google Scholar] [CrossRef] [PubMed]
- Akers, E.J.; Nicholls, S.J.; Di Bartolo, B.A. Plaque Calcification: Do Lipoproteins Have a Role? Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1902–1910. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Feng, W.; Su, X.; Luo, D.; Li, Z.; Zhou, Y.; Zhu, Y.; Zhang, M.; Chen, J.; Liu, B.; et al. SIRT6 protects vascular smooth muscle cells from osteogenic transdifferentiation via Runx2 in chronic kidney disease. J. Clin. Investig. 2022, 132, e150051. [Google Scholar] [CrossRef]
- Ouyang, L.; Yu, C.; Xie, Z.; Su, X.; Xu, Z.; Song, P.; Li, J.; Huang, H.; Ding, Y.; Zou, M.H. Indoleamine 2,3-Dioxygenase 1 Deletion-Mediated Kynurenine Insufficiency in Vascular Smooth Muscle Cells Exacerbates Arterial Calcification. Circulation 2022, 145, 1784–1798. [Google Scholar] [CrossRef]
- Bavishi, C.; Argulian, E.; Chatterjee, S.; Rozanski, A. CACS and the Frequency of Stress-Induced Myocardial Ischemia during MPI: A Meta-Analysis. JACC Cardiovasc. Imaging 2016, 9, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, T.S.; McClelland, R.L.; Jorgensen, N.W.; Bild, D.E.; Burke, G.L.; Guerci, A.D.; Greenland, P. Coronary artery calcium score and risk classification for coronary heart disease prediction. JAMA 2010, 303, 1610–1616. [Google Scholar] [CrossRef]
- Bell, K.J.L.; White, S.; Hassan, O.; Zhu, L.; Scott, A.M.; Clark, J.; Glasziou, P. Evaluation of the Incremental Value of a Coronary Artery Calcium Score Beyond Traditional Cardiovascular Risk Assessment: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2022, 182, 634–642. [Google Scholar] [CrossRef]
- Hecht, H.S.; Cronin, P.; Blaha, M.J.; Budoff, M.J.; Kazerooni, E.A.; Narula, J.; Yankelevitz, D.; Abbara, S. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. J. Cardiovasc. Comput. Tomogr. 2017, 11, 74–84. [Google Scholar] [CrossRef]
- Einstein, A.J.; Johnson, L.L.; Bokhari, S.; Son, J.; Thompson, R.C.; Bateman, T.M.; Hayes, S.W.; Berman, D.S. Agreement of visual estimation of coronary artery calcium from low-dose CT attenuation correction scans in hybrid PET/CT and SPECT/CT with standard Agatston score. J. Am. Coll. Cardiol. 2010, 56, 1914–1921. [Google Scholar] [CrossRef] [PubMed]
- Wieske, V.; Walther, M.; Dubourg, B.; Alkadhi, H.; Nørgaard, B.L.; Meijs, M.F.L.; Diederichsen, A.C.P.; Wan, Y.L.; Mickley, H.; Nikolaou, K.; et al. Computed tomography angiography versus Agatston score for diagnosis of coronary artery disease in patients with stable chest pain: Individual patient data meta-analysis of the international COME-CCT Consortium. Eur. Radiol. 2022, 32, 5233–5245. [Google Scholar] [CrossRef] [PubMed]
- Newby, D.E.; Adamson, P.D.; Berry, C.; Boon, N.A.; Dweck, M.R.; Flather, M.; Forbes, J.; Hunter, A.; Lewis, S.; MacLean, S.; et al. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N. Engl. J. Med. 2018, 379, 924–933. [Google Scholar] [PubMed]
- Budoff, M.J.; Young, R.; Lopez, V.A.; Kronmal, R.A.; Nasir, K.; Blumenthal, R.S.; Detrano, R.C.; Bild, D.E.; Guerci, A.D.; Liu, K.; et al. Progression of coronary calcium and incident coronary heart disease events: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2013, 61, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Hecht, H.; Blaha, M.J.; Berman, D.S.; Nasir, K.; Budoff, M.; Leipsic, J.; Blankstein, R.; Narula, J.; Rumberger, J.; Shaw, L.J. Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2017, 11, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Schenker, M.P.; Dorbala, S.; Hong, E.C.; Rybicki, F.J.; Hachamovitch, R.; Kwong, R.Y.; Di Carli, M.F. Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: A combined positron emission tomography/computed tomography study. Circulation 2008, 117, 1693–1700. [Google Scholar] [CrossRef] [PubMed]
- Kawase, Y.; Matsuo, H.; Kuramitsu, S.; Shiono, Y.; Akasaka, T.; Tanaka, N.; Amano, T.; Kozuma, K.; Nakamura, M.; Yokoi, H.; et al. Clinical use of physiological lesion assessment using pressure guidewires: An expert consensus document of the Japanese association of cardiovascular intervention and therapeutics-update 2022. Cardiovasc. Interv. Ther. 2022, 37, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Ando, H.; Yamaji, K.; Kohsaka, S.; Ishii, H.; Wada, H.; Yamada, S.; Sawano, M.; Inohara, T.; Numasawa, Y.; Ikari, Y.; et al. Japanese Nationwide PCI (J-PCI) Registry Annual Report 2019: Patient demographics and in-hospital outcomes. Cardiovasc. Interv. Ther. 2022, 37, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Kobayashi, Y.; Fujii, K.; Sonoda, S.; Tsujita, K.; Hibi, K.; Morino, Y.; Okura, H.; Ikari, Y.; Kozuma, K.; et al. CVIT 2023 clinical expert consensus document on intravascular ultrasound. Cardiovasc. Interv. Ther. 2024, 39, 1–14. [Google Scholar] [CrossRef]
- Saito, Y.; Kobayashi, Y. Contemporary coronary drug-eluting and coated stents: An updated mini-review (2023). Cardiovasc. Interv. Ther. 2024, 39, 15–17. [Google Scholar] [CrossRef]
- Fujimoto, Y.; Sakakura, K.; Fujita, H. Complex and high-risk intervention in indicated patients (CHIP) in contemporary clinical practice. Cardiovasc. Interv. Ther. 2023, 38, 269–274. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 100) | Epicardial CAD (>50%) on CAG | p Value | |
|---|---|---|---|---|
| No (n = 51) | Yes (n = 49) | |||
| Age (years) | 70.5 ± 11.5 | 68.7 ± 13.5 | 72.5 ± 8.7 | 0.10 |
| Men | 74 (74.0%) | 34 (66.7%) | 40 (81.6%) | 0.88 |
| BMI (kg/m2) | 23.3 ± 5.7 | 24.4 ± 6.9 | 22.3 ± 4.2 | 0.17 |
| Hypertension | 60 (60.0%) | 25 (49.0%) | 35 (71.4%) | 0.02 |
| Diabetes | 41 (41.0%) | 13 (25.5%) | 28 (57.1%) | 0.001 |
| Dyslipidemia | 34 (34.0%) | 12 (23.5%) | 22 (44.9%) | 0.02 |
| Current smoker | 29 (29.0%) | 17 (33.3%) | 12 (24.5%) | 0.32 |
| eGFR (mL/min/1.73 m2) | 62.0 ± 19.3 | 65.3 ± 21.5 | 59.4 ± 16.3 | 0.13 |
| Chronic kidney disease | 43 (43.0%) | 20 (39.2%) | 23 (46.9%) | 0.44 |
| Indication of CAG | ||||
| Heart failure | 42 (42.0%) | 27 (52.9%) | 15 (30.6%) | 0.02 |
| Suspected angina | 29 (29.0%) | 9 (17.6%) | 20 (40.8%) | 0.01 |
| Preoperative testing | 13 (13.0%) | 5 (9.8%) | 8 (16.3%) | 0.33 |
| Brady arrhythmia | 8 (8.0%) | 6 (11.8%) | 2 (4.1%) | 0.15 |
| PAD | 6 (6.0%) | 2 (3.9%) | 4 (8.2%) | 0.37 |
| Vasospastic angina | 2 (2.0%) | 2 (3.9%) | 0 (0%) | 0.16 |
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | |
|---|---|---|---|---|---|
| Standard CACS > 400 | 73 | 78 | 77 | 75 | 76 |
| No. of vessels with Ca > 5 mm | |||||
| 1 | 92 | 51 | 64 | 87 | 71 |
| 2 | 73 | 76 | 75 | 75 | 75 |
| 3 | 43 | 90 | 81 | 62 | 67 |
| No. of vessels with Ca > 10 mm | |||||
| 1 | 88 | 67 | 72 | 85 | 77 |
| 2 | 51 | 86 | 78 | 65 | 69 |
| 3 | 33 | 94 | 84 | 59 | 64 |
| No. of vessels with Ca > 15 mm | |||||
| 1 | 86 | 82 | 82 | 86 | 84 |
| 2 | 43 | 92 | 84 | 63 | 68 |
| 3 | 20 | 94 | 77 | 55 | 58 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, R.; Saito, Y.; Tokimasa, S.; Takaoka, H.; Kitahara, H.; Yamanouchi, M.; Kobayashi, Y. Diagnostic Ability of Manual Calcification Length Assessment on Non-Electrocardiographically Gated Computed Tomography for Estimating the Presence of Coronary Artery Disease. J. Clin. Med. 2024, 13, 2255. https://doi.org/10.3390/jcm13082255
Watanabe R, Saito Y, Tokimasa S, Takaoka H, Kitahara H, Yamanouchi M, Kobayashi Y. Diagnostic Ability of Manual Calcification Length Assessment on Non-Electrocardiographically Gated Computed Tomography for Estimating the Presence of Coronary Artery Disease. Journal of Clinical Medicine. 2024; 13(8):2255. https://doi.org/10.3390/jcm13082255
Chicago/Turabian StyleWatanabe, Ryota, Yuichi Saito, Satoshi Tokimasa, Hiroyuki Takaoka, Hideki Kitahara, Masato Yamanouchi, and Yoshio Kobayashi. 2024. "Diagnostic Ability of Manual Calcification Length Assessment on Non-Electrocardiographically Gated Computed Tomography for Estimating the Presence of Coronary Artery Disease" Journal of Clinical Medicine 13, no. 8: 2255. https://doi.org/10.3390/jcm13082255
APA StyleWatanabe, R., Saito, Y., Tokimasa, S., Takaoka, H., Kitahara, H., Yamanouchi, M., & Kobayashi, Y. (2024). Diagnostic Ability of Manual Calcification Length Assessment on Non-Electrocardiographically Gated Computed Tomography for Estimating the Presence of Coronary Artery Disease. Journal of Clinical Medicine, 13(8), 2255. https://doi.org/10.3390/jcm13082255