
Postoperative Benefits of Soft Tissue Wrist Arthroscopy: Retro- and Prospective Analyses of Outcome Measures


Abstract
1. Introduction
2. Materials and Methods
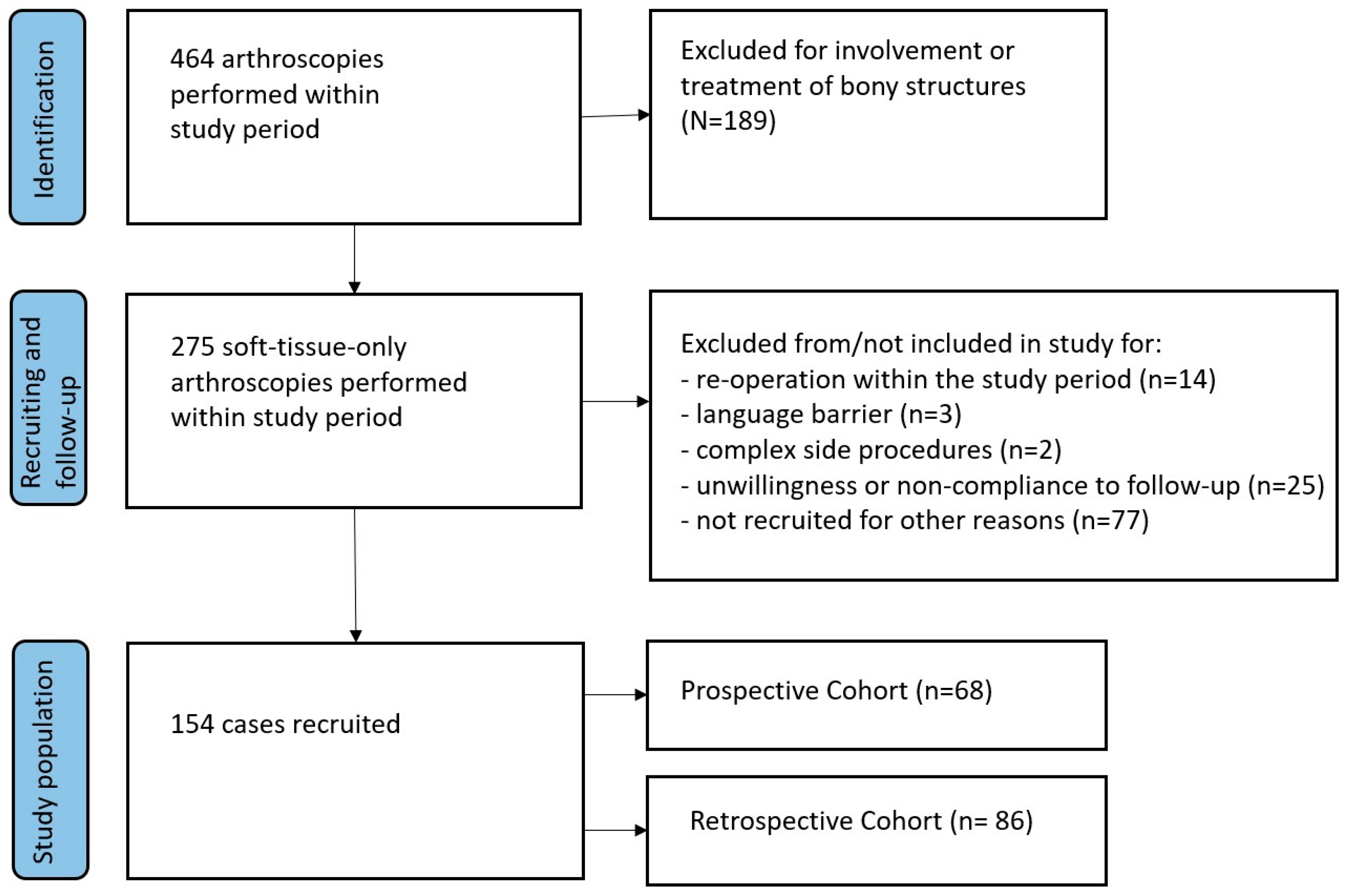
2.1. Study Design
2.2. Data Collection/Recall Survey and Validation
2.3. Methods of Measuring Objective Outcomes
2.4. Methods of Measuring Patient-Reported Outcomes (PROMs)
2.5. Statistical Analysis
3. Results
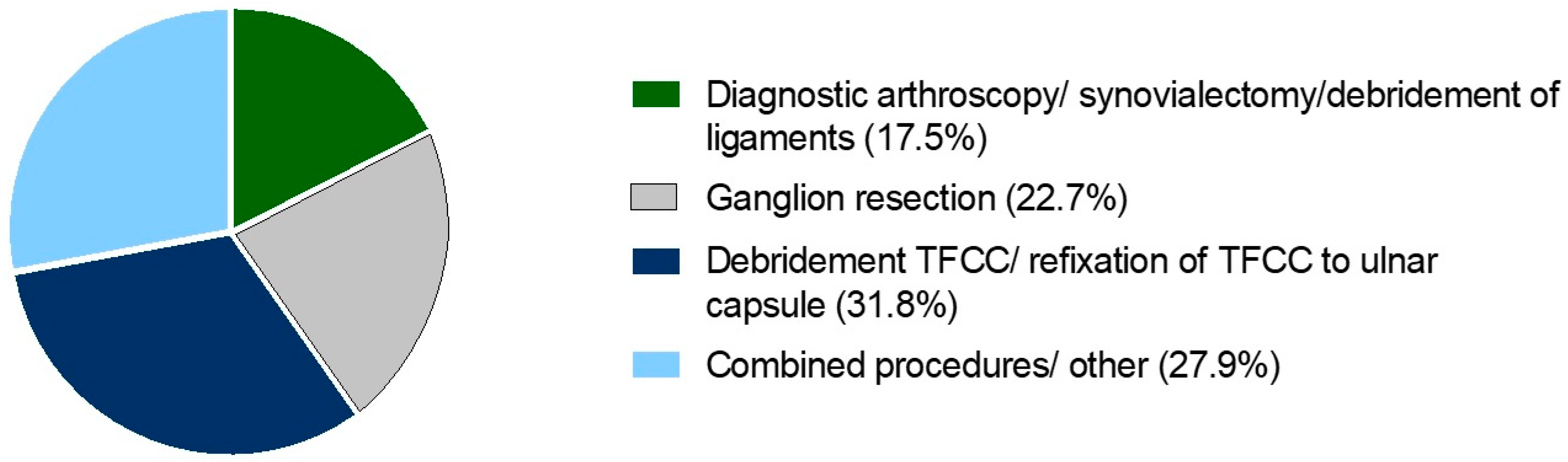
3.1. Demographic Data
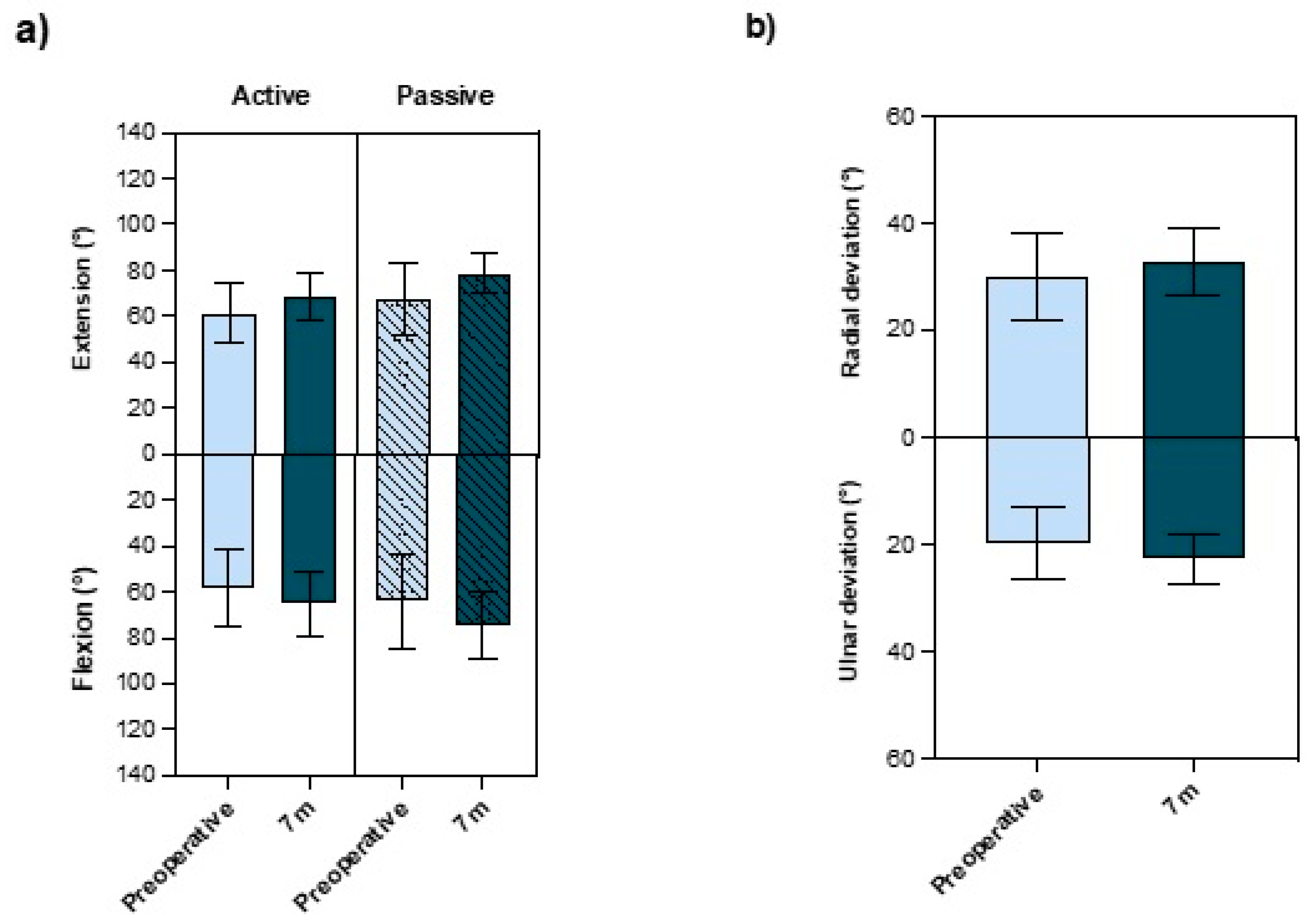
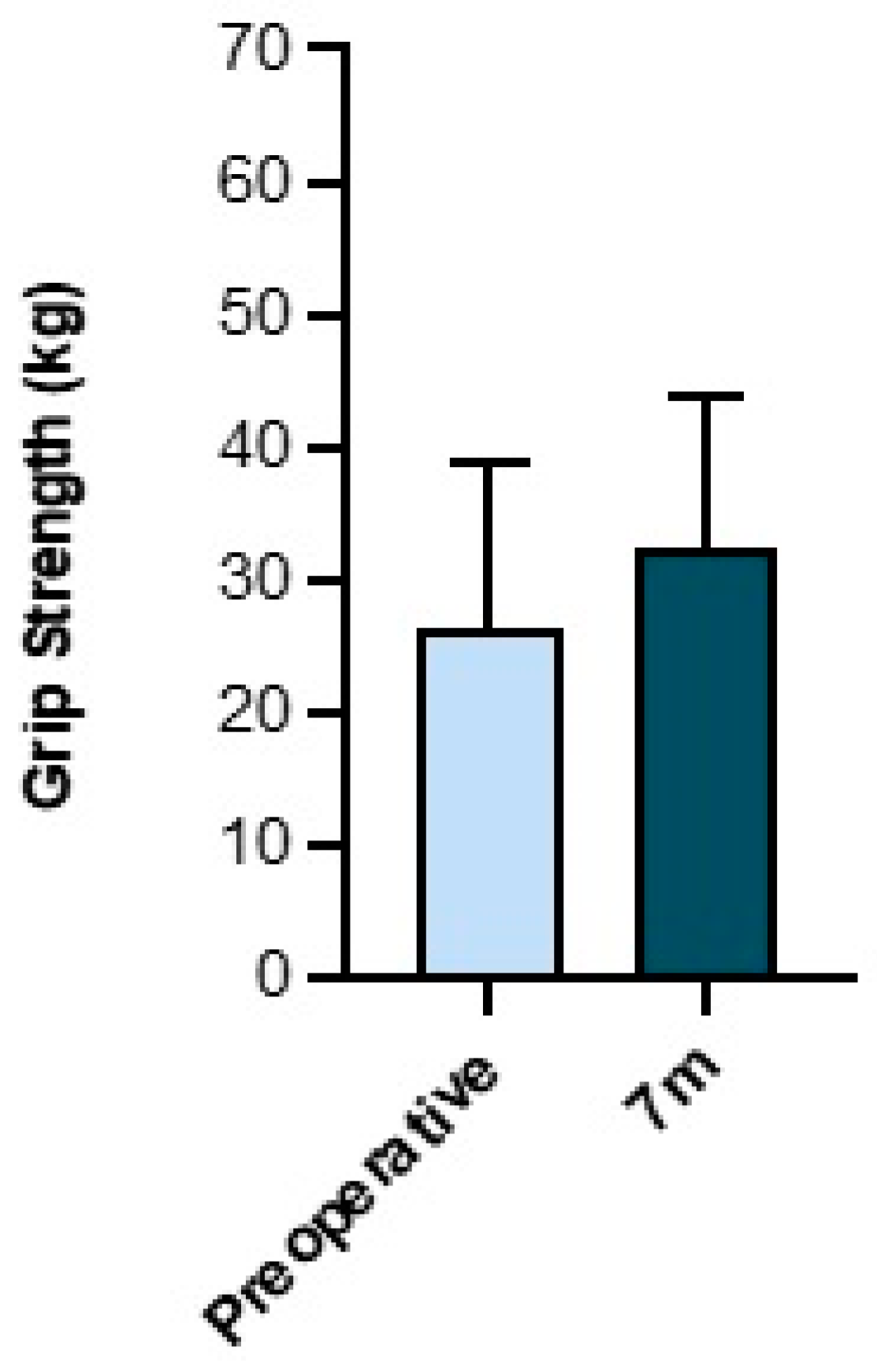
3.2. Results of Objective Outcome Measurements
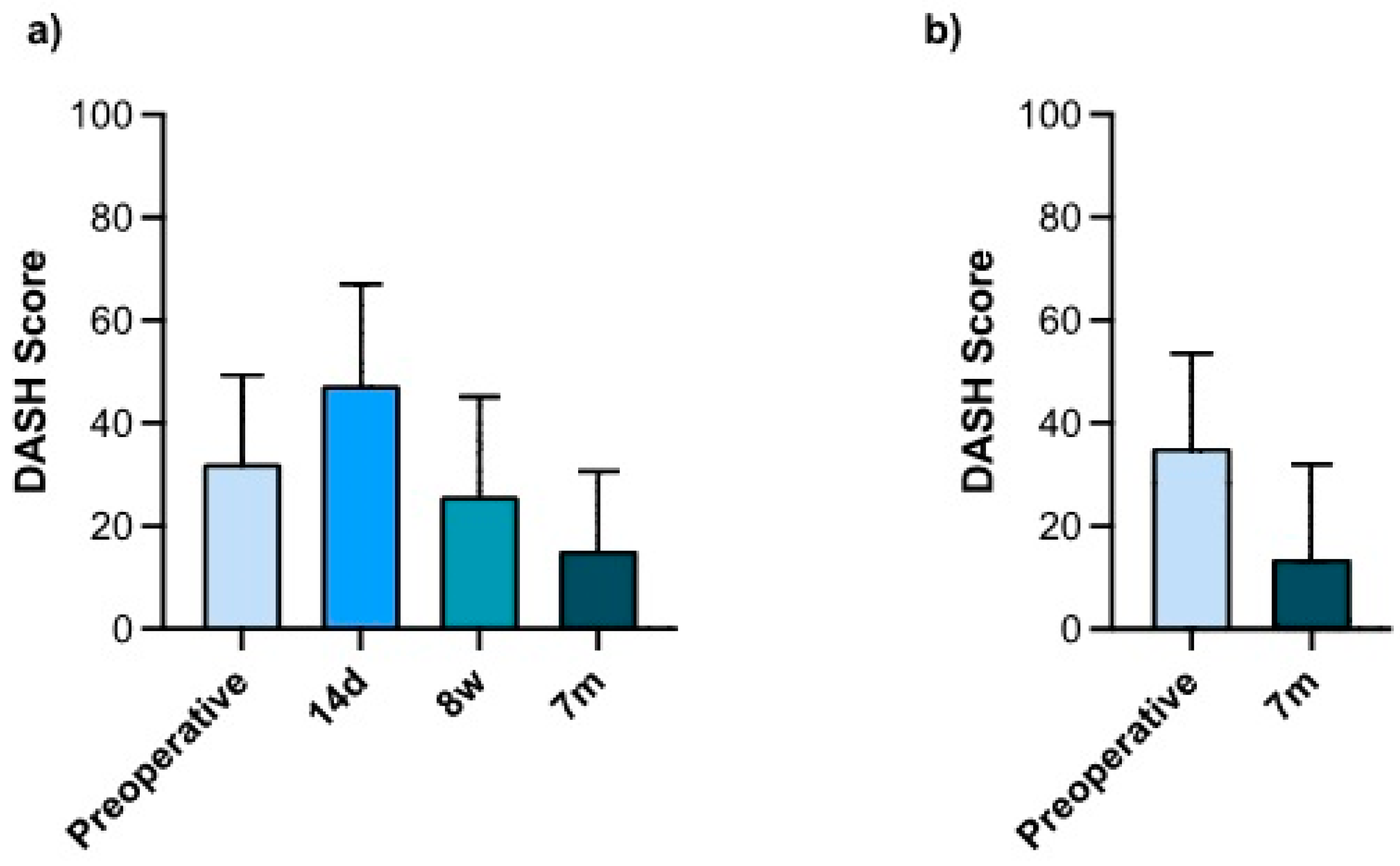
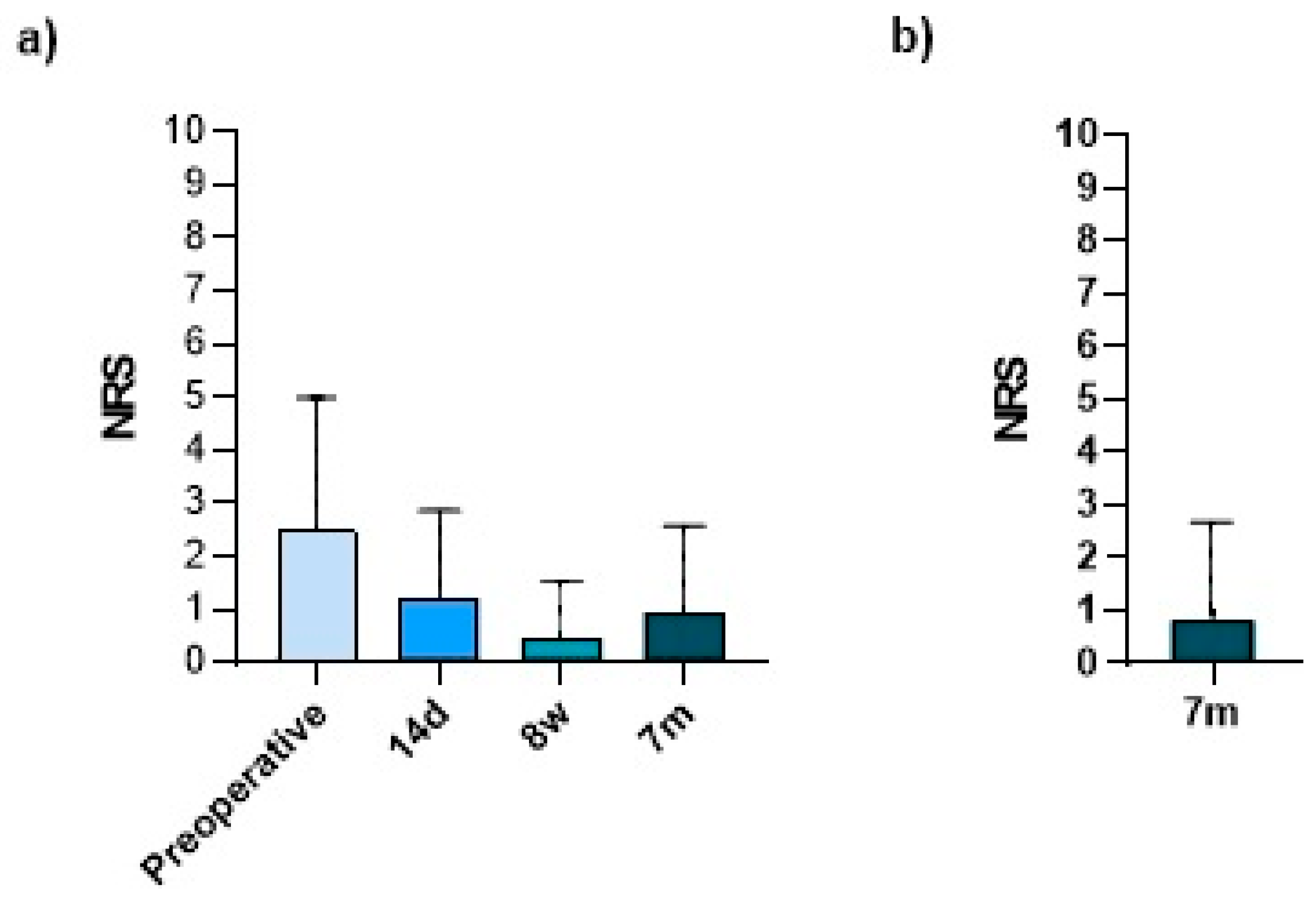
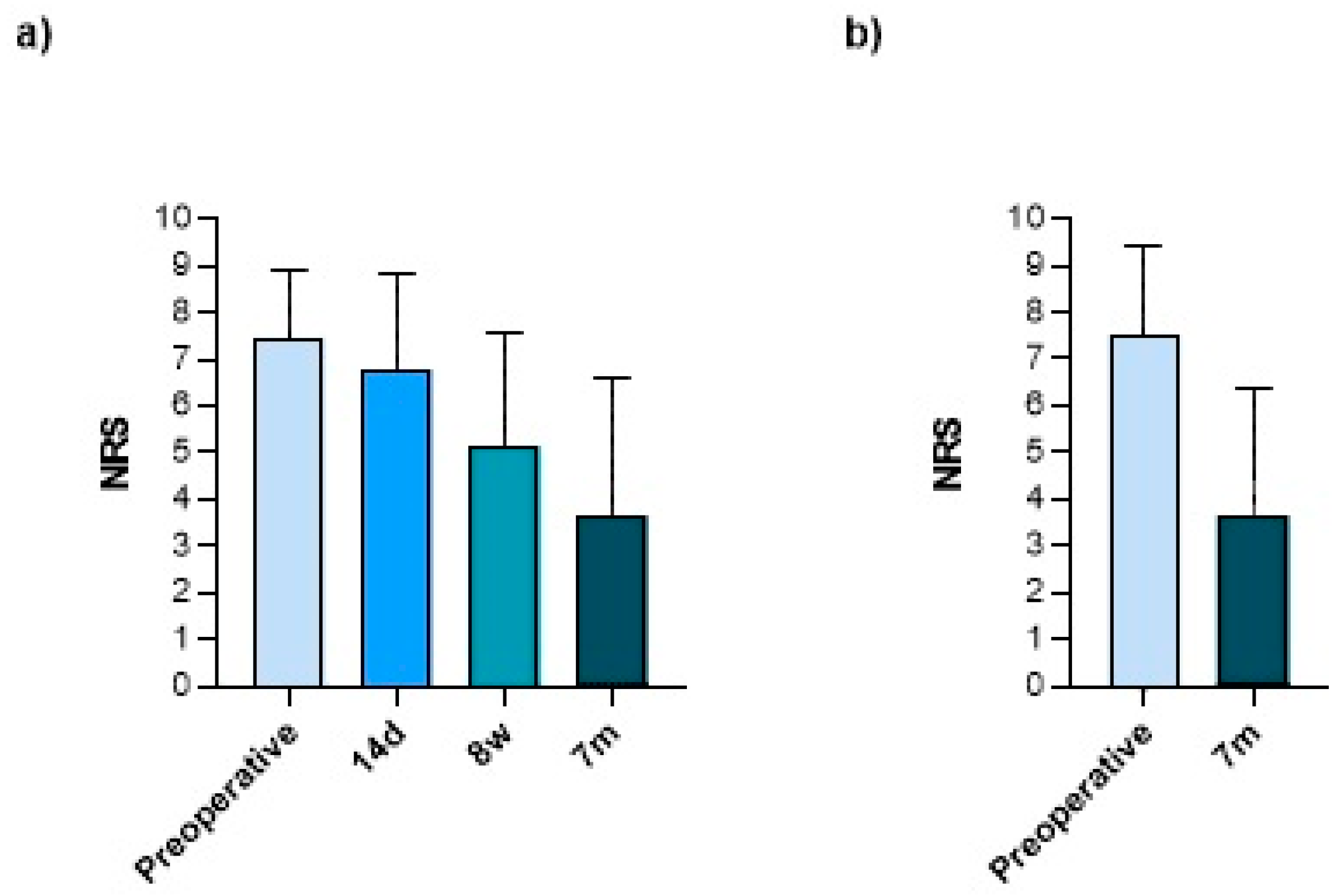
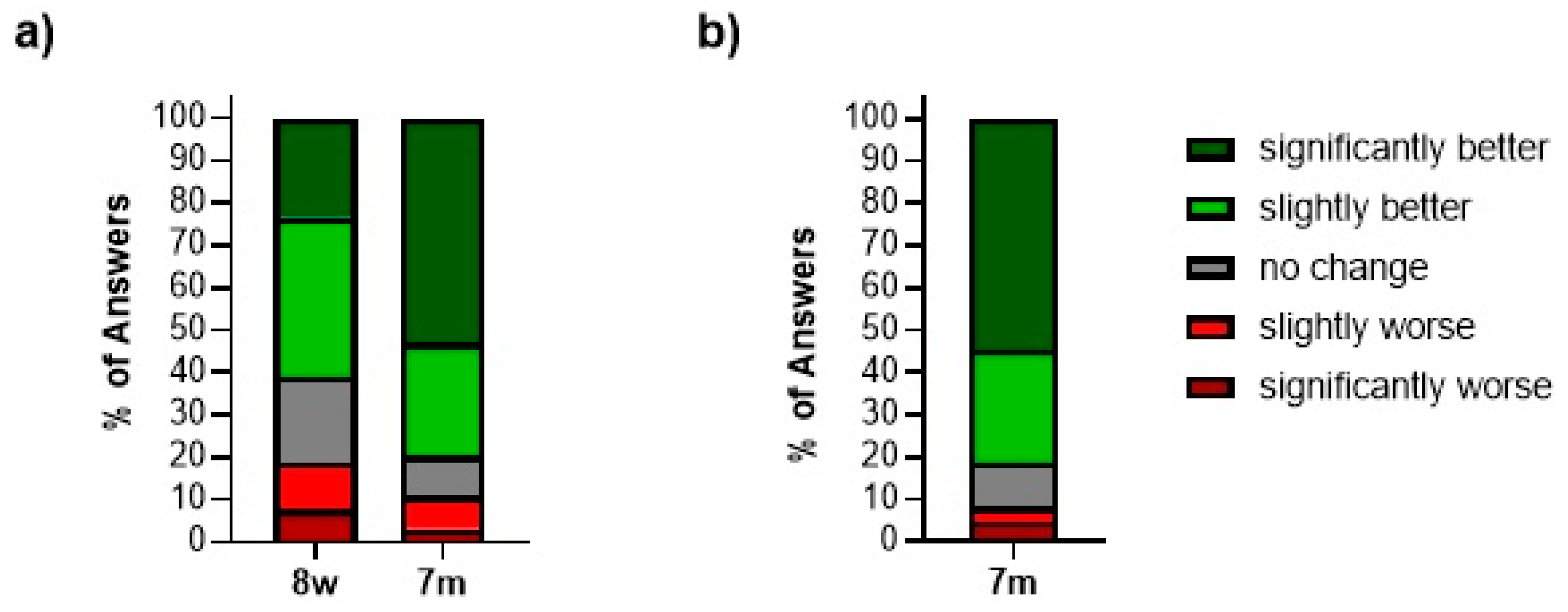
3.3. Results of Patient-Reported Outcome Measures (PROMs)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Unger, T.; Anand, P. Wrist Arthroscopy; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- van Schoonhoven, J. Arthroskopische Operationen am Handgelenk. Oper. Orthop. Traumatol. 2016, 28, 231–232. [Google Scholar] [CrossRef]
- Chen, Y.C. Arthroscopy of the wrist and finger joints. Orthop. Clin. N. Am. 1979, 10, 723–733. [Google Scholar]
- Watanabe, M. Present status and future of arthroscopy. Geka Chiryo 1972, 26, 73–77. [Google Scholar]
- Mathoulin, C. Wrist Arthroscopy Techniques, 2nd ed.; Thieme: Stuttgart, Germany, 2019. [Google Scholar]
- Wagner, J.; Ipaktchi, K.; Livermore, M.; Banegas, R. Current indications for and the technique of wrist arthroscopy. Orthopedics 2014, 37, 251–256. [Google Scholar] [CrossRef]
- Michelotti, B.F.; Chung, K.C. Diagnostic Wrist Arthroscopy. Hand Clin. 2017, 33, 571–583. [Google Scholar] [CrossRef]
- Tadjerbashi, K.; Rosales, R.S.; Atroshi, I. Intervention randomized controlled trials involving wrist and shoulder arthroscopy: A systematic review. BMC Musculoskelet. Disord. 2014, 15, 252. [Google Scholar] [CrossRef]
- Gagnier, J.J. Patient reported outcomes in orthopaedics. J. Orthop. Res. 2017, 35, 2098–2108. [Google Scholar] [CrossRef]
- Makhni, E.C. Meaningful Clinical Applications of Patient-Reported Outcome Measures in Orthopaedics. J. Bone Jt. Surg. Am. 2021, 103, 84–91. [Google Scholar] [CrossRef]
- Chanthana, P.; Atthakomol, P.; Manosroi, W.; Wongpakaran, T.; Kraisarin, J.; Sananpanich, K. Comparison of patient preferences and responsiveness among common patient-reported outcome measures for hand/wrist injuries or disorders. J. Orthop. Traumatol. 2023, 24, 2. [Google Scholar] [CrossRef]
- Westphal, T. Reliability and responsiveness of the German version of the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH). Der Unfallchirurg 2007, 110, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Dacombe, P.J.; Amirfeyz, R.; Davis, T. Patient-Reported Outcome Measures for Hand and Wrist Trauma: Is There Sufficient Evidence of Reliability, Validity, and Responsiveness? Hand 2016, 11, 11–21. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Safikhani, S.; Gries, K.S.; Trudeau, J.J.; Reasner, D.; Rüdell, K.; Coons, S.J.; Bush, E.N.; Hanlon, J.; Abraham, L.; Vernon, M. Response scale selection in adult pain measures: Results from a literature review. J. Patient Rep. Outcomes 2017, 2, 40. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Pritchett, Y.L.; Robinson, M.; Prakash, A.; Chappell, A. The clinical importance of changes in the 0 to 10 numeric rating scale for worst, least, and average pain intensity: Analyses of data from clinical trials of duloxetine in pain disorders. J. Pain 2010, 11, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Godil, S.S.; Parker, S.L.; Zuckerman, S.L.; Mendenhall, S.K.; McGirt, M.J. Accurately measuring the quality and effectiveness of cervical spine surgery in registry efforts: Determining the most valid and responsive instruments. Spine J. 2015, 15, 1203–1209. [Google Scholar] [CrossRef]
- Finsen, V.; Hillesund, S.; Fromreide, I. The Reliability of Remembered Pretreatment Visual Analog Scale Scores among Hand-Surgery Patients. J. Hand Microsurg. 2020, 12, 8–12. [Google Scholar] [CrossRef]
- Reynolds, N.; Thirkannad, S. The recall DASH score—A novel research tool. Hand Surg. 2013, 18, 11–14. [Google Scholar] [CrossRef]
- Carter, T.I.; Pansy, B.; Wolff, A.L.; Hillstrom, H.J.; Backus, S.I.; Lenhoff, M.; Wolfe, S.W. Accuracy and reliability of three different techniques for manual goniometry for wrist motion: A cadaveric study. J. Hand Surg. Am. 2009, 34, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Gajdosik, R.L.; Bohannon, R.W. Clinical measurement of range of motion. Review of goniometry emphasizing reliability and validity. Phys. Ther. 1987, 67, 1867–1872. [Google Scholar] [CrossRef]
- Horger, M.M. The reliability of goniometric measurements of active and passive wrist motions. Am. J. Occup. Ther. 1990, 44, 342–348. [Google Scholar] [CrossRef]
- Lefevre-Colau, M.M.; Poiraudeau, S.; Oberlin, C.; Demaille, S.; Fermanian, J.; Rannou, F.; Revel, M. Reliability, validity, and responsiveness of the modified Kapandji index for assessment of functional mobility of the rheumatoid hand. Arch. Phys. Med. Rehabil. 2003, 84, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Gong, H.S. Measurement and Interpretation of Handgrip Strength for Research on Sarcopenia and Osteoporosis. J. Bone Metab. 2020, 27, 85–96. [Google Scholar] [CrossRef]
- Towfigh, H. Handchirurgie; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Dellon, A.L.; Mackinnon, S.E.; Crosby, P.M. Reliability of two-point discrimination measurements. J. Hand Surg. Am. 1987, 12 Pt 1, 693–696. [Google Scholar] [CrossRef] [PubMed]
- Finnell, J.T.; Knopp, R.; Johnson, P.; Holland, P.C.; Schubert, W. A calibrated paper clip is a reliable measure of two-point discrimination. Acad. Emerg. Med. 2004, 11, 710–714. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Williams, N. Dash. Occup. Med. 2014, 64, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Canada Institute for Work & Health. Der DASH-Fragebogen Totonto: Institute for Work. & Health Canada. 2006. Available online: https://www.dash.iwh.on.ca/sites/dash/public/translations/DASH_German_2012.pdf (accessed on 5 March 2024).
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Canada Institute for Work & Health. What Is Considered to Be a Clinically Important Change for the DASH/QuickDASH? Toronto: Institute for Work & Health Canada 2006–2020. Available online: https://www.dash.iwh.on.ca/faq/what-considered-be-clinically-important-change-dashquickdash (accessed on 5 March 2024).
- Randall, D.J.; Zhang, Y.; Li, H.; Hubbard, J.C.; Kazmers, N.H. Establishing the Minimal Clinically Important Difference and Substantial Clinical Benefit for the Pain Visual Analog Scale in a Postoperative Hand Surgery Population. J. Hand Surg. Am. 2022, 47, 645–653. [Google Scholar] [CrossRef]
- Edwards, S.G.; Johansen, J.A. Prospective outcomes and associations of wrist ganglion cysts resected arthroscopically. J. Hand Surg. Am. 2009, 34, 395–400. [Google Scholar] [CrossRef]
- Chung, S.R.; Tay, S.C. Audit of Clinical and Functional Outcomes of Arthroscopic Resection of Wrist Ganglions. Hand Surg. 2015, 20, 415–420. [Google Scholar] [CrossRef]
- Tan, S.W.; Ng, S.W.; Tan, S.H.; Teoh, L.C. Arthroscopic debridement of intercarpal ligament and triangular fibrocartilage complex tears. Singap. Med. J. 2012, 53, 188–191. [Google Scholar]
- Gallego, S.; Mathoulin, C. Arthroscopic resection of dorsal wrist ganglia: 114 cases with minimum follow-up of 2 years. Arthroscopy 2010, 26, 1675–1682. [Google Scholar] [CrossRef] [PubMed]
- Broccoli, G.; Vaske, B.; Müller, L.; Kahmann, R.; Isenberg, J. Limits to arthroscopic treatment of degenerative triangular fibrocartilage complex lesions depending on the ulnar variance. Handchir. Mikrochir. Plast. Chir. 2014, 46, 151–162. [Google Scholar] [PubMed]
- Teng, X.; Xu, J.; Yuan, H.; He, X.; Chen, H. Comparison of Wrist Arthroscopy, Small Incision Surgery, and Conventional Surgery for the Treatment of Carpal Tunnel Syndrome: A Retrospective Study at a Single Center. Med. Sci. Monit. 2019, 25, 4122–4129. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Del Vescovo, R.; Cazzato, L.; Zobel, B.B.; Maffulli, N.; Denaro, V. Safety of dorsal wrist arthroscopy portals: A magnetic resonance study. Surgeon 2018, 16, 101–106. [Google Scholar] [CrossRef]
- Landgren, M.; Abramo, A.; Geijer, M.; Kopylov, P.; Tagil, M. Similar 1-year subjective outcome after a distal radius fracture during the 10-year-period 2003–2012. Acta Orthop. 2017, 88, 451–456. [Google Scholar] [CrossRef]
- Jester, A.; Harth, A.; Wind, G.; Germann, G.; Sauerbier, M. Disabilities of the arm, shoulder and hand (DASH) questionnaire: Determining functional activity profiles in patients with upper extremity disorders. J. Hand Surg. Br. 2005, 30, 23–28. [Google Scholar] [CrossRef]
- Saito, T.; Malay, S.; Chung, K.C. A Systematic Review of Outcomes after Arthroscopic Débridement for Triangular Fibrocartilage Complex Tear. Plast. Reconstr. Surg. 2017, 140, 697e–708e. [Google Scholar] [CrossRef]
- Arsalan-Werner, A.; Grüter, L.; Mehling, I.M.; Moll, W.; Wölfle, O.; Sauerbier, M. Results after arthroscopic treatment of central traumatic lesions of the triangular fibrocartilage complex. Arch. Orthop. Trauma. Surg. 2018, 138, 731–737. [Google Scholar] [CrossRef]
- Minami, A.; Ishikawa, J.-i.; Suenaga, N.; Kasashima, T. Clinical results of treatment of triangular fibrocartilage complex tears by arthroscopic debridement. J. Hand Surg. 1996, 21, 406–411. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjective Change in the Wrist Due to the Surgery | Significantly Worse □ | Slightly Worse □ | No Change □ | Slightly Better □ | Significantly Better □ |
|---|
| Pre-OP | 14 Days | 8 Weeks | 7 Months | |
|---|---|---|---|---|
| Objective Outcome measures | ||||
| Range of Motion | Prospective (n = 58) | - | Prospective (n = 27) | Prospective (n = 52) Retrospective (n = 73) |
| Grip Strength | Prospective (n = 59) | - | Prospective (n = 25) | Prospective (n = 54) Retrospective (n = 73) |
| Sensitivity Testing | Prospective (n = 36) | - | - | Prospective (n = 49) Retrospective (n = 46) |
| Patient-reported outcome measures (PROMs) | ||||
| DASH Score | Prospective (n = 63) * Retrospective (n = 86) | Prospective (n = 59) * | Prospective (n = 56) * | Prospective (n = 63) * Retrospective (n = 86) |
| Pain Assessment (NRS) | Prospective (n = 66) Retrospective (n = 86) ** | Prospective (n = 64) | Prospective (n = 68) | Prospective (n = 64) Retrospective (n = 86) |
| Patient Satisfaction | - | - | Prospective (n = 68) | Prospective (n = 64) Retrospective (n = 86) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demmer, W.; Meyer, E.; Ehrl, D.; Volkmer, E.; Lukas, B.; Knie, N.F.; Giunta, R.E.; Wachtel, N. Postoperative Benefits of Soft Tissue Wrist Arthroscopy: Retro- and Prospective Analyses of Outcome Measures. J. Clin. Med. 2024, 13, 2280. https://doi.org/10.3390/jcm13082280
Demmer W, Meyer E, Ehrl D, Volkmer E, Lukas B, Knie NF, Giunta RE, Wachtel N. Postoperative Benefits of Soft Tissue Wrist Arthroscopy: Retro- and Prospective Analyses of Outcome Measures. Journal of Clinical Medicine. 2024; 13(8):2280. https://doi.org/10.3390/jcm13082280
Chicago/Turabian StyleDemmer, Wolfram, Emanuel Meyer, Denis Ehrl, Elias Volkmer, Bernhard Lukas, Nina F. Knie, Riccardo E. Giunta, and Nikolaus Wachtel. 2024. "Postoperative Benefits of Soft Tissue Wrist Arthroscopy: Retro- and Prospective Analyses of Outcome Measures" Journal of Clinical Medicine 13, no. 8: 2280. https://doi.org/10.3390/jcm13082280
APA StyleDemmer, W., Meyer, E., Ehrl, D., Volkmer, E., Lukas, B., Knie, N. F., Giunta, R. E., & Wachtel, N. (2024). Postoperative Benefits of Soft Tissue Wrist Arthroscopy: Retro- and Prospective Analyses of Outcome Measures. Journal of Clinical Medicine, 13(8), 2280. https://doi.org/10.3390/jcm13082280