
Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
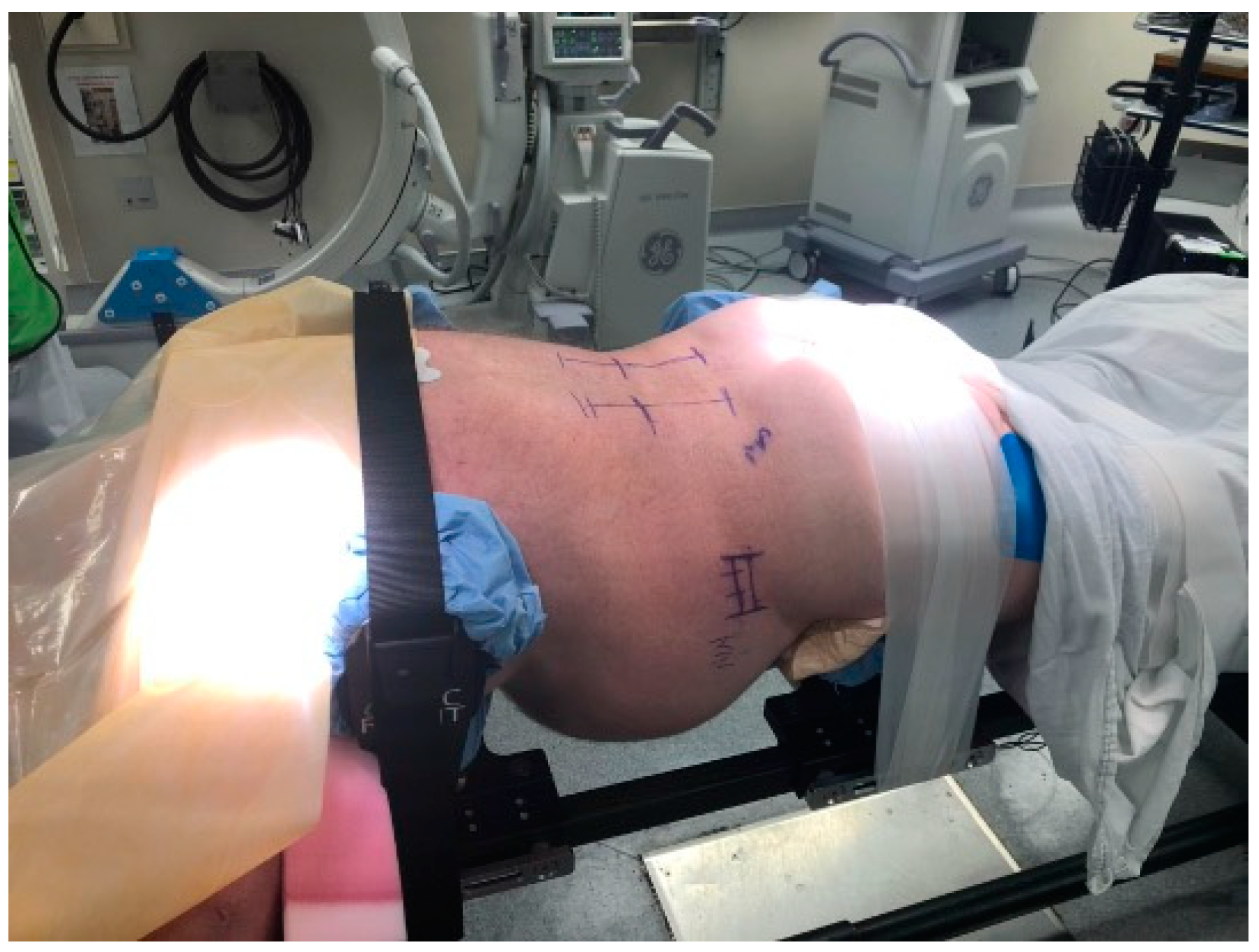
2.2. Technique
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic Information
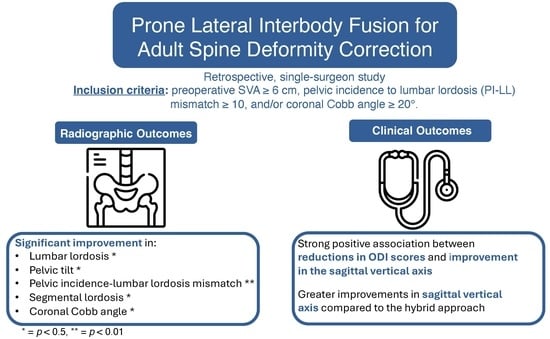
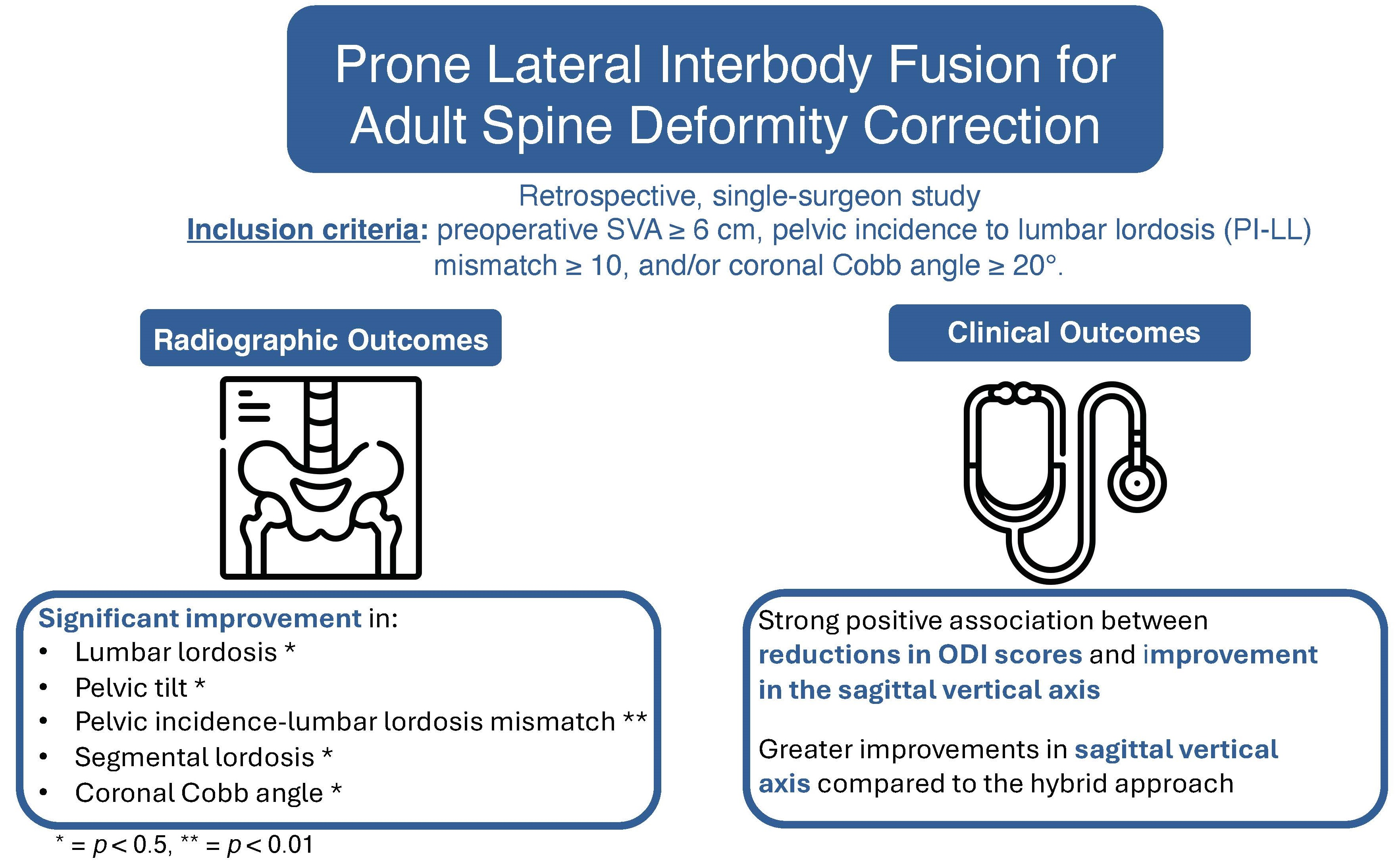
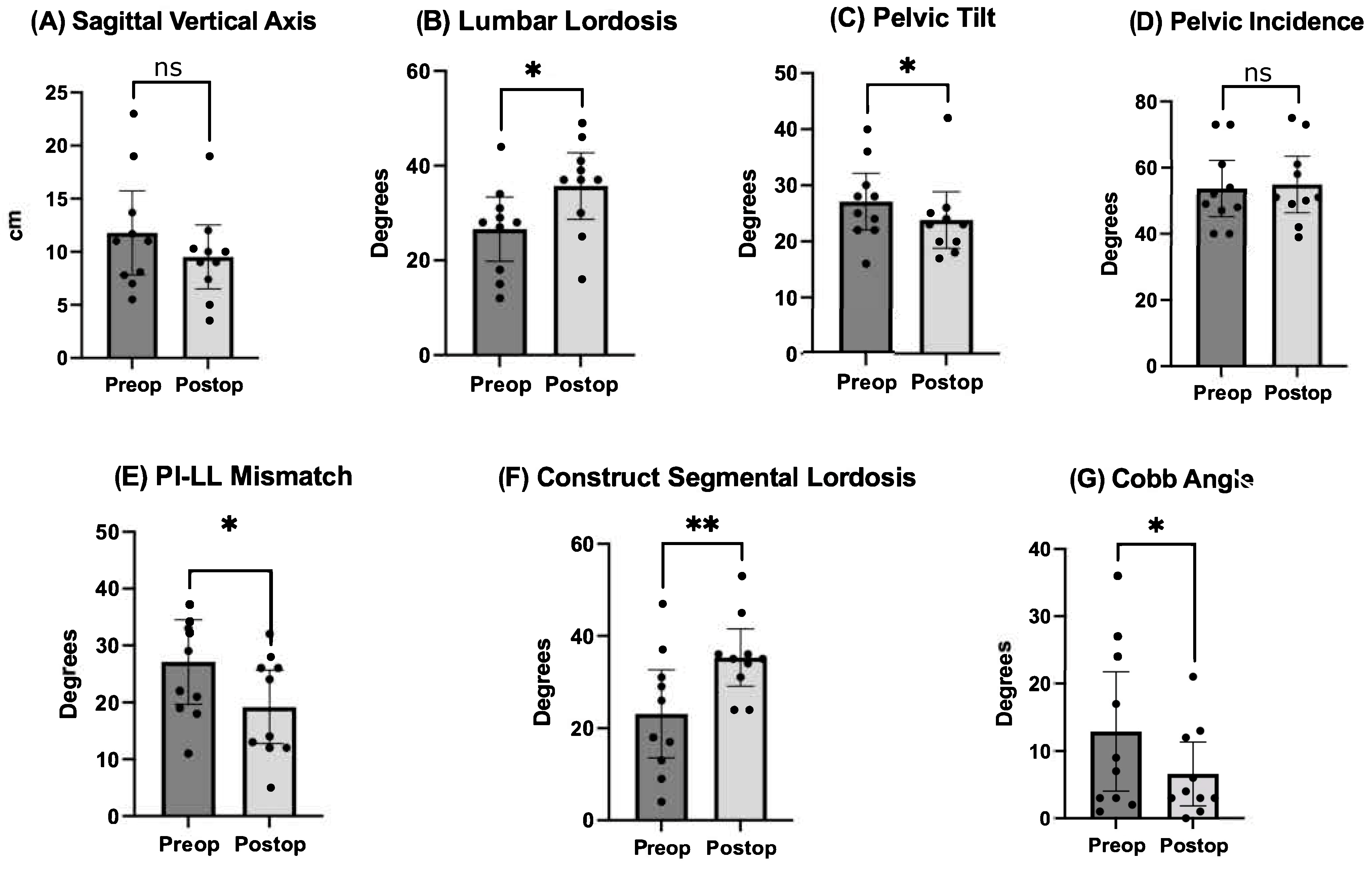
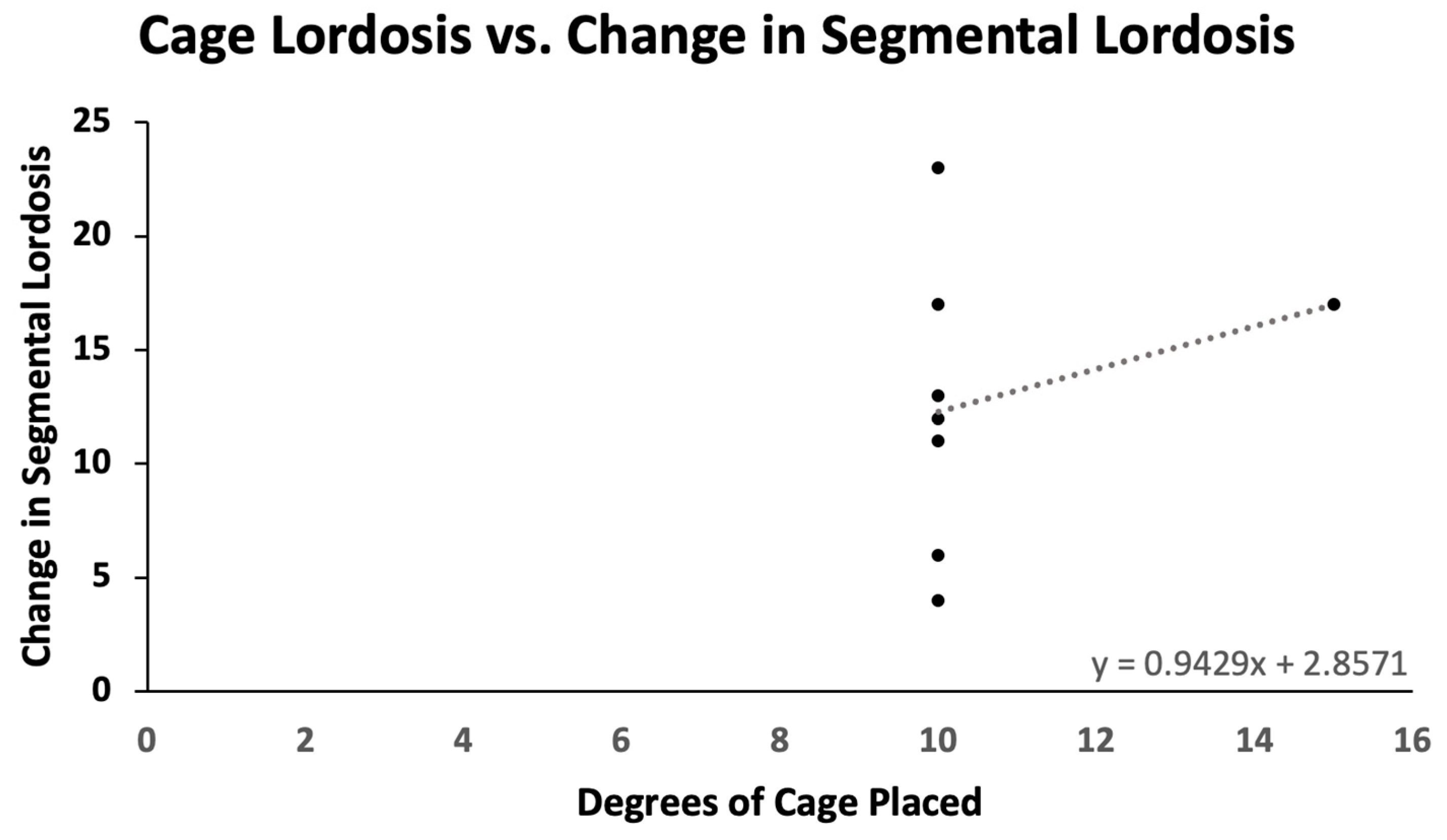
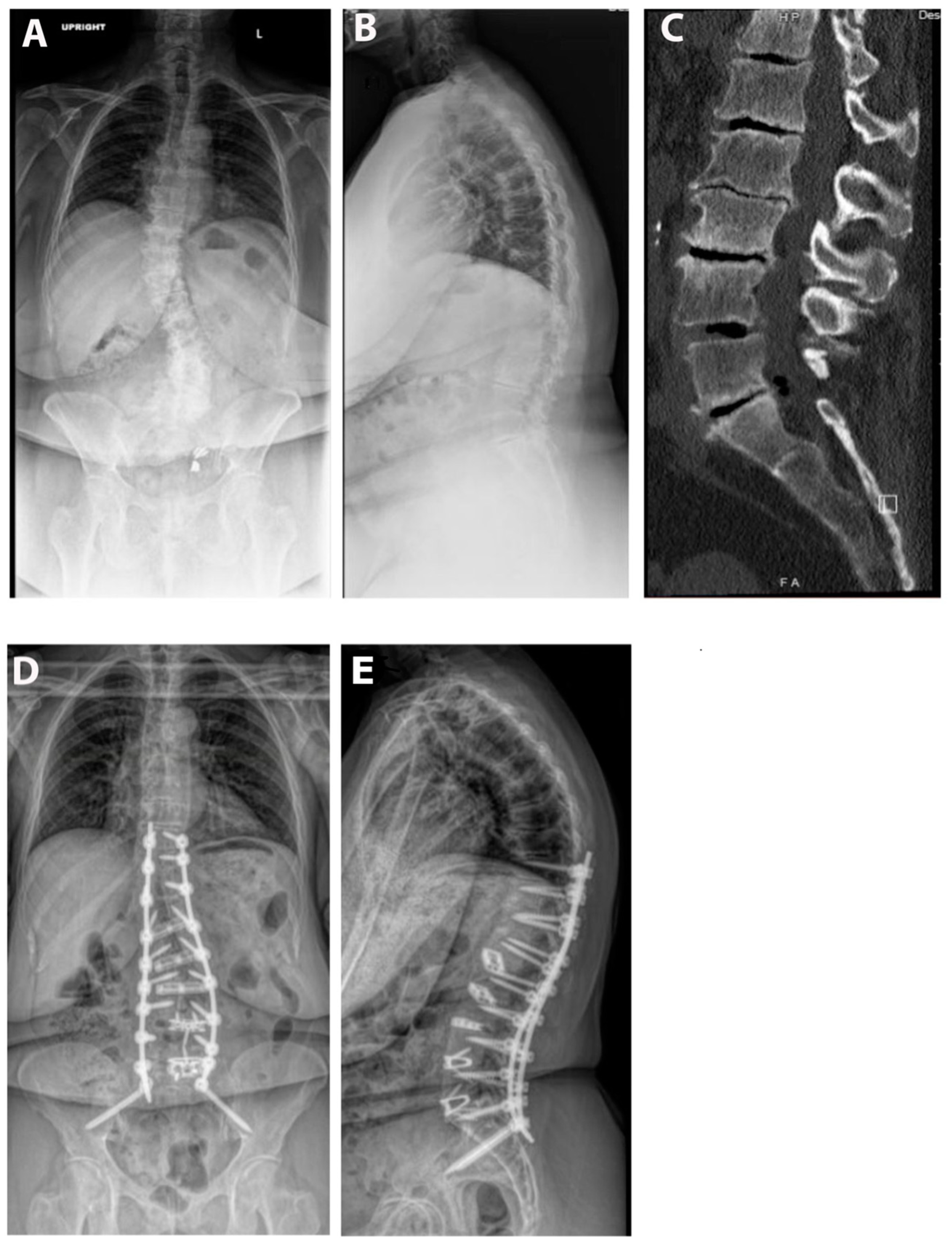
3.2. Radiographic Outcomes
3.3. Clinical Outcomes
3.4. Comparative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheer, J.K.; Hostin, R.; Robinson, C.; Schwab, F.; Lafage, V.; Burton, D.C.; Hart, R.A.; Kelly, M.P.; Keefe, M.; Polly, D.; et al. Operative Management of Adult Spinal Deformity Results in Significant Increases in QALYs Gained Compared to Nonoperative Management: Analysis of 479 Patients With Minimum 2-Year Follow-Up. Spine 2018, 43, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Lazaro, B.; Sardi, J.P.; Smith, J.S.; Kelly, M.P.; Yanik, E.L.; Dial, B.; Hills, J.; Gupta, M.C.; Baldus, C.R.; Yen, C.P.; et al. Proximal Junctional Failure in Primary Thoracolumbar Fusion/Fixation to the Sacrum/Pelvis for Adult Symptomatic Lumbar Scoliosis: Long-Term Follow-up of a Prospective Multicenter Cohort of 160 Patients. J. Neurosurg. Spine 2023, 38, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Daubs, M.D.; Lenke, L.G.; Cheh, G.; Stobbs, G.; Bridwell, K.H. Adult Spinal Deformity Surgery: Complications and Outcomes in Patients over Age 60. Spine 2007, 32, 2238–2244. [Google Scholar] [CrossRef]
- Januszewski, J.; Vivas, A.C.; Uribe, J.S. Limitations and Complications of Minimally Invasive Spinal Surgery in Adult Deformity. Ann. Transl. Med. 2018, 6, 109. [Google Scholar] [CrossRef]
- Bakare, A.A.; Fessler, D.R.; Wewel, J.T.; Fontes, R.B.V.; Fessler, R.G.; O’Toole, J.E. Changes in Segmental and Lumbar Lordosis After Lateral Lumbar Interbody Fusion With Different Lordotic Cage Angulations. Int. J. Spine Surg. 2021, 15, 440–448. [Google Scholar] [CrossRef]
- Amaral, R.; Moriguchi, R.; Pokorny, G.; Arnoni, D.; Barreira, I.; Marcelino, F.; Pokorny, J.; Pimenta, L. Comparison of Segmental Lordosis Gain of Prone Transpsoas (PTP) vs. Lateral Lumbar Interbody Fusion. Arch. Orthop. Trauma Surg. 2023, 143, 5485–5490. [Google Scholar] [CrossRef] [PubMed]
- Soliman, M.A.R.; Aguirre, A.O.; Ruggiero, N.; Kuo, C.C.; Mariotti, B.L.; Khan, A.; Mullin, J.P.; Pollina, J. Comparison of Prone Transpsoas Lateral Lumbar Interbody Fusion and Transforaminal Lumbar Interbody Fusion for Degenerative Lumbar Spine Disease: A Retrospective Radiographic Propensity Score-Matched Analysis. Clin. Neurol. Neurosurg. 2022, 213, 107105. [Google Scholar] [CrossRef]
- Ziino, C.; Konopka, J.A.; Ajiboye, R.M.; Ledesma, J.B.; Koltsov, J.C.B.; Cheng, I. Single Position versus Lateral-Then-Prone Positioning for Lateral Interbody Fusion and Pedicle Screw Fixation. J. Spine Surg. 2018, 4, 717–724. [Google Scholar] [CrossRef]
- Pimenta, L.; Taylor, W.R.; Stone, L.E.; Wali, A.R.; Santiago-Dieppa, D.R. Prone Transpsoas Technique for Simultaneous Single-Position Access to the Anterior and Posterior Lumbar Spine. Oper. Neurosurg. 2020, 20, E5–E12. [Google Scholar] [CrossRef]
- Farber, S.H.; Valenzuela Cecchi, B.; O’Neill, L.K.; Chapple, K.M.; Zhou, J.J.; Alan, N.; Gooldy, T.C.; DiDomenico, J.D.; Snyder, L.A.; Turner, J.D.; et al. Complications Associated with Single-Position Prone Lateral Lumbar Interbody Fusion: A Systematic Review and Pooled Analysis. J. Neurosurg. Spine 2023, 39, 380–386. [Google Scholar] [CrossRef]
- Theologis, A.A.; Mundis, G.M.; Nguyen, S.; Okonkwo, D.O.; Mummaneni, P.V.; Smith, J.S.; Shaffrey, C.I.; Fessler, R.; Bess, S.; Schwab, F.; et al. Utility of Multilevel Lateral Interbody Fusion of the Thoracolumbar Coronal Curve Apex in Adult Deformity Surgery in Combination with Open Posterior Instrumentation and L5-S1 Interbody Fusion: A Case-Matched Evaluation of 32 Patients. J. Neurosurg. Spine 2017, 26, 208–219. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.E.; O’Hehir, M.M.; Mao, J.Z.; Mullin, J.P.; Pollina, J. Prone Transpsoas Approach for Adjacent Segment Disease and Flatback Deformity: Technical Note and Case Report. Open J. Mod. Neurosurg. 2021, 11, 20–28. [Google Scholar] [CrossRef]
- Wang, T.Y.; Mehta, V.A.; Sankey, E.W.; Shaffrey, C.I.; Than, K.D.; Taylor, W.R.; Pollina, J.; Pimenta, L.; Abd-El-Barr, M.M. Single-Position Prone Transpsoas Fusion for the Treatment of Lumbar Adjacent Segment Disease: Early Experience of Twenty-Four Cases across Three Tertiary Medical Centers. Eur. Spine J. 2022, 31, 2255–2261. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.K.; Eastlack, R.K.; Fessler, R.G.; Than, K.D.; Chou, D.; Fu, K.-M.; Park, P.; Wang, M.Y.; Kanter, A.S.; Okonkwo, D.O.; et al. Two- and Three-Year Outcomes of Minimally Invasive and Hybrid Correction of Adult Spinal Deformity. J. Neurosurg. Spine 2022, 36, 595–608. [Google Scholar] [CrossRef] [PubMed]
- Wellington, I.J.; Antonacci, C.L.; Chaudhary, C.; Coskun, E.; Cote, M.P.; Singh, H.; Mallozzi, S.S.; Moss, I.L. Early Clinical Outcomes of the Prone Transpsoas Lumbar Interbody Fusion Technique. Int. J. Spine Surg. 2023, 17, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Fritzell, P.; Hägg, O.; Nordwall, A. Swedish Lumbar Spine Study Group Complications in Lumbar Fusion Surgery for Chronic Low Back Pain: Comparison of Three Surgical Techniques Used in a Prospective Randomized Study. A Report from the Swedish Lumbar Spine Study Group. Eur. Spine J. 2003, 12, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Saigal, R.; Mundis, G.M.; Eastlack, R.; Uribe, J.S.; Phillips, F.M.; Akbarnia, B.A. Anterior Column Realignment (ACR) in Adult Sagittal Deformity Correction: Technique and Review of the Literature. Spine 2016, 41 (Suppl. S8), S66–S73. [Google Scholar] [CrossRef] [PubMed]
- Mundis, G.M.; Turner, J.D.; Kabirian, N.; Pawelek, J.; Eastlack, R.K.; Uribe, J.; Klineberg, E.; Bess, S.; Ames, C.; Deviren, V.; et al. Anterior Column Realignment Has Similar Results to Pedicle Subtraction Osteotomy in Treating Adults with Sagittal Plane Deformity. World Neurosurg. 2017, 105, 249–256. [Google Scholar] [CrossRef]
- Shen, F.H.; Mason, J.R.; Shimer, A.L.; Arlet, V.M. Pelvic Fixation for Adult Scoliosis. Eur. Spine J. 2013, 22 (Suppl. S2), S265–S275. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Bridwell, K.H.; Kuklo, T.R.; Lenke, L.G.; Baldus, C. Minimum 5-Year Analysis of L5-S1 Fusion Using Sacropelvic Fixation (Bilateral S1 and Iliac Screws) for Spinal Deformity. Spine 2006, 31, 303–308. [Google Scholar] [CrossRef]
- Lovecchio, F.C.; Vaishnav, A.S.; Steinhaus, M.E.; Othman, Y.A.; Gang, C.H.; Iyer, S.; McAnany, S.J.; Albert, T.J.; Qureshi, S.A. Does Interbody Cage Lordosis Impact Actual Segmental Lordosis Achieved in Minimally Invasive Lumbar Spine Fusion? Neurosurg. Focus 2020, 49, E17. [Google Scholar] [CrossRef]
- Lee, N.J.; Marciano, G.; Puvanesarajah, V.; Park, P.J.; Clifton, W.E.; Kwan, K.; Morrissette, C.R.; Williams, J.L.; Fields, M.; Hassan, F.M.; et al. Incidence, Mechanism, and Protective Strategies for 2-Year Pelvic Fixation Failure after Adult Spinal Deformity Surgery with a Minimum Six-Level Fusion. J. Neurosurg. Spine 2023, 38, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Mundis, G.M.; Klineberg, E.; Hart, R.A.; Deviren, V.; Burton, D.C.; Protopsaltis, T.S.; Gupta, M.; Rolston, J.D.; Bess, S.; et al. Recovery Following Adult Spinal Deformity Surgery: The Effect of Complications and Reoperation in 149 Patients with 2-Year Follow-Up. Eur. Spine J. 2016, 25, 2612–2621. [Google Scholar] [CrossRef] [PubMed]
- Faraj, S.S.A.; De Kleuver, M.; Vila-Casademunt, A.; Holewijn, R.M.; Obeid, I.; Acaroğlu, E.; Alanay, A.; Kleinstück, F.; Pérez-Grueso, F.S.; Pellisé, F. Sagittal Radiographic Parameters Demonstrate Weak Correlations with Pretreatment Patient-Reported Health-Related Quality of Life Measures in Symptomatic de Novo Degenerative Lumbar Scoliosis: A European Multicenter Analysis. J. Neurosurg. Spine 2018, 28, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, D.K.; Kong, C.; Hiratzka, J.; Contag, A.G.; Ailon, T.; Line, B.; Daniels, A.; Smith, J.S.; Passias, P.; Protopsaltis, T.; et al. Patient Satisfaction After Adult Spinal Deformity Surgery Does Not Strongly Correlate With Health-Related Quality of Life Scores, Radiographic Parameters, or Occurrence of Complications. Spine 2017, 42, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Massie, L.W.; Macki, M.; Zakaria, H.M.; Gilmore, M.; Basheer, A.; Chang, V.W.; La Marca, F. Anterior Column Reconstruction vs Pedicle Subtraction Osteotomy for Severe Sagittal Plane Deformity: Early Clinical and Radiographic Outcomes Using a Hyperlordotic Expandable Lateral Interbody Device. Neurosurgery 2019, 66, 310. [Google Scholar] [CrossRef]
- Lau, D.; Haddad, A.F.; Deviren, V.; Ames, C.P. Complication Profile Associated with S1 Pedicle Subtraction Osteotomy Compared with 3-Column Osteotomies at Other Thoracolumbar Levels for Adult Spinal Deformity: Series of 405 Patients with 9 S1 Osteotomies. J. Neurosurg. Spine 2020, 33, 577–587. [Google Scholar] [CrossRef]
- Buchowski, J.M.; Bridwell, K.H.; Lenke, L.G.; Kuhns, C.A.; Lehman, R.A.; Kim, Y.J.; Stewart, D.; Baldus, C. Neurologic Complications of Lumbar Pedicle Subtraction Osteotomy: A 10-Year Assessment. Spine 2007, 32, 2245–2252. [Google Scholar] [CrossRef]
- Godzik, J.; de Andrada Pereira, B.; Hemphill, C.; Walker, C.T.; Wewel, J.T.; Turner, J.D.; Uribe, J.S. Minimally Invasive Anterior Longitudinal Ligament Release for Anterior Column Realignment. Glob. Spine J. 2020, 10, 101S–110S. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Park, P.; Shaffrey, C.I.; Wang, M.Y.; Uribe, J.S.; Fessler, R.G.; Chou, D.; Kanter, A.S.; Okonkwo, D.O.; Mundis, G.M.; et al. The MISDEF2 Algorithm: An Updated Algorithm for Patient Selection in Minimally Invasive Deformity Surgery. J. Neurosurg. Spine 2019, 32, 221–228. [Google Scholar] [CrossRef]
- McCarthy, M.H.; Lafage, R.; Smith, J.S.; Bess, S.; Ames, C.P.; Klineberg, E.O.; Kim, H.J.; Shaffrey, C.I.; Burton, D.C.; Mundis, G.M.; et al. How Much Lumbar Lordosis Does a Patient Need to Reach Their Age-Adjusted Alignment Target? A Formulated Approach Predicting Successful Surgical Outcomes. Glob. Spine J. 2022, 14, 21925682221092003. [Google Scholar] [CrossRef]
- Phan, K.; Kim, J.S.; Capua, J.D.; Lee, N.J.; Kothari, P.; Dowdell, J.; Overley, S.C.; Guzman, J.Z.; Cho, S.K. Impact of Operation Time on 30-Day Complications After Adult Spinal Deformity Surgery. Glob. Spine J. 2017, 7, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Cho, K.-J.; Edwards, C.C.; Rinella, A.S. Pseudarthrosis in Adult Spinal Deformity Following Multisegmental Instrumentation and Arthrodesis. J. Bone Jt. Surg. Am. 2006, 88, 721–728. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Glattes, C.R.; Rhim, S.; Cheh, G. Proximal Junctional Kyphosis in Adult Spinal Deformity after Segmental Posterior Spinal Instrumentation and Fusion: Minimum Five-Year Follow-Up. Spine 2008, 33, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Shaffrey, C.I.; Lenke, L.G.; Park, P.; Wang, M.Y.; La Marca, F.; Smith, J.S.; Mundis, G.M.; Okonkwo, D.O.; Moal, B.; et al. The Minimally Invasive Spinal Deformity Surgery Algorithm: A Reproducible Rational Framework for Decision Making in Minimally Invasive Spinal Deformity Surgery. Neurosurg. Focus 2014, 36, E6. [Google Scholar] [CrossRef] [PubMed]
- Labelle, H.; Roussouly, P.; Berthonnaud, E.; Dimnet, J.; O’Brien, M. The Importance of Spino-Pelvic Balance in L5-S1 Developmental Spondylolisthesis: A Review of Pertinent Radiologic Measurements. Spine 2005, 30, S27–S34. [Google Scholar] [CrossRef]
- Labelle, H.; Mac-Thiong, J.-M.; Roussouly, P. Spino-Pelvic Sagittal Balance of Spondylolisthesis: A Review and Classification. Eur. Spine J. 2011, 20, 641–646. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Mean (SD) |
|---|---|
| Sex | 70% Male, 30% Female |
| Age (Years) | 67.5 (5.8) |
| BMI (kg/m2) | 30.3 (4.6) |
| Active Smoking Status | 20% |
| Diabetes | 0% |
| Osteoporosis | 0% |
| Previous Surgeries | 20% Lumbar Decompression 20% Posterior Spinal Fusion |
| Metrics | Mean (SD) |
|---|---|
| Number of Operative Levels | 4.0 (1.5) |
| Number of Lateral Levels | 2.2 (0.6) |
| Direction of Approach | 80% Left, 20% Right |
| Skin-to-Skin (min) | 569 (158) |
| Fluoroscopy Dose (mGy) | 316 (97) |
| Estimated Blood Loss (mL) | 1010 (723) |
| Length of Hospital Stay (days) | 5.7 (2.2) |
| Complications (n patients) | Constipation (1) SI Joint Pain (1) Transient Weakness (1) |
| Radiographic Parameter | Baseline Mean (SD) | Postop Mean (SD) | Change Mean (SD) | p |
|---|---|---|---|---|
| Sagittal Vertical Axis (cm) | 11.8 (5.5) | 9.5 (4.2) | −2.4 (2.5) | 0.15 |
| Lumbar Lordosis (°) | 26.6 (9.5) | 35.7 (9.8) | +9.1 (9.6) | 0.01 |
| Pelvic Tilt (°) | 27.1 (7.0) | 23.8 (7.3) | −3.3 (4.5) | 0.04 |
| Pelvic Incidence (°) | 53.7 (11.9) | 54.9 (12.0) | 1.2 (5.0) | 0.27 |
| PI-LL Mismatch (°) | 27.1 (10.4) | 19.2 (9.0) | −7.9 (9.8) | 0.01 |
| Construct Segmental Lordosis (°) | 23.1 (12.6) | 35.3 (8.3) | +12.2 (8.8) | 0.004 |
| Cobb Angle (°) | 12.9 (12.4) | 6.6 (6.7) | −6.3 (9.4) | 0.03 |
| Change in Radiographic Parameter | Change in PROs | |
|---|---|---|
| ODI | VAS | |
| Sagittal Vertical Axis (cm) | −0.5778 | 0.1274 |
| Lumbar Lordosis (°) | −0.4772 | 0.3039 |
| Pelvic Tilt (°) | −0.3069 | −0.3377 |
| PI-LL Mismatch (°) | −0.4772 | 0.3039 |
| Segmental Lordosis (°) | −0.4421 | 0.4469 |
| Cobb Angle (°) | −0.1383 | −0.0765 |
| Radiographic Parameter | Prone Lateral | MIS | Hybrid | F | p |
|---|---|---|---|---|---|
| Sagittal Vertical Axis (cm) | −2.4 (2.5) | −0.59 (0.6) | 0.27 (4.9) | 3.7926 | 0.02 |
| Pelvic Tilt (°) | −3.3 (4.5) | 0.6 (7.1) | −0.1 (7.9) | 1.3467 | 0.26 |
| PI-LL Mismatch (°) | −7.9 (9.8) | −3.8 (14.7) | −6.8 (16.8) | 1.0672 | 0.35 |
| Cobb Angle (°) | −6.3 (9.4) | −14.5 (2.6) | −20.9 (13.6) | 18.1661 | <0.0001 |
| ODI | −11.6 (6.3) | −21.1 (21.1) | −19.3 (18) | 0.7865 | 0.4568 |
| VAS | −3.0 (1.4) | −2.8 (2.9) | −3.6 (2.8) | 25.6580 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartlett, A.M.; Dibble, C.F.; Sykes, D.A.W.; Drossopoulos, P.N.; Wang, T.Y.; Crutcher, C.L.; Than, K.D.; Bhomwick, D.A.; Shaffrey, C.I.; Abd-El-Barr, M.M. Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience. J. Clin. Med. 2024, 13, 2279. https://doi.org/10.3390/jcm13082279
Bartlett AM, Dibble CF, Sykes DAW, Drossopoulos PN, Wang TY, Crutcher CL, Than KD, Bhomwick DA, Shaffrey CI, Abd-El-Barr MM. Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience. Journal of Clinical Medicine. 2024; 13(8):2279. https://doi.org/10.3390/jcm13082279
Chicago/Turabian StyleBartlett, Alyssa M., Christopher F. Dibble, David A. W. Sykes, Peter N. Drossopoulos, Timothy Y. Wang, Clifford L. Crutcher, Khoi D. Than, Deb A. Bhomwick, Christopher I. Shaffrey, and Muhammad M. Abd-El-Barr. 2024. "Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience" Journal of Clinical Medicine 13, no. 8: 2279. https://doi.org/10.3390/jcm13082279
APA StyleBartlett, A. M., Dibble, C. F., Sykes, D. A. W., Drossopoulos, P. N., Wang, T. Y., Crutcher, C. L., Than, K. D., Bhomwick, D. A., Shaffrey, C. I., & Abd-El-Barr, M. M. (2024). Early Experience with Prone Lateral Interbody Fusion in Deformity Correction: A Single-Institution Experience. Journal of Clinical Medicine, 13(8), 2279. https://doi.org/10.3390/jcm13082279