

Retrospective Study of the Prevalence and Associated Factors of Gallbladder Polyps among Residents of Two Korean Cities


Abstract
:1. Introduction
2. Methods
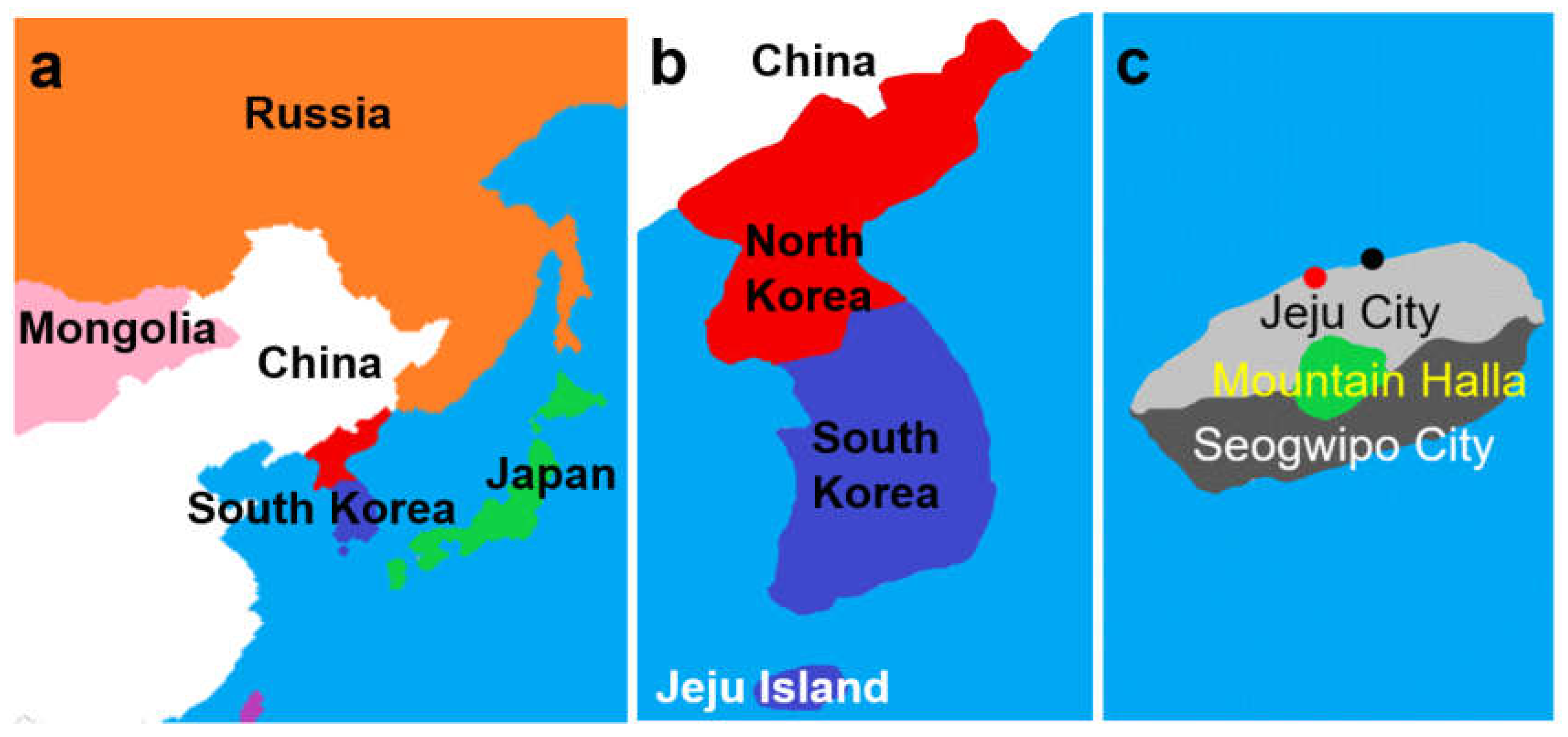
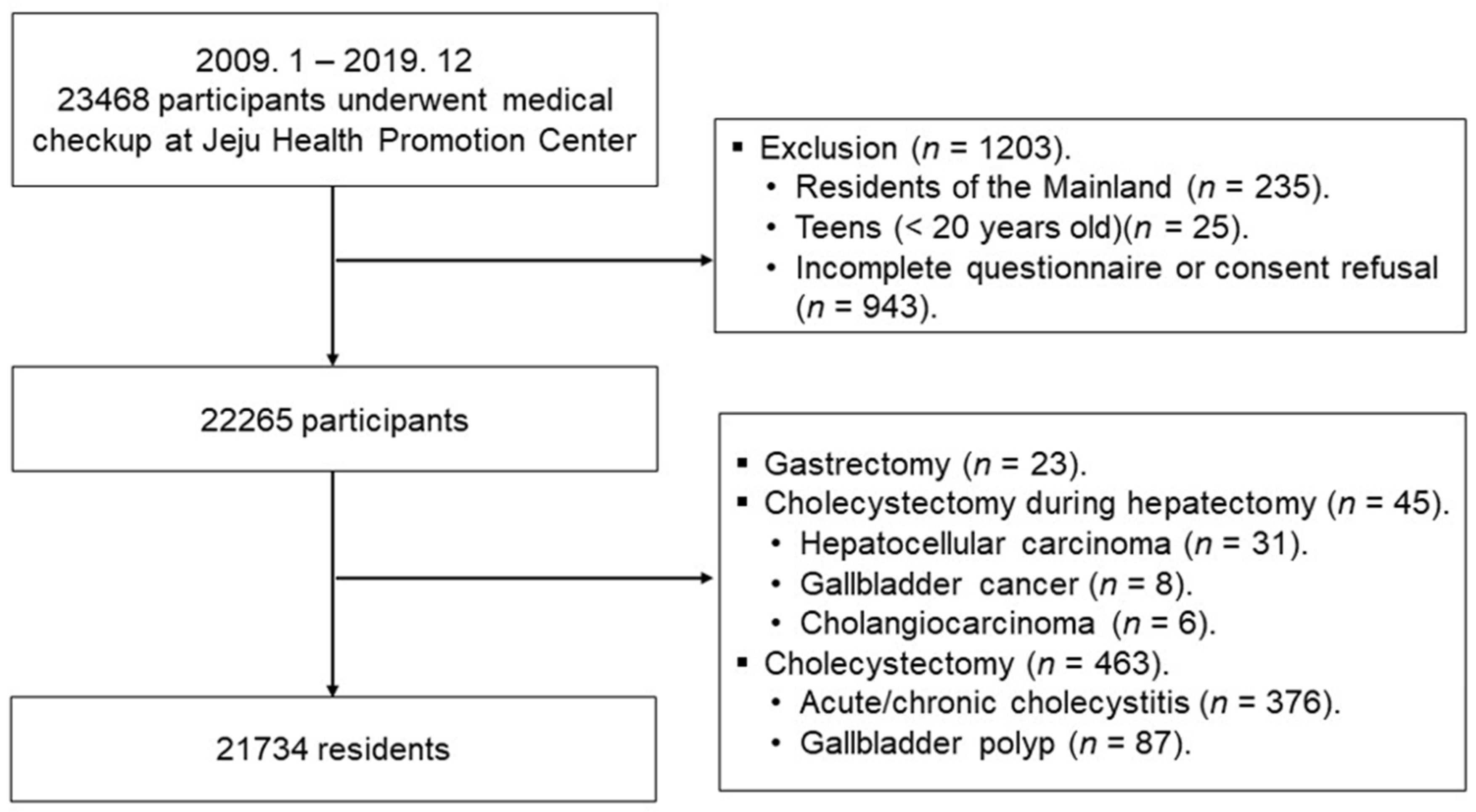
2.1. Residents
2.2. Questionnaire
2.3. Diagnosis of GBPs
2.4. Definition of Physical Activity
2.5. Definitions of High-Risk Alcohol Drinkers and Metabolic Syndrome
2.6. Physical Examination
2.7. Statistical Analysis
3. Results
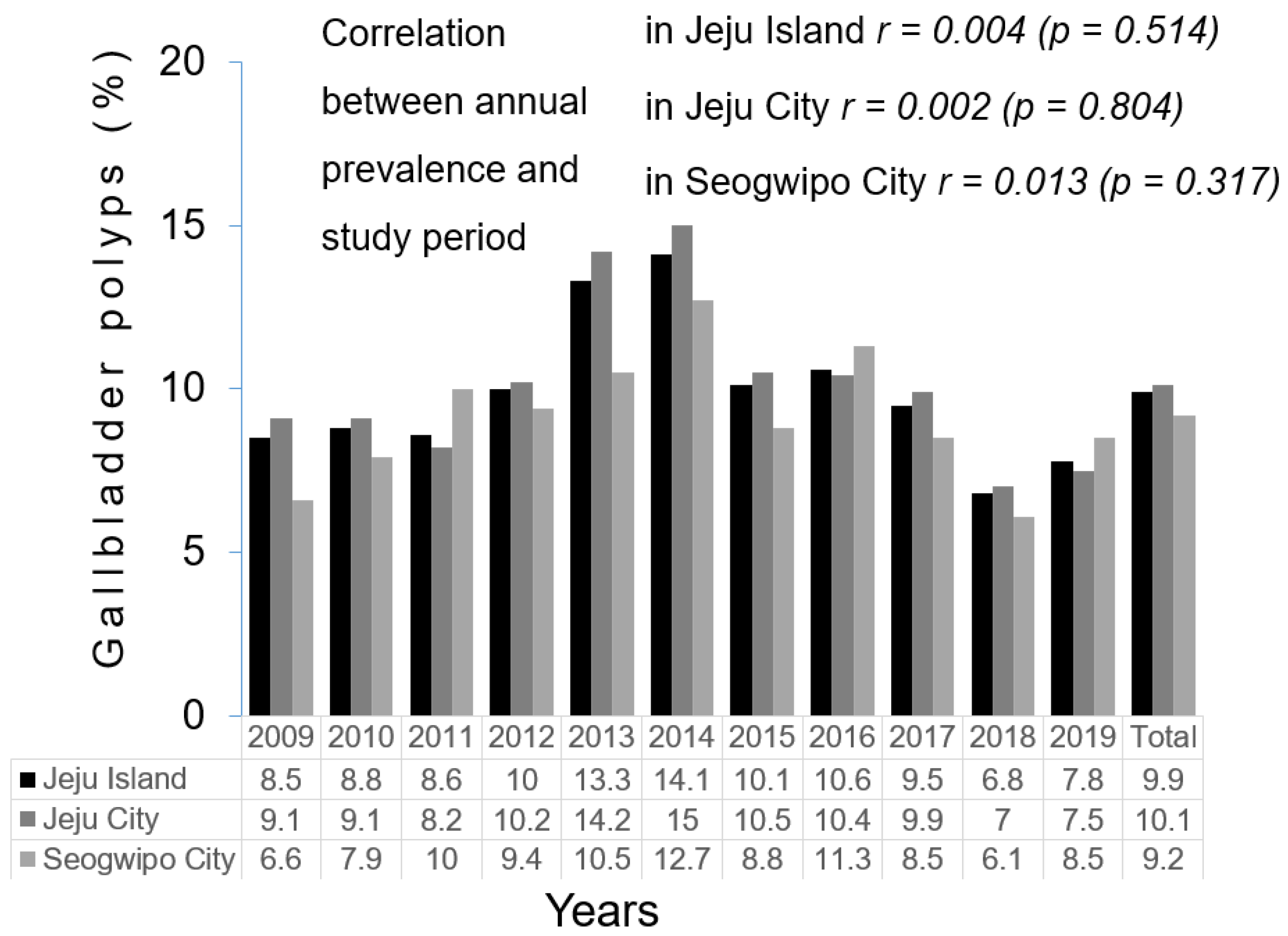
3.1. Overall and Annual Prevalence of GBPs
3.2. Comparisons of Factors Affecting GBPs
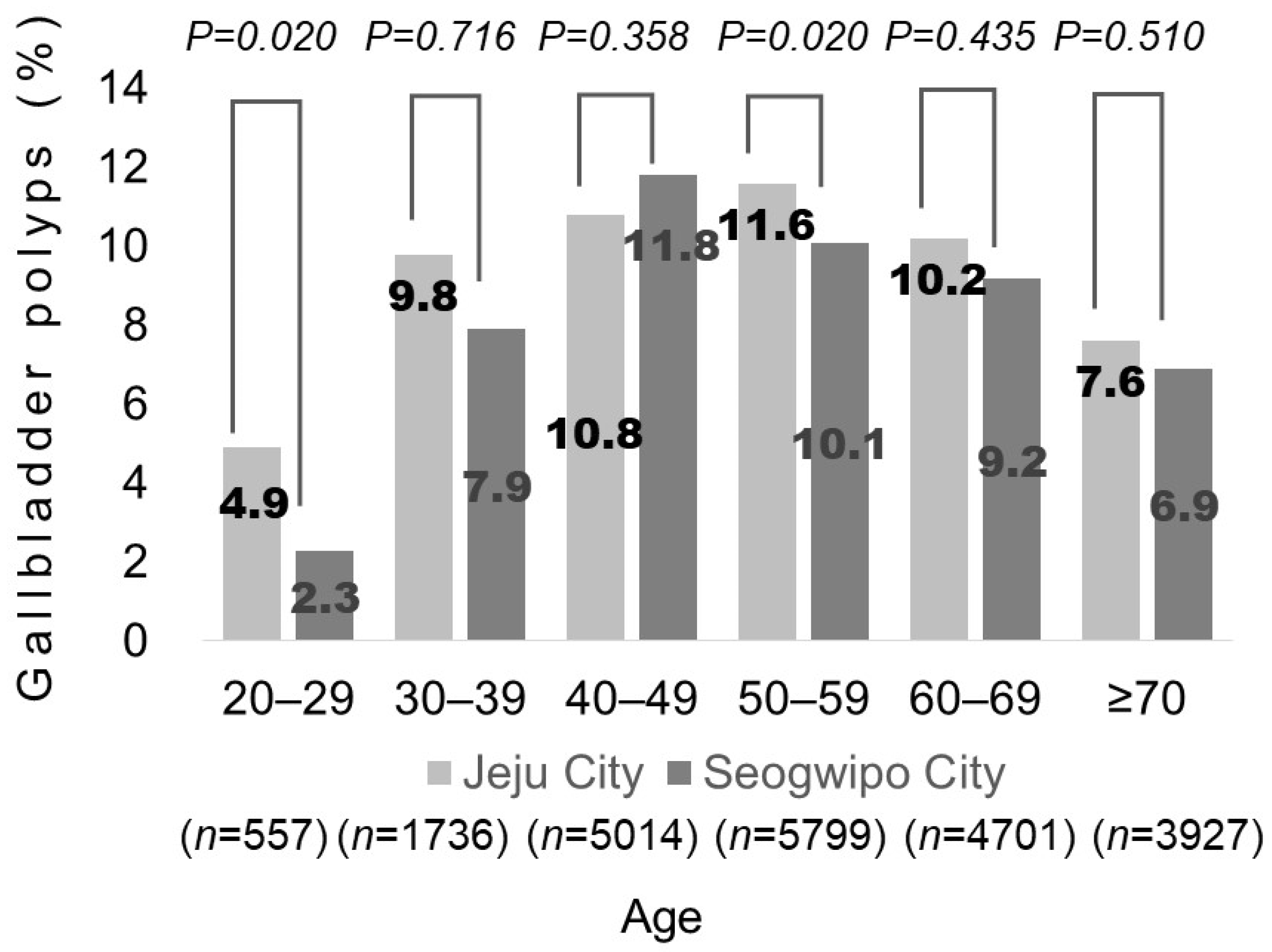
3.3. GBP Prevalence According to Age
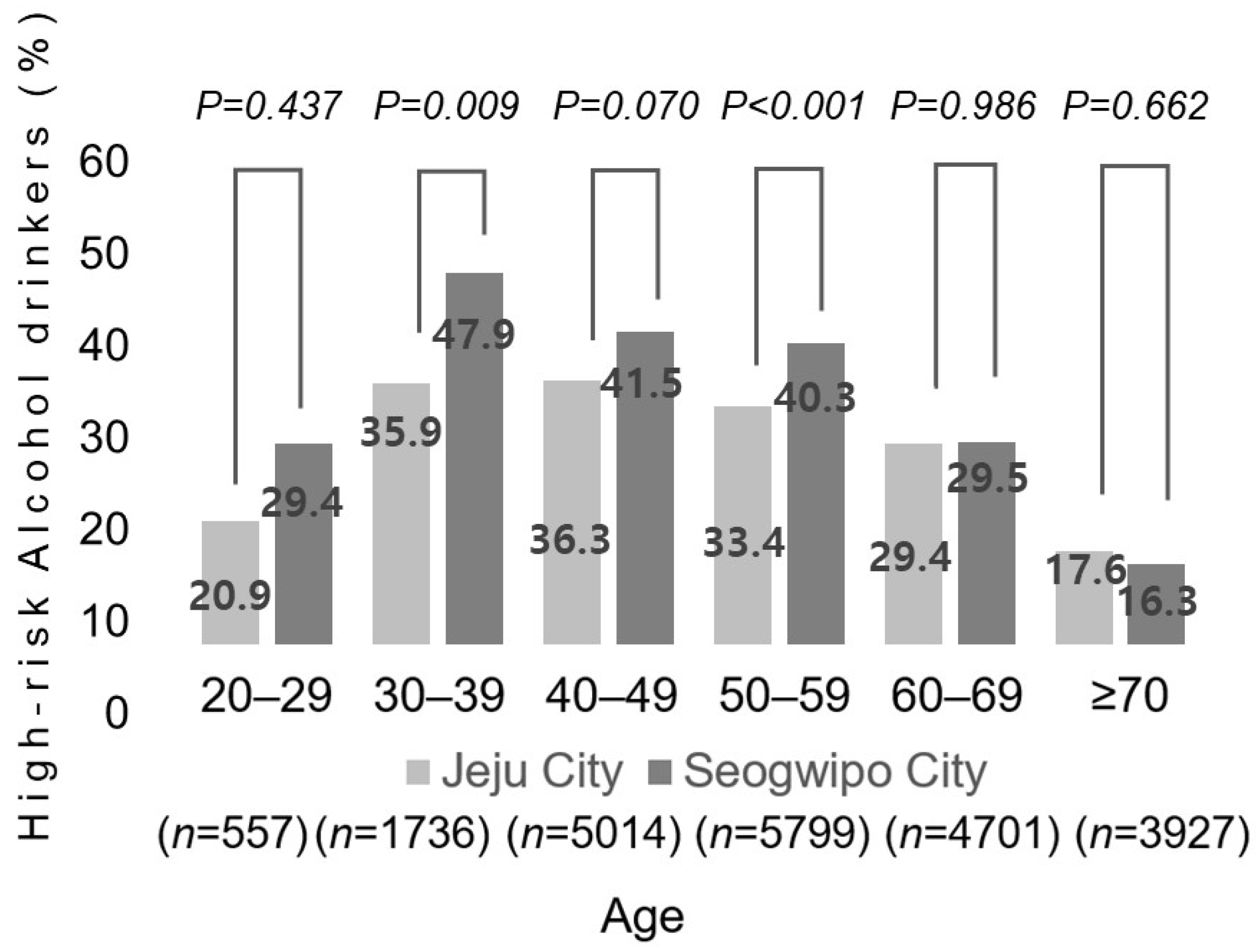
3.4. Prevalence of GBPs and Proportions of High-Risk Alcohol Drinkers According to Age Group by Decade
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Lee, Y.J.; Park, K.S.; Cho, K.B.; Kim, E.S.; Jang, B.K.; Chung, W.J.; Hwang, J.S. Shifting prevalence of gallbladder polyps in Korea. J. Korean Med. Sci. 2014, 29, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Do, J.H.; Seo, S.W.; Lee, S.E.; Oh, H.C.; Min, Y.J.; Kang, H. Prevalence and Risk Factors of Gallbladder Polypoid Lesions in a Healthy Population. Yonsei Med. J. 2016, 57, 1370–1375. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.G.; Lee, K.T.; Lee, J.K.; Park, J.H.; Ryu, K.H.; Rhee, P.L.; Kim, J.J.; Koh, K.C.; Paik, S.W.; Rhee, J.C. Prevalence and risk factors of gallbladder polyps in health screening subjects. Korean J. Med. 1999, 57, 1014–1020. [Google Scholar]
- Lee, E.S. Recent updates on the diagnosis and management of gallbladder polyps. Korean J. Pancreas Biliary Tract. 2014, 19, 64–70. [Google Scholar] [CrossRef]
- Kwon, O.-S.; Kim, Y.-K.; Her, K.H. The prevalence of gallstone disease is significantly lower in natives than in migrants of Jeju Island. Korean J. Fam. Med. 2018, 39, 147. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.C. 2019 Business Survey Statistical Table. 2021. Available online: https://www.jejusi.go.kr/information/statistics/years/2020.do (accessed on 1 January 2020).
- Jeju Special Self Governing Office. Population. Economic Growth. Industrial Structure. Available online: https://www.investkorea.org/jj-en/cntnts/i-1492/web.do (accessed on 1 May 2020).
- Zhao, X.; Zheng, H.; Shan, S.; Wang, K.; Zhang, M.; Xie, S.; Liu, C. Association between the non-HDL-cholesterol-to-HDL-cholesterol ratio and the risk of gallbladder polyp formation among men: A retrospective cohort study. Lipids Health Dis. 2020, 19, 146. [Google Scholar] [CrossRef] [PubMed]
- Silva, K.; Lopez, A.; Sánchez, V.; Villamil, H.; Leon, P.; Canizales, S.; Chávez, N.; Chabble, F.; Uribe, M.; Sánchez, N.M. The Variant I148M in PNPLA3 Is Associated With the Development of Gallbladder Cholesterol Polyps: 320. Off. J. Am. Coll. Gastroenterol. ACG 2014, 109, S97–S98. [Google Scholar] [CrossRef]
- Yu, L.; Liang, Q.; Zhou, W.; Huang, X.; Hu, L.; You, C.; Li, J.; Wu, Y.; Li, P.; Wu, Q. Association between physical activity and stroke in a middle-aged and elderly Chinese population. Medicine 2018, 97, e13568. [Google Scholar] [CrossRef]
- Yu, Z.; Yang, C.; Bai, X.; Yao, G.; Qian, X.; Gao, W.; Huang, Y.; Tian, X.; Cheng, S.; Zheng, Y. Risk factors for cholesterol polyp formation in the gallbladder are closely related to lipid metabolism. Lipids Health Dis. 2021, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Heitz, L.; Kratzer, W.; Grater, T.; Schmidberger, J. Gallbladder polyps—A follow-up study after 11 years. BMC Gastroenterol. 2019, 19, 42. [Google Scholar] [CrossRef]
- Yao, G.; Bai, X.; Yang, C.; Liu, L.; Zhou, Z.; Huang, Y.; Zheng, Y. Analysis of risk factors for gallbladder polyp formation—A retrospective study based on serial ultrasounds. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, M.; Yamagata, Z.; Takeda, Y.; Yoda, Y.; Kobayashi, K.; Fujino, M.A. The relationship between gallbladder disease and smoking and drinking habits in middle-aged Japanese. J. Gastroenterol. 2002, 37, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Schwesinger, W.H.; Kurtin, W.E.; Johnson, R. Alcohol protects against cholesterol gallstone formation. Ann. Surg. 1988, 207, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.W.; Koh, A.R.; Kim, C.H.; Bang, J.H.; Lee, J.H. Risk Factors of Gallbladder Polyp, and Association between Gallbladder Polyp and Dyslipidemia in Health Examines. Korean J. Fam. Pract. 2018, 8, 703–708. [Google Scholar] [CrossRef]
- LEE, M.-H.; Cho, P.-K.; Kwon, D.-M. Prevalence and risk factors of the gallbladder polyps diagnosed by ultrasound. J. Radiol. Sci. Technol. 2015, 38, 127–134. [Google Scholar] [CrossRef]
- Lin, S.H.; Wu, K.T.; Chiu, Y.C.; Wang, C.C.; Chiu, K.W. Risk factors for gallbladder polyps observed through second-look abdominal sonography in patients with fatty liver disease. Medicine 2022, 101, e29643. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M. One of 4 Is Migrant among Jeju People. Jeju Today. 2018. Available online: https://libguide.snu.ac.kr/c.php?g=321609&p=2151902 (accessed on 23 April 2018).
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; Volume 1, pp. 23–28. [Google Scholar]
- Kim, S.Y.; Kim, H.J. Trends in Alcohol Consumption for Korean Adults from 1998 to 2018: Korea National Health and Nutritional Examination Survey. Nutrients 2021, 13, 609. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Force IOT. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Available online: https://iris.who.int/bitstream/handle/10665/206936/0957708211_eng.pdf (accessed on 1 February 2020).
- Pickering, O.; Pucher, P.H.; Toale, C.; Hand, F.; Anand, E.; Cassidy, S.; McEntee, G.; Toh, S.K. Prevalence and sonographic detection of gallbladder polyps in a Western European population. J. Surg. Res. 2020, 250, 226–231. [Google Scholar] [CrossRef] [PubMed]
- McCain, R.S.; Diamond, A.; Jones, C.; Coleman, H.G. Current practices and future prospects for the management of gallbladder polyps: A topical review. World J. Gastroenterol. 2018, 24, 2844–2852. [Google Scholar] [CrossRef] [PubMed]
- Park, E.J.; Lee, H.S.; Lee, S.H.; Chun, H.J.; Kim, S.Y.; Choi, Y.K.; Ryu, H.J.; Shim, K.W. Association between metabolic syndrome and gallbladder polyps in healthy Korean adults. J. Korean Med. Sci. 2013, 28, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-L.; Kong, L.; Hou, L.-L.; Shen, H.-F.; Wang, Y.; Gu, X.-G.; Qin, J.-M.; Yin, P.-H.; Li, Q. Analysis of risk factors for polypoid lesions of gallbladder among health examinees. World J. Gastroenterol. WJG 2012, 18, 3015. [Google Scholar] [CrossRef] [PubMed]
- Yamin, Z.; Xuesong, B.; Guibin, Y.; Liwei, L.; Fei, L. Risk factors of gallbladder polyps formation in East Asian population: A meta-analysis and systematic review. Asian J. Surg. 2020, 43, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Kim, T.S.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I. Is it necessary to perform prophylactic cholecystectomy for asymptomatic subjects with gallbladder polyps and gallstones? J. Gastroenterol. Hepatol. 2010, 25, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.R.; Lin, D.Y.; Tai, D.I.; Hsieh, S.Y.; Lin, C.Y.; Sheen, I.S.; Chiu, C.T. Prevalence of and risk factors for gallbladder polyps detected by ultrasonography among healthy Chinese: Analysis of 34,669 cases. J. Gastroenterol. Hepatol. 2008, 23, 965–969. [Google Scholar] [CrossRef] [PubMed]
- Canturk, Z.; Senturk, O.; Canturk, N.Z.; Anik, Y.A. Prevalence and risk factors for gall bladder polyps. East. Afr. Med. J. 2007, 84, 336–341. [Google Scholar] [PubMed]
- Yamin, Z.; Xuesong, B.; Zhen, Z.; Yue, H.; Liwei, L.; Fei, L. Correlation of dyslipidemias and gallbladder polyps—A large retrospective study among Chinese population. Asian J. Surg. 2020, 43, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Jeju Special Self Governing Provincial Office of Education. Overall Status of Schools at Each Level. 2019. Available online: https://www.jje.go.kr/board/list.jje?boardId=BBS_0000093&menuCd=DOM_000000105005001000&contentsSid=1557&cpath= (accessed on 1 January 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Jeju City (n = 16,090) | Seogwipo City (n = 5644) | p-Value |
|---|---|---|---|
| GBPs (%) | 1577 (9.8) | 502 (8.9) | 0.043 |
| Men (%) | 8797 (54.6) | 3075 (54.5) | 0.804 |
| Metabolic syndrome | 2623 (16.3) | 909 (16.1) | 0.796 |
| Central obesity a | 6243 (38.8) | 2483 (44.0) | <0.001 |
| High blood pressure b | 6484 (40.3) | 2540 (45.0) | <0.001 |
| Age (years) | 54.5 ± 13.8 | 58.2 ± 14.1 | <0.001 |
| Body mass index (kg/m2) | 24.6 ± 3.2 | 24.9 ± 3.2 | <0.001 |
| Fasting blood glucose (mg/dL), (70–110) c | 100.1 ± 31.1 | 101.6 ± 32.4 | 0.003 |
| Total cholesterol (mg/dL), (<200) c | 195.3 ± 38.9 | 197.8 ± 39.2 | <0.001 |
| LDL cholesterol (mg/dL), (<100) c | 195.8 ± 38.7 | 198.1 ± 38.9 | <0.001 |
| HDL cholesterol (mg/dL), (>60) c | 53.6 ± 13.9 | 53.3 ± 13.9 | 0.191 |
| Triglycerides (mg/dL), (<150) c | 121.1 ± 94.1 | 121.9 ± 106.8 | 0.637 |
| AST (IU/L), (10–30) c | 28.8 ± 51.4 | 31.9 ± 102.1 | 0.003 |
| ALT (IU/L), (10–40) c | 30.8 ± 67.1 | 32.6 ± 106.6 | 0.150 |
| GGT (IU/L), (2–30) c | 50.9 ± 106.6 | 57.3 ± 130.3 | <0.001 |
| ALP (IU/L), (30–120) c | 215.5 ± 100.1 | 223.1 ± 115.2 | <0.001 |
| HBsAg | 965 (6.0) | 378 (6.7) | 0.088 |
| Physical activity | 5165 (32.1) | 1422 (25.2) | <0.001 |
| High-risk alcohol drinker d | 5149 (32.0) | 2003 (35.5) | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, O.-S.; Kim, Y.-K.; Kim, H.J. Retrospective Study of the Prevalence and Associated Factors of Gallbladder Polyps among Residents of Two Korean Cities. J. Clin. Med. 2024, 13, 2290. https://doi.org/10.3390/jcm13082290
Kwon O-S, Kim Y-K, Kim HJ. Retrospective Study of the Prevalence and Associated Factors of Gallbladder Polyps among Residents of Two Korean Cities. Journal of Clinical Medicine. 2024; 13(8):2290. https://doi.org/10.3390/jcm13082290
Chicago/Turabian StyleKwon, Oh-Sung, Young-Kyu Kim, and Hyeon Ju Kim. 2024. "Retrospective Study of the Prevalence and Associated Factors of Gallbladder Polyps among Residents of Two Korean Cities" Journal of Clinical Medicine 13, no. 8: 2290. https://doi.org/10.3390/jcm13082290
APA StyleKwon, O.-S., Kim, Y.-K., & Kim, H. J. (2024). Retrospective Study of the Prevalence and Associated Factors of Gallbladder Polyps among Residents of Two Korean Cities. Journal of Clinical Medicine, 13(8), 2290. https://doi.org/10.3390/jcm13082290