
Towards a Deeper Understanding: Utilizing Machine Learning to Investigate the Association between Obesity and Cognitive Decline—A Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
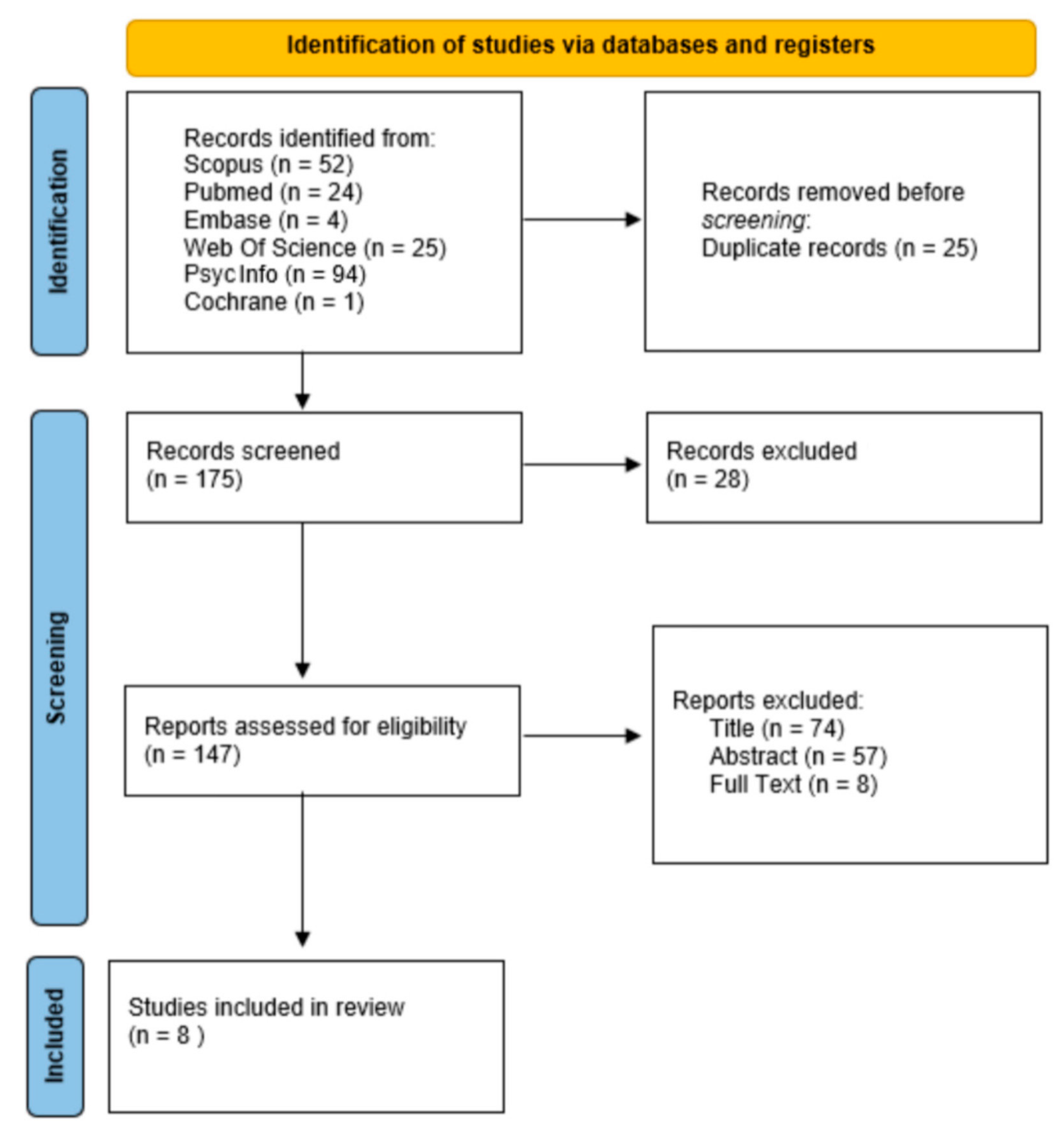
2.1. Search Strategy
2.2. PICO Model
2.3. Study Selection
2.4. Data Extraction and Analysis
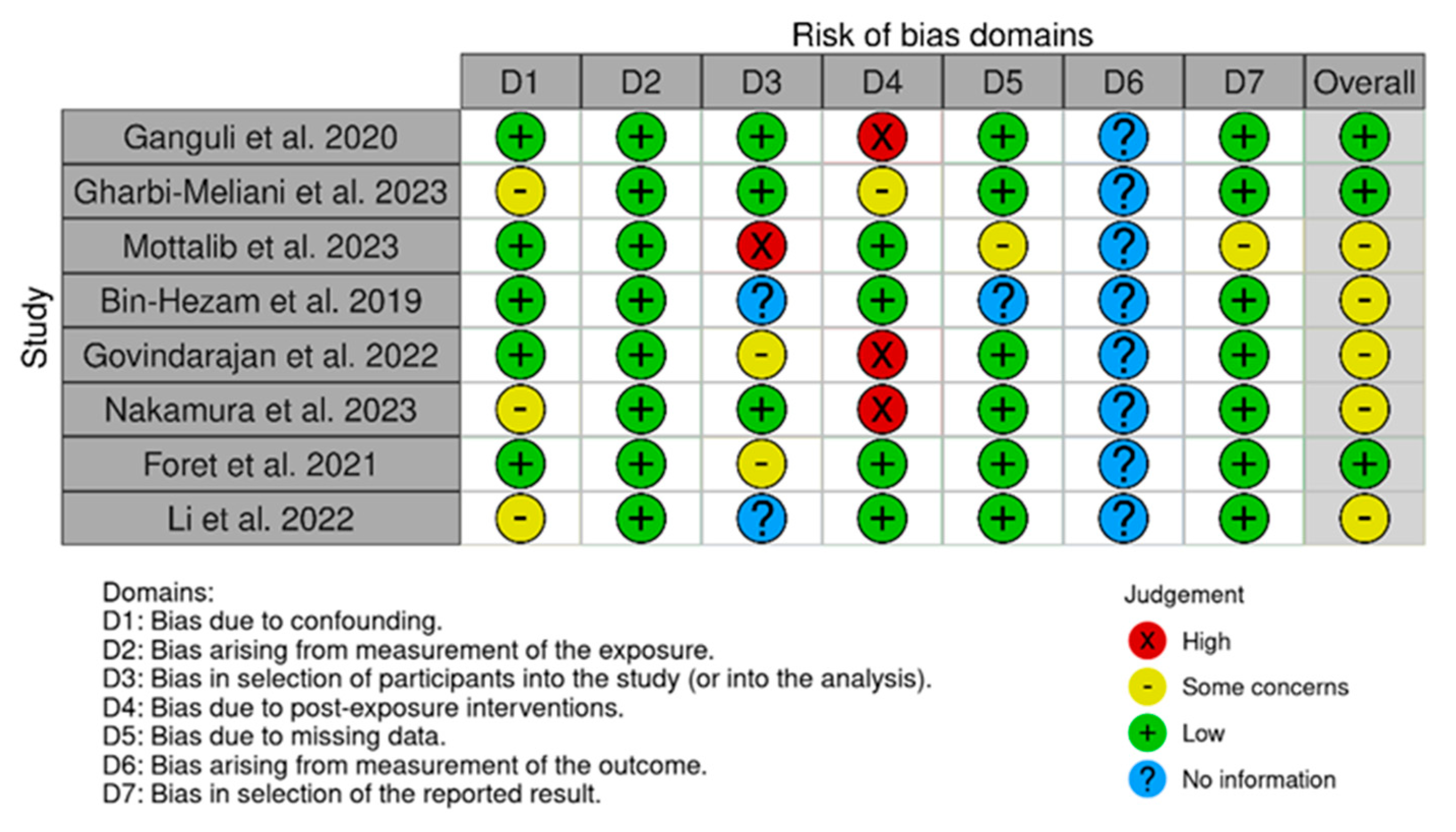
2.5. Risk of Bias within Individual Studies
3. Results
3.1. Synthesis of Evidence
3.2. Key Findings from Included Studies

| Study | Design | Sample Size | AI/ML Technique | Cognitive Decline and Assessment | Objective | Results |
|---|---|---|---|---|---|---|
| Bin-Hezam and Ward (2019) [52] | Secondary observational | 1812 subjects (aged 55–90) from ADNI. | LR, NB, DT, and RF | This study analyzes existing diagnoses and dementia risk factors within the ADNI dataset (e.g., depression, cognitive inactivity). | Detect dementia based on modifiable risk factors leveraging ML techniques. | ML models achieved high accuracy (up to 92%) in predicting dementia risk. BMI, cognitive, and physical activity were identified as important factors. |
| Ganguli et al., 2020 [44] | Prospective cohort | 478 individuals aged 65 and older from MYHAT | WHR-stratified ML analyses using CART | Neuropsychological tests for memory, attention, and other cognitive functions were administered at baseline and follow-up to assess global cognitive decline. | Investigate potential underlying mechanisms between diabetes, obesity, and cognitive decline in older adults. | Hyperglycemia in younger individuals with central obesity may lead to faster cognitive decline, while adiponectin could be a risk factor for cognitive decline in younger individuals without central obesity. |
| Foret et al. (2021) [55] | Observational | 266 individuals (121 males and 145 females; mean age ± SD: 49 ± 6 years for both) | Gaussian process | Standardized memory, fluency, and executive function tests were administered (e.g., MMSE, CVLT-II, WAIS-IV) to assess late-life cognitive decline. | Investigate the relationships between brain health and cardiovascular risk factors in midlife adults, with a specific focus on sex differences. | Men might be more vulnerable to the direct effects of metabolism on brain health, while women might experience more complex interactions involving brain health, metabolism, and potentially genetics. |
| Govindarajan et al. (2022) [53] | Cross-sectional observational study | N = 24,902 from 8 independent studies, 54.5% female, average age = 62.4, age range 45–75 years. | Linear support vector classifiers | This study analyzes existing data (diagnoses and MRI scans) from cognitively normal iSTAGING participants to develop CVM-related brain structure measures (SPARE-CVMs) relevant to dementia, AD, and brain aging. | Develop and evaluate ML-based indices that can capture the individual-level effects of CVMs on brain structure in cognitively unimpaired individuals. | ML successfully revealed distinct brain changes associated with specific CVMs like diabetes and hypertension in cognitively normal individuals. These indexes captured distinct patterns and were not linked to typical aging or AD markers, highlighting their potential for understanding CVM-brain health relationships. |
| Li et al. (2022) [56] | Observational | Data of AD and MetS in the GEO database | RF and LASSO | The study focuses on gene expression data from existing studies of AD and MetS. | Explore the connection between AD and MetS by identifying genes that could potentially diagnose both conditions. | The study found 8 genes potentially useful for diagnosing both AD and MetS. |
| Gharbi-Meliani et al. (2023) [45] | Longitudinal observational | Data of 15,278 baseline participants (aged 50 years and more) from SHARE | MFA and HCPC | Autonomy was assessed via ADL/IADL scales; cognition was assessed via immediate recall and VF for “Likely Dementia” status. | Explore the potential of unsupervised ML in identifying transition to probable dementia in longitudinal population aging surveys. | “Likely Dementia” is more common in older people, with a higher prevalence in females than males. Nine risk factors including hypertension, physical inactivity, diabetes, and obesity, increase the likelihood of transitioning to dementia. |
| Mottalib et al. (2023) [51] | Observational cohort study | Data from 1,531,374 patients (aged 20–70) collected from 1 January 2013 to 31 December 2018 | Unsupervised clustering | Focused on individuals having a diagnosis of one of the 18 major chronic diseases examined, including AD or dementia. | Classify the likelihood of 18 common chronic illnesses in individuals based solely on their obesity patterns, as indicated by the trajectory of their BMI. | The development of diabetes, hypertension, and dementia is directly related to the trajectory of BMI. |
| Nakamura et al. (2023) [54] | Observational cohort study | Data from 3238 individuals (1281 males, age 50.2 ± 16.2 years; 1957 females, age 51.5 ± 16.0 years) collected over 14 years (2005–2018). | Future-onset prediction models and p-mICE | 11 NCDs were considered, including incident dementia that was defined by the MMSE ≤ 23. | Investigate the potential of HDPDs for early detection and prevention of NCDs. | HDPDs revealed individual variations in health markers, suggesting personalized prevention strategies. Improving health beyond personal boundaries in HDPDs potentially prevented future disease onset in 7/11 diseases. |
3.3. Risk of Bias
4. Discussion
4.1. Future Directions
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Istituto Superiore di Sanità. Rapporto ISS 2020—Il Peso Degli Italiani. Available online: https://www.iss.it/ (accessed on 15 February 2024).
- World Health Organization. Obesity and Overweight. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 15 February 2022).
- Okunogbe, A.; Nugent, R.; Spencer, G.; Powis, J.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for 161 countries. BMJ Glob. Health 2022, 7, e009773. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Health Consequences of Being Overweight [Question and Answer] (6 October 2020). Available online: https://www.who.int/news-room/questions-and-answers/item/obesity-health-consequences-of-being-overweight (accessed on 15 February 2024).
- Collaborators, G.B.D.; Ärnlöv, J. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar]
- Puhl, R.M.; Heuer, C.A. Obesity Stigma: Important considerations for public health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Seidell, J.C.; Halberstadt, J. The global burden of obesity and the challenges of prevention. Ann. Nutr. Metab. 2015, 66 (Suppl. 2), 7–12. [Google Scholar] [CrossRef] [PubMed]
- Kumanyika, S.K. A Framework for Increasing Equity Impact in Obesity Prevention. Am. J. Public Health 2019, 109, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.C.; Killcross, A.S.; Jenkins, T.A. Obesity and cognitive decline: Role of inflammation and vascular changes. Front. Neurosci. 2018, 8, 121665. [Google Scholar] [CrossRef] [PubMed]
- Farooqui, T.; Farooqui, A.A. Aging: An important factor for the pathogenesis of neurodegenerative diseases. Mech. Ageing Dev. 2009, 130, 203–215. [Google Scholar] [CrossRef]
- Knopman, D.S.; Boeve, B.F.; Petersen, R.C. Essentials of the proper diagnoses of mild cognitive impairment, dementia, and major subtypes of dementia. Mayo Clin. Proc. 2003, 78, 1290–1308. [Google Scholar] [CrossRef]
- World Health Organization. Dementia 2023. Available online: https://apps.who.int/gho/data/node.dementia (accessed on 15 February 2024).
- Gustavsson, A.; Norton, N.; Fast, T.; Frölich, L.; Georges, J.; Holzapfel, D.; Kirabali, T.; Krolak-Salmon, P.; Rossini, P.M.; Ferretti, M.T.; et al. Global estimates on the number of persons across the Alzheimer’s disease continuum. Alzheimer’s Dement. 2023, 19, 658–670. [Google Scholar] [CrossRef]
- Barr, C.; Riolacci-Dhoyen, N.; Galbraith, M.; Leperre-Desplanques, A. Sharing knowledge to advance healthcare policies in Europe for people living with dementia and their carers: The ALCOVE project. Arch. Public Health 2012, 70, 21. [Google Scholar] [CrossRef]
- Anstey, K.J.; Cherbuin, N.; Budge, M.; Young, J. Body Mass Index in midlife and late life as a risk for dementia: A meta-analysis of prospective studies. Obes. Rev. 2011, 12, e426–e437. [Google Scholar] [CrossRef]
- Whitmer, R.A.; Gustafson, D.R.; Barrett-Connor, E.; Haan, M.N.; Gunderson, E.P.; Yaffe, K. Central obesity and increased risk of dementia more than three decades later. Neurology 2008, 71, 1057–1064. [Google Scholar] [CrossRef]
- Pedditizi, E.; Peters, R.; Beckett, N. The risk of overweight/obesity in mid-life and late life for the development of dementia: A systematic review and meta-analysis of longitudinal studies. Age Ageing 2016, 45, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Ajnakina, O.; Steptoe, A.; Cadar, D. Higher risk of dementia in English older individuals who are overweight or obese. Int. J. Epidemiol. 2020, 49, 1353–1365. [Google Scholar] [CrossRef]
- Mrak, R.E. Alzheimer-type neuropathological changes in morbidly obese elderly individuals. Clin. Neuropathol. 2009, 28, 40–45. [Google Scholar] [CrossRef]
- Gustafson, D.; Lissner, L.; Bengtsson, C.; Björkelund, C.; Skoog, I. A 24-year follow-up of body mass index and cerebral atrophy. Neurology 2004, 63, 1876–1881. [Google Scholar] [CrossRef]
- Hassing, L.B.; Dahl, A.K.; Pedersen, N.L.; Johansson, B. Overweight in midlife is related to lower cognitive function 30 years later: A prospective study with longitudinal assessments. Dement. Geriatr. Cogn. Disord. 2010, 29, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Devere, R. The cognitive consequences of obesity. Pract. Neurol. 2018, 18, 142–145. [Google Scholar]
- Raji, C.A.; Ho, A.J.; Parikshak, N.N.; Becker, J.T.; Lopez, O.L.; Kuller, L.H.; Hua, X.; Leow, A.D.; Toga, A.W.; Thompson, P.M. Brain structure and obesity. Hum. Brain Mapp. 2010, 31, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Amen, D.G.; Wu, J.; George, N.; Newberg, A. Patterns of Regional Cerebral Blood Flow as a Function of Obesity in Adults. J. Alzheimer’s Dis. 2020, 77, 1331–1337. [Google Scholar] [CrossRef]
- Stanek, K.M.; Strain, G.; Devlin, M.; Cohen, R.; Paul, R.; Crosby, R.D.; Mitchell, J.E.; Gunstad, J. Body mass index and neurocognitive functioning across the adult lifespan. Neuropsychology 2013, 27, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.S.; Friedrich, M.G.; Lee, D.S.; Awadalla, P.; Després, J.P.; Desai, D.; de Souza, R.J.; Dummer, T.; Parraga, G.; Larose, E.; et al. Evaluation of Adiposity and Cognitive Function in Adults. JAMA Netw. Open 2022, 5, e2146324. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Hansen, B.; Smith, S.C.; Cleeman, J.I.; Kahn, R.A.; American Heart, A.; National Heart, L.; Blood, I.; American Diabetes, A. Clinical management of metabolic syndrome: Report of the American Heart Association/National Heart, Lung, and Blood Institute/American Diabetes Association conference on scientific issues related to management. Arterioscler. Thromb. Vasc. Biol. 2004, 24, e19–e24. [Google Scholar] [CrossRef] [PubMed]
- Johri, A.; Roncati, L.; Lizcano, F. Editorial: Endocrine disruptors and diseases of brain and mind: Past and prelude. Front. Endocrinol. 2024, 15, 1362519. [Google Scholar] [CrossRef] [PubMed]
- Ezkurdia, A.; Ramírez, M.J.; Solas, M. Metabolic Syndrome as a Risk Factor for Alzheimer’s Disease: A Focus on Insulin Resistance. Int. J. Mol. Sci. 2023, 24, 4354. [Google Scholar] [CrossRef] [PubMed]
- Takechi, R.; Sharif, A.; Brook, E.; Majimbi, M.; Chan, D.C.; Lam, V.; Watts, G.F.; Mamo, J.C.L. Is type 2 diabetes associated dementia a microvascular early-Alzheimer’s phenotype induced by aberrations in the peripheral metabolism of lipoprotein-amyloid? Front. Endocrinol. 2023, 14, 1127481. [Google Scholar] [CrossRef]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Russell, S.J.; Norvig, P. Artificial Intelligence: A Modern Approach; Pearson: London, UK, 2016. [Google Scholar]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Futur. Health J. 2019, 6, 94–98. [Google Scholar] [CrossRef]
- Sarker, I.H.; Furhad, M.H.; Nowrozy, R. AI-driven cybersecurity: An overview, security intelligence modeling and research directions. SN Comput. Sci. 2021, 2, 173. [Google Scholar] [CrossRef]
- Alowais, S.A.; Alghamdi, S.S.; Alsuhebany, N.; Alqahtani, T.; Alshaya, A.I.; Almohareb, S.N.; Aldairem, A.; Alrashed, M.; Bin Saleh, K.; Badreldin, H.A.; et al. Revolutionizing healthcare: The role of artificial intelligence in clinical practice. BMC Med. Educ. 2023, 23, 689. [Google Scholar] [CrossRef]
- Veneziani, I.; Marra, A.; Formica, C.; Grimaldi, A.; Marino, S.; Quartarone, A.; Maresca, G. Applications of Artificial Intelligence in the Neuropsychological Assessment of Dementia: A Systematic Review. J. Pers. Med. 2024, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Myszczynska, M.A.; Ojamies, P.N.; Lacoste, A.M.B.; Neil, D.; Saffari, A.; Mead, R.; Hautbergue, G.M.; Holbrook, J.D.; Ferraiuolo, L. Applications of machine learning to diagnosis and treatment of neurodegenerative diseases. Nat. Rev. Neurol. 2020, 16, 440–456. [Google Scholar] [CrossRef] [PubMed]
- Formica, C.; Bonanno, L.; Giambò, F.M.; Maresca, G.; Latella, D.; Marra, A.; Cucinotta, F.; Bonanno, C.; Lombardo, M.; Tomarchio, O.; et al. Paving the Way for Predicting the Progression of Cognitive Decline: The Potential Role of Machine Learning Algorithms in the Clinical Management of Neurodegenerative Disorders. J. Pers. Med. 2023, 13, 1386. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Olds, T.; Brinsley, J.; Dumuid, D.; Virgara, R.; Matricciani, L.; Watson, A.; Szeto, K.; Eglitis, E.; Miatke, A.; et al. Systematic review and meta-analysis of the effectiveness of chatbots on lifestyle behaviours. NPJ Digit. Med. 2023, 6, 118. [Google Scholar] [CrossRef] [PubMed]
- Easton, K.; Potter, S.; Bec, R.; Bennion, M.; Christensen, H.; Grindell, C.; Mirheidari, B.; Weich, S.; De Witte, L.; Wolstenholme, D.; et al. A Virtual Agent to Support Individuals Living With Physical and Mental Comorbidities: Co-Design and Acceptability Testing. J. Med. Internet Res. 2019, 21, e12996. [Google Scholar] [CrossRef] [PubMed]
- Brown, D. A Review of the PubMed PICO Tool: Using Evidence-Based Practice in Health Education. Health Promot. Pract. 2020, 21, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Morgan, R.; Rooney, A.; Taylor, K.; Thayer, K.; Silva, R.; Lemeris, C.; Akl, A.; Arroyave, W.; ROBINS-E Development Group; et al. Risk of Bias in Non-randomized Studies—of Exposure (ROBINS-E). Launch Version. 20 June 2023. Available online: https://www.riskofbias.info/welcome/robins-e-tool (accessed on 25 February 2024).
- Rao, R.V.; Subramaniam, K.G.; Gregory, J.; Bredesen, A.L.; Coward, C.; Okada, S.; Kelly, L.; Bredesen, D.E. Rationale for a Multi-Factorial Approach for the Reversal of Cognitive Decline in Alzheimer’s Disease and MCI: A Review. Int. J. Mol. Sci. 2023, 24, 1659. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, M.; Beer, J.C.; Zmuda, J.M.; Ryan, C.M.; Sullivan, K.J.; Chang, C.H.; Rao, R.H. Aging, Diabetes, Obesity, and Cognitive Decline: A Population-Based Study. J. Am. Geriatr. Soc. 2020, 68, 991–998. [Google Scholar] [CrossRef]
- Gharbi-Meliani, A.; Husson, F.; Vandendriessche, H.; Bayen, E.; Yaffe, K.; Bachoud-Lévi, A.-C.; de Langavant, L.C. Identification of High Likelihood of Dementia in Population-Based Surveys Using Unsupervised Clustering: A Longitudinal Analysis. Alzheimer’s Res. Ther. 2023, 15, 209. [Google Scholar] [CrossRef]
- Burke, S.L.; Hu, T.; Fava, N.M.; Li, T.; Rodriguez, M.J.; Schuldiner, K.L.; Burgess, A.; Laird, A. Sex differences in the development of mild cognitive impairment and probable Alzheimer’s disease as predicted by hippocampal volume or white matter hyperintensities. J. Women Aging 2019, 31, 140–164. [Google Scholar] [CrossRef]
- Toro, C.A.; Zhang, L.; Cao, J.; Cai, D. Sex differences in Alzheimer’s disease: Understanding the molecular impact. Brain Res. 2019, 1719, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Plassman, B.; Langa, K.; Fisher, G.; Heeringa, S.; Weir, D.; Ofstedal, M.; Burke, J.; Hurd, M.D.; Potter, G.; Rodgers, W.; et al. Prevalence of Dementia in the United States: The Aging, Demographics, and Memory Study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Miech, R.A.; Breitner, J.C.; Zandi, P.P.; Khachaturian, A.S.; Anthony, J.C.; Mayer, L. Incidence of AD may decline in the early 90s for men, later for women—The Cache County study. Neurology 2002, 58, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Zandi, P.P.; Carlson, M.C.; Plassman, B.L.; Welsh-Bohmer, K.A.; Mayer, L.S.; Steffens, D.C.; Breitner, J.C.S. Cache County Memory Study Investigators. Hormone replacement therapy and incidence of Alzheimer disease in older women—The Cache County Study. JAMA-J. Am. Med. Assoc. 2002, 288, 2123–2129. [Google Scholar] [CrossRef]
- Mottalib, M.; Jones-Smith, J.C.; Sheridan, B.; Beheshti, R. Subtyping patients with chronic disease using longitudinal BMI patterns. IEEE J. Biomed. Health Inform. 2023, 27, 2083–2093. [Google Scholar] [CrossRef] [PubMed]
- Bin-Hezam, R.; Ward, T.E. A Machine Learning Approach towards Detecting Dementia based on its Modifiable Risk Factors. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 8. [Google Scholar] [CrossRef]
- Govindarajan, S.T.; Mamourian, E.; Erus, G.; Abdulkadir, A.; Melhem, R.; Doshi, J.; Pomponio, R.; Tosun, D.; An, Y.; Sotiras, A.; et al. Machine-learning based MRI neuro-anatomical signatures associated with cardiovascular and metabolic risk factors. Alzheimer’s Dement. 2022, 18, e067709. [Google Scholar] [CrossRef]
- Nakamura, K.; Uchino, E.; Sato, N.; Araki, A.; Terayama, K.; Kojima, R.; Murashita, K.; Itoh, K.; Mikami, T.; Tamada, Y.; et al. Individual health-disease phase diagrams for disease prevention based on machine learning. J. Biomed. Inform. 2023, 144, 104448. [Google Scholar] [CrossRef] [PubMed]
- Foret, J.T.; Dekhtyar, M.; Cole, J.H.; Gourley, D.D.; Caillaud, M.; Tanaka, H.; Haley, A.P. Network Modeling Sex Differences in Brain Integrity and Metabolic Health. Front. Aging Neurosci. 2021, 13, 691691. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Y.; Lu, T.; Liang, R.; Wu, Z.; Liu, M.; Qin, L.; Chen, H.; Yan, X.; Deng, S.; et al. Identification of diagnostic genes for both Alzheimer’s disease and Metabolic syndrome by the machine learning algorithm. Front. Immunol. 2022, 13, 1037318. [Google Scholar] [CrossRef]
- Pigeyre, M.; Yazdi, F.T.; Kaur, Y.; Meyre, D. Recent progress in genetics, epigenetics and metagenomics unveils the pathophysiology of human obesity. Clin. Sci. 2016, 130, 943–986. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, J.A.; Tang, M.-X.; Stern, Y.; Shea, S.; Mayeux, R. Diabetes mellitus and risk of Alzheimer’s disease and dementia with stroke in a multiethnic cohort. Am. J. Epidemiol. 2001, 154, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Blackwell, T.; Kanaya, A.M.; Davidowitz, N.; Barrett-Connor, E.; Krueger, K. Diabetes, impaired fasting glucose, and development of cognitive impairment in older women. Neurology 2004, 63, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, H.; Barger, S.; Barnum, S.; Bradt, B.; Bauer, J.; Cole, G.M.; Cooper, N.R.; Eikelenboom, P.; Emmerling, M.; Fiebich, B.L.; et al. Inflammation and Alzheimer’s disease. Neurobiol. Aging 2000, 21, 383–421. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.-H.; Yamamoto, M.; Hernandez, C.M.; Khodadadi, H.; Baban, B.; Stranahan, A.M. Visceral adipose NLRP3 impairs cognition in obesity via IL-1R1 on CX3CR1+ cells. J. Clin. Investig. 2020, 130, 1961–1976. [Google Scholar] [CrossRef]
- Quaye, E.; Galecki, A.T.; Tilton, N.; Whitney, R.; Briceño, E.M.; Elkind, M.S.; Fitzpatrick, A.L.; Gottesman, R.F.; Griswold, M.; Gross, A.L.; et al. Association of Obesity With Cognitive Decline in Black and White Americans. Neurology 2023, 100, e220–e231. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.A.; Spencer, S.J. Obesity and neuroinflammation: A pathway to cognitive impairment. Brain Behav. Immun. 2014, 42, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-W.; Zong, Y.; Cao, X.-P.; Tan, L.; Tan, L. Microglial priming in Alzheimer’s disease. Ann. Transl. Med. 2018, 6, 176. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Mareljic, N.; Michaelsen, M.; Parhizkar, S.; Heindl, S.; Nuscher, B.; Farny, D.; Czuppa, M.; Schludi, C.; Graf, A.; et al. Active poly-GA vaccination prevents microglia activation and motor deficits in a C9orf72 mouse model. EMBO Mol. Med. 2019, 12, e10919. [Google Scholar] [CrossRef]
- Caunca, M.R.; Gardener, H.; Simonetto, M. Measures of obesity are associated with MRI markers of brain aging: The Northern Manhattan Study. Neurology 2019, 93, e791–e803. [Google Scholar] [CrossRef]
- Chaldakov, G.N.; Stankulov, I.S.; Hristova, M.; Ghenev, P.I. Adipobiology of disease: Adipokines and adipokine-targeted pharmacology. Curr. Pharm. Des. 2003, 9, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Landin, K.; Stigendal, L.; Eriksson, E.; Krotkiewski, M.; Risberg, B.; Tengborn, L.; Smith, U. Abdominal obesity is associated with an impaired fibrinolytic activity and elevated plasminogen activator inhibitor-1. Metabolism 1990, 39, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Funahashi, H.; Yada, T.; Suzuki, R.; Shioda, S. Distribution, function, and properties of leptin receptors in the brain. Int. Rev. Cytol. 2003, 224, 1–27. [Google Scholar]
- Harvey, J. Novel actions of leptin in the hippocampus. Ann. Med. 2003, 35, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Fewlass, D.C.; Noboa, K.; Pi-Sunyer, F.X.; Johnston, J.M.; Yan, S.D.; Tezapsidis, N. Obesity-related leptin regulates Alzheimer’s Abeta. FASEB J. 2004, 18, 1870–1878. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.A.; Carlsson, C.M.; Trivedi, M.A.; Sager, M.A.; Johnson, S.C. The effect of body mass index on global brain volume in middle-aged adults: A cross sectional study. BMC Neurol. 2005, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Jagust, W.; Harvey, D.; Mungas, D.; Haan, M. Central Obesity and the Aging Brain. Arch. Neurol. 2005, 62, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-Y.; Kim, K.; Hong, C.H.; Lee, S.Y.; Jung, Y.-S. Sex differences in cardiovascular risk factors for dementia. Biomol. Ther. 2018, 26, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.S.; Oskotsky, T.; Havaldar, S.; Mantyh, W.G.; Bicak, M.; Solsberg, C.W.; Woldemariam, S.; Zeng, B.; Hu, Z.; Oskotsky, B.; et al. Deep phenotyping of Alzheimer’s disease leveraging electronic medical records identifies sex-specific clinical associations. Nat. Commun. 2022, 13, 675. [Google Scholar] [CrossRef]
- Fillit, H.; Nash, D.T.; Rundek, T.; Zuckerman, A. Cardiovascular risk factors and dementia. Am. J. Geriatr. Pharmacother. 2008, 6, 100–118. [Google Scholar] [CrossRef]
- Villablanca, A.; Dugger, B.N.; Nuthikattu, S.; Chauhan, J.; Cheung, S.; Chuah, C.-N.; Garrison, S.L.; Milenkovic, D.; Norman, J.E.; Oliveira, L.C.; et al. How cy pres Promotes Transdisciplinary Convergence Science: An Academic Health Center for Women’s Cardiovascular and Brain Health. J. Clin. Transl. Sci. 2024, 8, e16. [Google Scholar] [CrossRef] [PubMed]
- Rich-Edwards, J.W.; Kaiser, U.B.; Chen, G.L.; Manson, J.E.; Goldstein, J.M. Sex and Gender Differences Research Design for Basic, Clinical, and Population Studies: Essentials for Investigators. Endocr. Rev. 2018, 39, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Eun, S.-J.; Kim, E.J.; Kim, J. Artificial intelligence-based personalized serious game for enhancing the physical and cognitive abilities of the elderly. Futur. Gener. Comput. Syst. 2023, 141, 713–722. [Google Scholar] [CrossRef]
- Alotaibi, M.; Alnajjar, F.; Cappuccio, M.; Khalid, S.; Alhmiedat, T.; Mubin, O. Efficacy of Emerging Technologies to Manage Childhood Obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 1227–1244. [Google Scholar] [CrossRef]
- Bays, H.E.; Fitch, A.; Cuda, S.; Gonsahn-Bollie, S.; Rickey, E.; Hablutzel, J.; Censani, M. Artificial intelligence and obesity management: An obesity medicine association (OMA) clinical practice statement (CPS). Obes. Pillars 2003, 6, 100065. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veneziani, I.; Grimaldi, A.; Marra, A.; Morini, E.; Culicetto, L.; Marino, S.; Quartarone, A.; Maresca, G. Towards a Deeper Understanding: Utilizing Machine Learning to Investigate the Association between Obesity and Cognitive Decline—A Systematic Review. J. Clin. Med. 2024, 13, 2307. https://doi.org/10.3390/jcm13082307
Veneziani I, Grimaldi A, Marra A, Morini E, Culicetto L, Marino S, Quartarone A, Maresca G. Towards a Deeper Understanding: Utilizing Machine Learning to Investigate the Association between Obesity and Cognitive Decline—A Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2307. https://doi.org/10.3390/jcm13082307
Chicago/Turabian StyleVeneziani, Isabella, Alessandro Grimaldi, Angela Marra, Elisabetta Morini, Laura Culicetto, Silvia Marino, Angelo Quartarone, and Giuseppa Maresca. 2024. "Towards a Deeper Understanding: Utilizing Machine Learning to Investigate the Association between Obesity and Cognitive Decline—A Systematic Review" Journal of Clinical Medicine 13, no. 8: 2307. https://doi.org/10.3390/jcm13082307
APA StyleVeneziani, I., Grimaldi, A., Marra, A., Morini, E., Culicetto, L., Marino, S., Quartarone, A., & Maresca, G. (2024). Towards a Deeper Understanding: Utilizing Machine Learning to Investigate the Association between Obesity and Cognitive Decline—A Systematic Review. Journal of Clinical Medicine, 13(8), 2307. https://doi.org/10.3390/jcm13082307