1. Introduction
The catheter ablation of ventricular arrhythmias is increasingly considered a treatment option for patients with and without structural heart disease. Symptoms, risk of sudden cardiac death (SCD) and recurrence of ventricular arrhythmias determine the treatment choice. The importance of catheter ablation for the treatment of ventricular tachycardia (VT) and premature ventricular complexes (PVC) increased significantly over the last decades [
1,
2,
3]. Often, catheter ablation is performed as a sole therapy in patients with an idiopathic VT or with idiopathic PVCs [
4]. This is different for patients with an underlying structural heart disease, where the implantation of an implantable cardioverter defibrillator (ICD) is the mainstay for SCD prevention [
5]. These are life-saving devices; however, they are associated with significant morbidity, including posttraumatic stress disorder [
6] or depression [
7], due to ICD shocks. Antiarrhythmic drugs are then usually prescribed to reduce the recurrence of VTs and consecutive ICD therapies. However, the efficacy of these drugs is limited, and moreover, significant side effects as well as proarrhythmias may occur [
8].
Catheter ablation can be an effective and safe alternative or adjunct to pharmacological therapy to reduce the recurrence of VT in these patients when performed in experienced centers. It is the only treatment option that can change the arrhythmogenic substrate. In recent years, significant progress has been made in identifying and ablating the right targets due to improved techniques and increased experience.
The purpose of this retrospective analysis of consecutive ablation procedures for VTs and PVCs was to report on acute success rates and procedural complication rates in an experienced tertiary care center in Switzerland.
2. Methods
All patients who underwent ablation therapy for VT or PVC at the University Heart Center in Zurich, Switzerland, between March 2012 and April 2017 were included in this study.
Prior to ablation in the left ventricle, transthoracic echocardiography (TTE) was performed in all patients to exclude intracardiac thrombi. If feasible, cardiac computed tomography (CT) or cardiac magnetic resonance imaging (MRI) scans were also performed. The data were then merged into the electroanatomic mapping system (CARTO, Biosense Webster, Diamond Bar, CA, USA).
Acute complete success of VT ablation was defined as abolition of all sustained VTs. Acute partial success was defined by abolition of the clinical VT. At the end of the procedure, the initial induction protocol was repeated to demonstrate non-inducibility of the VT in all patients when the clinical VT was hemodynamically stable. The non-inducibility protocol included 3 extrastimuli and was performed at two different sites of the right ventricle, RV apex and RV outflow tract. In those patients with hemodynamically unstable VT who underwent substrate mapping and substrate-based ablation, success was defined as abolition of all local late potentials and fragmented electrograms in the scar area.
In PVC ablation, complete abolition of the clinical PVC was labeled an acute success. Ability to induce single PVCs at the end of the procedure but to a significantly reduced degree or with a different morphology not resembling the spontaneous clinical PVC was labeled a partial success.
2.1. Catheter Ablation
Anterograde and/or retrograde access routes were chosen at the operator’s discretion, often according to cardiac anatomy and the targeted arrhythmia. Decision for epicardial access could be made by the responsible operator when the substrate was deemed to be epicardial based on etiology of the VT (non-ischemic cardiomyopathies) or in patients after failed endocardial ablations.
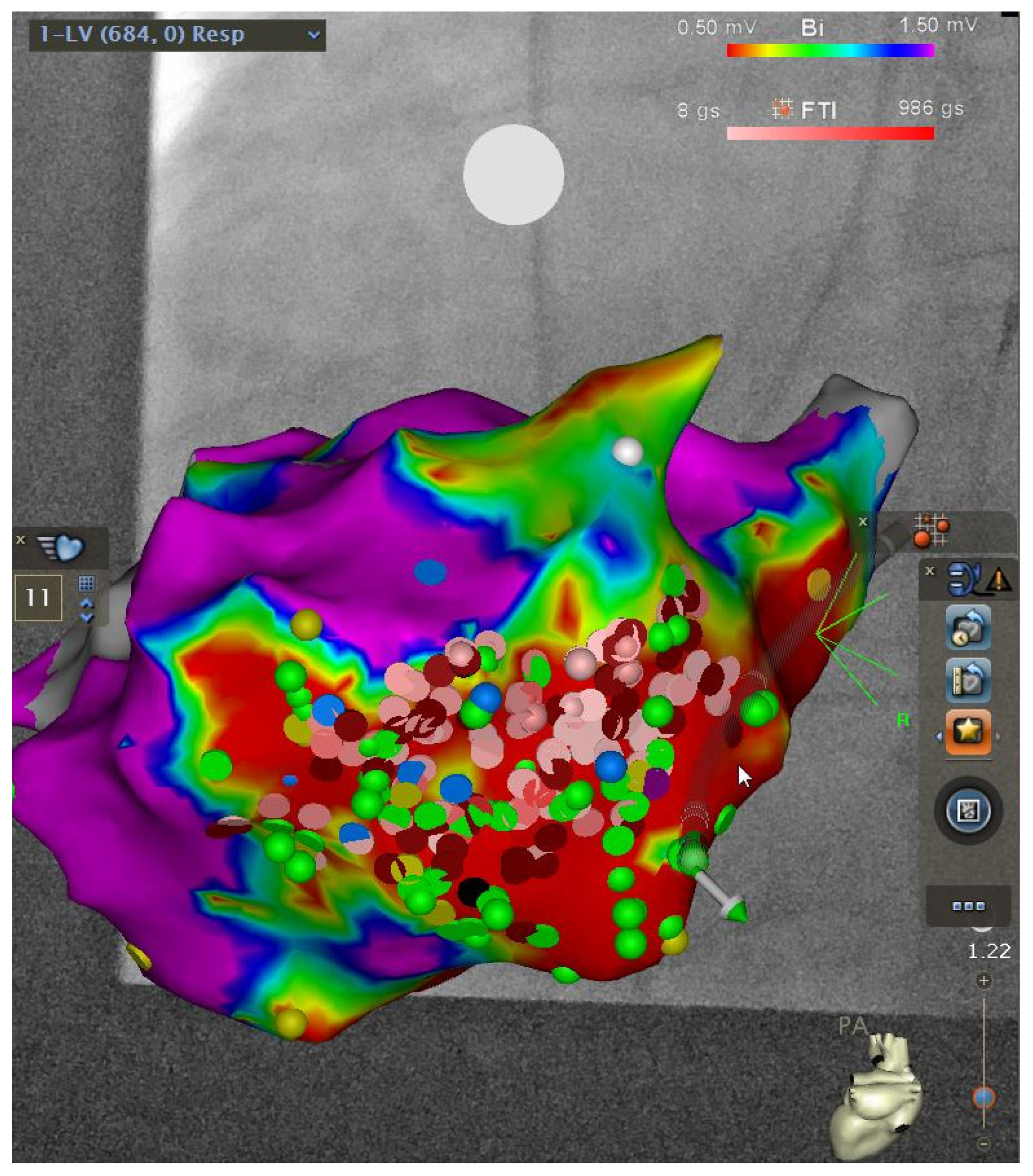
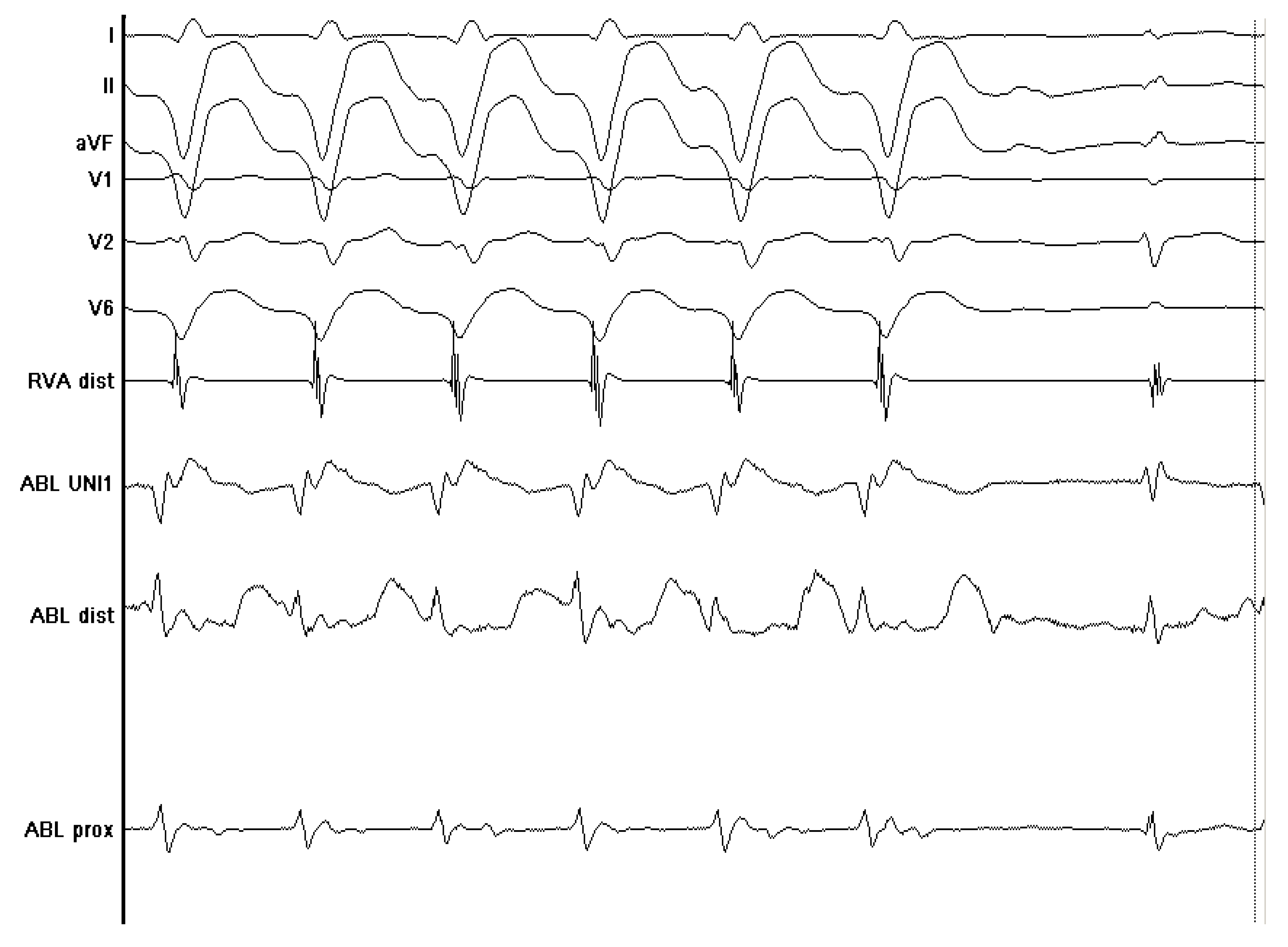
Various techniques were used prior to ablation in all patients to map the ventricle for localization of specific targets. In activation mapping, endocardial electrograms were sampled by a mapping catheter and then compared with the timing of the QRS complex on the surface electrocardiogram (ECG). A site that was activated 20 to 40 ms before the onset of the surface QRS complex was considered close to the origin of the VT/PVC. In pace mapping, different sites of the ventricle were stimulated until a QRS pattern was induced that matched the QRS pattern of the spontaneous VT. Pace mapping was used when the relevant VT could not be induced, and a surface ECG of the spontaneous VT was obtained prior to ablation. Entrainment mapping was also used in patients with scar-based VT and involved pacing during a VT at a slightly faster rate than the VT rate. An isolated mid-diastolic potential with a low amplitude from within the critical isthmus of the VT, where entrainment with concealed fusion could be demonstrated, was considered a good site for ablation. Some patients, especially those with structural heart disease, would not have tolerated activation mapping and entrainment due to hemodynamic instability. Inability to induce sustained VT during a procedure was another situation where different techniques came into consideration, categorized as substrate mapping. In substrate mapping, areas of low electrical voltage or delayed potentials were recorded during sinus rhythm (examples shown in
Figure 1 and
Figure 2).
2.2. Statistical Analysis
Continuous variables were summarized as mean (SD), and categorical values were summarized as n/total or % of total. Descriptive analyses were performed with Microsoft Excel. To detect differences between groups for acute success and acute complication rates, Fisher’s exact test was performed with GraphPad Prism version 10. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics
The demographic and clinical baseline characteristics are summarized in
Table 1. Patients were predominantly male (84 out of 120 patients; 70%), and the mean age was 55 ± 15 years. Out of 120 patients who were included, 69 (57.5%) were ablated for VT and 51 (42.5%) for PVC. The etiology of arrhythmias was due to structural heart disease in 70 patients (58%), mainly ischemic cardiomyopathy (
Table 1). The remaining 50 patients (42%) were diagnosed with idiopathic arrhythmias.
Indications for ablation treatment are summarized in
Table 2. Several indications were possible (33 patients had two indications, and 3 patients had three indications). Antiarrhythmic drugs prior to ablation were used in a majority of patients (86 patients; 72%), mostly patients undergoing VT ablation. Details concerning the use of antiarrhythmic drugs are summarized in
Table 1.
Left ventricular ejection fraction (LVEF) was assessed with TTE in all patients undergoing VT ablation and in 48 out of 51 patients (94%) undergoing PVC ablation. Mean LVEF was 44 percent and 56 percent, respectively. This gap is understandable when different rates of structural vs. idiopathic origins of arrhythmias are being taken into account.
3.2. Catheter Ablation Procedure
In all 120 but one patient, radiofrequency was the energy source used for ablation. In one patient, cryo ablation was used for the ablation of PVC after failure with radiofrequency ablation. Most procedures were performed with local anesthesia or mild deep sedation; however, 26 out of 120 procedures (21%), mostly VT ablations, were performed with general anesthesia. Regarding the entire patient cohort, 66/120 patients (55%) underwent left-sided ablation only. Right-sided only ablation was performed in 43/120 (35.8%) patients. Four patients (3.3%) underwent ablation both in the left and in the right ventricle. In six cases (5%), additional epicardial ablation was performed, and in one patient (8.3%), ablation was performed in the left coronary cusp.
Most of the VT ablations were performed in the LV only (48 out of 69 patients, 69.6%). In 15 out of 69 patients (21.7%), VT ablation was performed in the RV only. In 8 out of 69 patients undergoing VT ablation (11.6% of all VT patients), where an epicardial substrate was expected due to history or ECG morphology, subxiphoidal epicardial access was chosen, and in 6 out of 69 VT patients (8.7%), epicardial ablation was performed (in four cases, ablation was in the LV plus epicardial; in two cases, ablation was in the RV plus epicardial).
In PVC patients, ablation only in the LV was performed in 18/51 patients (35.3%). In 28 out of 51 patients (54.9%), PVC ablation was performed in the RV only. However, in 4/51 patients (7.8%), PVC ablation was performed both in the left and in the right ventricle. In 1 out of 51 patients (2%), PVC ablation was performed in the left coronary cusp.
In 27 out of 120 procedures (23%) in this study, substrate mapping was the preferred mapping method because of hemodynamic instability during VT. We used a multielectrode mapping catheter (Pentaray, Biosense Webster, Inc., Irvine, CA, USA) from 2015 onward in 31/120 procedures (26%).
3.3. Acute Procedural Success
In the entire patient cohort, ablation procedures were successful in 112 out of 120 patients (93.3%).
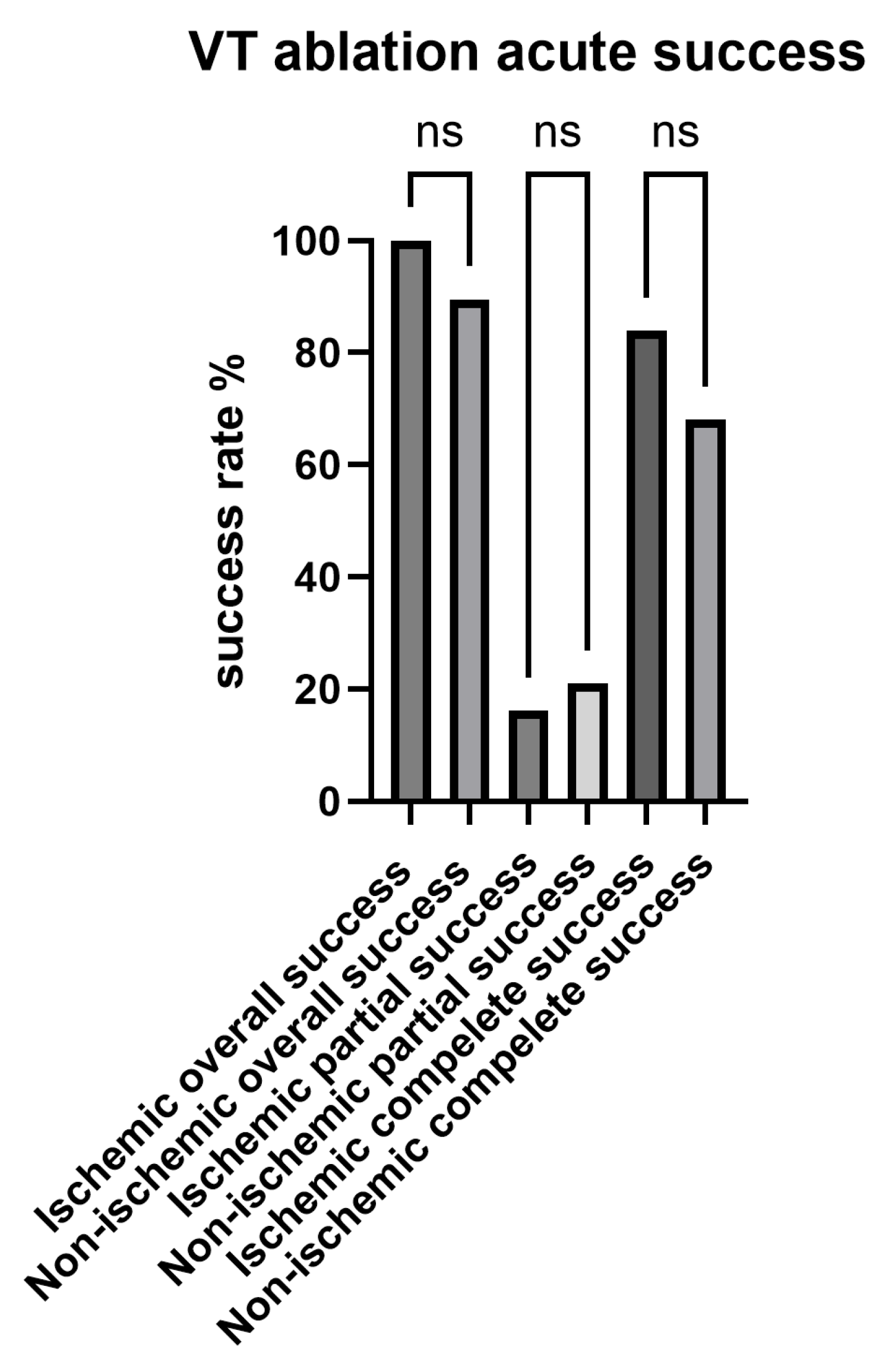
In VT ablation, acute success rate was 94.2%. Complete success was achieved in 52 out of 69 patients (75.4%), whereas partial success was achieved in 13 out of 69 patients (18.8%). Success rates in VT ablation were numerically higher for patients with ischemic cardiomyopathy as compared with non-ischemic cardiomyopathy, with complete success in 26 out of 31 patients (83.9%) vs. 26 out of 38 patients (68%) and partial success in 5 out of 31 patients (16.1%) in ischemic vs. 8 out of 38 patients (21.1%). However, the differences in success rates between ischemic and non-ischemic cardiomyopathy were not statistically different (
p = ns,
Appendix A Figure A1). In 24 out of 69 VT ablations (35%), at least one external defibrillation was necessary to treat hemodynamically unstable VT not responding to overstimulation. This was necessary in just one patient (2%) undergoing PVC ablation.
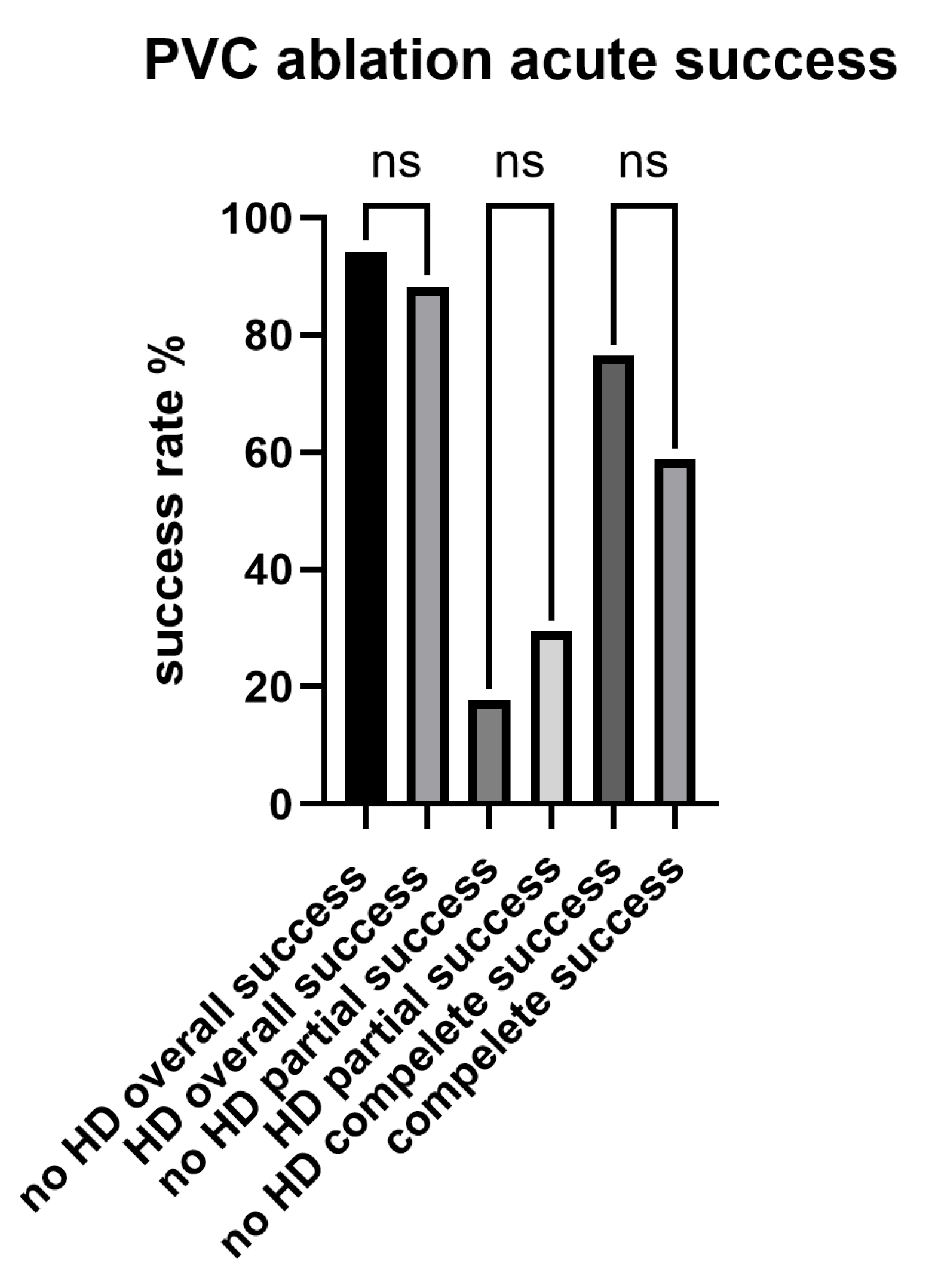
In PVC ablation, acute success rate was 92.2%. Complete success was achieved in 36 out of 51 patients (70.6%), whereas partial success was achieved in 11 out of 51 patients (21.6%). Success rates in PVC ablation were numerically higher for patients without structural heart disease as compared with patients with structural heart disease, with complete success in 26 out of 34 patients (76.5%) vs. 10 out of 17 patients (58.8%) and partial success in 6 out of 34 patients (17.7%) vs. 5 out of 17 patients (29.4%). The differences in success rates between normal hearts and structural heart disease in PVC ablation were not statistically different (
p = ns,
Appendix A Figure A2).
In most patients, one single target was ablated. However, in 36 out of 120 procedures (30%), two targets were ablated; in 18 procedures (15%), three targets were ablated and in 7 procedures (6%), four or more targets were ablated. In 32 out of 120 patients (27%), one or more antiarrhythmic drug could be discontinued after successful ablation.
3.4. Acute Complications
In 11 out of 120 patients (9%), minor or major procedural complications occurred (
Table 3). The most frequent complication was pericardial tamponade, which occurred in 6 patients (5%). Five cases of pericardial tamponade (83%) were resolved by means of percutaneous puncture, whereas one case (17%) had to be resolved by thoracotomy. Vascular complications occurred in two patients (2%). Third-degree AV block occurred in one patient (1%) and left bundle branch block in one patient (1%). In one patient (1%), periprocedural stroke was suspected, as assessed by cerebral MRI. There was no procedural complication leading to death.
3.5. Procedural Safety according to Ablation Site and Approach
In general, there was a trend towards a higher complication rate in patients undergoing left-sided ablation (8 out of 66, 12.1%) when compared with right-sided ablation (1 out of 43, 2.3%). However, this did not reach statistical significance (p = 0.085). In patients with ablation in the LV and RV (n = 4) and aortic cusp (n = 1), no complications were reported.
In patients undergoing epicardial ablation (n = 6), the complication rate was 33% (two out of six patients) with one tamponade and one left bundle branch block (epicardial plus endocardial ablation was performed in this case). Thus, we report a numerically higher rate for these patients in comparison to the remaining VT ablation group, where complications occurred in 5 out of 63 patients (7.9%). However, this did not reach statistical significance (p = ns).
3.6. Procedural Safety according to Arrhythmia Type VT vs. PVC
There were numerically higher procedural complications during VT ablations when compared with PVC ablations (7/69; 10% and 4/51; 8%, respectively). Also, the rate of pericardial tamponade was numerically higher in patients undergoing VT ablations (four patients, 6%) when compared with patients undergoing PVC ablations (two patients, 4%), but both differences were not statistically significant (p = ns).
3.7. Procedural Safety according to Presence or Absence of Structural Heart Disease
Of note, all 11 complications in our study cohort occurred in patients with structural heart disease in comparison to no complications in patients with the absence of structural heart disease. This difference was statistically significant (p = 0.0025).
In the VT subgroup, 76.8% of individuals had structural heart disease, whereas within the PVC group, 33.3% had structural heart disease. Seven complications in VT ablation (100%) occurred in patients with structural heart disease, whereas no complication occurred in patients without structural heart disease, but this difference was statistically not significant (p = ns). However, in PVC ablation, where all four complications (100%) occurred in patients with structural heart disease and none in patients without heart disease, the difference was statistically significant (p = 0.0095).
4. Discussion
4.1. Acute Success Rates of Catheter Ablation
Acute procedural success rates were reassuringly higher than 90% both in VT and PVC ablations. Comparing the acute success rates in our study with those of other studies is difficult due to large heterogeneity in patient selection, definition of clinical endpoints, ablation techniques, and other factors. The Cooled RF Ablation System clinical trial was a multicenter, prospective, nonrandomized study, enrolling patients with ischemic cardiomyopathy (ICM) with previous ICD implantation and reported acute success rates of 75 percent [
9]. It needs to be noted, however, that acute success was defined as the elimination of all mappable VTs. The Multicenter THERMOCOOL VT Ablation Trial [
10] enrolled high-risk patients with hemodynamically unstable and unmappable VTs, thus explaining the lower acute success rates of 49 percent [
10]. Another observational study [
11] reported an 81 percent rate of acute procedural success in patients with ICM.
In a study from Germany [
12], acute procedural success rates for ablation of PVC were reported to be 67% and 73% in patients <65 and >65 years of age, respectively. The authors of the German Ablation Registry [
13] reported acute success rates for PVC ablations of 82% in the overall patient group. In patients without structural heart disease, acute procedural success was significantly higher when compared with patients with structural heart disease (86 vs. 74%,
p = 0.002). Another study from the United States [
14] described acute procedural success rates of 76% in a series of 194 consecutively enrolled patients undergoing catheter ablation for PVC.
4.2. Procedural Complications
Procedural complication rates are in part driven by the degree of structural heart disease as well as by comorbidities. In the Multicenter THERMOCOOL VT Ablation Trial [
10], high-risk patients with hemodynamically unstable and unmappable VTs were enrolled. This helps explain the reported procedural mortality of 3% in the latter study. At the other end of the spectrum, some authors report no major procedural complications in low-risk patients after the ablation of PVC originating from the right ventricular outflow tract (RVOT) [
15].
In our study, two major complications occurred: one pericardial tamponade had to be resolved by means of cardiac surgery, and in one patient, periprocedural stroke was suspected as assessed by cranial MRI. Balancing between interventional success and complications is very important. Our study contains a heterogeneous patient cohort, including patients with structural heart disease (majority of patients undergoing VT ablation) and patients without structural heart disease (majority of patients undergoing PVC ablation). It is important to emphasize that all of the 11 complications in our study occurred in patients with structural heart disease. None of the patients without structural heart disease suffered from complications. We also observed a trend towards a higher number of complications in patients undergoing left-sided ablation in comparison with right-sided ablation; however, the difference did not result in statistical significance. Of note, the complication in our patient cohort that occurred in the group of right-sided ablation was a stroke. But this occurred after retrograde access of the LVOT, and thus, left-sided ablation was finally not performed.
4.3. Catheter Ablation vs. Pharmacological Treatment
A multicenter randomized controlled trial (VANISH) [
8] compared catheter ablation with escalation of antiarrhythmic drug therapy (AAD) in patients with ICM and implanted ICD who experienced VT despite treatment with AAD. The primary endpoint in the VANISH trial was a composite endpoint of all-cause mortality, appropriate ICD shock after 30 days of treatment or VT storm. There was a 28 percent relative risk reduction, reaching statistical significance, in experiencing the composite endpoint in the 132 patients randomized to the catheter ablation group. Very recently, Della Bella et al. showed in the PARTITA trial that VT ablation after the first ICD shock is associated with a reduced risk of heart failure hospitalization, mortality and recurrent ICD shocks as compared with standard therapy [
16]. Arenal et al. found reassuring results in their multicenter randomized SURVIVE-VT trial: patients with ischemic cardiomyopathy and ICD had reduced cardiovascular death, ICD shock, heart failure hospitalization or severe treatment-related complications in comparison to antiarrhythmic drug therapy [
17]. These encouraging findings may shift the field more towards catheter ablation in this patient group.
5. Conclusions
Our results confirm that catheter ablation for VT and PVC is an effective and safe therapy when performed by experienced professionals in experienced centers. Recognition of this development in the community led to increasing numbers of ablation procedures during the last years, and that will likely further increase. Patients should be considered for catheter ablation for VT at an earlier stage, given that this treatment option can change the arrhythmogenic substrate and, thereby, prevent progression over time. This argument weighs even more in young patients with idiopathic PVC, where a one-time ablation procedure is often considered curative and can prevent patients from taking AAD for long periods and, thus, from significant long-term complications.
In summary, the data in our study suggest that catheter ablation of ventricular arrhythmia in structurally normal hearts is safe, whereas periprocedural complications have to be taken into account when dealing with structural heart disease.
Limitations
We reported on acute success and complications in the catheter ablation of VT and PVC in 120 consecutive patients over 5 years. However, the population and the results concern very different patients. Moreover, we reported on acute success rates, which can be high after ablation but different a few days after. It is well known that recurrences of VT and PVC are frequent. Mortality after ablation can be delayed. Immediate good results do not mean that the patient will always improve. Our results are limited to acute success since long-term follow-up data are missing in our patient cohort.
Author Contributions
Validation, C.B.; Formal analysis, C.S. and J.B.; Investigation, L.M.H.; Data curation, C.S. and A.M.S.; Writing—original draft, C.S. and J.B.; Writing—review & editing, J.B., F.D., A.M.S. and L.M.H.; Visualization, J.B.; Supervision, F.D. and C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Kantonale Ethikkommission of the Canton of Zurich, 2016-00116 on 11 April 2016.
Informed Consent Statement
Patient consent was waived due to the retrospective and anonymized nature of the analysis.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
A.M.S. has received educational grants through his institution from Abbott, Bayer Healthcare, Biosense Webster, Biotronik, Boston Scientific, BMS/Pfizer, and Medtronic; and speaker/advisory board/consulting fees from Bayer Healthcare, Biotronik, Daiichi-Sankyo, Medtronic, Novartis, Pfizer, Stride Bio Inc. and Zoll. L.M.H. has received institutional grants from Abbott, Abiomed, Amgen, Astra Zeneca, Bayer, Biosense Webster, Biotronik, Boston Scientific, Bracco, B. Braun, Daiichi-Sankyo, Edwards, Medtronic, MicroPort, Novartis, Vascular Medical and Zoll. The other authors declare no conflict of interest.
Appendix A
Figure A1.
Differences in acute success rates in VT ablation (ischemic vs. non-ischemic); ns = not significant.
Figure A1.
Differences in acute success rates in VT ablation (ischemic vs. non-ischemic); ns = not significant.
Figure A2.
Differences in acute success rates in PVC ablation (no structural heart disease vs. structural heart disease); ns = not significant; HD = heart disease.
Figure A2.
Differences in acute success rates in PVC ablation (no structural heart disease vs. structural heart disease); ns = not significant; HD = heart disease.
References
- Brunckhorst, C.B.; Delacretaz, E.; Soejima, K.; Maisel, W.H.; Friedman, P.L.; Stevenson, W.G. Identification of the Ventricular Tachycardia Isthmus After Infarction by Pace Mapping. Circulation 2004, 110, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Palaniswamy, C.; Kolte, D.; Harikrishnan, P.; Khera, S.; Aronow, W.S.; Mujib, M.; Mellana, W.M.; Eugenio, P.; Lessner, S.; Ferrick, A.; et al. Catheter ablation of postinfarction ventricular tachycardia: Ten-year trends in utilization, in-hospital complications, and in-hospital mortality in the United States. Hear. Rhythm. 2014, 11, 2056–2063. [Google Scholar] [CrossRef] [PubMed]
- Gasperetti, A.; Sicuso, R.; Russo, A.D.; Zucchelli, G.; Saguner, A.M.; Notarstefano, P.; Soldati, E.; Bongiorni, M.G.; Della Rocca, D.G.; Mohanty, S.; et al. Prospective use of ablation index for the ablation of right ventricle outflow tract premature ventricular contractions: A proof of concept study. Europace 2021, 23, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Doppalapudi, H.; McELDERRY, H.T.; Okada, T.; Murakami, Y.; Inden, Y.; Yoshida, Y.; Kaneko, S.; Yoshida, N.; Murohara, T.; et al. Idiopathic Ventricular Arrhythmias Originating from the Papillary Muscles in the Left Ventricle: Prevalence, Electrocardiographic and Electrophysiological Characteristics, and Results of the Radiofrequency Catheter Ablation. J. Cardiovasc. Electrophysiol. 2010, 21, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; A Blom, N.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Hear. J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef] [PubMed]
- Sears, S.F.; Hauf, J.D.; Kirian, K.; Hazelton, G.; Conti, J.B. Posttraumatic stress and the implantable cardioverter-defibrillator patient what the electrophysiologist needs to know. Circ. Arrhythm. Electrophysiol. 2011, 4, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Ensslin, C.; Berg, J.; Hermes-Laufer, J.; Keller, L.S.; Niederseer, D.; Pazhenkottil, A.; von Känel, R.; Schmied, C. Depressive symptoms in patients after primary and secondary prophylactic ICD implantation. Clin. Res. Cardiol. 2022, 111, 1210–1218. [Google Scholar] [CrossRef] [PubMed]
- Sapp, J.L.; Wells, G.A.; Parkash, R.; Stevenson, W.G.; Blier, L.; Sarrazin, J.-F.; Thibault, B.; Rivard, L.; Gula, L.; Leong-Sit, P.; et al. Ventricular Tachycardia Ablation versus Escalation of Antiarrhythmic Drugs. N. Engl. J. Med. 2016, 375, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Epstein, A.; Packer, D.; Arria, A.M.; Hummel, J.; Gilligan, D.M. Catheter Ablation of Ventricular Tachycardia in Patients with Structural Heart Disease Using Cooled Ra-diofrequency Energy Results of a Prospective Multicenter Study. J. Am. Coll. Cardiol. 2000, 35, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, W.G.; Wilber, D.J.; Natale, A.; Jackman, W.M.; Marchlinski, F.E.; Talbert, T.; Nakagawa, H. Irrigated radiofrequency catheter ablation guided by electroanatomic mapping for recurrent ventricular tachycardia after myocardial infarction the multicenter thermocool ventricular tachycardia ablation trial. Circulation 2008, 118, 2773–2782. [Google Scholar] [CrossRef] [PubMed]
- Tanner, H.; Hindricks, G.; Volkmer, M.; Furniss, S.; Kühlkamp, V.; Lacroix, D.; DE Chillou, C.; Almendral, J.; Caponi, D.; Kuck, K.; et al. Catheter Ablation of Recurrent Scar-Related Ventricular Tachycardia Using Electroanatomical Mapping and Irrigated Ablation Technology: Results of the Prospective Multicenter Euro-VT-Study. J. Cardiovasc. Electrophysiol. 2010, 21, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, P.; Jungmann, J.; Huemer, M.; Parwani, A.S.; Boldt, L.-H.; Haverkamp, W.; Wutzler, A. Catheter ablation of premature ventricular contractions in elderly patients: Feasibility and success. Aging Clin. Exp. Res. 2016, 28, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Fichtner, S.; Registry, F.T.G.A.; Senges, J.; Hochadel, M.; Tilz, R.; Willems, S.; Eckardt, L.; Deneke, T.; Lewalter, T.; Dorwarth, U.; et al. Safety and efficacy in ablation of premature ventricular contraction: Data from the German ablation registry. Clin. Res. Cardiol. 2017, 106, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Baser, K.; Bas, H.D.; Yokokawa, M.; Latchamsetty, R.; Morady, F.; Bogun, F. Infrequent Intraprocedural Premature Ventricular Complexes: Implications for Ablation Outcome. J. Cardiovasc. Electrophysiol. 2014, 25, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Darrieux, F.C.; Scanavacca, M.I.; Hachul, D.T.; Melo, S.L.; D’Ávilla, A.B.; Gruppi, C.J.; Sosa, E.A. Radiofrequency Catheter Ablation of Premature Ventricular Contractions Originating in the Right Ventricular Outflow Tract. Arq. Bras. Cardiol. 2007, 88, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Della Bella, P.; Baratto, F.; Vergara, P.; Bertocchi, P.; Santamaria, M.; Notarstefano, P.; Radinovic, A. Does Timing of Ventricular Tachycardia Ablation Affect Prognosis in Patients with an Implantable Car-dioverter Defibrillator? Results from the Multicenter Randomized PARTITA Trial. Circulation 2022, 145, 1829–1838. [Google Scholar] [CrossRef] [PubMed]
- Arenal, Á.; Ávila, P.; Jiménez-Candil, J.; Tercedor, L.; Calvo, D.; Arribas, F.; Fernández-Portales, J.; Merino, J.L.; Hernández-Madrid, A.; Fernández-Avilés, F.J.; et al. Substrate Ablation vs Antiarrhythmic Drug Therapy for Symptomatic Ventricular Tachycardia. J. Am. Coll. Cardiol. 2022, 79, 1441–1453. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}