
The Potential Role of Presepsin in Predicting Severe Infection in Patients with Diabetic Foot Ulcers
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical and Biochemical Measurements
2.3. Statistical Analysis
2.4. Outcomes
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2009, 32 (Suppl. S1), S62–S67. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, N.A.; Aleppo, G.; Bannuru, R.R.; Beverly, E.A.; Bruemmer, D.; Collins, B.S.; Cusi, K.; Darville, A.; Das, S.R.; Ekhlaspour, L.; et al. Introduction and Methodology: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. S1), S1–S4. [Google Scholar]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Cusi, K.; Hilliard, M.E.; Isaacs, D.; et al. Addendum. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes—2023. Diabetes Care 2023;46(Suppl. 1):S49–S67. Diabetes Care 2023, 46, 1718–1720. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.H.; Han, K.D.; Ko, S.H.; Yang, Y.S.; Choi, J.H.; Choi, K.M.; Kwon, H.S.; Won, K.C. Diabetes Fact Sheet in Korea 2021. Diabetes Metab. J. 2022, 46, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Giri, B.; Dey, S.; Das, T.; Sarkar, M.; Banerjee, J.; Dash, S.K. Chronic hyperglycemia mediated physiological alteration and metabolic distortion leads to organ dysfunction, infection, cancer progression and other pathophysiological consequences: An update on glucose toxicity. Biomed. Pharmacother. 2018, 107, 306–328. [Google Scholar] [CrossRef] [PubMed]
- McDermott, K.; Fang, M.; Boulton, A.J.M.; Selvin, E.; Hicks, C.W. Etiology, Epidemiology, and Disparities in the Burden of Diabetic Foot Ulcers. Diabetes Care 2023, 46, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.Q.; Tang, W.; Hu, S.Q.; Fu, X.L.; Wu, H.; Shen, W.Q.; Chen, H.L. C-reactive protein and diabetic foot ulcer infections: A meta-analysis. J. Tissue Viability 2022, 31, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Jeandrot, A.; Richard, J.L.; Combescure, C.; Jourdan, N.; Finge, S.; Rodier, M.; Corbeau, P.; Sotto, A.; Lavigne, J.P. Serum procalcitonin and C-reactive protein concentrations to distinguish mildly infected from non-infected diabetic foot ulcers: A pilot study. Diabetologia 2008, 51, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Pizzolato, E.; Ulla, M.; Galluzzo, C.; Lucchiari, M.; Manetta, T.; Lupia, E.; Mengozzi, G.; Battista, S. Role of presepsin for the evaluation of sepsis in the emergency department. Clin. Chem. Lab. Med. 2014, 52, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Al-Shammaree, S.A.W.; Abu, A.B.A.; Salman, I.N. Procalcitonin levels and other biochemical parameters in patients with or without diabetic foot complications. J. Res. Med. Sci. 2017, 22, 95. [Google Scholar] [CrossRef] [PubMed]
- Umapathy, D.; Dornadula, S.; Rajagopalan, A.; Murthy, N.; Mariappanadar, V.; Kesavan, R.; Kunka Mohanram, R. Potential of circulatory procalcitonin as a biomarker reflecting inflammation among South Indian diabetic foot ulcers. J. Vasc. Surg. 2018, 67, 1283–1291.e2. [Google Scholar] [CrossRef] [PubMed]
- Velissaris, D.; Pantzaris, N.D.; Platanaki, C.; Antonopoulou, N.; Gogos, C. Procalcitonin as a diagnostic and prognostic marker in diabetic foot infection. A current literature review. Rom. J. Intern. Med. 2018, 56, 3–8. [Google Scholar] [PubMed]
- Paraskevas, T.; Chourpiliadi, C.; Demiri, S.; Micahilides, C.; Karanikolas, E.; Lagadinou, M.; Velissaris, D. Presepsin in the diagnosis of sepsis. Clin. Chim. Acta 2023, 550, 117588. [Google Scholar] [CrossRef] [PubMed]
- Azim, A. Presepsin: A Promising Biomarker for Sepsis. Indian. J. Crit. Care Med. 2021, 25, 117–118. [Google Scholar] [PubMed]
- Velissaris, D.; Zareifopoulos, N.; Karamouzos, V.; Karanikolas, E.; Pierrakos, C.; Koniari, I.; Karanikolas, M. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus 2021, 13, e15019. [Google Scholar] [CrossRef]
- Aliu-Bejta, A.; Atelj, A.; Kurshumliu, M.; Dreshaj, S.; Baršić, B. Presepsin values as markers of severity of sepsis. Int. J. Infect. Dis. 2020, 95, 1–7. [Google Scholar] [CrossRef]
- Liu, B.; Chen, Y.X.; Yin, Q.; Zhao, Y.Z.; Li, C.S. Diagnostic value and prognostic evaluation of Presepsin for sepsis in an emergency department. Crit. Care 2013, 17, R244. [Google Scholar] [CrossRef] [PubMed]
- Piccioni, A.; Santoro, M.C.; de Cunzo, T.; Tullo, G.; Cicchinelli, S.; Saviano, A.; Valletta, F.; Pascale, M.M.; Candelli, M.; Covino, M.; et al. Presepsin as Early Marker of Sepsis in Emergency Department: A Narrative Review. Medicina 2021, 57, 770. [Google Scholar] [CrossRef] [PubMed]
- Narendra, S.; Wyawahare, M.; Adole, P.S. Presepsin vs Procalcitonin as Predictors of Sepsis Outcome. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Okamura, Y. Usefulness of Presepsin Measurement: A New Biomarker for Sepsis. Rinsho Byori 2015, 63, 62–71. [Google Scholar] [PubMed]
- Chenevier-Gobeaux, C.; Bardet, V.; Poupet, H.; Poyart, C.; Borderie, D.; Claessens, Y.E. Presepsin (sCD14-ST) secretion and kinetics by peripheral blood mononuclear cells and monocytic THP-1 cell line. Ann. Biol. Clin. 2016, 74, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Cappon, G.; Vettoretti, M.; Sparacino, G.; Facchinetti, A.; Kim, M.K.; Ko, S.H.; Kim, B.Y.; Kang, E.S.; Noh, J.; Kim, S.K.; et al. 2019 Clinical Practice Guidelines for Type 2 Diabetes Mellitus in Korea. Diabetes Metab J. 2019, 43, 398–406. [Google Scholar]
- Armstrong, D.G.; Lavery, L.A.; Harkless, L.B. Validation of a diabetic wound classification system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care 1998, 21, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Ferraresi, R.; Ucci, A.; Pizzuto, A.; Losurdo, F.; Caminiti, M.; Minnella, D.; Casini, A.; Clerici, G.; Montero-Baker, M.; Mills, J. A Novel Scoring System for Small Artery Disease and Medial Arterial Calcification Is Strongly Associated With Major Adverse Limb Events in Patients With Chronic Limb-Threatening Ischemia. J. Endovasc. Ther. 2021, 28, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Yeom, J.G. PATHFAST Presepsin; Asanpharm: Seoul, Republic of Korea, 2021. [Google Scholar]
- Massara, M.; De Caridi, G.; Serra, R.; Barillà, D.; Cutrupi, A.; Volpe, A.; Cutrupi, F.; Alberti, A.; Volpe, P. The role of procalcitonin as a marker of diabetic foot ulcer infection. Int. Wound J. 2017, 14, 31–34. [Google Scholar] [CrossRef]
- Malabu, U.H.; Al-Rubeaan, K.A.; Al-Derewish, M. Diabetic foot osteomyelitis: Usefulness of erythrocyte sedimentation rate in its diagnosis. West Afr. J. Med. 2007, 26, 113–116. [Google Scholar]
- Aragón-Sánchez, J.; Víquez-Molina, G.; López-Valverde, M.E.; Rojas-Bonilla, J.M. Systemic Immune-Inflammation Index in Diabetic Foot Infections and Osteomyelitis. Int. J. Low. Extrem. Wounds 2023. online ahead of print. [Google Scholar] [CrossRef]
- Farkas, J.D. The complete blood count to diagnose septic shock. J. Thorac. Dis. 2020, 12 (Suppl. S1), S16–S21. [Google Scholar] [CrossRef]
- Biron, B.M.; Ayala, A.; Lomas-Neira, J.L. Biomarkers for Sepsis: What Is and What Might Be? Biomark. Insights 2015, 10 (Suppl. S4), 7–17. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Song, J.; Park, D.W.; Seok, H.; Ahn, S.; Kim, J.; Park, J.; Cho, H.J.; Moon, S. Diagnostic and prognostic value of presepsin and procalcitonin in non-infectious organ failure, sepsis, and septic shock: A prospective observational study according to the Sepsis-3 definitions. BMC Infect. Dis. 2022, 22, 8. [Google Scholar] [CrossRef] [PubMed]
- Baik, S.M.; Park, J.; Kim, T.Y.; Choi, S.H.; Hong, K.S. Validation of presepsin measurement for mortality prediction of sepsis: A preliminary study. Acute Crit. Care 2022, 37, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhu, Y. Utility of sTREM-1 and Presepsin (sCD14-ST) as Diagnostic and Prognostic Markers of Sepsis. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef] [PubMed]
- Endo, S.; Suzuki, Y.; Takahashi, G.; Shozushima, T.; Ishikura, H.; Murai, A.; Nishida, T.; Irie, Y.; Miura, M.; Iguchi, H.; et al. Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J. Infect. Chemother. 2012, 18, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Abdelshafey, E.E.; Nasa, P.; Elgohary, A.E.; Khalil, M.F.; Rashwan, M.A.; Ghezala, H.B.; Tayar, A.A. Role of Presepsin for the Diagnosis of Sepsis and ICU Mortality: A Prospective Controlled Study. Indian J. Crit. Care Med. 2021, 25, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Lee, B.; Yoon, S.J.; Park, C.M.; Jung, C.W.; Ahn, M.J.; Park, H.D.; Hwang, S.Y.; Shin, T.G.; Kang, E.S. Complementary Use of Presepsin with the Sepsis-3 Criteria Improved Identification of High-Risk Patients with Suspected Sepsis. Biomedicines 2021, 9, 1076. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.; Perna, B.; Maritati, M.; Remelli, F.; Trevisan, C.; Spampinato, M.D.; Costanzini, A.; Volpato, S.; Contini, C.; De Giorgio, R. Presepsin levels and COVID-19 severity: A systematic review and meta-analysis. Clin. Exp. Med. 2023, 23, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Delva, M.L.; Samuel, L.T.; Acuña, A.J.; Kamath, A.F. Presepsin as a diagnostic biomarker of peri-prosthetic joint infection: A review of the literature. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 695–700. [Google Scholar] [CrossRef]
- Chang, Y.; Liu, L.; Wang, H.; Liu, J.; Liu, Y.; Du, C.; Hua, M.; Liu, X.; Liu, J.; Li, A. Presepsin Predicts Severity and Secondary Bacterial Infection in COVID-19 by Bioinformatics Analysis. Comput. Math. Methods Med. 2022, 2022, 9914927. [Google Scholar] [CrossRef]
- Zhang, H.Y.; Lu, Z.Q.; Wang, G.X.; Xie, M.R.; Li, C.S. Presepsin as a biomarker for risk stratification for acute cholangitis in emergency department: A single-center study. World J. Clin. Cases 2021, 9, 9857–9868. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, K.; Hata, A.; Fujita, M.; Hatachi, S.; Yagita, M. Presepsin and procalcitonin as biomarkers of systemic bacterial infection in patients with rheumatoid arthritis. Int. J. Rheum. Dis. 2018, 21, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Igna, R.; Gîrleanu, I.; Cojocariu, C.; Huiban, L.; Muzîca, C.; Sîngeap, A.M.; Sfarti, C.; Chiriac, S.; Petrea, O.C.; Zenovia, S.; et al. The Role of Presepsin and Procalcitonin in Early Diagnosis of Bacterial Infections in Cirrhotic Patients with Acute-on-Chronic Liver Failure. J. Clin. Med. 2022, 11, 5410. [Google Scholar] [CrossRef] [PubMed]
- Qi, Z.J.; Yu, H.; Zhang, J.; Li, C.S. Presepsin as a novel diagnostic biomarker for differentiating active pulmonary tuberculosis from bacterial community acquired pneumonia. Clin. Chim. Acta 2018, 478, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Shiota, J.; Tagawa, H.; Ohura, N.; Kasahara, H. Presepsin is a potent biomarker for diagnosing skin wound infection in hemodialysis patients compared to white blood cell count, high-sensitivity C-reactive protein, procalcitonin, and soluble CD14. Ren. Replace. Ther. 2017, 3, 31. [Google Scholar] [CrossRef]
- Karakas, A.; Arslan, E.; Cakmak, T.; Aydin, I.; Akgul, E.O.; Demirbas, S. Predictive Value of Soluble CD14, Interleukin-6 and Procalcitonin For Lower Extremity Amputation in People with Diabetes with Foot Ulcers: A Pilot Study. Pak. J. Med. Sci. 2014, 30, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Chenevier-Gobeaux, C.; Trabattoni, E.; Roelens, M.; Borderie, D.; Claessens, Y.E. Presepsin (sCD14-ST) in emergency department: The need for adapted threshold values? Clin. Chim. Acta 2014, 427, 34–36. [Google Scholar] [CrossRef]
- Arakawa, K.; Saeki, A.; Ide, R.; Matsushita, Y. Presepsin cut-off value for diagnosis of sepsis in patients with renal dysfunction. PLoS ONE 2022, 17, e0273930. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Liu, J.; Sun, H. Risk factors for lower extremity amputation in patients with diabetic foot ulcers: A meta-analysis. PLoS ONE 2020, 15, e0239236. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No Amputation (n = 27) | Amputation (n = 46) | p Value | |
|---|---|---|---|
| Age (year) | 60.2 ± 18.3 | 61.8 ± 14.1 | 0.95 |
| Gender (male %) | 12 (44.4%) | 32 (69.6%) | 0.04 |
| BMI 1 (kg/m2) | 22.4 ± 4.9 | 24.1 ± 4.2 | 0.06 |
| Duration of diabetes (year) | 19.1 ± 8.8 | 18.2 ± 9.6 | 0.69 |
| Hospital stays (day) | 21.1 ± 11.4 | 32.4 ± 18.7 | <0.01 |
| HbA1c 2 (%) | 8.5 ± 2.1 | 9.2 ± 2.5 | 0.28 |
| BUN 3 (mg/dL) | 26.4 ± 14.7 | 30.5 ± 19.1 | 0.47 |
| Creatinine (mg/dL) | 1.7 ± 1.3 | 3.0 ± 3.4 | 0.31 |
| eGFR 4 (mL/min/1.73 m2) | 57.5 ± 34.2 | 56.1 ± 49.0 | 0.48 |
| Osteomyelitis (%) | 6 (22.2%) | 36 (78.3%) | <0.01 |
| Ankle Brachial Index | 0.9 ± 0.4 | 0.9 ± 0.4 | 0.90 |
| Toe Brachial Index | 0.5 ± 0.4 | 0.4 ± 0.4 | 0.17 |
| Wound culture (%) | 19 (26.0%) | 41 (56.2%) | 0.05 |
| Texas grade | |||
| Grade 0 | 0 (0%) | 1 (1.4%) | <0.01 |
| Grade 1 | 15 (20.5%) | 10 (13.7%) | |
| Grade 2 | 9 (12.3%) | 18 (24.7%) | |
| Grade 3 | 3 (4.1%) | 17 (23.3%) | |
| Texas stage | |||
| Stage A | 6 (8.2%) | 6 (8.2%) | 0.88 |
| Stage B | 6 (8.2%) | 18 (24.7%) | |
| Stage C | 7 (9.6%) | 7 (9.6%) | |
| Stage D | 8 (11.0%) | 15 (20.5%) | |
| MAC 5 score | |||
| No | 20 (27.4%) | 28 (38.4%) | 0.50 |
| Moderate | 3 (4.1%) | 17 (23.3%) | |
| Severe | 4 (5.4%) | 1 (1.4%) | |
| Smoking (%) | 4 (5.5%) | 16 (21.9%) | 0.07 |
| Drinking (%) | 3 (4.1%) | 8 (11.0%) | 0.47 |
| Hypertension (%) | 19 (26.0%) | 27 (37.0%) | 0.32 |
| Dialysis (%) | 2 (2.7%) | 12 (16.4%) | 0.05 |
| Diabetic retinopathy (%) | 4 (5.5%) | 13 (17.8%) | 0.19 |
| Diabetic neuropathy (%) | 2 (2.7%) | 5 (6.8%) | 0.63 |
| Stroke (%) | 4 (5.5%) | 4 (5.5%) | 0.42 |
| Coronary artery disease (%) | 7 (9.6%) | 12 (16.4%) | 0.99 |
| Presepsin (pg/mL) | <675 (n = 33) | ≥675 (n = 40) | p Value |
|---|---|---|---|
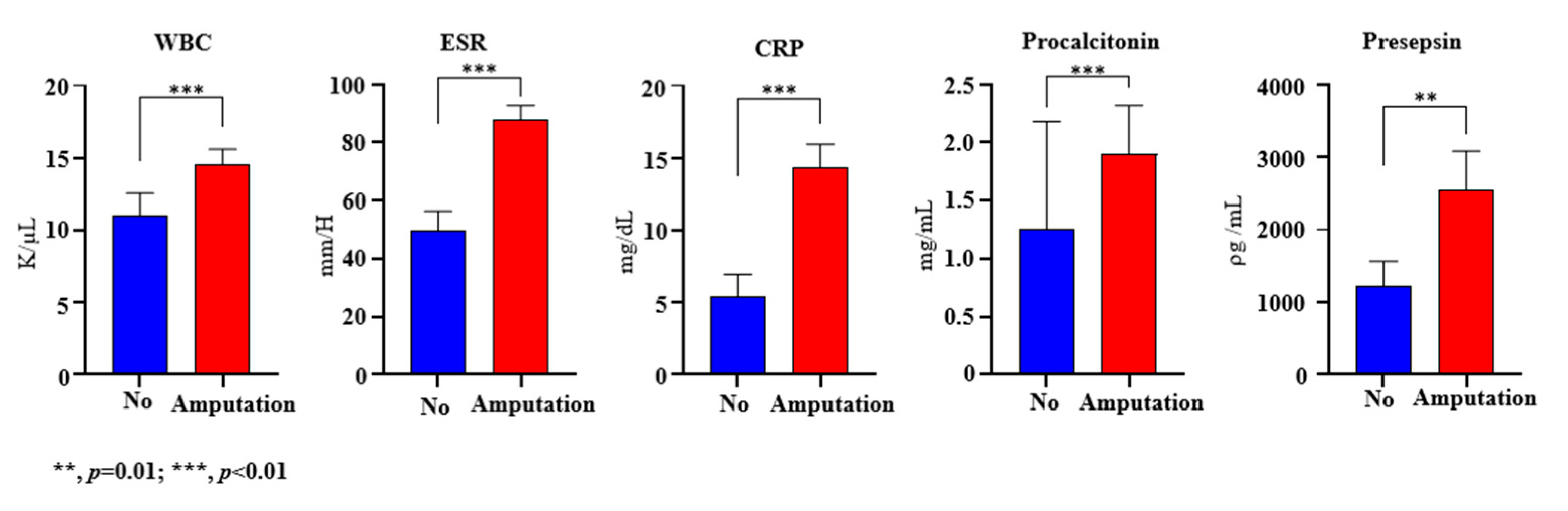
| Presepsin (pg/mL) | 428.6 ± 158.7 | 3402.2 ± 3728.9 | <0.01 |
| Age (year) | 65.0 ± 15.3 | 58.0 ± 15.4 | 0.04 |
| Gender (male %) | 19 (26.0%) | 25 (34.2%) | 0.67 |
| BMI (kg/m2) | 22.2 ± 5.0 | 24.5 ± 3.8 | 0.01 |
| Duration of diabetes (year) | 21.7 ± 8.6 | 15.9 ± 9.0 | 0.01 |
| Hospital stays (day) | 25.0 ± 19.5 | 30.9 ± 14.8 | 0.02 |
| Wound culture (%) | 27 (37%) | 33 (45.2%) | 0.94 |
| WBC (K/µL) | 9.4 ± 3.5 | 16.4 ± 8.8 | <0.01 |
| ESR (mm/H) | 53.8 ± 36.2 | 89.0 ± 35.2 | <0.01 |
| CRP (mg/dL) | 4.8 ± 5.5 | 16.3 ± 11.1 | <0.01 |
| Procalcitonin (mg/mL) | 0.1 ± 0.2 | 2.9 ± 4.6 | <0.01 |
| HbA1c (%) | 8.6 ± 2.3 | 9.2 ± 2.5 | 0.23 |
| eGFR (mL/min/1.73 m2) | 76.9 ± 43.7 | 39.8 ± 36.7 | <0.01 |
| Ankle Brachial Index | 18 (24.7%) | 24 (32.9%) | 0.64 |
| Toe Brachial Index | 0.9 ± 0.4 | 0.9 ± 0.4 | 0.78 |
| Osteomyelitis (%) | 0.5 ± 0.4 | 0.4 ± 0.4 | 0.64 |
| Texas grade | |||
| Grade 0 | 0 (0.0%) | 1 (1.4%) | 0.24 |
| Grade 1 | 14 (19.2%) | 11 (15.1%) | |
| Grade 2 | 12 (16.4%) | 15 (20.5%) | |
| Grade 3 | 7 (9.6%) | 13 (17.8%) | |
| Texas stage | |||
| Stage A | 4 (5.5%) | 8 (10.9%) | 0.48 |
| Stage B | 11 (15.1%) | 13 (17.8%) | |
| Stage C | 7 (9.6%) | 7 (9.6%) | |
| Stage D | 11 (15.1%) | 12 (16.4%) | |
| Amputation | |||
| No | 18 (24.7%) | 9 (12.3%) | <0.01 |
| Minor | 13 (17.8%) | 21 (28.8%) | |
| Major | 2 (2.7%) | 10 (13.7%) | |
| MAC score | |||
| No | 26 (35.6%) | 22 (30.2%) | 0.05 |
| Moderate | 5 (6.9%) | 15 (20.5%) | |
| Severe | 2 (2.7%) | 3 (4.1%) |
| Crude OR 1 (95% CI) | Crude p Value | Adjusted 2 OR (95% CI) | Adjusted p Value | |
|---|---|---|---|---|
| Age (year) | 1.06 (1.00, 1.13) | 0.06 | 1.06 (1.00, 1.13) | 0.05 |
| Gender (male %) | 0.68 (0.11, 4.05) | 0.67 | ||
| WBC (K/µL) | 0.79 (0.67, 0.93) | 0.01 | 0.79 (0.67, 0.93) | 0.01 |
| ESR (mm/H) | 1.03 (0.99, 1.07) | 0.13 | 1.03 (1.00, 1.06) | 0.05 |
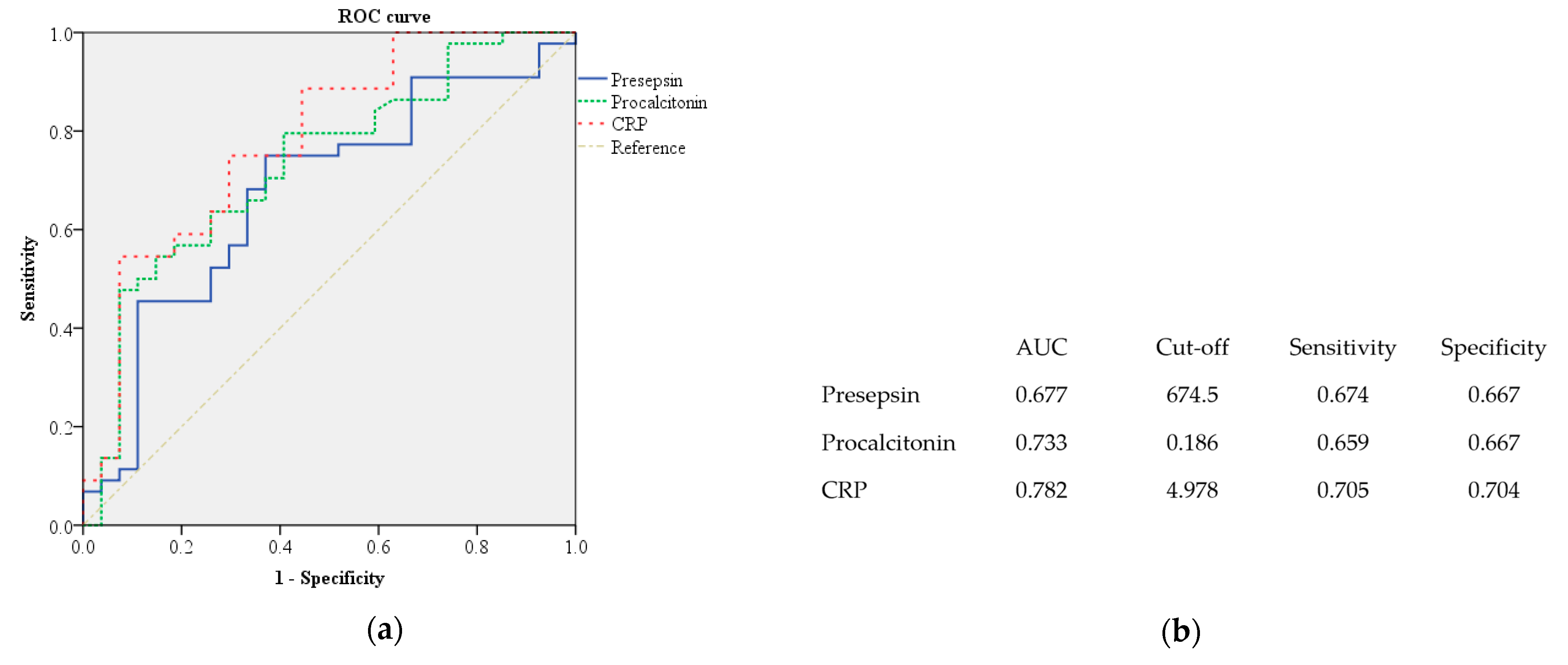
| CRP ≥ 4.978 (mg/dL) | 0.74 (0.05, 11.60) | 0.83 | ||
| Procalcitonin ≥ 0.186 (mg/mL) | 0.60 (0.07, 5.15) | 0.64 | ||
| Presepsin ≥ 675 (pg/mL) | 171.91 (5.12, 5770.37) | <0.01 | 64.64 (4.14, 1010.23) | <0.01 |
| HbA1c (%) | 1.81 (0.96, 3.41) | 0.07 | 1.80 (1.03, 3.12) | 0.04 |
| Osteomyelitis (%) | 152.67 (10.61, 2196.24) | <0.01 | 134.99 (10.33, 1763.35) | <0.01 |
| eGFR (mL/min/1.73 m2) | 1.01 (0.99, 1.04) | 0.31 | ||
| Wound culture (%) | 1.95 (0.12, 30.50) | 0.64 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, E.Y.; Park, I.R.; Chung, S.M.; Roh, Y.N.; Park, C.H.; Kim, T.-G.; Kim, W.; Moon, J.S. The Potential Role of Presepsin in Predicting Severe Infection in Patients with Diabetic Foot Ulcers. J. Clin. Med. 2024, 13, 2311. https://doi.org/10.3390/jcm13082311
Ha EY, Park IR, Chung SM, Roh YN, Park CH, Kim T-G, Kim W, Moon JS. The Potential Role of Presepsin in Predicting Severe Infection in Patients with Diabetic Foot Ulcers. Journal of Clinical Medicine. 2024; 13(8):2311. https://doi.org/10.3390/jcm13082311
Chicago/Turabian StyleHa, Eun Yeong, Il Rae Park, Seung Min Chung, Young Nam Roh, Chul Hyun Park, Tae-Gon Kim, Woong Kim, and Jun Sung Moon. 2024. "The Potential Role of Presepsin in Predicting Severe Infection in Patients with Diabetic Foot Ulcers" Journal of Clinical Medicine 13, no. 8: 2311. https://doi.org/10.3390/jcm13082311