
Impact of Effectiveness of Physical Activity in a Virtual Environment on the Regulation of Sclerostin and Interleukin 6 Levels in Haemodialysis Patients

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
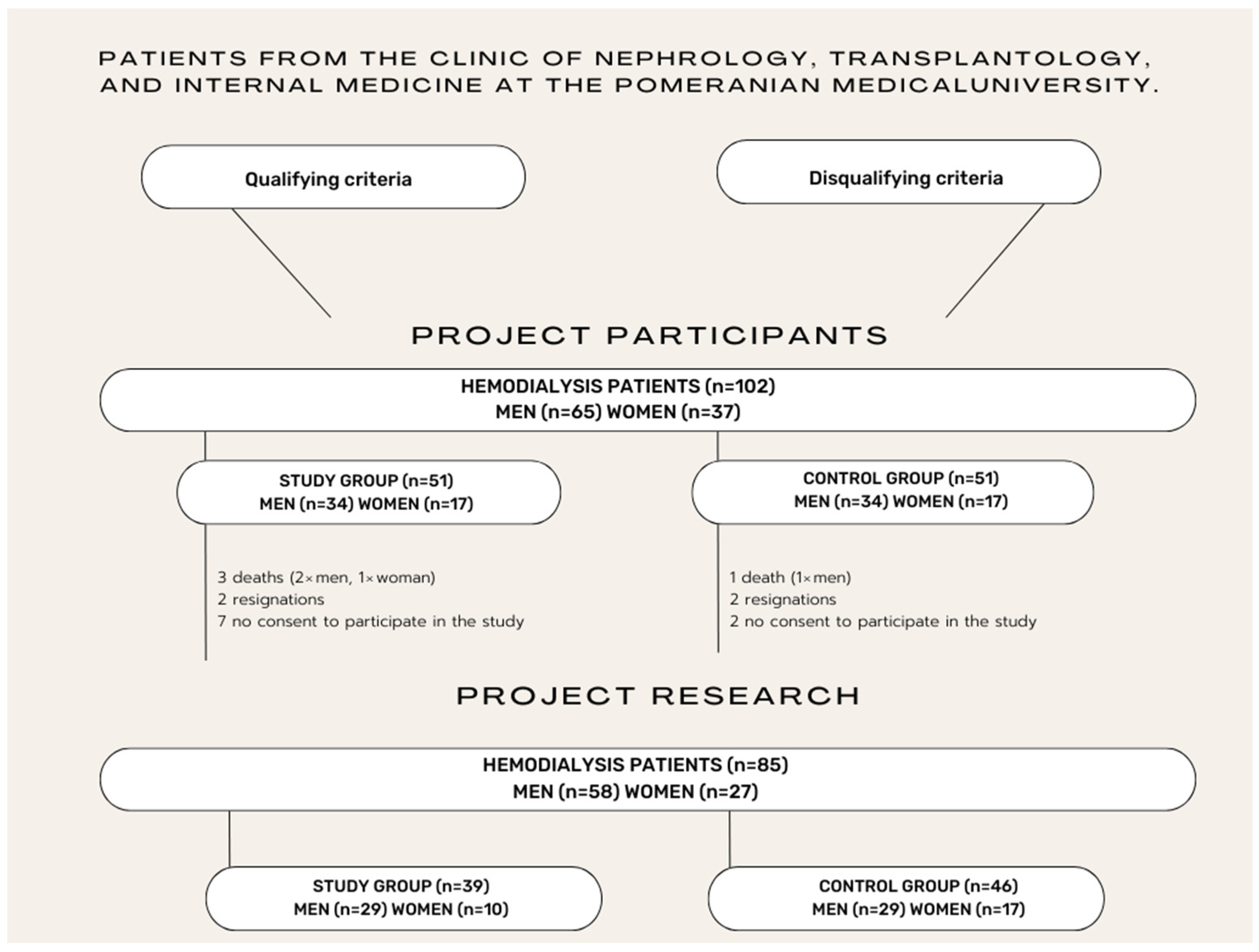
2.1. Patients
2.2. Study Process
2.2.1. Level of Physical Activity
- (1)
- High—individuals with 3 or more days of intensive exercise (at least 1500 MET) or 7 or more days of any exercise (at least 3000 MET per week)
- (2)
- Adequate—individuals with 3 or more days of intensive exercise (at least 20 min/day) or 3 or more days of moderate exercise/walking (at least 30 min/day) or 5 or more days of any exercise (at least 600 MET per week)
- (3)
- Insufficient—lack of activity or did not meet the criteria for adequate and high activity [19].
2.2.2. Level of Physical Capacity
2.2.3. Blood Sampling
2.2.4. ELISA Tests
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xiong, L.; Jung, J.U.; Wu, H.; Xia, W.F.; Pan, J.X.; Shen, C.; Mei, L.; Xiong, W.C. Lrp4 in osteoblasts suppresses bone formation and promotes osteoclastogenesis and bone resorption. Proc. Natl. Acad. Sci. USA 2015, 112, 3487–3492. [Google Scholar] [CrossRef] [PubMed]
- Barcellos, F.C.; Santos, I.S.; Umpierre, D.; Bohlke, M.; Hallal, P.C. Effects of exercise in the whole spectrum of chronic kidney disease: A systematic review. Clin. Kidney J. 2015, 8, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Turon-Skrzypinska, A.; Dutkiewicz, G.; Marchelek-Mysliwiec, M.; Dziedziejko, V.; Ciechanowski, K.; Ryl, A.; Rotter, I. Assessment of Sclerostin and Interleukin 6 Levels and Selected Anthropometric Parameters in Patients Receiving Hemodialysis Replacement Therapy—Pilot Study. Medicina 2019, 55, 784. [Google Scholar] [CrossRef] [PubMed]
- Turoń-Skrzypińska, A.; Dutkiewicz, G.; Marchelek-Myśliwiec, M.; Rył, A.; Dziedziejko, V.; Safranow, K.; Ciechanowski, K.; Rotter, I. Physical Activity versus Sclerostin and Interleukin 6 Concentration in Patients Receiving Renal Replacement Therapy by Hemodialysis. Risk Manag. Healthc. Policy 2020, 7, 1467–1475. [Google Scholar] [CrossRef] [PubMed]
- Bonani, M.; Rodriguez, D.; Fehr, T.; Mohebbi, N.; Brockmann, J.; Blum, M.; Graf, N.; Frey, D.; Wüthrich, R.P. Sclerostin blood levels before and after kidney transplantation. Kidney Blood Press. Res. 2014, 39, 230–239. [Google Scholar] [CrossRef]
- Desjardins, L.; Liabeuf, S.; Oliveira, R.B.; Louvet, L.; Kamel, S.; Lemke, H.D.; Vanholder, R.; Choukroun, G.; Massy, Z.A.; European Uremic Toxin (EUTox) Work Group. Uremic toxicity and sclerostin in chronic kidney disease patients. Nephrol. Ther. 2014, 10, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Jean, G.; Chazot, C.; Bresson, E.; Zaoui, E.; Cavalier, E. High Serum Sclerostin Levels Are Associated with a Better Outcome in Haemodialysis Patients. Nephron 2016, 132, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Evenepoel, P.; Claes, K.; Viaene, L.; Bammens, B.; Meijers, B.; Naesens, M.; Sprangers, B.; Kuypers, D. Decreased Circulating Sclerostin Levels in Renal Transplant Recipients With Persistent Hyperparathyroidism. Transplantation 2016, 100, 2188–2193. [Google Scholar] [CrossRef] [PubMed]
- Janik, M.; Stuss, M.; Michalska-Kasiczak, M.; Jegier, A.; Sewerynek, E. Effects of physical activity on sclerostin concentrations. Endokrynol. Pol. 2018, 69, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Storer, T.W. Exercise Training for Individuals with Advanced Chronic Kidney Disease. In Red: Nutritional Management of Renal Disease, 3rd ed.; Joel, D., Ed.; Academic Press: Amsterdam, The Netherlands, 2013; pp. 739–773. [Google Scholar]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- Aksoy, A.; Akpınar, T.S.; Yıldız, A.; Akgül, S.U.; Torun, E.S.; Oğuz, F.S.; Erten, N.; Taşçıoğlu, C.; Saka, B. Association of inflammation with nutritional status, lean body mass, and physical activity in non-dialysis-dependent chronic kidney disease. Clin. Sci. Nutr. 2019, 1, 16–23. [Google Scholar] [CrossRef]
- Gracia-Iguacel, C.; González-Parra, E.; Barril-Cuadrado, G.; Sánchez, R.; Egido, J.; Ortiz-Arduán, A.; Carrero, J.J. Defining protein-energy wasting syndrome in chronic kidney disease: Prevalence and clinical implications. Nefrología 2014, 34, 507–519. [Google Scholar]
- Yamaguchi, T.; Yabe, H.; Kono, K.; Moriyama, Y.; Yamada, T. Influence of sex differences in maintenance-hemodialysis participants on motivation of exercise therapy implementation: A multicenter cross-sectional study. J. Nephrol. 2022, 35, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Turoń-Skrzypińska, A.; Tomska, N.; Mosiejczuk, H.; Rył, A.; Szylińska, A.; Marchelek-Myśliwiec, M.; Ciechanowski, K.; Nagay, R.; Rotter, I. Impact of virtual reality exercises on anxiety and depression in hemodialysis. Sci. Rep. 2023, 1, 12435. [Google Scholar] [CrossRef]
- Segura-Ortí, E.; Pérez-Domínguez, B.; Ortega-Pérez de Villar, L.; Meléndez-Oliva, E.; Martínez-Gramage, J.; García-Maset, R.; Gil-Gómez, J.A. Virtual reality exercise intradialysis to improve physical function: A feasibility randomized trial. Scand. J. Med. Sci. Sports 2019, 29, 89–94. [Google Scholar] [CrossRef]
- Cho, H.; Sohng, K.Y. The effect of a virtual reality exercise program on physical fitness, body composition, and fatigue in hemodialysis patients. J. Phys. Ther. Sci. 2014, 26, 1661–1665. [Google Scholar] [CrossRef]
- Brończyk-Puzoń, A.; Koszowska, A.; Bieniek, J. Podstawowe pomiary antropometryczne i pochodne wskaźniki w poradnictwie dietetycznym–część pierwsza. Piel. Zdr. Publ. 2018, 8, 217–222. [Google Scholar] [CrossRef][Green Version]
- Biernat, E.; Stupnicki, R.; Gajewski, A. International Physical Activity Questionnaire (IPAQ)—Polish version. Wych. Fiz. Sport 2007, 51, 47–54. [Google Scholar]
- Singh, S.J.; Puhan, M.A.; Andrianopoulos, V.; Hernandes, N.A.; Mitchell, K.E.; Hill, C.J.; Lee, A.L.; Camillo, C.A.; Troosters, T.; Spruit, M.A.; et al. An official systematic review of the European Respiratory Society/American Thoracic Society: Measurement properties of field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1447–1478. [Google Scholar] [CrossRef] [PubMed]
- Perez-Dominguez, B.; Casaña-Granell, J.; Garcia-Maset, R.; Garcia-Testal, A.; Melendez-Oliva, E.; Segura-Orti, E. Effects of exercise programs on physical function and activity levels in patients undergoing hemodialysis: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2021, 57, 994–1001. [Google Scholar] [CrossRef]
- Rhee, S.Y.; Song, J.K.; Hong, S.C.; Choi, J.W.; Jeon, H.J.; Shin, D.H.; Ji, E.H.; Choi, E.H.; Lee, J.; Kim, A.; et al. Intradialytic exercise improves physical function and reduces intradialytic hypotension and depression in hemodialysis patients. Korean J. Intern. Med. 2019, 34, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Z.; Zheng, K.; Zhang, H.; Feng, J.; Wang, L.; Zhou, H. Physical Exercise and Patients with Chronic Renal Failure: A Meta-Analysis. BioMed Res. Int. 2017, 2017, 7191826. [Google Scholar] [CrossRef] [PubMed]
- Turoń-Skrzypińska, A.; Rotter, I.; Przybyciński, J.; Szylińska, A.; Mińko, A.; Ciechanowski, K.; Dutkiewicz, G. Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8? J. Clin. Med. 2023, 17, 5358. [Google Scholar] [CrossRef] [PubMed]
- Weber-Nowakowska, K.; Gębska, M.; Myślak, M.; Żyżniewska-Banaszak, E.; Stecko, M. Rola aktywności fizycznej w leczeniu pacjentów z przewlekłą chorobą nerek. Pomeranian J. Life Sci. 2017, 63, 27–30. [Google Scholar] [CrossRef][Green Version]
- Fang, H.Y.; Burrows, B.T.; King, A.C.; Wilund, K.R. A Comparison of Intradialytic versus Out-of-Clinic Exercise Training Programs for Hemodialysis Patients. Blood Purif. 2020, 49, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Segura-Ortí, E.; García-Testal, A. Intradialytic virtual reality exercise: Increasing physical activity through technology. Semin. Dial. 2019, 32, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Kalampakos, N.; Fousekis, K.; Mylonas, K.; Angelopoulos, P.; Matzaroglou, C.; Bita, T.; Gliatis, J.; Tsepis, E.; Billis, E. Risk of sarcopenia, fear of COVID-19, anxiety, depression and physical activity levels: Associations across patients on hemodialysis within Greece. J. Frailty Sarcopenia Falls 2023, 8, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, R.L.; Micali, P.N.; Carmo, E.G.; Orlandi, F.D.; Costa, J.L. Cognitive abilities and physical activity in chronic kidney disease patients undergoing hemodialysis. Dement. Neuropsychol. 2019, 13, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Nah, R.; Robertson, N.; Niyi-Odumosu, F.A.; Clarke, A.L.; Bishop, N.C.; Smith, A.C. Relationships between illness representations, physical activity and depression in chronic kidney disease. J. Ren. Care 2019, 45, 74–82. [Google Scholar] [CrossRef]
- Tamiya, H.; Tamura, Y.; Mochi, S.; Akazawa, Y.; Mochi, Y.; Banba, N.; Nakatani, Y.; Hoshiai, M.; Ueno, A.; Nagao, M.; et al. Extended Sedentary Time Increases the Risk of All-Cause Death and New Cardiovascular Events in Patients ith Diabetic Kidney Disease. Circ. J. 2020, 84, 2190–2197. [Google Scholar] [CrossRef]
- Rosa, C.S.; Gracia-Marco, L.; Barker, A.R.; Freitas, I.F.; Monteiro, H.L. Assessment of Physical Activity by Accelerometer and IPAQ-Short Version in Patients with Chronic Kidney Disease Undergoing Hemodialysis. Blood Purif. 2015, 40, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Grzegorzewska, A.E.; Izdebska, A.; Niepolski, L.; Warchoł, W.; Jagodziński, P.P. Self-Reported Physical Activity, Quality of Life, and Psychological Status in Relation to Plasma 25-Hydroxyvitamin D Concentration in Patients Treated with Hemodialysis. Kidney Blood Press. Res. 2016, 41, 886–900. [Google Scholar] [CrossRef] [PubMed]
- Tabibi, M.A.; Cheema, B.; Salimian, N.; Corrêa, H.L.; Ahmadi, S. The effect of intradialytic exercise on dialysis patient survival: A randomized controlled trial. BMC Nephrol. 2023, 24, 100. [Google Scholar] [CrossRef] [PubMed]
- Arazi, T.; Aliasgharpour, M.; Mohammadi, S.; Mohammadi, N.; Kazemnejad, A. Effect of a Breathing Exercise on Respiratory Function and 6-Minute Walking Distance in Patients Under Hemodialysis: A Randomized Controlled Trial. J. Nurs. Res. 2021, 29, e146. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Kim, J.C.; Shapiro, B.B.; Zhang, M.; Li, Y.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Kalantar-Zadeh, K. Factors affecting daily physical activity and physical performance in maintenance dialysis patients. J. Ren. Nutr. 2015, 25, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Kono, K.; Nishida, Y.; Moriyama, Y.; Yabe, H.; Taoka, M.; Sato, T. Investigation of factors affecting the six-minute walk test results in hemodialysis patients. Ther. Apher. Dial. 2014, 18, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Baião, V.M.; Cunha, V.A.; Duarte, M.P.; Andrade, F.P.; Ferreira, A.P.; Nóbrega, O.T.; Viana, J.L.; Ribeiro, H.S. Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Metabolites 2023, 13, 795. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Ketteler, M.; Johnson, R.J.; Lindholm, B.; Pecoits-Filho, R.; Riella, M.; Heimbürger, O.; Cederholm, T.; Girndt, M. IL-10, IL-6, and TNF-alpha: Central factors in the altered cytokine network of uremia--the good, the bad, and the ugly. Kidney Int. 2005, 67, 1216–1233. [Google Scholar] [CrossRef]
- Cheema, B.S.B.; Abas, H.; Smith, B.C.F.; O’Sullivan, A.J.; Chan, M.; Patwardhan, A.; Kelly, J.; Gillin, A.; Pang, G.; Lloyd, B.; et al. Effect of resistance training during hemodialysis on circulating cytokines: A randomized controlled trial. Eur. J. Appl. Physiol. 2011, 111, 1437–1445. [Google Scholar] [CrossRef]
- Cruz, L.G.D.; Zanetti, H.R.; Andaki, A.C.R.; Mota, G.R.; Neto, O.B.; Mendes, E.L. Intradialytic aerobic training improves inflammatory markers in patients with chronic kidney disease: A randomized clinical trial. Mot. Rev. Educ. Física 2018, 24, e017517. [Google Scholar] [CrossRef][Green Version]
- Liao, M.T.; Liu, W.C.; Lin, F.H.; Huang, C.F.; Chen, S.Y.; Liu, C.C.; Lin, S.H.; Lu, K.C.; Wu, C.C. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine 2016, 95, e4134. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Oliva, E.; Sánchez-Vera Gómez-Trelles, I.; Segura-Orti, E.; Pérez-Domínguez, B.; García-Maset, R.; García-Testal, A.; Lavandera-Díaz, J.L. Effect of an aerobic and strength exercise combined program on oxidative stress and inflammatory biomarkers in patients undergoing hemodialysis: A single blind randomized controlled trial. Int. Urol. Nephrol. 2022, 54, 2393–2405. [Google Scholar] [CrossRef] [PubMed]
- Gombos, G.C.; Bajsz, V.; Pék, E.; Schmidt, B.; Sió, E.; Molics, B.; Betlehem, J. Direct effects of physical training on markers of bone metabolism and serum sclerostin concentrations in older adults with low bone mass. BMC Musculoskelet. Disord. 2016, 17, 254. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Amrein, S.; Drexler, C.; Dimai, H.P.; Dobnig, H.; Pfeifer, K.; Tomaschitz, A.; Pieber, T.R.; Fahrleitner-Pammer, A. Sclerostin and its association with physical activity, age, gender, body composition, and bone mineral content in healthy adults. J. Clin. Endocrinol. Metab. 2012, 97, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Ardawi, M.S.M.; Al-Kadi, H.A.; Rouzi, A.A.; Quari, M.H. Determinants of serum sclerostin in healthy pre- and postmenopausal women. J. Bone Miner. Res. 2011, 26, 2812–2822. [Google Scholar] [CrossRef] [PubMed]
- Frings-Meuthen, P.; Boehme, G.; Liphard, A.M.; Baecker, N.; Heer, M.; Rittweger, J. Sclerostin and DKK1 levels during 14 and 21 days of bed rest in healthy young men. J. Musculoskelet. Neuronal Interact. 2013, 13, 45–52. [Google Scholar]
- Gaudio, A.; Pennisi, P.; Bratengeier, C.; Torrisi, V.; Lindner, B.; Mangiafico, R.A.; Pulvirenti, I.; Hawa, G.; Tringali, G.; Fiore, C.E. Increased sclerostin serum levels associated with bone formation and resorption markers in patients with immobilization-induced bone loss. J. Clin. Endocrinol. Metab. 2010, 95, 2248–2253. [Google Scholar] [CrossRef]


{kind=link}
| Qualifying Criteria | Disqualifying Criteria |
|---|---|
|
|
| Physical activity in MET min/week | = | Number of days per week during which physical activity occurred | × | Average duration of activity | × | MET value |
| Level of physical activity | = | MET (intensive exercise) | + | MET (moderate exercise) | + | MET (walking) |
| Study Group (n = 39) | Control Group (n = 46) | p | ||
|---|---|---|---|---|
| Age, mean [SD; Me] | 57.56 [17.61; 63.0] | 62.63 [15.47; 64.0] | 0.27 | |
| Sex, n (%) | males | 29 (74.36%) | 29 (63.04%) | 0.26 |
| females | 10 (25.64%) | 17 (36.96%) | ||
| BMI (kg/m2) | 28.23 [5.75; 28.28] | 27.89 [5.79; 27.57] | 0.76 | |
| Professional activity currently, n (%) | no | 26 (72.22%) | 40 (88.89%) | 0.10 |
| yes | 10 (27.78%) | 5 (11.11%) | ||
| Professional activity before the start of haemodialysis, n (%) | no | 10 (27.78%) | 21 (46.67%) | 0.08 |
| yes | 26 (72.22%) | 24 (53.33%) | ||
| Type of job, n (%) | blue-collar | 18 (47.37%) | 18 (54.55%) | 0.83 |
| white-collar | 11 (28.95%) | 7 (21.21%) | ||
| no job | 9 (23.68%) | 8 (24.24%) | ||
| Currently smoking cigarettes, n (%) | no | 30 (76.92%) | 35 (76.09%) | 0.87 |
| yes | 9 (23.08%) | 11 (23.91%) | ||
| Number of cigarettes per day, mean [SD; Me] | 14.44 [6.13; 15.0] | 14.09 [7.41; 10.0] | 0.68 | |
| How many years ago quit smoking, mean [SD; Me] | 9.71 [10.95; 5.0] | 16.67 [16.17; 13.0] | 0.52 | |
| Number of HD per week, mean [SD; Me] | 2.95 [0.23; 3.0] | 2.98 [0.15; 3.0] | 0.81 | |
| Duration of dialysis [min], mean [SD; Me] | 223.85 [20.47; 240.0] | 216.52 [28.92; 210.0] | 0.11 | |
| Concomitant diseases | ||||
| Diabetes, n (%) | 5 (14.71%) | 13 (28.89%) | 0.22 | |
| Arterial hypertension, n (%) | 25 (73.53%) | 32 (71.11%) | 0.81 | |
| Epilepsy, n (%) | 4 (12%) | 3 (7%) | 0.69 | |
| Ophthalmic, n (%) | 8 (24%) | 15 (33%) | 0.48 | |
| Neurological, n (%) | 2 (6%) | 3 (7%) | 0.75 | |
| Treatment with another renal replacement therapy (peritoneal dialysis/kidney transplant) before starting hemodialysis treatment, n (%) | 7 (20.59%) | 8 (17.78%) | 0.98 | |
| Study Group (n = 39) | Control Group (n = 46) | p | |||||
|---|---|---|---|---|---|---|---|
| Mean | Me | SD | Mean | Me | SD | ||
| Laboratory results | |||||||
| IL-6 Measurement 1 | 187.83 | 143.46 | 146.86 | 197.53 | 150.44 | 127.66 | 0.35 |
| IL-6 Measurement 2 | 143.49 | 131.17 | 65.09 | 250.54 | 159.75 | 255.98 | 0.04 * |
| SOST Measurement 1 | 17.62 | 6.84 | 18.95 | 16.44 | 8.38 | 18.37 | 0.45 |
| SOST Measurement 2 | 9.56 | 7.56 | 6.53 | 17.58 | 9.99 | 16.15 | 0.03 * |
| Study Group (n = 39) | Control Group (n = 46) | p | ||
|---|---|---|---|---|
| Measurement 1 | ||||
| Physical activity MET min. week mean [SD; Me] | 1734.99 [1616.7; 1254.8] | 1354.62 [1457.5; 706.5] | 0.16 | |
| Level of physical activity MET, n (%) | insufficient | 6 (15.79%) | 17 (36.96%) | 0.08 |
| adequate | 24 (63.16%) | 23 (50.00%) | ||
| high | 8 (21.05%) | 6 (13.04%) | ||
| Measurement 2 | ||||
| Physical activity MET min. week mean [SD; Me] | 2358.62 [2150.6; 1392.8] | 1174.4 [1311.2; 693.0] | <0.001 * | |
| Level of physical activity MET, n (%) | insufficient | 3 (8.82%) | 19 (42.22%) | 0.003 * |
| adequate | 23 (67.65%) | 22 (48.89%) | ||
| high | 8 (23.53%) | 4 (8.89%) | ||
| Study Group (n = 39) | Control Group (n = 46) | p | |||||
|---|---|---|---|---|---|---|---|
| Mean | Me | SD | Mean | Me | SD | ||
| 6MWT 1 [m] | 406.90 | 422.50 | 107.55 | 372.04 | 360.00 | 118.54 | 0.31 |
| 6MWT 2 [m] | 432.72 | 430.00 | 100.57 | 364.04 | 340.00 | 118.64 | 0.04 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turoń-Skrzypińska, A.; Mińko, A.; Rył, A.; Mańkowska, K.; Ciechanowski, K.; Bereda, Z.; Rotter, I.; Dutkiewicz, G. Impact of Effectiveness of Physical Activity in a Virtual Environment on the Regulation of Sclerostin and Interleukin 6 Levels in Haemodialysis Patients. J. Clin. Med. 2024, 13, 2321. https://doi.org/10.3390/jcm13082321
Turoń-Skrzypińska A, Mińko A, Rył A, Mańkowska K, Ciechanowski K, Bereda Z, Rotter I, Dutkiewicz G. Impact of Effectiveness of Physical Activity in a Virtual Environment on the Regulation of Sclerostin and Interleukin 6 Levels in Haemodialysis Patients. Journal of Clinical Medicine. 2024; 13(8):2321. https://doi.org/10.3390/jcm13082321
Chicago/Turabian StyleTuroń-Skrzypińska, Agnieszka, Alicja Mińko, Aleksandra Rył, Katarzyna Mańkowska, Kazimierz Ciechanowski, Zuzanna Bereda, Iwona Rotter, and Grażyna Dutkiewicz. 2024. "Impact of Effectiveness of Physical Activity in a Virtual Environment on the Regulation of Sclerostin and Interleukin 6 Levels in Haemodialysis Patients" Journal of Clinical Medicine 13, no. 8: 2321. https://doi.org/10.3390/jcm13082321
APA StyleTuroń-Skrzypińska, A., Mińko, A., Rył, A., Mańkowska, K., Ciechanowski, K., Bereda, Z., Rotter, I., & Dutkiewicz, G. (2024). Impact of Effectiveness of Physical Activity in a Virtual Environment on the Regulation of Sclerostin and Interleukin 6 Levels in Haemodialysis Patients. Journal of Clinical Medicine, 13(8), 2321. https://doi.org/10.3390/jcm13082321