
Positive Emotions in Family Caregivers of Alzheimer’s Disease Patients: Factors Associated with Gain in Caregiving from a Gender Perspective


Abstract
1. Introduction
Gain in Caregiving
2. Materials and Methods
2.1. Participants, Design, and Procedure
2.2. Measures
2.2.1. Psychological Distress
2.2.2. Burden
2.2.3. Gain
2.2.4. Sociodemographic Variables, Objective Burden, and Perceived Physical Health
2.3. Statistical Analysis
3. Results
3.1. Gender Differences
3.2. Correlational Analysis
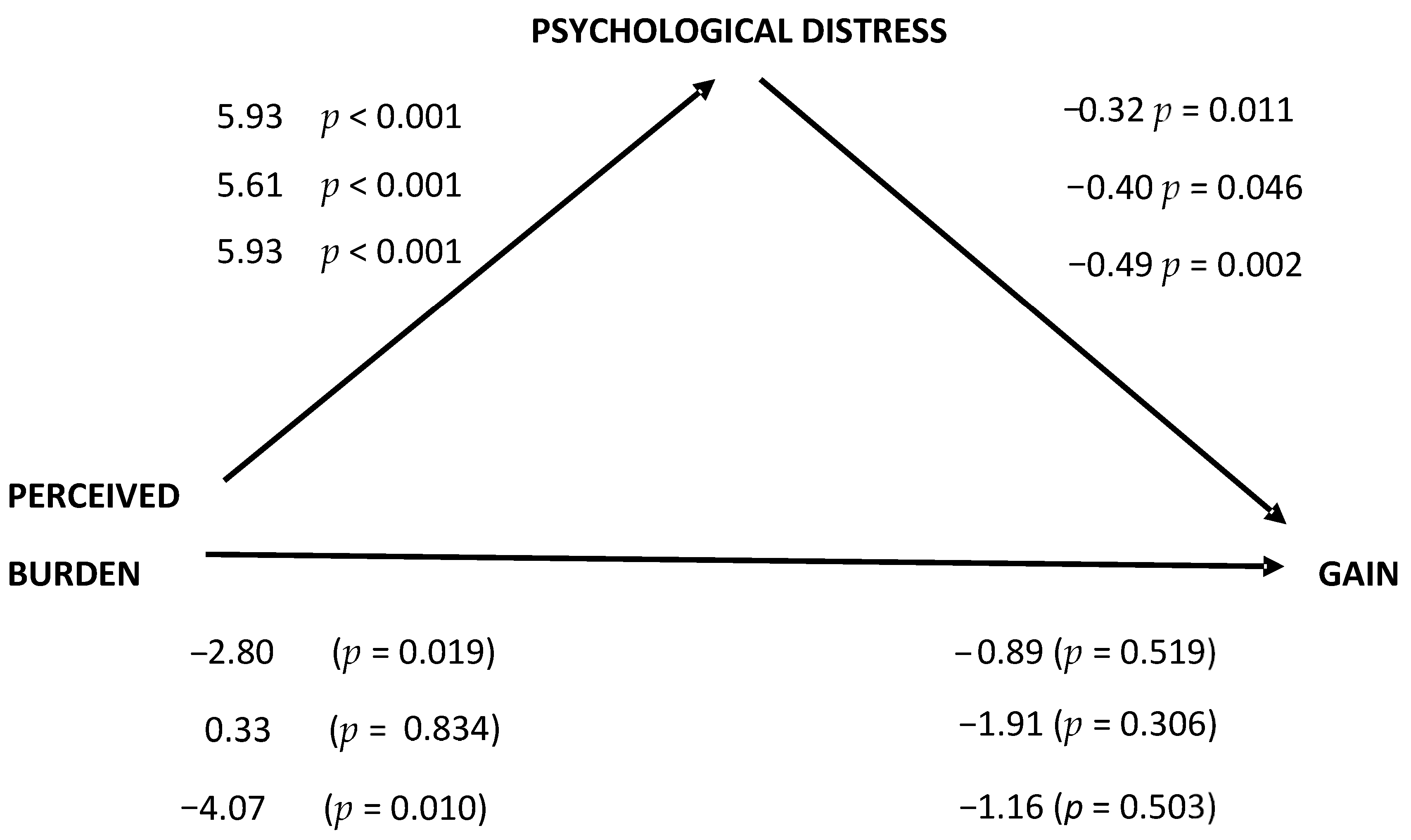
3.3. Mediational Analysis
3.4. Comparison of Studies and Gender Differences in the GAIN Scale Responses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Dementia; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- INE (Instituto Nacional de Estadística). Encuesta de Discapacidad, Autonomía Personal y Situaciones de Dependencia [Survey on Disability, Personal Autonomy and Dependency Situations]; EDAD 2020; Spanish Government: Madrid, Spain, 2022; Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176782&menu=resultados&idp=1254735573175#!tabs-1254736195764 (accessed on 10 February 2024).
- Alzheimer Association. Stages of Alzheimer. Available online: https://www.alz.org/alzheimers-dementia/stages (accessed on 2 February 2024).
- Frank, J.B. Evidence for Grief as the Major Barrier Faced by Alzheimer Caregivers: A Qualitative Analysis. Am. J. Alzheimer’s Dis. Other Dement. 2008, 22, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Civiriain-San Miguel, L.; Moré-Rubio, B. Systematic review of the profile of Alzheimer’s family caregivers over the last ten years. Portales Médicos 2021, 16, 161. [Google Scholar]
- Akpinar, B.; Küçükgüçlü, Ö.; Yener, G. Effects of gender on burden among caregivers of Alzheimer’s patients. J. Nurs. Scholarsh. 2011, 3, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Biscardi, M.; Astell, A.; Nalder, E.; Cameron, J.I.; Mihailidis, A.; Colantonio, A. Sex and gender differences in caregiving burden experienced by family caregivers of persons with dementia: A systematic review. PLoS ONE 2020, 15, e0231848. [Google Scholar] [CrossRef] [PubMed]
- Pöysti, M.M.; Laakkonen, M.L.; Strandberg, T.; Savikko, M.; Tilvis, R.S.; Eloniemi-Sulkava, U.; Pitkälä, K.H. Gender differences in dementia spousal caregiving. Int. J. Alzheimers Dis. 2012, 2012, 162960. [Google Scholar] [CrossRef] [PubMed]
- Sallim, A.S.; Sayampanathan, A.A.; Cuttilan, A.; Ho, R.C.M. Prevalence of mental health disorders among caregivers of patients with Alzheimer disease. JAMDA 2015, 16, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Donkin, M. Family caregivers of people with dementia. Dial. Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.; Wright, J.; Oyebode, J.; Job, D.; Crome, P.; Bentham, P.; Jones, L.; Lendon, C. Determinants of burden in those who care for someone with dementia. Int. J. Geriatr. Psychiatry 2008, 23, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Gender differences in caregiver stressors, social resources, and health: An updated meta-analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Díaz, A.; Ponsoda, J.M.; Beleña, A. Optimism as a key to improving mental health in family caregivers of people living with Alzheimer’s disease. Aging Ment. Health 2020, 24, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Carbonneau, H.; Caron, C.; Desrosiers, J. Development of a conceptual framework of positive aspects of caregiving in dementia. Dementia 2010, 9, 327–353. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Folkman, S. Positive psychological states and coping with severe stress. Soc. Sci. Med. 1997, 45, 1207–1221. [Google Scholar] [CrossRef] [PubMed]
- Tennen, H.; Affleck, G. Benefit-finding and benefit-reminding. In Handbook of Positive Psychology; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Fredrickson, B.L. The broaden-and-build theory of positive emotions. Philos. Trans. R. Soc. B Biol. 2004, 359, 1367–1378. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L.; Tugade, M.M.; Waugh, C.E.; Larkin, G.R. What good are positive emotions in crises? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J. Pers. Soc. Psychol. 2003, 84, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Kramer, B.J. Gain in the caregiving experience: Where are we? What next? Gerontologist 1997, 37, 218–232. [Google Scholar] [CrossRef] [PubMed]
- Rapp, S.R.; Chao, D. Appraisals of strain and of gain: Effects on psychological wellbeing of caregivers of dementia patients. Aging Ment. Health 2000, 4, 142–147. [Google Scholar] [CrossRef]
- Sanders, S. Is the glass half empty or half full? Reflections on strain and gain in caregivers of individuals with Alzheimer’s disease. Soc. Work Health Care 2005, 40, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Netto, N.R.; Jenny, G.Y.N.; Philip, Y.L.K. Growing and gaining through caring for a loved one with dementia. Dementia 2009, 8, 245–261. [Google Scholar] [CrossRef]
- Yap, P.; Luo, N.; Ng, W.Y.; Chionh, H.L.; Lim, J.; Goh, J. Gain in Alzheimer care Instrument—A new scale to measure caregiving gains in dementia. Am. J. Geriatr. Psychiatry 2010, 18, 68–76. [Google Scholar] [CrossRef]
- Picot, S.J. Rewards, costs, and coping of African American caregivers. Nurs. Res. 1995, 44, 147–152. [Google Scholar] [CrossRef]
- García-Castro, F.J.; Hernández, A.; Blanca, M.J. Life satisfaction and the mediating role of character strengths and gains in informal caregivers. J. Psychiatr. Ment. Health Nurs. 2021, 29, 829–841. [Google Scholar] [CrossRef] [PubMed]
- García-Castro, J.; Holgado-Tello, F.P.; Blanca, M.J. New evidence for the psychometric properties of the Spanish Version of the Gain in Alzheimer Care Instrument. Span. J. Psychol. 2021, 24, e32. [Google Scholar] [CrossRef] [PubMed]
- Liew, T.M.; Luo, N.; Ng, W.Y.; Chionh, H.L.; Goh, J.; Yap, P. Predicting gains in dementia caregiving. Dement. Geriatr. Cogn. Disord. 2010, 29, 115–122. [Google Scholar] [CrossRef]
- Tew, C.W.; Tan, L.F.; Luo, N.; Ng, W.Y.; Yap, P. Why family caregivers choose to institutionalize a loved one with dementia: A Singapore perspective. Dement. Geriatr. Cogn. Disord. 2010, 30, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Parveen, S.; Morrison, V. Predicting caregiver gains: A longitudinal study. Br. J. Health Psychol. 2012, 17, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Fabà, J.; Villar, F. Ganancias asociadas al cuidado de personas con demencia: Adaptación al español de la escala GAIN [Gains associated with caring for people with dementia: A Spanish adaptation of the GAIN]. Rev. Esp. Geriatr. Gerontol. 2013, 48, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Picot, S.J.; Debanne, S.M.; NamazI, K.H.; Wykle, M.L. Religiosity and perceived rewards of black and white caregivers. Gerontologist 1997, 37, 89–101. [Google Scholar] [CrossRef]
- Swinkels, J.C.; Broese, M.I.; de Boer, A.; Tilburg, T.G.V. Male and female partner-caregivers burden: Does it get worse over time? Gerontologist 2019, 59, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Mathias, K.; Kermode, M.; San Sebastian, M.; Davar, B.; Goicolea, I. An asymmetric burden experiences of men women as caregivers of people with psychosocial disabilities in rural North India. Transcult. Psychiatry 2019, 56, 76–102. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.B. Alzheimer’s disease caregiver burden: Does resilience matter? J. Hum. Behav. Soc. Environ. 2013, 23, 879–892. [Google Scholar] [CrossRef]
- Takano, M.; Arai, H. Gender differences and caregivers’ burden in early-onset Alzheimer disease. Psychogeriatrics 2005, 5, 73–77. [Google Scholar] [CrossRef]
- Feldman, H.H.; Woodward, M. The staging and assessment of moderate to severe Alzheimer disease. Neurology 2005, 65 (6_suppl_3), S10–S17. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Cifre, E.; Salanova, M. Validación factorial de “General Health Questionnaire” (GHQ-12) mediante un análisis factorial confirmatorio [Factor validation of “General Health Questionnaire” (GHQ-12) through a confirmatory factor analysis]. J. Health Psychol. 2000, 12, 75–89. [Google Scholar]
- Zarit, S.H.; Zarit, J.M. The Memory and Behavior Problems Checklist and the Burden Interview; Technical Report; Pennsylvania State University: State College, PA, USA, 1987. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 3rd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Wong, D.F.K.; Ng, T.K.; Zhuang, X.Y. Caregiving burden and psychological distress in Chinese spousal caregivers: Gender difference in the moderating role of positive aspects of caregiving. Aging Ment. Health 2019, 23, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Gratao, A.C.M.; Vale, F.D.; Roriz-Cruz, M.; Haas, V.J.; Lange, C.; Talmelli, L.F.; Rodrigues, R.A. The demands of family caregivers of elderly individuals with dementia. Rev. Esc. Enferm. USP 2010, 44, 873–880. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
| Male | Female | ||||
|---|---|---|---|---|---|
| Variables | n | % | n | % | χ2-Value (p) |
| Education level | 2.25 (0.522) | ||||
| No studies | 3 | 6.8 | 3 | 3.1 | |
| Primary | 18 | 40.9 | 45 | 46.9 | |
| Secondary | 18 | 40.9 | 32 | 33.3 | |
| University | 5 | 11.4 | 16 | 16.7 | |
| Marital Status | 0.30 (0.587) | ||||
| Single/separated/widow | 8 | 14.6 | 14 | 14.6 | |
| Married | 36 | 85.4 | 82 | 85.4 | |
| Hours/day caring | 2.18 (0.535) | ||||
| <5 h | 7 | 15.9 | 19 | 19.8 | |
| 5–10 h | 8 | 18.2 | 26 | 27.1 | |
| 11–15 h | 6 | 13.6 | 12 | 12.5 | |
| >15 h | 23 | 52.3 | 39 | 40.6 | |
| Perceived physical health | 6.87 (0.143) | ||||
| Very bad | 0 | 0.0 | 1 | 1.0 | |
| Bad | 2 | 4.5 | 4 | 4.2 | |
| Medium | 9 | 20.5 | 37 | 38.5 | |
| Good | 31 | 70.7 | 46 | 47.9 | |
| Very good | 2 | 4.5 | 8 | 8.3 | |
| Relation with the AD patient | 3.98 (0.552) | ||||
| Espouse | 11 | 25.0 | 13 | 13.5 | |
| Daughter/son | 28 | 63.6 | 67 | 69.8 | |
| Daughter/son-in-law | 3 | 6.8 | 10 | 10.4 | |
| Grandchild | 1 | 2.3 | 4 | 4.2 | |
| Nephew/niece | 1 | 2.3 | 2 | 2.0 | |
| AD phase of the patient | 0.25 (0.883) | ||||
| Mild | 14 | 31.8 | 28 | 29.2 | |
| Moderate | 20 | 45.5 | 48 | 50.0 | |
| Severe | 10 | 22.7 | 20 | 20.8 | |
| Male (n = 44) | Female (n = 96) | ||||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | d | |
| Age | 58.81 | 13.90 | 54.55 | 10.95 | 1.80 | 0.077 | --- |
| Months caring | 49.43 | 31.72 | 52.48 | 36.56 | 0.48 | 0.634 | --- |
| Perceived burden | 50.25 | 10.53 | 52.10 | 13.03 | −0.83 | 0.409 | --- |
| Psychological Distress | 13.34 | 4.79 | 15.46 | 5.75 | −2.13 | 0.035 | 0.54 |
| Gain | 32.02 | 5.04 | 29.99 | 7.84 | −1.84 | 0.067 | --- |
| Variables | Whole Sample | Male | Female | |
|---|---|---|---|---|
| Pearson’s r (p) | Age | −0.05 (0.534) | 0.17 (0.274) | 0.17 (0.094) |
| Months caring | 0.14 (0.111) | 0.37 (0.013) | 0.09 (0.410) | |
| Burden | −0.24 (0.005) | 0.10 (0.658) | −0.30 (0.003) | |
| Psychological distress | −0.28 (<0.001) | 0.27 (0.081) | −0.40 (<0.001) | |
| Spearman’s Rho (p) | Studies | −0.06 (0.473) | −0.28 (0.069) | 0.03 (0.775) |
| Marital status | −0.03 (0.749) | −0.30 (0.049) | 0.08 (0.420) | |
| Hours/day caring | 0.10 (0.248) | 0.32 (0.035) | 0.07 (0.964) | |
| Perceived Physical Health | 0.00 (0.962) | −0.25 (0.090) | 0.10 (0.518) | |
| Relation with the AD patient | 0.02 (0.815) | −0.10 (0.534) | 0.07 (0.346) | |
| AD phase of the patient | 0.19 (0.023) | 0.16 (0.301) | 0.23 (0.025) |
| Point Estimate | Standard Error | Bootstrapping 95% Confidence Interval | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Whole sample | −1.91 | 0.94 | −3.84 | −0.12 |
| Female | −2.91 | 1.12 | −5.27 | −0.82 |
| Male | 2.23 | 1.56 | 0.19 | 6.24 |
| Disagree a Lot Score 0 | Disagree a Little Score 1 | Neither Agree Nor Disagree Score 2 | Agree a Little Score 3 | Agree a Lot Score 4 | Mean Item Score | |
|---|---|---|---|---|---|---|
| 1. … be more patient and understanding… | 6.4 | 2.9 | 8.6 | 32.1 | 50 | 3.16 |
| 2. … stronger and more resilient… | 2.1 | 6.4 | 13.6 | 32.9 | 45.0 | 3.12 |
| 3. … more aware of myself… | 0.7 | 5.0 | 20.7 | 35.0 | 38.6 | 3.06 |
| 4. … knowledge and skills in dementia… | 0.7 | 4.3 | 10.7 | 29.3 | 55.0 | 3.34 |
| 5. … grow closer to my relative… | 2.1 | 5.0 | 11.4 | 22.1 | 59.3 | 3.31 |
| 6. … bond my family closer… | 2.9 | 9.3 | 25.0 | 30.0 | 32.9 | 2.81 |
| 7. … better relation to dementia and olders… | 2.9 | 4.3 | 19.3 | 28.6 | 45.0 | 3.09 |
| 8. … insight into the meaning of life… | 2.1 | 4.3 | 14.3 | 30.7 | 48.6 | 3.19 |
| 9. … grow spiritually… | 13.6 | 10.0 | 20.0 | 27.9 | 28.6 | 3.48 |
| 10. … altruistic goals… | 1.4 | 2.9 | 22.1 | 34.3 | 39.3 | 3.07 |
| Gain Scores | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0–19 | 20–30 | 31–40 | |||||||
| n | % | n | % | n | % | χ2-Value | p | ||
| Gender | 9.19 | 0.010 | |||||||
| Male | 0 | 0.0 | 11 | 25 | 33 | 75 | |||
| Female | 12 | 12.5 | 34 | 35.4 | 50 | 52.1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponsoda, J.M.; Díaz, A. Positive Emotions in Family Caregivers of Alzheimer’s Disease Patients: Factors Associated with Gain in Caregiving from a Gender Perspective. J. Clin. Med. 2024, 13, 2322. https://doi.org/10.3390/jcm13082322
Ponsoda JM, Díaz A. Positive Emotions in Family Caregivers of Alzheimer’s Disease Patients: Factors Associated with Gain in Caregiving from a Gender Perspective. Journal of Clinical Medicine. 2024; 13(8):2322. https://doi.org/10.3390/jcm13082322
Chicago/Turabian StylePonsoda, José Manuel, and Amelia Díaz. 2024. "Positive Emotions in Family Caregivers of Alzheimer’s Disease Patients: Factors Associated with Gain in Caregiving from a Gender Perspective" Journal of Clinical Medicine 13, no. 8: 2322. https://doi.org/10.3390/jcm13082322
APA StylePonsoda, J. M., & Díaz, A. (2024). Positive Emotions in Family Caregivers of Alzheimer’s Disease Patients: Factors Associated with Gain in Caregiving from a Gender Perspective. Journal of Clinical Medicine, 13(8), 2322. https://doi.org/10.3390/jcm13082322