
A Psychometric Evaluation of the Dysphagia Handicap Index Using Rasch Analysis

Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item # | Domain | Item Description |
|---|---|---|
| 1 | 1P | I cough when I drink liquids. |
| 2 | 2P | I cough when I eat solid food. |
| 3 | 3P | My mouth is dry. |
| 4 | 4P | I need to drink fluids to wash food down. |
| 5 | 5P | I’ve lost weight because of my swallowing problem. |
| 6 | 1F | I avoid some foods because of my swallowing problem. |
| 7 | 2F | I have changed the way I swallow to make it easier to eat. |
| 8 | 1E | I am embarrassed to eat in public. |
| 9 | 3F | It takes me longer to eat a meal than it used to. |
| 10 | 4F | I eat smaller meals more often due to my swallowing problem. |
| 11 | 6P | I have to swallow again before food will go down. |
| 12 | 2E | I feel depressed because I cannot eat what I want. |
| 13 | 3E | I do not enjoy eating as much as I used to. |
| 14 | 5F | I do not socialise as much due to my swallowing problem. |
| 15 | 6F | I avoid eating because of my swallowing problem. |
| 16 | 7F | I eat less because of my swallowing problem. |
| 17 | 4E | I am nervous because of my swallowing problem. |
| 18 | 5E | I feel handicapped because of my swallowing problem. |
| 19 | 6E | I get angry at myself because of my swallowing problem. |
| 20 | 7P | I choke when I take my medication. |
| 21 | 7E | I am afraid that I will choke and stop breathing because of my swallowing problem. |
| 22 | 8F | I must eat another way (e.g., feeding tube) because of my swallowing problem. |
| 23 | 9F | I’ve changed my diet due to my swallowing problem. |
| 24 | 8P | I feel a strangling sensation when I swallow. |
| 25 | 9P | I cough up food after I swallow. |
2. Methods
2.1. Participants and Procedure
2.2. Instrument
2.3. Statistical Analysis
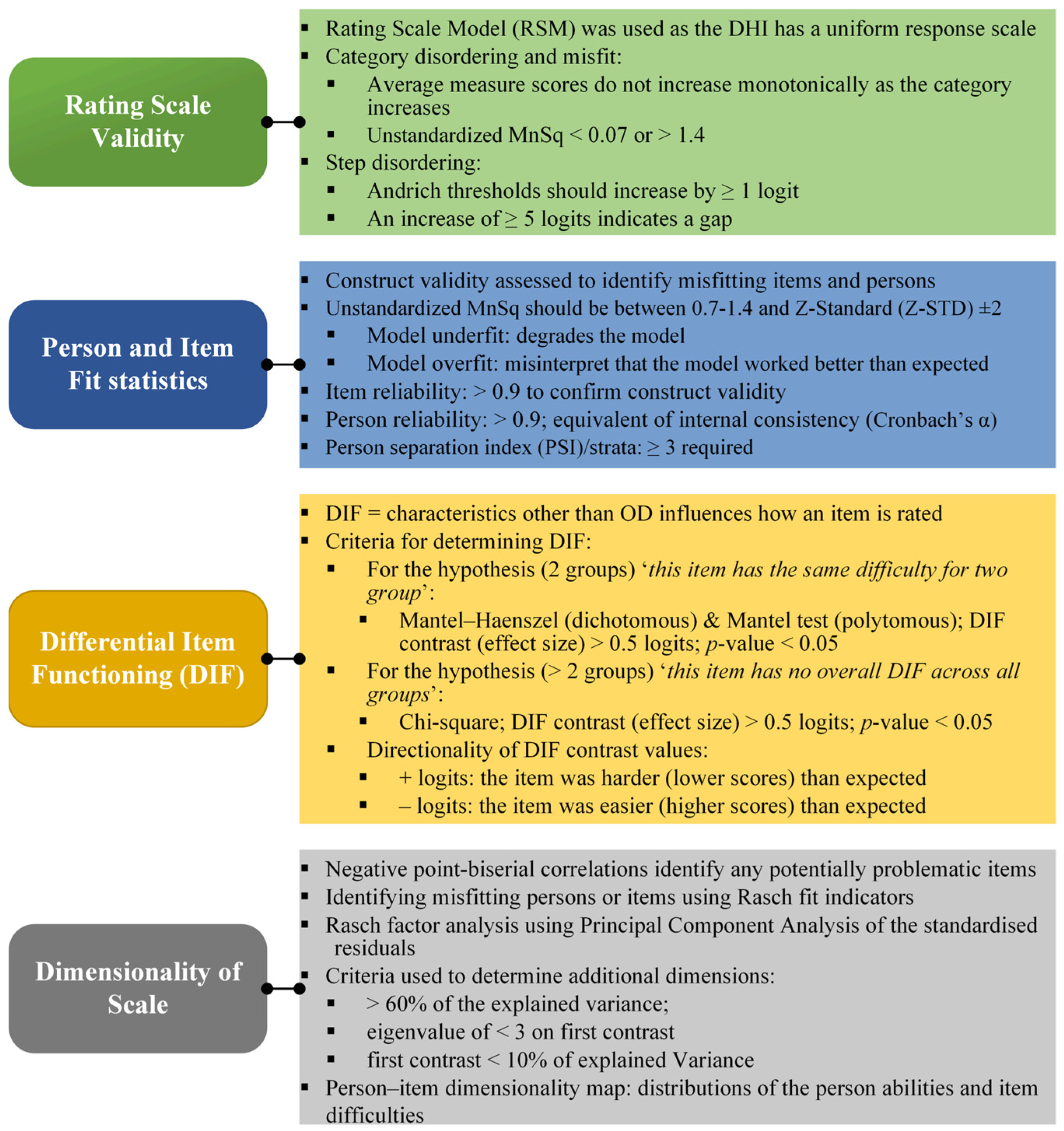
2.4. Rating Scale Validity
2.5. Person and Item Fit Statistics
2.6. Differential Item Analysis
2.7. Dimensionality of the Scale
3. Results
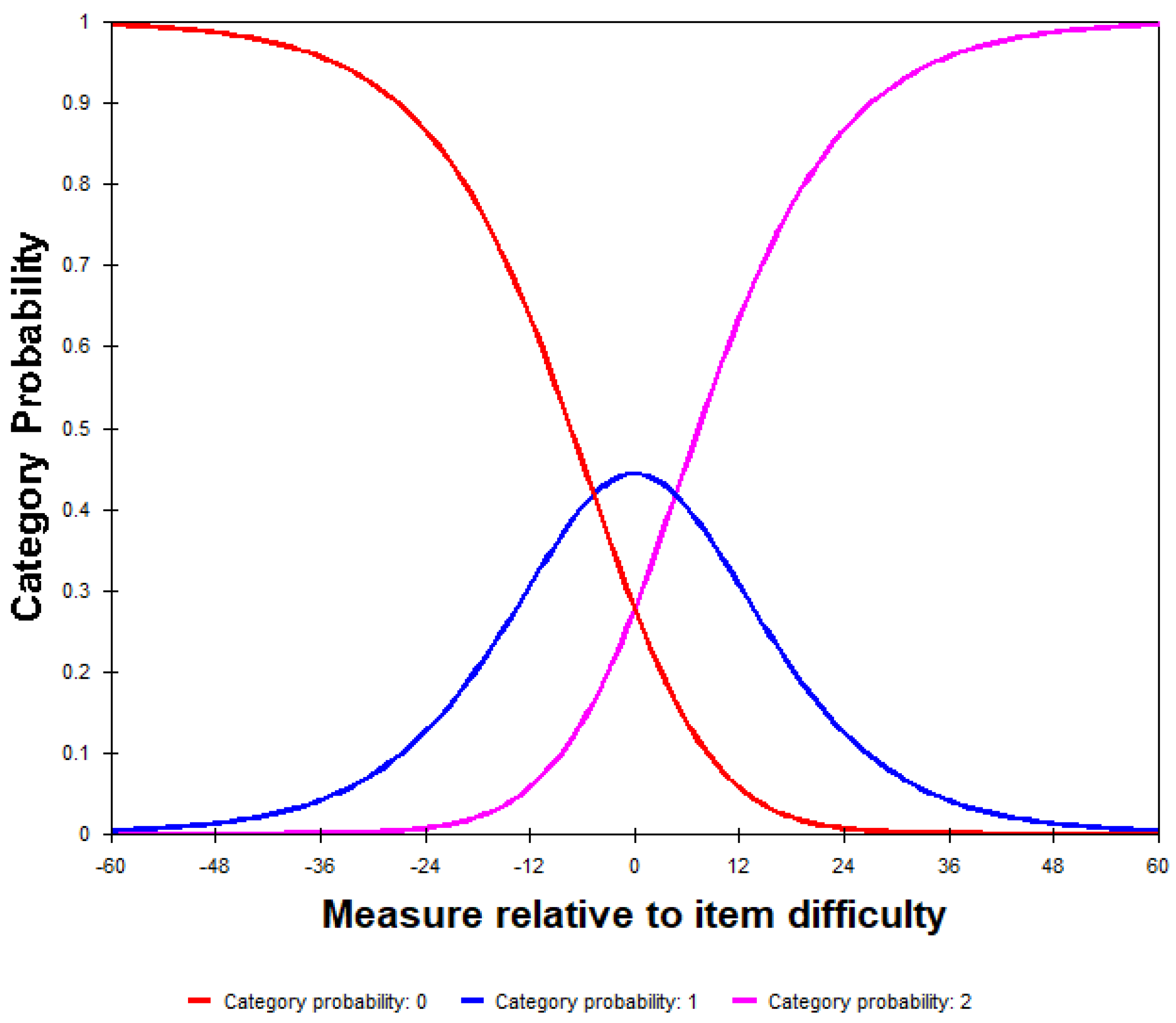
3.1. Rating Scale Validity
Category Order
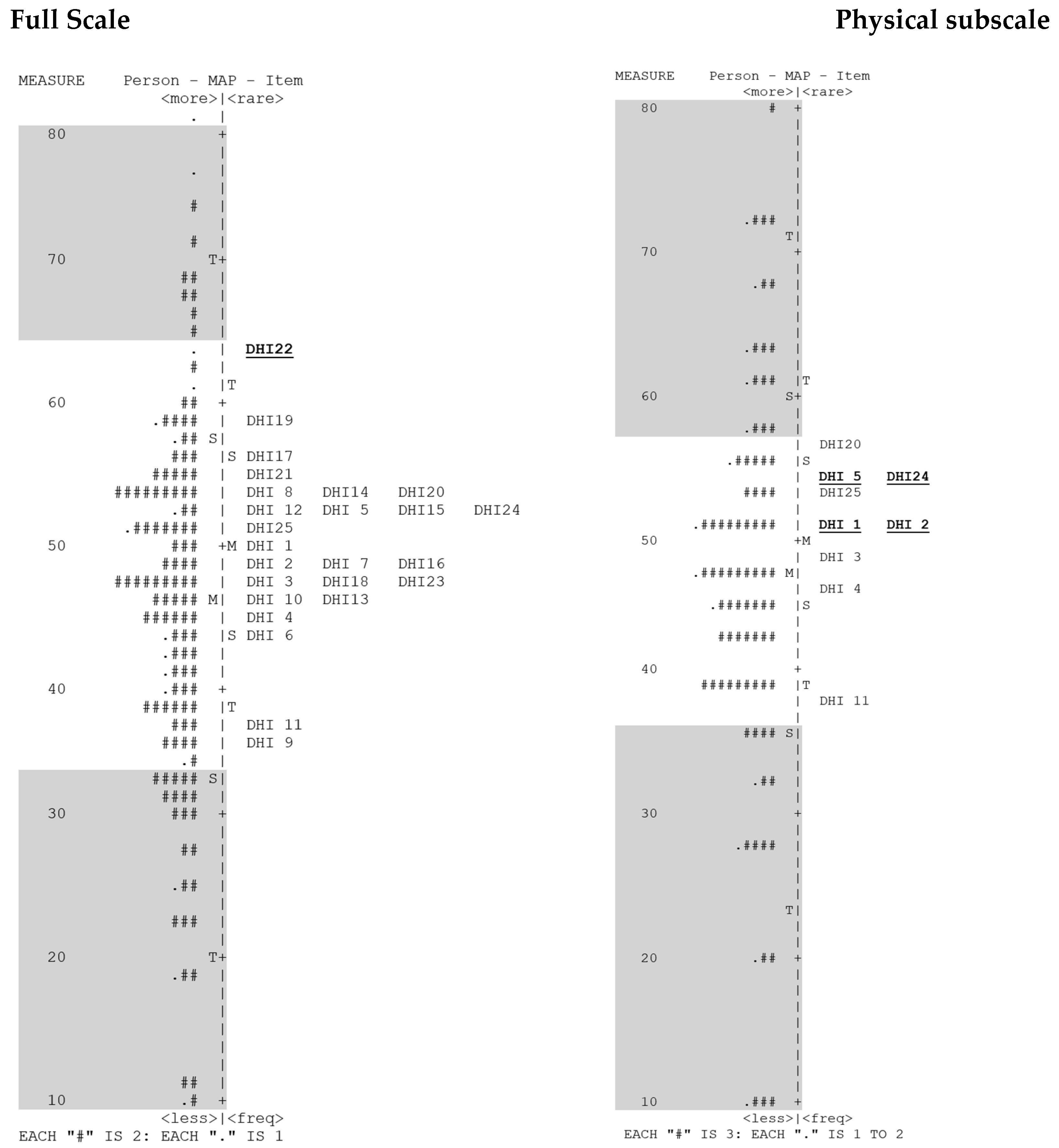
3.2. Person and Item Fit
3.2.1. Physical Subscale
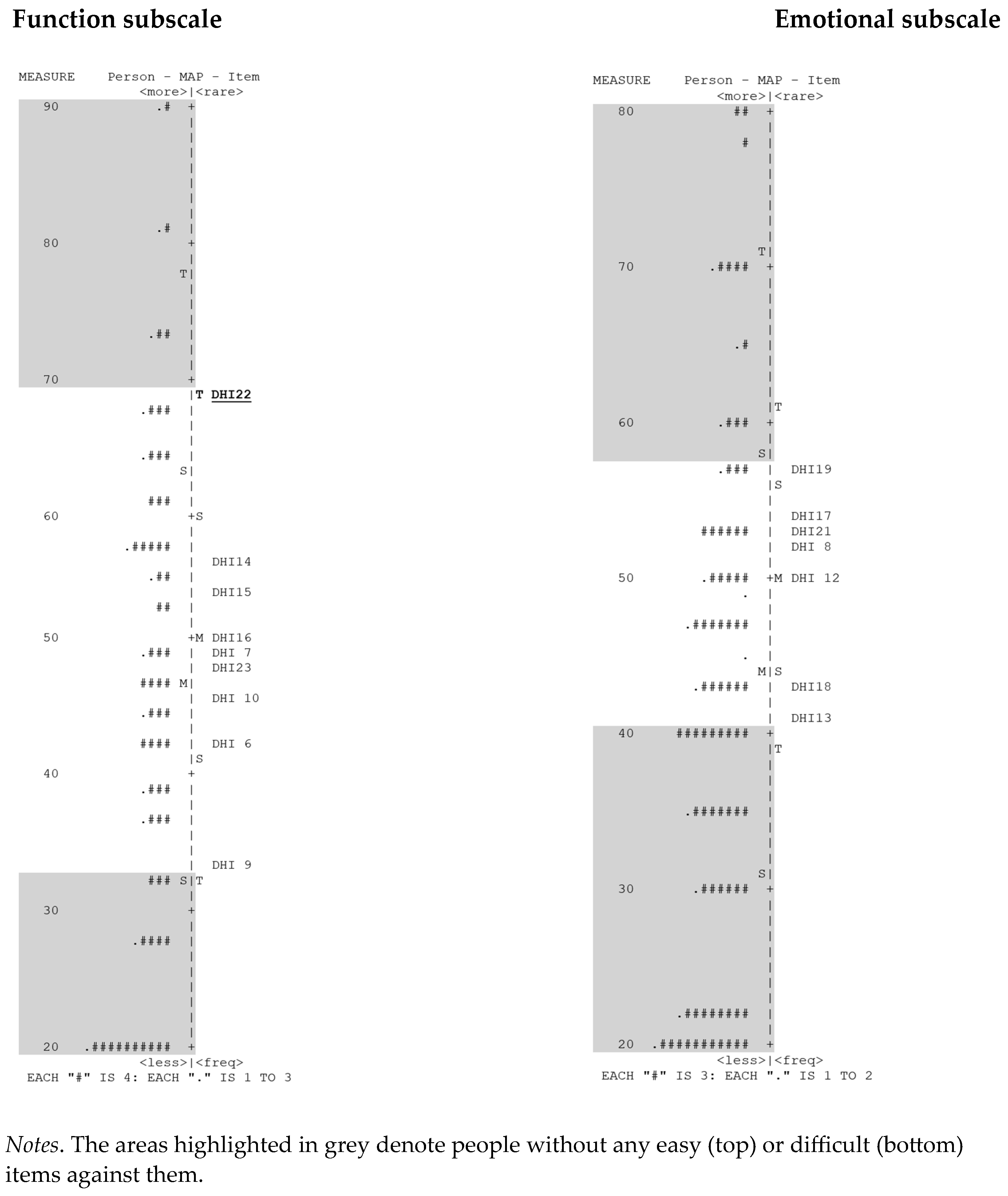
3.2.2. Functional Subscale
3.2.3. Emotional Subscale
3.3. Differential Item Functioning
3.4. Dimensionality
4. Discussion
4.1. Summary Statistics
4.2. Rating Scale
4.3. Person and Item Fit
4.4. Differential Item Functioning
4.5. Dimensionality
4.6. Future Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viñas, P.; Martín-Martínez, A.; Cera, M.; Riera, S.A.; Escobar, R.; Clavé, P.; Ortega, O. Characteristics and Therapeutic Needs of Older Patients with Oropharyngeal Dysphagia Admitted to a General Hospital. J. Nutr. Health Aging 2023, 27, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Rajati, F.; Ahmadi, N.; Naghibzadeh, Z.A.S.; Kazeminia, M. The global prevalence of oropharyngeal dysphagia in different populations: A systematic review and meta-analysis. J. Transl. Med. 2022, 20, 175. [Google Scholar] [CrossRef] [PubMed]
- Pacheco-Castilho, A.C.; Miranda, R.P.C.; Norberto, A.M.Q.; Favoretto, D.B.; Rimoli, B.P.; Alves, L.B.d.M.; Weber, K.T.; Santos, T.E.G.; Moriguti, J.C.; Leite, J.P.; et al. Dysphagia is a strong predictor of death and functional dependence at three months post-stroke. Arq. Neuro-Psiquiatr. 2022, 80, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Balaguer, M.; Cugy, E.; Devoucoux, C.; Morinière, S.; Soriano, G.; Vérin, E.; Woisard, V. Expert consensus on clinical decision-making in the disease trajectory of oropharyngeal dysphagia in adults: An international Delphi study. J. Clin. Med. 2023, 12, 6572. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Speyer, R.; Kertscher, B.; Swan, K.; Wagg, B.; Cordier, R. Health-related quality of life in oropharyngeal dysphagia. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef] [PubMed]
- Swan, K.; Speyer, R.; Heijnen, B.J.; Wagg, B.; Cordier, R. Living with oropharyngeal dysphagia: Effects of bolus modification on health-related quality of life—A systematic review. Qual. Life Res. 2015, 24, 2447–2456. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Cordier, R.; Denman, D.; Windsor, C.; Krisciunas, G.P.; Smithard, D.G.; Heijnen, B.J. Development of two patient self-reported measures on functional health status (FOD) and health-related quality of life (QOD) in adults with oropharyngeal dysphagia using the Delphi technique. J. Clin. Med. 2022, 11, 5920. [Google Scholar] [CrossRef]
- Speyer, R.; Cordier, R.; Farneti, F.; Nascimento, W.; Pilz, W.; Verin, E.; Walshe, M.; Woisard, V. White paper by the European society for Swallowing Disorders: Screening and non-instrumental assessment for dysphagia in adults. Dysphagia 2022, 37, 333–349. [Google Scholar] [CrossRef]
- Ferrans, C.E.; Zerwic, J.J.; Wilbur, J.E.; Larson, J.L. Conceptual Model of Health-Related Quality of Life. J. Nurs. Sch. 2005, 37, 336–342. [Google Scholar] [CrossRef]
- Cordier, R.; Joosten, A.; Clavé, P.; Schindler, A.; Bülow, M.; Demir, N.; Serel Arslan, S.; Speyer, R. Evaluating the psychometric properties of the Eating Assessment Tool (EAT-10) using Rasch analysis. Dysphagia 2017, 32, 250–260. [Google Scholar] [CrossRef]
- Swan, K.; Speyer, R.; Scharitzer, M.; Farneti, D.; Brown, T.; Woisard, V.; Cordier, R. Measuring What Matters in Healthcare: A Practical Guide to Psychometric Principles and Instrument Development. Front. Psychol. 2023, 18, 1225850. [Google Scholar] [CrossRef] [PubMed]
- Prinsen, C.A.; Vohra, S.; Rose, M.R.; Boers, M.; Tugwell, P.; Williamson, P.R.; Terwee, C.B. How to select outcome measurement instruments for outcomes included in a “Core Outcome Set”—A practical guideline. Trials 2016, 13, 449. [Google Scholar] [CrossRef] [PubMed]
- Speyer, R.; Kim, J.-H.; Doma, K.; Chen, Y.-W.; Denman, D.; Phyland, D.; Parsons, L.; Cordier, R. Measurement properties of self-report questionnaires on health-related quality of life and functional health status in dysphonia: A systematic review using the COSMIN taxonomy. Qual. Life Res. 2019, 28, 283–296. [Google Scholar] [CrossRef]
- Timmerman, A.A.; Speyer, R.; Heijnen, B.J.; Klijn-Zwijnenberg, I.R. Psychometric characteristics of health-related quality-of-life questionnaires in oropharyngeal dysphagia. Dysphagia 2014, 29, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Cordier, R.; Speyer, R.; Schindler, A.; Hamdy, S.; Michou, E.; Heijnen, B.J.; Baijens, L.W.J.; Karaduman, A.; Swan, K.; Clave, P.; et al. Using Rasch analysis to evaluate the reliability and validity of the Swallowing Quality of Life questionnaire: An item response theory approach. Dysphagia 2018, 33, 441–456. [Google Scholar] [CrossRef] [PubMed]
- Cordier, R.; Speyer, R.; Martinez, M.; Parsons, L. Non-instrumental clinical assessments in oropharyngeal dysphagia: A systematic review on validity and reliability. J. Clin. Med. 2023, 12, 721. [Google Scholar] [CrossRef] [PubMed]
- Swan, K.; Speyer, R.; Brown, T.; Cordier, R. Psychometric properties of visuoperceptual measures of videofluoroscopic and fibre-endoscopic evaluations of swallowing: A systematic review. Dysphagia 2019, 34, 2–33. [Google Scholar] [CrossRef] [PubMed]
- Cappelleri, J.C.; Jason Lundy, J.; Hays, R.D. Overview of classical test theory and item response theory for the quantitative assessment of items in developing patient-reported outcomes measures. Clin. Ther. 2014, 36, 648–662. [Google Scholar] [CrossRef]
- Linacre, J.M. A User’s Guide to Winsteps Raschmodel Computer Programs: Program Manual 3.92.0; Mesa-Press: Chicago, IL, USA, 2016. [Google Scholar]
- Kean, J.; Bisson, E.F.; Brodke, D.S.; Biber, J.; Gross, P.H. An introduction to item response theory and Rasch analysis: Application using the eating assessment tool (EAT-10). Brain Impair. 2018, 19, 91–102. [Google Scholar] [CrossRef]
- Chen, A.Y.; Frankowski, R.; Bishop-Leone, J.; Hebert, T.; Leyk, S.; Lewin, J.; Goepfert, H. The development and validation of a dysphagiaspecific quality-of-life questionnaire for patients with head and neck cancer. Arch. Otolaryngol.-Head Neck Surg. 2001, 127, 870–876. [Google Scholar]
- McHorney, C.A.; Robbins, J.; Lomax, K.; Rosenbek, J.C.; Chignell, K.; Kramer, A.E.; Bricker, D.E. The SWAL–QOL and SWAL–CARE outcomes tool for oropharyngeal dysphagia in adults: III. Documentation of reliability and validity. Dysphagia 2002, 17, 97–114. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- Silbergleit, A.K.; Schultz, L.; Jacobson, B.H.; Beardsley, T.; Johnson, A.F. The Dysphagia handicap index: Development and validation. Dysphagia 2012, 27, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.; Kjaersgaard, A. Item analysis of the Eating Assessment Tool (EAT-10) by the Rasch model: A secondary analysis of cross-sectional survey data obtained among community-dwelling elders. Health Qual. Life Outcomes 2020, 18, 139. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; de Fátima Lago Alvite, M.; Robles-Rodriguez, W.G.; Barcons, N.; Clavé, P. History and Science behind the Eating Assessment Tool-10 (Eat-10): Lessons Learned. J. Nutr. Health Aging 2023, 27, 597–606. [Google Scholar] [CrossRef]
- Hazelwood, R.J.; Armeson, K.E.; Hill, E.G.; Bonilha, H.S.; Martin-Harris, B. Relating Physiologic Swallowing Impairment, Functional Swallowing Ability, and Swallow-Specific Quality of Life. Dysphagia 2023, 38, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Silbergleit, A.K.; Schultz, L.; Hamilton, K.; LeWitt, P.A.; Sidiropoulos, C. Self-Perception of Voice and Swallowing Handicap in Parkinson’s Disease. J. Park. Dis. 2021, 11, 2027–2034. [Google Scholar] [CrossRef]
- Ginocchio, D.; Ninfa, A.; Pizzorni, N.; Lunetta, C.; Sansone, V.A.; Schindler, A. Cross-Cultural Adaptation and Validation of the Italian Version of the Dysphagia Handicap Index (I-DHI). Dysphagia 2022, 37, 1120–1136. [Google Scholar] [CrossRef]
- Silva-Carvalho, I.; Martins, A.; Casanova, M.J.; Freitas, S.; Meireles, L. Cross-Cultural Adaptation and Validation of the European Portuguese Dysphagia Handicap Index. Dysphagia 2023, 38, 1072–1079. [Google Scholar] [CrossRef]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Prinsen, C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; De Vet, H.; Terwee, C.B.; Mokkink, L. COSMIN Methodology for Systematic Reviews of Patient-Reported Outcome Measures (PROMs). User Manual. 2018, pp. 1–78. Available online: https://www.cosmin.nl/wp-content/uploads/COSMIN-syst-review-for-PROMs-manual_version-1_feb-2018-1.pdf (accessed on 1 April 2024).
- Linacre, J.M. Winsteps® Rasch Measurement Computer Program. 2016. Available online: https://www.winsteps.com/index.htm (accessed on 1 April 2024).
- Wright, B. Rating scale model (RSM) or partial credit model (PCM). Rasch Meas. Trans. 1998, 12, 641–642. [Google Scholar]
- Linacre, J.M. Investigating rating scale category utility. J. Outcome Meas. 1999, 3, 103–122. [Google Scholar] [PubMed]
- Bond, T.; Fox, C. Applying the Rasch Model: Fundamental Measurement in the Human Sciences, 3rd ed.; Routledge: London, UK, 2015. [Google Scholar]
- Dziewas, R.; Allescher, H.-D.; Aroyo, I.; Bartolome, G.; Beilenhoff, U.; Bohlender, J.; Breitbach-Snowdon, H.; Fheodoroff, K.; Glahn, J.; Heppner, H.-J. Diagnosis and treatment of neurogenic dysphagia—S1 guideline of the German Society of Neurology. Neurol. Res. Pract. 2021, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Baijens, W.J.; Walshe, M.; Aaltonen, L.-M.; Arens, C.; Cordier, R.; Cras, P.; Crevier-Buchman, L.; Golusinski, W.; Govender, R.; Grau Eriksen, J.; et al. European Society For Swallowing Disorders—Confederation Of European Otorhinolaryngology Head and Neck Surgery. White Paper: Oropharyngeal dysphagia in head and neck cancer. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 577–616. [Google Scholar] [CrossRef] [PubMed]
- Rudler, F.; Pineton de Chambrun, G.; Lallemant, B.; Garrel, R.; Pouderoux, P.; Ramdani, M.; Caillo, L.; Reynaud, C.; Valats, J.C.; Blanc, P. Management of the Zenker diverticulum: Multicenter retrospective comparative study of open surgery and rigid endoscopy versus flexible endoscopy. Surg. Endosc. 2023, 37, 7064–7072. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Zhou, S.; Hur, K.; Chambers, T.; O’Dell, K.; Johns, M. Disparities in the prevalence of self-reported dysphagia and treatment among U.S. adults. Am. J. Otolaryngol. 2023, 44, 103774. [Google Scholar] [CrossRef]
- Otaka, Y.; Harada, Y.; Shiroto, K.; Morinaga, Y.; Shimizu, T. Early swallowing rehabilitation and promotion of total oral intake in patients with aspiration pneumonia: A retrospective study. PLoS ONE 2024, 19, e0296828. [Google Scholar] [CrossRef]
- Guilera, G.; Gómez-Benito, J.; Hidalgo, M.D.; Sánchez-Meca, J. Type I error and statistical power of the Mantel-Haenszel procedure for detecting DIF: A meta-analysis. Psychol. Methods 2013, 18, 553. [Google Scholar] [CrossRef] [PubMed]
- Linacre, J.M. Detecting multidimensionality: Which residual data-type works best? J. Outcome Meas. 1998, 2, 266–283. [Google Scholar]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; de Vet, H.C.W.; Bouter, L.M.; Alonso, J.; Westerman, M.J.; Patrick, D.L.; Mokkink, L.B. COSMIN Methodology for Assessing the Content Validity of PROMs—User Manual, Version 1.0. COSMIN, Ed.; VU University Medical Center: Amsterdam, The Netherlands, 2018.
- United Nations. Disability Inclusive Language Guidelines; The United Nations Office at Geneva: Geneva, Switzerland, 2019. [Google Scholar]




| Participant Characteristics | Oropharyngeal Dysphagia Group (n = 188) | No Oropharyngeal Dysphagia Group (n = 68) | Combined Groups (N = 256) |
|---|---|---|---|
| Sex: n (%) | |||
| Male | 103 (54.8%) | 33 (48.5%) | 136 (53.1%) |
| Female | 85 (45.2%) | 35 (51.5%) | 120 (46.9%) |
| Age (≥18 years): | |||
| MN (SD) | 66.4 (13.8) | 61.8 (14.8) | 65.2 (14.2) |
| Range | 18–96 | 18–88 | 18–96 |
| Age group: n (%) | |||
| 18–39 | 7 (3.7%) | 6 (8.8%) | 13 (5.1%) |
| 40–59 | 42 (22.3%) | 19 (27.9%) | 61 (23.8%) |
| 60–69 | 52 (27.7%) | 18 (26.5%) | 70 (27.3%) |
| 70–79 | 58 (30.9%) | 22 (32.4%) | 80 (31.3%) |
| ≥80 | 29 (15.4%) | 3 (4.4%) | 32 (12.5%) |
| Medical diagnosis: n (%) | |||
| Neurological disorders | 60 (31.9%) | 16 (23.5%) | 76 (29.7%) |
| Head and Neck oncology | 59 (31.4%) | 9 (13.2%) | 68 (26.6%) |
| Other | 69 (36.7%) | 43 63.2%) | 112 (43.8%) |
| FOIS | - | ||
| All levels: Med (25; 75%) | 6 (5; 6) | 7 (7; 7) | |
| Per level: n (%) | |||
| 1. Nothing by mouth | 14 (7.4%) | - | - |
| 2. Tube dependent with minimal attempts of food or liquid | 12 (6.4%) | - | - |
| 3. Tube dependent with consistent oral intake of food or liquid | 6 (3.2%) | - | - |
| 4. Total oral diet of a single consistency | 11 (5.9%) | - | - |
| 5. Total oral diet with multiple consistencies, requiring special preparation or compensations | 44 (23.4%) | - | - |
| 6. Total oral diet with multiple consistencies without special preparation, but with specific food limitation | 58 (30.9%) | - | - |
| 7. Total oral diet with no restrictions | 111 (22.9%) | - | - |
| DHI severity (missing data = 13) | (n = 181) | (n = 62) | (N = 243) |
| 1. No difficulty at all | 1 (0.6%) | 8 (12.9%) | 9 (3.7%) |
| 2. | 8 (4.4%) | 8 (12.9%) | 16 (6.6%) |
| 3. | 14 (7.7%) | 2 (3.2%) | 16 (6.6%) |
| 4. Somewhat of a problem | 36 (19.9%) | 14 (22.6%) | 50 (20.6%) |
| 5. | 38 (21.0%) | 10 (16.1%) | 48(19.8%) |
| 6. | 50 (27.6%) | 15 (24.2%) | 65 (26.7%) |
| 7. The worse problem you could have | 34 (18.8%) | 5 (8.1%) | 39 (16.0%) |
| Category | N | % | Average Measures | Infit MnSq | Outfit MnSq | Andrich Thresholds |
|---|---|---|---|---|---|---|
| 0 | 2759 | 43 | −13.52 | 1.05 | 1.10 | None |
| 1 | 1983 | 31 | −2.83 | 0.93 | 1.00 | −4.69 |
| 2 | 1656 | 26 | 8.49 | 0.97 | 1.01 | 4.69 |
| Analysis | Scales | Item/ Person | Rel | Sep | PSI * | Mean Measure | Model SE | MnSq | Z-STD | MnSq | Z-STD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | All 25 items | Person | 0.91 | 3.23 | 4.64 | 45.60 | 3.56 | 1.01 | −0.08 | 1.04 | −0.03 |
| Item | 0.97 | 5.76 | - | 50.00 | 1.03 | 1.01 | −0.15 | 1.04 | 0.12 | ||
| 2 | Physical | Person | 0.76 | 1.76 | 2.68 | 47.51 | 5.73 | 1.01 | −0.05 | 1.02 | −0.05 |
| Scale | Item | 0.96 | 4.89 | - | 50.00 | 1.05 | 1.00 | −0.21 | 1.02 | 0.07 | |
| 3 | Function | Person | 0.82 | 2.13 | 3.17 | 47.40 | 6.27 | 1.00 | −0.04 | 1.03 | 0.02 |
| Scale | Item | 0.98 | 7.72 | - | 50.00 | 1.16 | 1.02 | −0.16 | 1.03 | −0.25 | |
| 4 | Emotional | Person | 0.72 | 1.61 | 2.48 | 44.16 | 6.95 | 1.01 | −0.04 | 1.04 | 0.00 |
| Scale | Item | 0.96 | 4.61 | - | 50.00 | 1.19 | 0.99 | −0.28 | 1.04 | 0.11 |
| All 25 Items | Physical Subscale | Function Subscale | Emotional Subscale | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Infit | Outfit | Infit | Outfit | Infit | Outfit | Infit | Outfit | |||||||||||||
| Items | MnSq | Z-STD | MnSq | Z-STD | PTM Corr. | MnSq | Z-STD | MnSq | Z-STD | PTM Corr. | MnSq | Z-STD | MnSq | Z-STD | PTM Corr. | MnSq | Z-STD | MnSq | Z-STD | PTM Corr. |
| 1 | 0.96 | −0.55 | 1.24 | 2.06 | 0.46 | 0.83 | −2.23 | 0.97 | −0.28 | 0.56 | - | - | - | - | - | - | - | - | - | - |
| 2 | 0.80 | −2.68 | 0.86 | −1.35 | 0.59 | 0.75 | −3.43 | 0.79 | −2.45 | 0.64 | - | - | - | - | - | - | - | - | - | - |
| 3 | 1.28 | 3.38 | 1.53 | 4.41 | 0.46 | 1.08 | 1.01 | 1.15 | 1.65 | 0.58 | - | - | - | - | - | - | - | - | - | - |
| 4 | 1.12 | 1.46 | 1.05 | 0.54 | 0.59 | 0.99 | −0.08 | 0.94 | −0.65 | 0.66 | - | - | - | - | - | - | - | - | - | - |
| 5 | 1.25 | 2.94 | 1.17 | 1.42 | 0.55 | 1.46 | 5.05 | 1.48 | 4.26 | 0.51 | - | - | - | - | - | - | - | - | - | - |
| 6 | 0.99 | −0.05 | 0.94 | −0.53 | 0.68 | - | - | - | - | - | 0.82 | −2.02 | 0.75 | 2.05 | 0.78 | - | - | - | - | - |
| 7 | 1.24 | 2.87 | 1.37 | 3.18 | 0.52 | - | - | - | - | - | 1.38 | 3.79 | 1.62 | 4.26 | 0.62 | - | - | - | - | - |
| 8 | 1.16 | 1.87 | 1.18 | 1.35 | 0.55 | - | - | - | - | - | - | - | - | - | - | 1.23 | 2.38 | 1.20 | 1.78 | 0.66 |
| 9 | 1.02 | 0.29 | 1.01 | 0.16 | 0.64 | - | - | - | - | - | 1.31 | 2.79 | 1.59 | 2.86 | 0.66 | - | - | - | - | - |
| 10 | 1.01 | 0.18 | 0.99 | −0.08 | 0.64 | - | - | - | - | - | 1.11 | 1.19 | 1.10 | 0.79 | 0.71 | - | - | - | - | - |
| 11 | 1.09 | 1.09 | 1.03 | 0.28 | 0.63 | 1.10 | 1.17 | 0.96 | −0.35 | 0.66 | - | - | - | - | - | - | - | - | - | - |
| 12 | 0.70 | −4.18 | 0.66 | −3.17 | 0.69 | - | - | - | - | - | - | - | - | - | - | 0.69 | −3.96 | 0.68 | −3.46 | 0.78 |
| 13 | 0.75 | −3.48 | 0.70 | −3.21 | 0.72 | - | - | - | - | - | - | - | - | - | - | 1.03 | 0.39 | 1.16 | 1.51 | 0.72 |
| 14 | 0.80 | −2.65 | 0.69 | −2.75 | 0.67 | - | - | - | - | - | 0.97 | −0.26 | 0.90 | −0.67 | 0.69 | - | - | - | - | - |
| 15 | 0.84 | −2.05 | 0.76 | −2.17 | 0.67 | - | - | - | - | - | 0.78 | −2.64 | 0.75 | −1.93 | 0.74 | - | - | - | - | - |
| 16 | 0.76 | −3.31 | 0.69 | −3.23 | 0.71 | - | - | - | - | - | 0.80 | −2.42 | 0.77 | −1.91 | 0.76 | - | - | - | - | - |
| 17 | 0.90 | −1.16 | 1.33 | 2.24 | 0.55 | - | - | - | - | - | - | - | - | - | - | 0.86 | −1.56 | 1.01 | 0.16 | 0.70 |
| 18 | 0.70 | −4.35 | 0.68 | −3.43 | 0.72 | - | - | - | - | - | - | - | - | - | - | 0.77 | −2.87 | 0.75 | −2.72 | 0.78 |
| 19 | 1.06 | 0.68 | 1.04 | 0.28 | 0.52 | - | - | - | - | - | - | - | - | - | - | 1.05 | 0.56 | 1.01 | 0.13 | 0.65 |
| 20 | 1.06 | 0.77 | 1.30 | 2.20 | 0.47 | 0.87 | −1.65 | 0.92 | −0.76 | 0.60 | - | - | - | - | - | - | - | - | - | - |
| 21 | 1.15 | 1.69 | 1.35 | 2.40 | 0.46 | - | - | - | - | - | - | - | - | - | - | 1.30 | 3.06 | 1.44 | 3.38 | 0.59 |
| 22 | 1.48 | 3.90 | 1.18 | 0.93 | 0.46 | - | - | - | - | - | 1.41 | 3.18 | 1.26 | 1.03 | 0.56 | - | - | - | - | - |
| 23 | 0.81 | −2.65 | 0.74 | −2.72 | 0.71 | - | - | - | - | - | 0.61 | −5.03 | 0.53 | −4.62 | 0.81 | - | - | - | - | - |
| 24 | 1.25 | 2.88 | 1.54 | 3.96 | 0.44 | 1.09 | 1.15 | 1.15 | 1.51 | 0.55 | - | - | - | - | - | - | - | - | - | - |
| 25 | 0.94 | −0.69 | 1.01 | 0.10 | 0.56 | 0.78 | −2.93 | 0.79 | −2.35 | 0.65 | - | - | - | - | - | - | - | - | - | - |
| Sex | Age | OD vs. No OD | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Items | Mantel–Haenszel Prob. | Prob. | DIF Contrast (Effect Size) & | Summary DIF Chi-Squared | Prob. | DIF Contrast (Effect Size) ∧ | Mantel–Haenszel Prob. | Prob. | DIF Contrast (Effect Size) # |
| 1 | 0.0219 | 0.8824 | 2.14 | 1.7218 | 0.7866 | −4.57 | 0.3165 | 0.5737 | −4.98 |
| 2 | 0.4132 | 0.5204 | 1.98 | 0.4891 | 0.9746 | −1.15 | 0.2510 | 0.6164 | −1.85 |
| 3 | 4.8669 | 0.0274 * | 6.85 * | 5.6128 | 0.2295 | −3.57 | 0.0002 | 0.9897 | −4.35 |
| 4 | 0.2014 | 0.6536 | 0.22 | 12.4567 | 0.0142 * | 9.19 * | 0.2211 | 0.6382 | −2.84 |
| 5 | 0.0312 | 0.8597 | 0.00 | 4.5205 | 0.3395 | 14.08 | 0.3449 | 0.5570 | −1.54 |
| 6 | 0.6014 | 0.4380 | 0.49 | 6.8033 | 0.1462 | 11.80 | 1.2673 | 0.2603 | 6.47 |
| 7 | 1.7715 | 0.1832 | −3.82 | 6.7215 | 0.1509 | −4.57 | 1.4411 | 0.2300 | 1.14 |
| 8 | 0.0009 | 0.9761 | −0.55 | 2.5851 | 0.6291 | −4.77 | 0.2077 | 0.6486 | 0.61 |
| 9 | 1.1216 | 0.2896 | −1.85 | 5.1270 | 0.2740 | 0.46 | 0.3166 | 0.5737 | −0.88 |
| 10 | 0.0597 | 0.8069 | −0.48 | 8.0170 | 0.0906 | 13.02 | 0.4347 | 0.5097 | 1.44 |
| 11 | 0.1059 | 0.7449 | −1.14 | 6.2638 | 0.1798 | 7.12 | 0.0129 | 0.9095 | 2.56 |
| 12 | 0.8468 | 0.3575 | −1.37 | 2.3896 | 0.6641 | 0.92 | 1.8811 | 0.1702 | 0.00 |
| 13 | 0.0373 | 0.8469 | 0.66 | 1.2558 | 0.8688 | 1.25 | 0.8347 | 0.3609 | 2.89 |
| 14 | 0.6785 | 0.4101 | −0.92 | 3.4626 | 0.4830 | −4.26 | 0.0536 | 0.8170 | 4.54 |
| 15 | 0.4824 | 0.4874 | −1.91 | 1.4846 | 0.8292 | 4.67 | 0.8328 | 0.3615 | 0.34 |
| 16 | 0.1101 | 0.7400 | −0.44 | 8.0518 | 0.0894 | 13.90 | 0.0697 | 0.7918 | 4.06 |
| 17 | 0.0623 | 0.8029 | −0.56 | 5.1775 | 0.2690 | −11.16 | 1.8024 | 0.1794 | −5.50 |
| 18 | 2.5779 | 0.1084 | −1.36 | 2.9914 | 0.5588 | −5.21 | 0.0091 | 0.9239 | 3.73 |
| 19 | 1.4001 | 0.2367 | −4.45 | 3.2293 | 0.5197 | −4.07 | 2.0638 | 0.1508 | −4.15 |
| 20 | 0.7719 | 0.3796 | 1.41 | 4.7219 | 0.3165 | −8.17 | 0.0333 | 0.8553 | −5.26 |
| 21 | 0.9496 | 0.3298 | 0.22 | 6.6618 | 0.1544 | −8.41 | 2.3633 | 0.1242 | 1.72 |
| 22 | 0.5081 | 0.4760 | −3.12 | 9.0681 | 0.0592 | 7.28 | 3.0012 | 0.0832 | 17.38 |
| 23 | 0.0064 | 0.9363 | −0.69 | 5.4813 | 0.2408 | 12.56 | 2.9663 | 0.0850 | 9.85 |
| 24 | 5.7798 | 0.0162 * | 7.22 * | 6.6305 | 0.1563 | −13.21 | 6.5539 | 0.0105 * | −10.13 * |
| 25 | 0.9615 | 0.3268 | −1.43 | 7.2009 | 0.1253 | −10.65 | 0.0156 | 0.9005 | −2.91 |
| Diagnostic Category | FOIS | DHI Severity | |||||||
| Items | Summary DIF Chi-Squared | Prob. | DIF Contrast (Effect Size) + | Summary DIF Chi-Squared | Prob. | DIF Contrast (Effect Size)$ | Summary DIF Chi-Squared | Prob. | DIF Contrast (Effect Size) £ |
| 1 | 5.7028 | 0.0566 | −5.40 | 19.5947 | 0.0033 * | −8.00 | 15.6503 | 0.0285 * | −12.13 |
| 2 | 3.3906 | 0.1807 | −3.05 | 4.1668 | 0.6540 | −0.71 | 6.7506 | 0.4552 | −10.05 |
| 3 | 2.2554 | 0.3202 | −0.08 | 20.1350 | 0.0026 * | −7.72 | 25.6152 | 0.0006 * | −10.82 |
| 4 | 2.0901 | 0.3480 | 3.79 | 8.9374 | 0.1769 | 1.30 | 11.2011 | 0.1300 | −8.03 |
| 5 | 1.2538 | 0.5312 | −0.09 | 4.7373 | 0.5778 | 4.88 | 7.9177 | 0.3398 | −0.53 |
| 6 | 6.3553 | 0.0408 * | 4.30 | 27.9819 | 0.0001 * | 9.57 | 6.8707 | 0.4423 | −4.19 |
| 7 | 1.8709 | 0.3888 | −3.36 | 4.7594 | 0.5749 | −4.09 | 9.4548 | 0.2215 | −23.96 |
| 8 | 0.0916 | 0.9571 | −0.80 | 7.1079 | 0.3108 | 2.67 | 4.8344 | 0.6801 | −0.53 |
| 9 | 3.6838 | 0.1559 | −2.94 | 12.6267 | 0.0493 * | 3.36 | 4.0174 | 0.7777 | 15.13 |
| 10 | 0.2233 | 0.8959 | 0.97 | 8.4497 | 0.2068 | 9.09 | 9.1300 | 0.2433 | 15.67 |
| 11 | 1.2911 | 0.5213 | −3.21 | 10.2473 | 0.1145 | 5.36 | 5.4449 | 0.6057 | 7.12 |
| 12 | 3.7545 | 0.1505 | 2.85 | 6.8650 | 0.3333 | −0.51 | 6.8843 | 0.4409 | 3.19 |
| 13 | 1.8676 | 0.3894 | 2.09 | 3.7856 | 0.7056 | 11.78 | 6.8097 | 0.4488 | 15.67 |
| 14 | 0.9241 | 0.6278 | 0.96 | 3.1711 | 0.7870 | −4.42 | 12.2744 | 0.0918 | 13.78 |
| 15 | 1.9981 | 0.3646 | −1.02 | 15.3185 | 0.0179 * | −2.44 | 0.3943 | 0.2990 | −4.65 |
| 16 | 1.2585 | 0.5299 | 2.79 | 14.8529 | 0.0214 * | −1.72 | 9.4284 | 0.2232 | 11.82 |
| 17 | 1.9294 | 0.3775 | −2.10 | 12.6429 | 0.0490 * | −9.87 | 3.4994 | 0.8353 | −2.16 |
| 18 | 0.9943 | 0.6059 | 2.28 | 6.6258 | 0.3566 | 1.29 | 11.6305 | 0.1133 | 15.68 |
| 19 | 0.0177 | 0.9920 | 0.26 | 9.5248 | 0.1460 | −3.01 | 3.6010 | 0.8244 | −11.71 |
| 20 | 16.8816 | 0.0002 * | −0.36 | 22.1033 | 0.0012 * | 4.40 | 20.1818 | 0.0052 * | 15.68 |
| 21 | 0.5044 | 0.7769 | −1.05 | 8.6827 | 0.1920 | −7.73 | 8.2005 | 0.3151 | −16.65 |
| 22 | 10.7063 | 0.0046 * | −1.43 | 56.8543 | 0.0000 * | 0.88 | 11.7623 | 0.1086 | −14.55 |
| 23 | 7.7838 | 0.0199 * | 6.45 | 31.6820 | 0.0000 * | 8.13 | 9.9422 | 0.1917 | 9.80 |
| 24 | 30.8835 | 0.0000 * | −0.76 | 25.5090 | 0.0003 * | −0.96 | 8.2663 | 0.3096 | −0.53 |
| 25 | 1.6022 | 0.4453 | −1.11 | 10.9412 | 0.0901 | −2.30 | 14.8209 | 0.0383 * | 3.19 |
| All 25 Items | Physical Scale | Function Scale | Emotional Scale | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variance | Eigenvalue | Observed (%) | Expected (%) | Eigenvalue | Observed (%) | Expected (%) | Eigenvalue | Observed (%) | Expected (%) | Eigenvalue | Observed (%) | Expected (%) |
| Total raw variance in observations | 43.80 | 100 | 100 | 14.70 | 100 | 100 | 19.65 | 100.0 | 100.0 | 12.66 | 100.0 | 100.0 |
| Raw variance explained by measures | 18.80 | 42.9 | 42.7 | 5.70 | 38.8 | 38.4 | 10.65 | 54.2 | 54.2 | 5.66 | 44.7 | 43.9 |
| Raw variance explained by persons | 9.05 | 20.7 | 20.6 | 2.72 | 18.5 | 18.3 | 5.53 | 28.2 | 28.2 | 3.02 | 23.8 | 23.4 |
| Raw variance explained by items | 9.75 | 22.3 | 22.2 | 2.98 | 20.3 | 20.1 | 5.12 | 26.0 | 26.0 | 2.64 | 20.9 | 20.5 |
| Unexplained Variance | Raw Unexplained Variance (Total) | 1st Contrast | 2nd Contrast | 3rd Contrast | 4th Contrast | 5th Contrast | |
|---|---|---|---|---|---|---|---|
| Full scale | Eigenvalue | 25.0 | 3.4 | 2.1 | 1.8 | 1.6 | 1.3 |
| Observed (%) | 57.1 | 7.8 | 4.8 | 4.1 | 3.7 | 3.0 | |
| Expected | 57.3 | 13.7 | 8.4 | 7.2 | 6.4 | 5.2 | |
| Physical subscale | Eigenvalue | 9.0 | 1.7 | 1.4 | 1.3 | 1.1 | 1.0 |
| Observed (%) | 61.2 | 11.7 | 9.6 | 9.0 | 7.6 | 7.0 | |
| Expected (%) | 61.6 | 19.1 | 15.6 | 14.7 | 12.4 | 11.4 | |
| Function subscale | Eigenvalue | 9.0 | 1.9 | 1.5 | 1.2 | 1.0 | 1.0 |
| Observed (%) | 45.8 | 9.4 | 7.4 | 6.2 | 5.3 | 5.2 | |
| Expected (%) | 45.8 | 20.6 | 16.2 | 13.6 | 11.5 | 11.4 | |
| Emotional subscale | Eigenvalue | 7.0 | 1.7 | 1.2 | 1.2 | 1.1 | 1.0 |
| Observed (%) | 55.3 | 13.6 | 9.7 | 9.1 | 8.5 | 7.9 | |
| Expected (%) | 56.1 | 24.6 | 17.6 | 16.4 | 15.4 | 14.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordier, R.; Joosten, A.V.; Heijnen, B.J.; Speyer, R. A Psychometric Evaluation of the Dysphagia Handicap Index Using Rasch Analysis. J. Clin. Med. 2024, 13, 2331. https://doi.org/10.3390/jcm13082331
Cordier R, Joosten AV, Heijnen BJ, Speyer R. A Psychometric Evaluation of the Dysphagia Handicap Index Using Rasch Analysis. Journal of Clinical Medicine. 2024; 13(8):2331. https://doi.org/10.3390/jcm13082331
Chicago/Turabian StyleCordier, Reinie, Annette Veronica Joosten, Bas J. Heijnen, and Renée Speyer. 2024. "A Psychometric Evaluation of the Dysphagia Handicap Index Using Rasch Analysis" Journal of Clinical Medicine 13, no. 8: 2331. https://doi.org/10.3390/jcm13082331